2023 Cancer student copy
Cancer Education and Care
Cancer Pathophysiology
Mutation of cellular genes leads to abnormal cell growth.
Lack of cell division limit
contact inhibition
grow invade tissue
Cancer Classification
Benign
Noninvasive
slow growth rate
no metastasis
well-differentiated
encapsulated
Malignancy
Gains access to blood and lymph channels
invassice
variable or rapid growth rate
infiltrates surrounding tissue
undifferentiated
By Tissue of Origin:
Carcinoma: Cancer that originates in epithelial cells, which line the internal and external surfaces of the body. Examples include breast, lung, and prostate cancer.
Sarcoma: Cancer that originates in connective tissues such as bone, cartilage, fat, muscle, or blood vessels.
Leukemia: Cancer of the blood or bone marrow, characterized by the rapid production of abnormal white blood cells.
Lymphoma: Cancer that begins in the lymphatic system, which includes the lymph nodes, spleen, and other organs of the immune system.
Myeloma: Cancer that develops in plasma cells, a type of white blood cell found in the bone marrow.
Origin varies from organs, connective tissue, organs fighting infection, epithelial cells, and plasma cells.
Etiology
Factors like carcinogen exposure and cancer cell growth contribute.
Carcinogen: A substance capable of causing cancer in living tissue. Common examples include tobacco smoke, asbestos, and certain chemicals.
Cancer Cell Growth and Reproduction:
Cancer cells grow uncontrollably due to mutations in genes that regulate cell division. They can reproduce rapidly, forming tumors that invade surrounding tissues and spread to other parts of the body through metastasis.
Initiation: Genetic mutations occur, often due to exposure to carcinogens or genetic factors, initiating abnormal cell growth.
Promotion: Initiated cells undergo further changes, promoted by factors like hormones or inflammation, leading to increased cell proliferation.
Progression: Cells become increasingly malignant, acquiring more mutations and characteristics that enable invasion and metastasis, marking the transition to aggressive cancer.
A healthy immune system can destroy cancer cells before tumor formation.
Risk factors
Tobacco Use: Smoking and using tobacco products increase the risk of many types of cancer, including lung, mouth, throat, esophagus, bladder, kidney, and pancreatic cancer.
Exposure to Carcinogens: Exposure to certain chemicals and substances in the environment, workplace, or household can increase cancer risk. This includes exposure to asbestos, benzene, arsenic, radon, and certain industrial chemicals.
Ultraviolet (UV) Radiation: Overexposure to UV radiation from the sun or tanning beds increases the risk of skin cancer, including melanoma, basal cell carcinoma, and squamous cell carcinoma.
Diet and Nutrition: A diet high in processed meats and red meats and low in fruits, vegetables, and fiber may increase the risk of colorectal cancer. Obesity and overweight are also linked to an increased risk of several cancers, including breast, prostate, colorectal, and pancreatic cancer.(Fiber and vitamins A,C,D reduce risk)
Alcohol Consumption: Excessive alcohol consumption is associated with an increased risk of several cancers, including liver, breast, colorectal, and esophageal cancer.
Physical Activity Level: Lack of regular physical activity or sedentary behavior is linked to an increased risk of various cancers, including breast, colon, and endometrial cancer.
Genetic Factors: Inherited genetic mutations can increase the risk of certain types of cancer, such as breast cancer (BRCA1 and BRCA2 mutations), colorectal cancer (hereditary nonpolyposis colorectal cancer or Lynch syndrome), and others.
Age: The risk of developing cancer increases with age, as cellular damage accumulates over time.
Chronic Inflammation: Chronic inflammation, such as that caused by conditions like inflammatory bowel disease (IBD) or chronic infections, can increase the risk of certain cancers, including colorectal and liver cancer.
Hormonal Factors: Hormonal factors can influence the risk of certain cancers. For example, hormone replacement therapy (HRT) and oral contraceptives may increase the risk of breast and ovarian cancer, while hormonal imbalances can increase the risk of endometrial and prostate cancer.
Metastasis
Metastasis is the process by which cancer cells spread from the primary tumor to other parts of the body, forming secondary tumors. It involves several steps:
Invasion: Cancer cells break away from the primary tumor and invade nearby tissues. They can penetrate the surrounding tissue's blood vessels, lymphatic vessels, or other structures.
Transportation: Once cancer cells invade blood vessels or lymphatic vessels, they can travel through the bloodstream or lymphatic system to distant parts of the body. This transportation can occur via mechanical means, such as the flow of blood or lymph fluid carrying the cancer cells to different locations.
Lodgment: Cancer cells reach distant organs or tissues and may exit the bloodstream or lymphatic vessels. They then lodge and establish themselves in the new location, where they start to grow and form secondary tumors.
Growth: Cancer cells proliferate and grow in the new location, forming metastatic tumors. These tumors can disrupt the normal function of the affected organ or tissue and can be more challenging to treat than the primary tumor.
Prevention
Early detection, regular screening, genetic testing, healthy lifestyle, Protectant foods( Folate, Fruits, and vegetables), Vaccines
Vaccines play a significant role in preventing certain types of cancer by targeting infectious agents known to cause cancer or by boosting the body's immune response against cancer cells. Here are some examples of vaccines and their relation to cancer:
HPV Vaccine: Prevents HPV infections, lowering the risk of cervical and other cancers.
Hepatitis B Vaccine: Reduces the risk of liver cancer by preventing chronic HBV infection.
Hepatitis C Treatment: Antiviral treatments for HCV decrease the risk of liver cancer.
Experimental Cancer Vaccines: Being developed to stimulate the immune system to target and destroy cancer cells.
Diagnostic Tests
Imaging Tests: X-rays, CT scans, MRIs, ultrasounds, and PET scans provide detailed images of the body to detect tumors.
Biopsy: Tissue samples are taken and examined under a microscope to confirm the presence of cancer cells.
Blood Tests: Analyze blood for markers(WBCS) Hemoglobin that low, that may indicate cancer, such as tumor markers or genetic tests.
Anemia: Lower than normal levels of red blood cells or hemoglobin may indicate certain types of cancer, such as leukemia or gastrointestinal bleeding.
Leukocytosis or Leukopenia: Elevated or decreased levels of white blood cells may indicate infections or leukemia.
Thrombocytosis or Thrombocytopenia: Elevated or decreased levels of platelets may suggest leukemia, lymphoma, or bone marrow disorders.
Endoscopy: Uses a camera to examine internal organs like the gastrointestinal tract or respiratory system for signs of cancer.
Molecular Testing: Analyzes DNA, RNA, or proteins in tumors to identify specific genetic mutations or biomarkers.
Tumor Markers
Prostate-Specific Antigen (PSA): Associated with prostate cancer. PSA levels can also be elevated in non-cancerous conditions such as benign prostatic hyperplasia (BPH) or prostatitis.
Carcinoembryonic Antigen (CEA): Associated with colorectal cancer and other gastrointestinal cancers. Elevated levels can also be seen in other conditions such as inflammatory bowel disease (IBD) or smoking.
CA-125: Associated with ovarian cancer. CA-125 levels can also be elevated in conditions such as endometriosis or pelvic inflammatory disease.
CA 15-3 and CA 27.29: Associated with breast cancer. Elevated levels may also be seen in other conditions such as benign breast disease or liver disease.
AFP (Alpha-fetoprotein): Associated with liver cancer (hepatocellular carcinoma) and certain germ cell tumors. AFP levels can also be elevated in pregnancy or certain liver diseases.
CA 19-9: Associated with pancreatic cancer and other gastrointestinal cancers. Elevated levels can also be seen in conditions such as pancreatitis or bile duct obstruction.
Cancer Staging
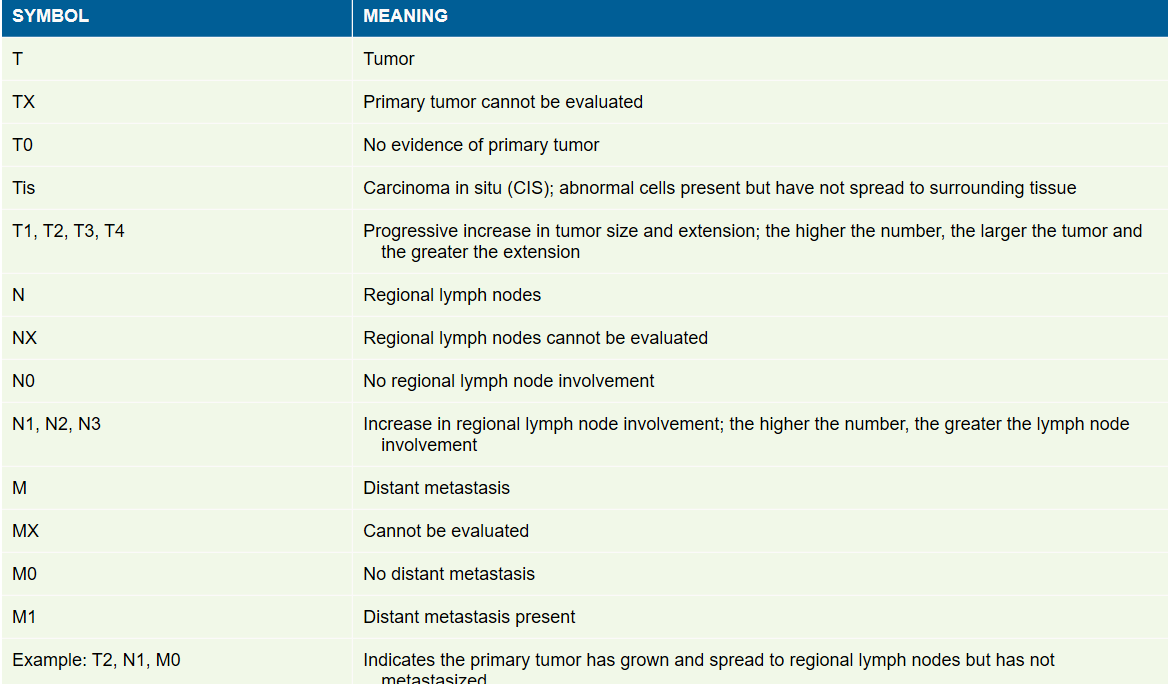
Cancer staging is a system used to describe the extent and spread of cancer in the body. Staging helps doctors determine the appropriate treatment plan and predict the prognosis for patients. The most commonly used cancer staging system is the TNM system, which stands for:
T (Tumor): Indicates the size and extent of the primary tumor. Tumor size is often categorized into different stages, with higher stages indicating larger or more invasive tumors.
T1=small t2=medium t3=large t4=very large
N (Node): Indicates whether cancer has spread to nearby lymph nodes. Lymph nodes are small, bean-shaped structures that play a role in the body's immune system. The presence of cancer cells in lymph nodes may indicate a higher risk of cancer spreading to other parts of the body.
M (Metastasis): Indicates whether cancer has spread to distant organs or tissues beyond the primary tumor and nearby lymph nodes. The presence of metastasis usually indicates a more advanced stage of cancer.
In addition to the TNM system, cancer staging often includes a numerical stage grouping, typically ranging from stage 0 to stage IV, to simplify communication about the extent of cancer. The specific stages may vary depending on the type of cancer, but they generally follow a similar pattern:
Stage 0: Indicates cancer in situ, meaning it is confined to its site of origin and has not spread to nearby tissues.
Stage I: Indicates a small tumor that has not spread beyond its site of origin.
Stage II: Indicates a larger tumor or one that has spread to nearby tissues or lymph nodes.
Stage III: Indicates a more advanced tumor that may have spread to nearby tissues or lymph nodes, depending on the cancer type.
Stage IV: Indicates cancer that has spread to distant organs or tissues, also known as metastatic cancer.
Tumor Grade:
Tumor grade refers to a system used to classify cancer cells based on their appearance and how abnormal they appear under a microscope compared to normal cells. Tumor grade provides information about how quickly a tumor is likely to grow and spread. The higher the grade the more aggressive the cancer is. The grading system varies depending on the type of cancer, but it generally includes the following grades:
Grade 1 (Low Grade): The cancer cells resemble normal cells and tend to grow slowly. These tumors are considered well-differentiated and are less aggressive.
Grade 2 (Intermediate Grade): The cancer cells are somewhat abnormal in appearance and may grow and spread at a moderate rate. These tumors are moderately differentiated.
Grade 3 (High Grade): The cancer cells appear highly abnormal and are likely to grow and spread rapidly. These tumors are poorly differentiated or undifferentiated and are more aggressive.
Grade 4 (highly abnormal) grow rapidly, and are poorly differentiated. They are associated with aggressive behavior and typically require aggressive treatment. Prognosis for Grade 4 tumors is generally poorer compared to lower grade tumors.
Warning Signs of Cancer
Change in bowel or bladder habits
A sore that does not heal
Unusual bleeding or discharge in stool
Thickening or lump in the breast, testicles, or elsewhere
Indigestion or difficulty swallowing
Obvious change in the size of wart or mole
Nagging cough or hoarsenes
Types of cancer
10 most common types in the U.S:
Skin cancer
Breast cancer
Prostate cancer
Lung cancer
Colorectal cancer
Melanoma Bladder cancer
Non-Hodgkin's lymphoma
Kidney (renal) cancer
Endometrial cancer
Pancreatic Brain Cancer
Liver Cancer Testicular
Cancer Thyroid Cancer
Skin cancer
Basal Cell Carcinoma (BCC): Basal cell carcinoma is the most common type of skin cancer. It typically appears as a small, shiny bump or a pinkish patch of skin. BCC usually grows slowly and rarely spreads to other parts of the body. It is often found on sun-exposed areas such as the face, scalp, ears, and neck.
Squamous Cell Carcinoma (SCC): Squamous cell carcinoma is the second most common type of skin cancer. It often appears as a red, scaly patch or a firm, raised bump, Crusted or scaly. ( If the lesion is neglected or irritated. SCC can grow more quickly than BCC and has a higher risk of spreading to other parts of the body, although this is still relatively uncommon. It is also commonly found on sun-exposed areas of the skin.
Melanoma: Melanoma is less common than basal cell carcinoma and squamous cell carcinoma but is more likely to spread if not detected and treated early. Melanoma typically appears as a new spot or a change in an existing mole. It may have irregular borders and uneven coloring and can vary in size. Melanoma can occur anywhere on the body, including areas not exposed to the sun.- Most dangerous
Risk Factors
Fair skin
Prolonged UV exposure
Multiple moles X-ray therapy
Scar tissue
Ulceration
Signs of skin cancer
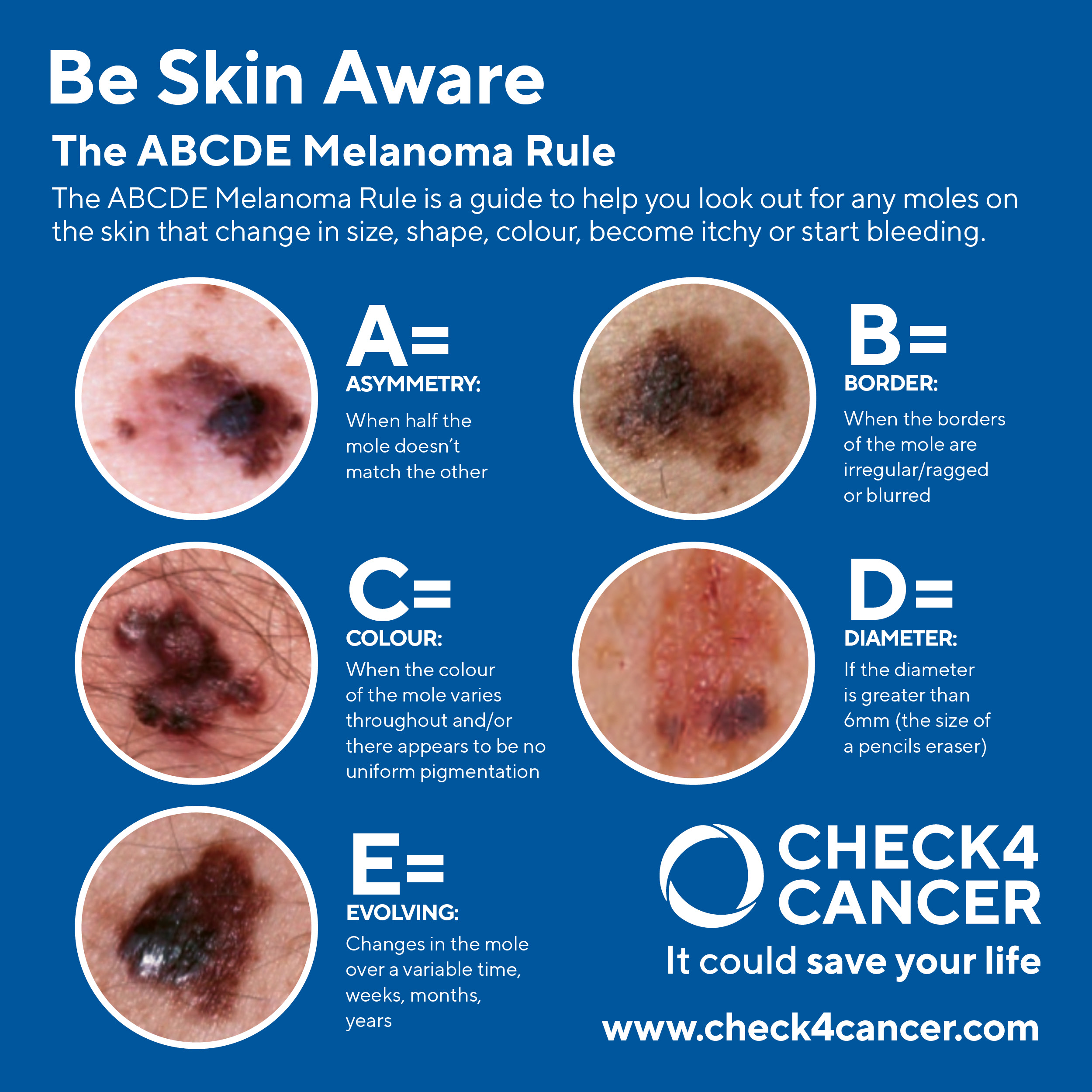
The ABCDE rule is a helpful mnemonic used for identifying signs of melanoma, the deadliest form of skin cancer. Here's what each letter stands for:
A: Asymmetry: One half of the mole or spot does not match the other half in size, shape, or color.
B: Border irregularity: The edges of the mole are irregular, ragged, notched, or blurred instead of smooth.
C: Color variation: The mole has different colors or shades within it, such as black, brown, tan, red, white, or blue.
D: Diameter: The mole is larger than 6 millimeters (about the size of a pencil eraser) in diameter, although melanomas can sometimes be smaller.
E: Evolution or change: The mole has changed in size, shape, color, or elevation, or it looks different from other moles on the body.
Treatment
Excision is a medical procedure involving the surgical removal of tissue or a part of the body. It is commonly used to remove tumors, cysts, or other abnormal growths. The goal of excision is to eliminate the diseased or unwanted tissue while preserving as much healthy tissue as possible.
Cryosurgery is a medical procedure that uses extreme cold to destroy abnormal tissues, such as tumors or warts. Liquid nitrogen or argon gas is applied to the targeted area, causing the tissue to freeze and eventually die. This minimally invasive technique is commonly used in dermatology and oncology for various conditions.
Electrodessication is a medical procedure that uses an electric current to destroy tissue, often used to remove skin lesions or tumors. The electric current heats the tissue, causing it to dry out and eventually fall off. This method is commonly used in dermatology for the treatment of various skin conditions.
Radiation therapy is a cancer treatment that uses high-energy radiation to shrink tumors and kill cancer cells. It can be used alone or in combination with other treatments like surgery and chemotherapy. The goal of radiation therapy is to destroy cancer cells while minimizing damage to surrounding healthy tissue.
Chemotherapy is a cancer treatment that uses drugs to kill cancer cells. It can be given orally or intravenously and works by targeting rapidly dividing cells, which includes cancer cells. Chemotherapy can be used alone or in combination with other treatments like surgery or radiation therapy to help shrink tumors, prevent cancer from spreading, or relieve symptoms. It can have side effects such as hair loss, nausea, and fatigue, but these are usually temporary.
Breast Cancer
Risk factors: female, >50 old, first degree relatives who had breast cancer, radiation treatment, early menarche, late menopause, obesity, no children, treatment with estrogen
S/S: painless fixed or movable mass, bloody discharge from nipple, skin dimpling, nipple retraction, size difference MRI (in situ)
Genetic mutations: BRCA 1 and BRCA 2
Diagnosis- mammogram, biopsy, breast exam,
Treatment: surgery, sentinel node mapping, chemotherapy, hormone therapy, immunotherapy, cancer vaccines, early intervention 99%-mammogram and breast self exam
tamoxifen-blocks estrogen receptors on the cell--s/s menopausal symptoms: hot flashes, bone density, vaginal bleeding
vaccines that work for HER 2’
Surgery
Lumpectomy (Breast-Conserving Surgery):
A lumpectomy involves removing the cancerous tumor along with a margin of surrounding healthy breast tissue. The goal is to preserve as much of the breast as possible while ensuring complete removal of the cancer. Lumpectomy is typically performed for early-stage breast cancer when the tumor is small and localized.
Mastectomy:
Mastectomy involves the surgical removal of the entire breast. There are several types of mastectomy, including:
Total (Simple) Mastectomy: Removal of the entire breast tissue, including the nipple and areola.
Modified Radical Mastectomy: Removal of the entire breast tissue, including the nipple and areola, as well as the axillary lymph nodes.
Radical Mastectomy: Rarely performed today, radical mastectomy involves removal of the entire breast tissue, including the chest muscles under the breast, as well as the axillary lymph nodes.
Skin-Sparing Mastectomy: Removal of the breast tissue while preserving the breast skin, nipple, and areola. This allows for breast reconstruction with a more natural appearance.
Nipple-Sparing Mastectomy: Removal of the breast tissue while preserving the breast skin, nipple, and areola. This procedure is suitable for selected patients with small tumors and no involvement of the nipple-areolar complex.
Sentinel Lymph Node Biopsy:
Sentinel lymph node biopsy involves removing one or a few sentinel lymph nodes, which are the first lymph nodes to which cancer cells are likely to spread from the primary tumor. This procedure helps determine whether cancer has spread to the lymph nodes and helps guide further treatment decisions.
Axillary Lymph Node Dissection:
Axillary lymph node dissection involves removing a greater number of lymph nodes from the armpit (axilla) to assess the extent of lymph node involvement and to reduce the risk of cancer recurrence. This procedure is typically performed if sentinel lymph node biopsy indicates lymph node involvement or if there is a high risk of lymph node metastasis.
Breast Reconstruction:
Breast reconstruction may be performed at the time of mastectomy or as a separate procedure after mastectomy to restore the breast's shape, size, and appearance. Reconstruction can be achieved using various techniques, including implants, autologous tissue (flap) reconstruction, or a combination of both.
Nursing Care
Emotional support
Education
Wound care
Metastases
Lymph nodes -first place to go two
Skeletal-very common to go to next-fractures-physical weakness,bone aches, calcium breaks down from boness- check electroyle scale for high ca
Pulmonary
Brain
Adrenals
Liver
Lung Cancer
Leading cause of cancer death in US for men and women
Four types-type of cells (Box 21-6) Small cell lung cancer,
Non-Small Cell Lung Cancer (NSCLC):
Adenocarcinoma: This type of lung cancer originates in the cells lining the air sacs (alveoli) of the lungs. It is the most common type of lung cancer, especially in non-smokers and women.
Squamous Cell Carcinoma: Squamous cell carcinoma arises in the thin, flat cells that line the passages of the respiratory tract. It often develops in the central airways of the lungs and is strongly associated with smoking.
Large Cell Carcinoma: Large cell carcinoma is a less common type of NSCLC that can occur in any part of the lung. It tends to grow and spread quickly.
Small Cell Lung Cancer (SCLC):
Small Cell Carcinoma: Small cell lung cancer is characterized by small, round cells that grow rapidly and tend to spread early to other parts of the body. It is strongly associated with smoking and comprises a smaller proportion of lung cancer cases compared to NSCLC.
Risk factors: tobacco smoke, secondhand smoke, irritants S/S: persistent cough, repeated infections, thick sputum, dyspnea, wheezing; later- weight loss, anemia, chest pain
Complications- head and neck edema, pericardial effusion, metastasis to lymph nodes, liver, brain, bones
Diagnosis: Chest x-ray, sputum analysis, bronchoscopy, CT, bone scan
Treatment- TNM staging, radiation, chemotherapy targeted therapy, surgery
Bladder Cancer
Most common in the urinary system, men > women Risk factors: tobacco, environmental carcinogens, bladder infections, family history, pelvic chemo or radiation
S/S: painless hematuria, UTI symptoms, later- urinary retention or frequency, pelvic or lower back pain
Diagnosis: Blue light fluorescence cystoscopy + biopsy, retrograde pyelogram, CT scan, MRI, bone scan
Outline: Surgery for Bladder Cancer
Clinical Stage Determines Surgery
Partial or Segmental Cystectomy
Small, confined tumors
Radical Cystectomy
Tumor penetrated muscle wall
Surgical Procedures
Partial Cystectomy
Removal of part of the bladder
Radical Cystectomy
Total removal of the bladder
Urinary Diversion
Redirecting urine to another collecting system
Radical Cystectomy in Women
Removal of various organs
Bladder, ureters, uterus, fallopian tubes, ovaries, vaginal wall, urethra
Radical Cystectomy in Men
Removal of various organs
Bladder, ureters, prostate, seminal vesicles
Urinary Diversion Techniques
Incontinent Urinary Diversions
External ostomy bags
Continent Urinary Diversions
Reservoir within the body, catheterized drainage
Neobladder (Continent Orthotopic Bladder Substitution)
Intestine reservoir connected to ureters and urethra
Management of Urinary Diversion
Incontinent Diversions
Constant urine flow, external pouch
Continent Diversions
Periodic catheterization, no external pouch
Neobladder
Normal urination, possible incontinence, occasional catheter use
Bladder surgery
Obtain complete medical, drug, and allergy history
Evaluate general physical and emotional status, vital signs, and weight
Address emotional responses and provide support
Discuss stoma care and self-catheterization
Explain preoperative preparations and postoperative care
Preoperative Preparations
Insertion of nasogastric tube, IV lines, and enemas
Administer cleansing enemas and antibiotics for specific procedures
Discuss insurance coverage for ostomy supplies
Educate client and family on surgery preparations and management
Postoperative Care
Monitor for complications and manage standard postoperative care
Observe for leakage, maintain renal function, and assess for peritonitis
Ensure integrity of urinary diversion and collection devices
Monitor skin and stomal integrity, promote positive body image, and provide education on diversion management
Specific Procedures
Ileal Conduit: Monitor stoma, manage leakage, and protect skin
Continent Urinary Diversion: Inspect stoma, teach self-catheterization
Ureterosigmoidostomy: Monitor drainage, prevent skin breakdown, and manage fluid/electrolyte imbalances
Trauma to Urinary Tract
Types of injuries: gunshot wounds, crushing injuries, forceful blows
Pathophysiology: tears, hemorrhage, penetration of urinary tract parts
Severity of injuries: blood and urine leakage, peritoneal cavity involvement
Treatment of Bladder Cancer
General Overview
Treatment varies based on grade and stage of tumor
Metastases usually absent if tumor hasn't penetrated muscle wall
Surgical Interventions
Small, superficial tumors removed by resection or fulguration with TURBT
High recurrence rate, necessitating cystoscopic exams every 2-3 months
Clients with no recurrence for 1 year need exams every 6 months for life
Topical Drug Therapy
Antineoplastic drug applied topically post-TURBT via intravesicular injection
Limited fluid intake to concentrate drug in bladder for 2 hours, followed by increased oral fluids
Other Drug Therapies
Bacillus Calmette-Guérin (BCG) Live and interferon alfa-2a used for inflammatory reactions and immune stimulation
Mitomycin, valrubicin, docetaxel, thiotepa, and gemcitabine for chemotherapeutic effects
Electromotive mitomycin therapy for improved effects of mitomycin
Photodynamic Therapy
Experimental treatment involving IV photosensitizing agent and laser activation to destroy malignant cells
Radiation Therapy
Used for clients not undergoing full bladder removal to eradicate remaining cancer cells
Side effects include alopecia, skin reactions, nausea, fatigue, and bone marrow depression.
Safety measures like limiting time, increasing distance, and using shielding are crucial.
Treatment: Surgery:
Curative Surgery: This type of surgery aims to remove the cancerous tumor or tumors from the body with the intention of curing the disease. Curative surgery is often performed when the cancer is localized and has not spread to other parts of the body. The goal is to completely eliminate the cancer and achieve long-term remission or cure.
Prophylactic Surgery: Prophylactic surgery is performed to reduce the risk of developing cancer in individuals who are at high risk due to genetic predisposition, family history, or the presence of precancerous conditions. This preventive measure involves removing tissues or organs that have a high likelihood of developing cancer in the future. For example, prophylactic mastectomy may be recommended for individuals with a strong family history of breast cancer or a known genetic mutation (such as BRCA1 or BRCA2).
Palliative Surgery: Palliative surgery is aimed at relieving symptoms, improving quality of life, and enhancing comfort for patients with advanced or metastatic cancer. The goal is not to cure the disease but to alleviate pain, discomfort, or complications caused by the cancer. Palliative surgery may involve removing tumors that are causing obstruction, relieving pain through nerve block procedures, or addressing other issues such as bleeding or fluid buildup.
Reconstructive Surgery: Reconstructive surgery is performed to restore the appearance and function of the body part affected by cancer surgery or other treatments. This type of surgery may be necessary after the removal of tumors or organs to improve physical appearance, preserve body function, and enhance overall well-being. Reconstructive surgery can be an integral part of the treatment plan for certain cancers, such as breast cancer, where breast reconstruction may be performed following mastectomy.
Postoperative Period
Clients undergoing urinary diversion are subject to the same conditions and complications as any surgical client. Refer to Chapter 14 for nursing diagnoses and interventions for managing standard postoperative care. Management issues related specifically to urinary diversion procedures include observing for leakage of urine or stool from the anastomosis, maintaining renal function, assessing for signs and symptoms of peritonitis, maintaining integrity of the urinary diversion and urine collection devices, maintaining skin and stomal integrity, promoting a positive body image, and teaching the client how to manage the diversion.
The nurse checks the client’s chart for information regarding the type and extent of surgery and orders for connection of catheters or drains, IV fluids, and analgesics. Clients will have multiple drainage tubes, ureteral stents, and a nasogastric tube. All urinary drainage tubes must be labeled, and the urine output from each catheter or stoma must be measured and recorded hourly.
Maintaining accurate intake and output measurements during the postoperative period is important because it indicates both renal function and the integrity of the urinary diversion structures. Obstruction of urine flow can severely damage the kidneys. If urinary drainage stops or decreases to less than 30 mL/hour, or if the client complains of back pain, the nurse needs to notify the primary provider immediately. Inspection of the urine includes checking for color, clarity, and presence of blood. It is essential to immediately report concentrated, cloudy, or bloody urine to the primary provider. Ureteral stents remain in place for several days after surgery.
The nasogastric tube is connected to low intermittent suction. This prevents distention and pressure on the suture line owing to the collection of gas in the bowel. The nasogastric tube is removed once peristalsis has returned and the diet can be advanced. All laboratory reports are reviewed as soon as they are received and abnormalities reported to the primary provider promptly. The following sections address management issues specific to the most common procedures.
Ileal Conduit
A transparent ostomy bag is applied over the stoma to make stomal assessment easier. The nurse contacts the primary provider immediately if there is excessive bleeding, changes in the color of the stoma (e.g., from a normal to a cyanotic color), or separation of the stoma edges from the surrounding skin. The nurse uses gauze pads to clean mucus away from the stoma. Because the intestinal anastomosis can leak fecal material or the ileal conduit may leak urine into the peritoneal cavity, they observe for and promptly report symptoms of peritonitis (e.g., abdominal tenderness or distention, fever, severe pain). Management of the urinary stoma is similar to management of a fecal stoma (see Chapter 48). The skin needs protection, the surgical dressings must be changed promptly when they become wet, and the appliances need care and cleansing. Each time they change a temporary drainage bag, the nurse inspects the skin around the stoma for signs of infection and skin breakdown.
Continent Urinary Diversion (Kock Pouch, Indiana Pouch)
The nurse inspects the stoma for bleeding or cyanosis. They may irrigate the pouch, if ordered, to prevent mucous plugs or blood clots. The nurse teaches the client how to perform intermittent self-catheterization. Initially, this is done every 1 to 2 hours but eventually will be performed every 4 to 6 hours.
Ureterosigmoidostomy.
A catheter is inserted in the rectum to drain urine continuously. The nurse checks the amount and color of drainage from the rectal catheter every 1 or 2 hours and inspects the anal and gluteal areas for signs of early skin breakdown. The catheter is removed when peristalsis returns. Because the sigmoid colon reabsorbs urinary constituents, clients are prone to fluid and electrolyte imbalances throughout the postoperative period (as well as for the rest of their lives). Observation for signs of electrolyte losses is essential. The nurse teaches the client exercises to improve sphincter control. Once good control is achieved, the nurse instructs the client to void (rectally) every 2 hours to prevent reabsorption of fluid and electrolytes. Clients must never have enemas, suppositories, or laxatives.
Pathophysiology and Etiology
Various types of injury can affect the urinary tract. Gunshot and stab wounds, crushing injuries, and forceful blows can result in tears, hemorrhage, or penetration of one or more parts. Some penetrating bladder injuries are small, whereas others are large, with a rapid collection of urine in the peritoneal cavity. Injuries to the kidney area may result in bruising or tearing of the kidney and its capsule. Depending on the severity of the injury, blood and urine may leak into the peritoneal cavity.
Radiation therapy
also known as radiotherapy, is a common treatment for cancer that uses high-energy radiation to target and destroy cancer cells. It can be delivered externally using a machine (external beam radiation therapy) or internally through radioactive materials placed directly into or near the tumor (brachytherapy).
Radiation therapy works by damaging the DNA of cancer cells, which prevents them from growing and dividing. Healthy cells can also be affected by radiation, but they are usually better able to repair themselves than cancer cells. Radiation therapy is carefully planned to minimize damage to healthy tissues surrounding the tumor while effectively targeting cancer cells.
There are several types of radiation therapy, including:
External Beam Radiation Therapy (EBRT): This is the most common type of radiation therapy, where radiation is delivered from outside the body using a machine called a linear accelerator. The radiation is precisely targeted at the tumor from different angles to maximize its effectiveness while minimizing damage to surrounding healthy tissues.
Intensity-Modulated Radiation Therapy (IMRT): IMRT is a type of external beam radiation therapy that uses computer-controlled linear accelerators to deliver precise radiation doses to a tumor or specific areas within the tumor. It allows for the modulation of the intensity of the radiation beams, which can help spare nearby healthy tissues and organs.
Stereotactic Body Radiation Therapy (SBRT): SBRT delivers high doses of radiation to small tumors in a few sessions, typically over one to five days. It is often used for tumors that are difficult to treat surgically or in areas where surgery is not feasible.
Brachytherapy: In brachytherapy, radioactive sources are placed directly inside or next to the tumor. This allows for a high dose of radiation to be delivered precisely to the tumor while minimizing radiation exposure to surrounding healthy tissues. Brachytherapy is commonly used for prostate cancer, cervical cancer, and certain types of skin cancer.
Radiation Side Effects
Alopecia
Skin reactions
Stomatitis, xerostomia
Nausea, vomiting, anorexia, diarrhea
Cystitis
Fatigue
Bone marrow depression
Radiation safety in hospitals
Regulatory Compliance: Hospitals must adhere to regulatory standards and guidelines established by governmental and professional organizations, such as the Nuclear Regulatory Commission (NRC) or the International Atomic Energy Agency (IAEA). These regulations govern the safe use of radiation in medical facilities and set requirements for training, equipment, and quality assurance.
Training and Education: Healthcare professionals who work with radiation, including radiologists, radiation oncologists, radiologic technologists, and nurses, receive comprehensive training on radiation safety and protocols. Training covers topics such as radiation physics, radiation protection principles, proper use of equipment, patient positioning, and radiation dose optimization.
Quality Assurance: Hospitals implement quality assurance programs to ensure that medical imaging equipment, such as X-ray machines, CT scanners, and fluoroscopy units, operate safely and accurately. Regular equipment maintenance, calibration, and performance testing are conducted to maintain image quality while minimizing radiation dose.
Patient Dose Optimization: Healthcare providers employ techniques to optimize radiation doses for patients while maintaining diagnostic image quality. This includes the use of appropriate imaging protocols, dose reduction techniques (e.g., dose modulation, iterative reconstruction), and the ALARA (As Low As Reasonably Achievable) principle to minimize unnecessary radiation exposure.
Personal Protective Equipment (PPE): Healthcare workers who perform or assist with radiological procedures wear appropriate PPE, such as lead aprons, thyroid shields, and leaded eyewear, to reduce radiation exposure. PPE usage is essential for protecting staff members from scatter radiation during procedures.
Radiation Shielding: Hospital facilities are designed with radiation shielding measures to minimize radiation exposure to personnel and the public. This includes lead-lined walls, doors, and windows in radiology and radiation therapy areas, as well as leaded glass barriers and control panels.
Patient and Public Safety: Hospitals implement measures to ensure the safety of patients and visitors in areas where radiation is used. This includes posting radiation safety signage, restricting access to radiological areas, and providing patient education on radiation risks and safety measures.
Emergency Preparedness: Hospitals have emergency response plans in place to address incidents or accidents involving radiation. These plans outline procedures for managing radiation emergencies, evacuating affected areas, and providing medical care to individuals exposed to radiation
Chemotherapy
Action = Cytotoxic
Routes of administration
• Oral
• Intravenous -> extravasation
Treatment of Extravasation
General Measures
Stop administration of drug.
Leave needle in place.
Gently aspirate residual drug and blood into tubing or needle.
Inject neutralizing solution such as sodium thiosulfate, hyaluronidase, or sodium bicarbonate to reduce tissue damage. Selection of neutralizing agent depends on vesicant.
Vesicant-Specific Measures
Doxorubicin
Elevate and rest extremity.
Apply topical cooling for 24 hours.
Give hydrocortisone as ordered.
Nitrogen mustard
Apply cold compresses.
Administer thiosulfate as ordered.
Vinca alkaloids (vinblastine, vincristine, vindesine)
Apply warm compresses.
Do not apply ice—increases skin toxicity.
Administer hyaluronidase as ordered.
Mitomycin
Apply ice.
Administer dimethyl sulfoxide (DMSO) as ordered.
Intramuscular, subcutaneous
Topical, cavity
combination chemotherapy
Chemotherapy Side Effects
Bone marrow depression at nadir
Neutropenia ‘
Leukopenia
Thrombocytopenia
Anemia
Nausea and vomiting
Stomatitis, mouth sores
Alopecia
Managing Clients Receiving Chemotherapy
Monitor client for symptoms of anaphylactic reaction: urticaria (hives), pruritus (itching), sensation of lump in throat, shortness of breath, wheezing.
Assess for electrolyte imbalances
Prevent extravasation of vesicant drugs. Implement measures to treat extravasation of vesicant medications if it occurs (see Box 18-7).
Assess for signs of bone marrow depression: decreased white and red blood cell, granulocyte, and platelet counts.
Assess for signs of bleeding and infection.
Monitor for signs of renal insufficiency:
Elevated urine specific gravity
Abnormal electrolyte values
Insufficient urine output (<30 mL/hour)
Elevated blood pressure, blood urea nitrogen (BUN), and serum creatinine
Inform client about the reasons for nausea and vomiting.
Administer antiemetics before and during administration of chemotherapy or as indicated.
Assess oral mucosa for dryness, redness, swelling, lesions, ulcerations, viscous (sticky) saliva, or white patches.
Other Treatments
Stem cell transplant
Targeted therapies
Hyperthermia
Photodynamic therapy
Gene therapy
Clinical trials
Complementary and alternative therapies
Nursing Care
Assessment:
Understanding of the situation
Coping mechanisms being used
Energy levels
Nutrition status
Support:
Psychological support
Grief counseling
Addressing body image concerns
Providing care for the family
Interventions:
Managing pain
Preventing infections
Addressing fatigue
Controlling bleeding
Maintaining skin integrity
Meeting nutritional needs
Hospice Care
Characteristics:
Prognosis of less than 6 months
Can be provided in inpatient or outpatient settings
Involves an interdisciplinary team
Focuses on supporting both the patient and family/caregivers
Comparison with Palliative Care:
Hospice care is typically for patients with a prognosis of less than 6 months, while palliative care can be provided at any stage of illness
Palliative care focuses on improving quality of life for patients with serious illnesses, while hospice care is specifically for end-of-life care.