Process for Regulating Acid–Base Balance
Acid–Base Homeostasis
To understand acid–base balance, it is important to first have a basic knowledge of pH, which is a reflection of the degree of acidity or alkalinity of a substance determined by the hydrogen ion (H+) concentration. On the pH scale, which ranges from 0 (strongly acidic) to 14 (strongly alkaline), 7 is considered neutral. pH concentrations that are less than 7 are considered acidic, while those that are higher than 7 are considered alkaline. The expected reference range for the pH of human blood is quite narrow, 7.35 to 7.45, with few individuals surviving with a pH of 6.9 or less. The body maintains the blood’s pH in this narrow window through the use of buffers and respiratory and renal regulation, which prevent the blood from becoming too acidic or alkaline. A buffer is a substance that has the chemical ability to absorb changes in pH when an acid or base is added to the solution. The lungs utilize carbonic acid, which is created when carbon dioxide (CO2) mixes with water, which is slightly acidic, while the kidneys utilize bicarbonate (HCO3–), which is slightly alkaline, to maintain the appropriate acid–base balance. These processes, along with the chemical buffers such as lactic acid, amino acids, and plasma proteins, help maintain the homeostasis of acidic and basic (alkaline) compounds in the blood to maintain blood pH between 7.35 and 7.45.
acid–base balance
The homeostasis of acidic and basic (alkaline) compounds in the blood to maintain a blood pH of between 7.35 and 7.45.
Minimal variations from the expected pH reference ranges can lead to significant effects on vital organs in the body. An arterial blood gas (ABG) is the laboratory evaluation used to interpret acid–base balance in the body. To perform an ABG, a blood sample is drawn from an artery, usually the radial artery. The sample is then analyzed for pH, which determines the acidity or alkalinity of the blood; partial pressure of carbon dioxide (PaCO2); and bicarbonate (HCO3–). These results will indicate whether there is an acid–base imbalance in the body. An ABG also provides an indirect measure of the oxygen content in the arterial blood (PaO2) and the percentage of hemoglobin saturation of the blood (O2 sat).
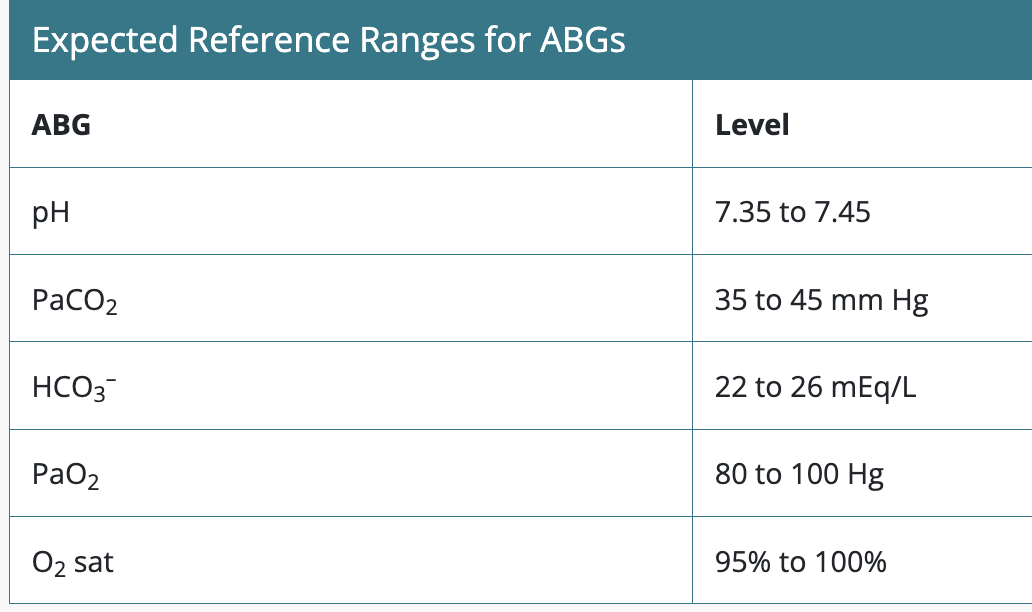
The pH represents the amount of hydrogen ions in the blood. As noted earlier, the expected reference level for the pH of blood in the body is a narrow range, 7.35 to 7.45. When the acidity of the blood increases, the pH level decreases. When the alkalinity of the blood increases, the pH level rises.
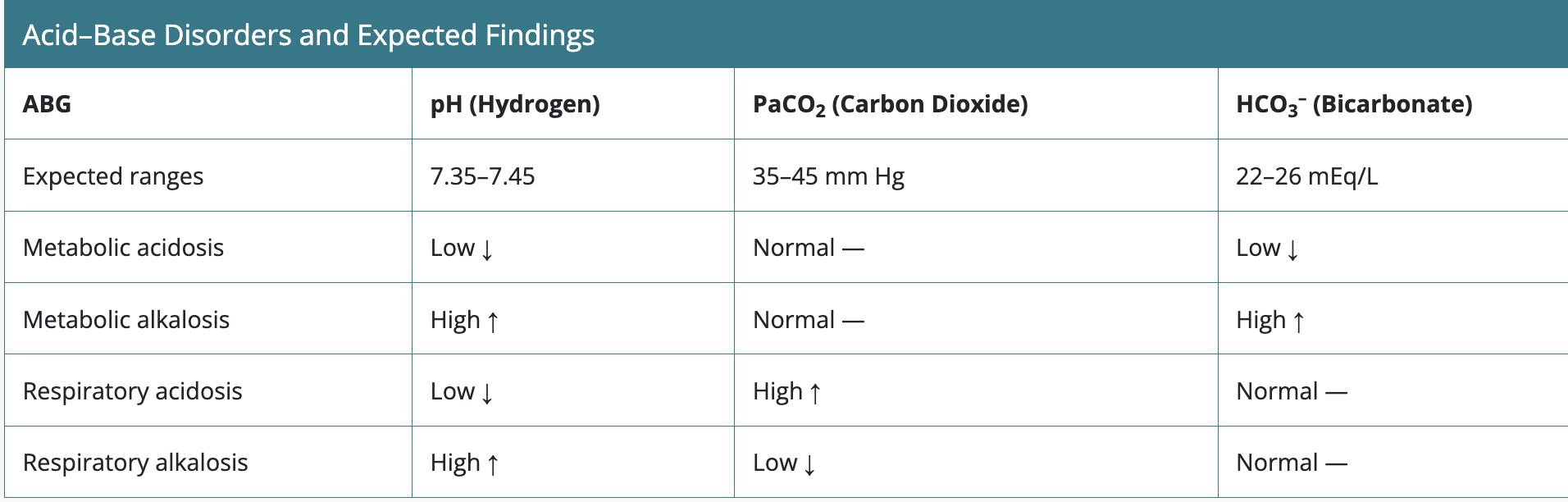
Imbalances of pH will lead to either acidosis (a pH lower than the expected reference of 7.35 on the pH scale) or alkalosis (a higher pH than the expected reference of 7.45 on the pH scale). The origin of the imbalance can be attributed, in many cases, to a respiratory or a metabolic problem. This determination is based on clinical conditions and whether the pH level is altered due to changes in PaCO2, which would indicate a respiratory problem, or HCO3–, which indicates a metabolic problem.
acidosis
Levels of acid in the blood are too high, a pH of less than 7.35.
alkalosis
The blood is too alkaline, a pH of greater than 7.45.
Respiratory imbalances occur with changes in ventilation and reflect the amount of carbon dioxide present. When carbon dioxide combines with water, it forms carbonic acid (which makes for an acidic environment). When a client experiences hypoventilation, CO2 is retained, more CO2 is converted to carbonic acid, and an increase in acidity occurs.
Metabolic imbalances may also occur with systemic changes. The kidneys filter hydrogen (H+) and HCO3– and either excrete them in the urine or reabsorb them back into the bloodstream. If HCO3– is excreted and H+ is retained, the pH level will decrease, resulting in metabolic acidosis. In contrast, if H+ is excreted and HCO3– is retained, the pH level will increase, resulting in metabolic alkalosis.
In most cases, the kidneys and lungs work collaboratively and balance the acids and buffers maintaining homeostasis. However, when one or both of these systems fail, an acid–base imbalance (acidosis or alkalosis) occurs.
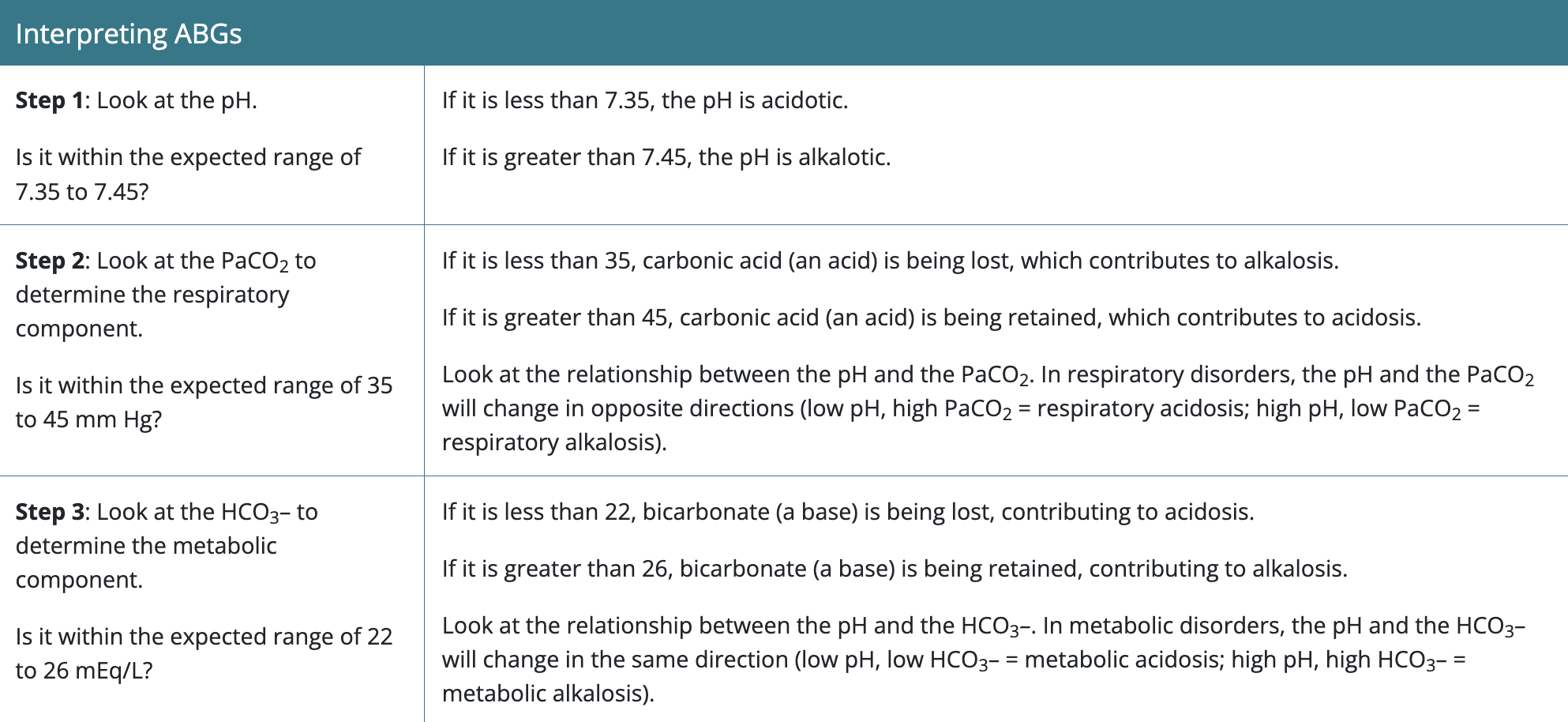
Interpreting ABGs
Example 1
Lab Results
pH: 7.42
PaCO2: 37 mm
HgHCO3–: 25 mEq/L
Is each level within the expected reference range? If not, is it low or high?
All levels are within the expected reference range.
What do these labs indicate?
The client’s labs are within expected reference range. The client is not experiencing an imbalance.
Example 2
Lab Results
pH: 7.33
PaCO2: 35 mm
HgHCO3–: 20 mEq/L
Is each level within the expected reference range? If not, is it low or high?
The pH is low, which means it is acidic. The PaCO2 is normal. The HCO3– is low, which represents a metabolic issue (lack of base leading to acidosis).
What do these labs indicate?
These labs indicate metabolic acidosis.
Example 3
Lab Results
pH: 7.49
PaCO2: 32 mm
HgHCO3–: 24 mEq/L
Is each level within the expected reference range? If not, is it low or high?
The pH is high, which means it is alkalotic. The PaCO2 is low, which represents a respiratory issue (lack of acid leading to alkalosis). The HCO3– is normal.
What do these labs indicate?
These labs indicate respiratory alkalosis.
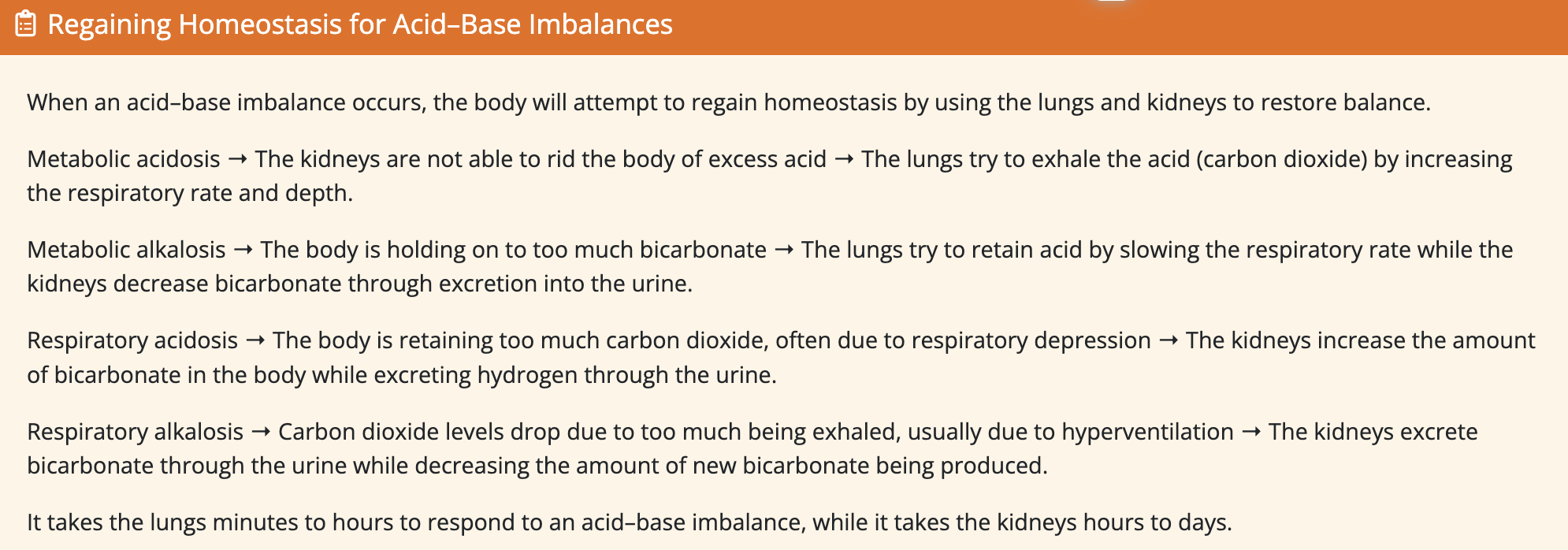
When an acid–base imbalance occurs, the body will take actions to resume homeostasis. It does this through a form of counterbalance. For example, if the client is experiencing metabolic acidosis, the body will try to correct this imbalance using the respiratory system. Specifically, the client will increase the rate and depth of respirations in an attempt to excrete CO2 and increase the pH of the blood.
Acid–Base Balance, Imbalances, and Excretion
The causes and manifestations of acid–base imbalances vary. When the lungs cannot remove enough carbon dioxide from the body, respiratory acidosis can occur (low pH, elevated PaCO2). Causes of respiratory acidosis include the following:
Central nervous system depression—for example, from trauma, opioids, sedatives, or anesthesia
Spinal cord injury with impaired respiratory function
Pulmonary diseases—for example, atelectasis, pneumonia, pulmonary embolism, or obstructive pulmonary disorders
Functional disorders limiting respirations—for example, chest wall injury or abdominal distention (Patel, 2023)
As these causes indicate, respiratory acidosis can be an acute or a chronic condition. In chronic conditions, such as chronic obstructive pulmonary disorder (COPD), the body adjusts over time. In contrast, acute episodes of respiratory acidosis occur quickly and require intervention. The body will attempt to regain homeostasis by retaining HCO3– (a base); however, it takes the kidneys hours to days to regain homeostasis. Exacerbations of chronic respiratory conditions are often due to a respiratory virus infection and will result in respiratory acidosis.
Manifestations of respiratory acidosis can include anxiety and confusion, fatigue, shortness of breath, lethargy, and sleepiness. Treatment depends on identifying the underlying cause and can include supplemental oxygen administration and medications such as bronchodilators and corticosteroids. Nursing interventions for a client who is experiencing respiratory acidosis include monitoring respiratory effort, lung sounds, and the airway; monitoring vital signs, I&O, and subsequent ABGs or other laboratory results; and administering treatments as prescribed.
Like respiratory acidosis, respiratory alkalosis (high pH, decreased PaCO2) can be acute or chronic. It can be caused by any condition that results in hyperventilation, such as pain, anxiety, severe stress, head injury, stroke, hyperthyroidism, trauma, or medications. Manifestations of respiratory alkalosis depend on the severity of the PaCO2 decrease. Along with hyperventilation, other signs include lightheadedness, dizziness, confusion, chest discomfort, tachycardia, and altered mental status.
Treatment of respiratory alkalosis focuses on decreasing the rate of breathing in addition to treating the cause. If the alkalosis is the result of anxiety, breathing into a paper bag or applying oxygen using a partial rebreathing mask can help increase the CO2 levels—with these interventions, the client rebreathes the air they have expired. Nursing interventions include monitoring the client’s respiratory status, including effort, depth, and rate; vital signs; I&O; neuromuscular status; and subsequent ABGs or other laboratory results. The nurse should place the client on fall precautions related to the neurologic and musculoskeletal manifestations of the imbalance.
Metabolic acidosis (low pH, decreased HCO3–) can be the result of either too little HCO3- in the bloodstream or too much acid other than CO2. Causes of metabolic acidosis include the following conditions:
Renal or hepatic failure
Pancreatitis
Dehydration
Diarrhea
Starvation
Diabetic ketoacidosis
Lactic acidosis (cancer, alcohol toxicity, cardiac arrest)
Salicylate intoxication
Manifestations of metabolic acidosis depend on the cause, but can include long and deep breaths (Kussmaul respirations), confusion, headache, tachycardia, lethargy, loss of appetite, and nausea and vomiting. If the cause is not corrected, metabolic acidosis can become severe, and shock or death can occur.
Treatment of metabolic acidosis is aimed at correcting the underlying cause, with the goal of ridding the body of the excess acid. Sodium bicarbonate (a base) is often given to neutralize the acid in the blood, and IV fluids will be administered. Nursing interventions for a client who is experiencing respiratory acidosis include monitoring respiratory effort, lung sounds, and the airway; monitoring vital signs, I&O, and subsequent ABGs or other laboratory results; and administering medications and treatments as prescribed.
Metabolic alkalosis (high pH, elevated HCO3) occurs when there is an excessive amount of HCO3- in the blood or an increased loss of acid. Causes of metabolic alkalosis may include prolonged vomiting, gastric suctioning, excessive use of diuretics or antacids, renal impairment, hypokalemia, or hypovolemia.
Manifestations of metabolic alkalosis can include the following:
Muscle twitching or spasms
Lethargy
Nausea and vomiting
Tremors or numbness of the hands
Tingling of the face or feet
Lightheadedness
Headache
With severe metabolic alkalosis, confusion, seizures, agitation, and coma; arrhythmias can occur
Treatment depends on identifying and reversing the underlying cause. Nursing interventions include monitoring the client’s respiratory status including effort, depth, and rate; vital signs; I&O; neuromuscular status; and subsequent ABGs or other laboratory results. The nurse should place the client on fall precautions related to the neurologic and musculoskeletal manifestations of the imbalance.
Role of the Nurse: Clients Who Have Acid-Base Imbalance
The nursing process can lead the nurse who is caring for a client who is experiencing an acid–base imbalance. Nursing actions that should be performed for the client include assessment, analysis, planning, implementation, and evaluation. During the assessment phase, the nurse should assess subjective and objective data, including reports from the client, vital signs, manifestations, and ABG reports. Nursing analysis should be performed by the RN to assist in developing a plan of care while following Maslow’s hierarchy of needs. Client goals are formulated during the planning stage in collaboration with the client. Goals should be specific, measurable, attainable, realistic, and time oriented. The plan of care is put into action during the implementation phase by initiating nursing interventions that promote recovery for the client. The final stage of the plan of care evaluates outcomes to determine if the interventions implemented met the established goals.
Through a careful review of the client’s laboratory values, history, and clinical presentation, the nurse can assist in identifying the cause of an acid–base imbalance. Utilizing the nursing process is an effective means of identifying needs, developing and implementing interventions, and then evaluating the outcome of those interventions. If a client is suspected of having an acid–base imbalance, appropriate nursing assessment and analysis should be completed. Obtaining ABGs can help narrow the list of potential problems, especially if the client has experienced any of the following:
Respiratory distress
Changes in the level of consciousness
Trauma
Diabetes mellitus
Sepsis
Dehydration
Intoxication with poisons or other toxins
In each case, it is important to look at the big picture, including the manifestations the client is experiencing, the client’s medications, the client’s clinical condition, and any lab results that are available, such as electrolytes, blood urea nitrogen, and creatinine as well as ECG tracings to identify potential arrhythmias. If ABGs have been obtained, the nurse’s role includes analysis of the results and determination of the client’s condition (e.g., acidosis versus alkalosis, metabolic versus respiratory). Interventions that may potentially be implemented include monitoring and addressing hypoxia, such as by elevating the head of the bed and providing oxygen if needed. Blood glucose levels and maintaining the client’s safety are also important interventions. In some cases, such as with clients having metabolic alkalosis, it would be important to initiate seizure precautions and continuous cardiac monitoring.
A client who is experiencing respiratory alkalosis would be expected to have an ineffective breathing pattern due to hyperventilation. Hyperventilation will affect the client’s respiratory rate, depth, and overall effort. If the client’s breathing pattern has changed from the baseline, anxiety or pain may be the cause. During the planning phase of the nursing process, goals should be developed that are tailored to the client’s needs and the cause of the client’s current problem. For example, if a client is experiencing respiratory alkalosis caused by hyperventilation, a pertinent goal would be to stabilize the client’s respiratory rate and pattern. Determining the cause of the client’s changed breathing pattern will help determine the best intervention for care to reach this goal. Nursing interventions for this goal include offering a paper bag for the client to breathe into to promote rebreathing and help decrease anxiety. Other interventions might include encouraging the client to speak and breathe slowly and providing comfort to the client. The nurse should also work with the members of the interprofessional team to complete a medication reconciliation and identify any medications that may have resulted in the acid–base imbalance. The final step in the nursing process is evaluation, in which the nurse determines if the interventions have helped the client meet the goals. This can be done by reviewing subsequent ABG or other laboratory results that have been prescribed by the client’s provider. The nurse should continue to monitor the client’s respiratory depth, rate, and effort.
While caring for a client with an acid–base imbalance, the nurse may have to repeat the steps of the nursing process several times to reach the end goal of restoring the client’s homeostasis. Once the client is stable, it is important to provide education about the link between the acid–base imbalance and the identified cause, as well as risk factors for continued acid–base imbalance.