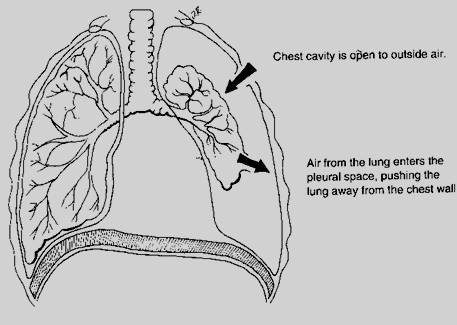
Pneumothorax (Air in Lungs)
It is the accumulation of air in the pleural space, which results in partial or complete lung collapse.
Diagnosis
X-ray or CT scan - shows tracheal deviation or placement away from affected side
Types:
Tension – air enters but can’t leave pleural space (one-way valve)
Secondary – air enters the pleural space as a result of injury to the chest wall, respiratory structures or esophagus
Spontaneous – air enters the pleural space when air-filled blebs (blisters) on the lung surface rupture.
Etiology
Tension pneumothorax - unknown causes
Secondary pneumothorax – injury to the chest wall from trauma
Spontaneous – ruptured bleb (common to smokers).
Pathophysiologic Processes and Manifestations
Severity of symptoms depends on the size of injury and the amount of tissue left intact.
Symptoms can include
Pleuritic pain (sharp pain occurring during inhalation)
Increased RR
Dyspnea
Asymmetry of chest wall (from rib fractures)
Decreased breath sounds over the area of pneumothorax
Hyperresonance in percussion
Trachea deviating to the injury site
Shifting of mediastinal structures to unaffected side of unaffected chest
Signs of shock (due to large pneumothorax)
In tension pneumothorax, onset is sudden and painful (can affect the heart)
Nursing Interventions
Monitor V/S, signs of shock
No shortness of breath, no treatment
Observe respiration; changing pattern may indicate worsening situation
Semi-Fowler’s position
Administer oxygen if necessary
Analgesics as ordered
Chest tube - escape route for air given in worse situation like tension or spontaneous
Maintain sterile dressing at chest tube insertion site
Maintain patency and integrity of closed chest drainage system
Evaluate amount of fluid and breath sounds.