Discussion questions 3
Definitions
What are social networks and how are they linked to health outcomes?
Social networks: the number of contacts and the frequency of those contacts (based on the amount of interaction)
→ Their size and density influence the information, resources, and access to opportunities available
→ They affect people’s behaviours, including health behaviours
Links to health outcomes:
The richer your social network, the better your physical and mental health because it improves you life (you have access to more resources and more control over your life prospects)
Social networks discipline members into adhering to norms, beliefs, and values, which can be potentially health enhancing
Certain characteristics of social networks affect the prevalence of obesity (ex: social distance → being close to obese people = more likely to develop obesity) *Christakis & Fowler
What is social cohesion and how is it linked to health outcomes?
Social cohesion: includes participation in community affairs, the number of community-based organizations, the level of interpersonal trust, and crime statistics in a society
Links to health outcomes:
High social cohesion improves life expectancy and reduces disease incidence
What is social capital and how is it linked to health outcomes?
Social capital: type of social cohesion concerned with features of social structures (levels of interpersonal trust, norms of reciprocity and mutual aid…) that act as resources for individuals and facilitate collective action
Links to health outcomes:
Higher social capital leads to lower all-cause mortality
What is social exclusion and how is it linked to health outcomes?
Social exclusion: includes economic hardships and marginalization of racialized/minority groups
Links to health outcomes:
There are big health gaps between dominant groups and racialized/minority groups in populations
Visible minorities have more negative health outcomes
Example: healthy migrant effect (before they immigrate they are healthy, after the immigrate and the longer they stay in the new country their health deteriorates)
Homeless people have worse health outcomes *Luscombe
What is social support and how can it improve health outcomes?
Social support: qualitative aspect of support including emotional, informational, and material support
3 mechanisms through which social support improves health:
Mediated relationship | Confounded relationship | Independent relationship |
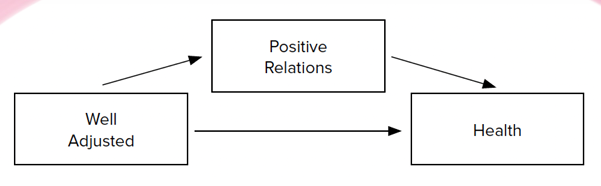 | 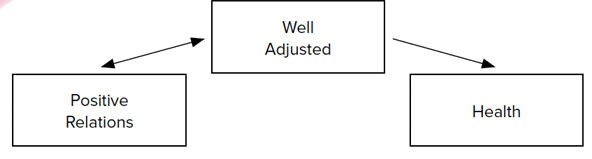 | 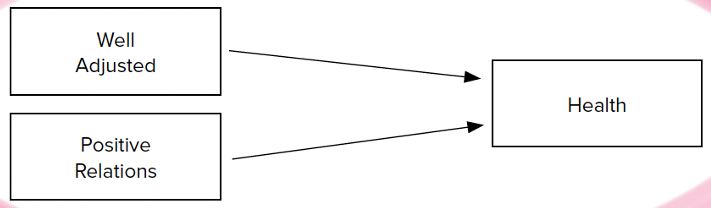 |
Being well-adjusted → building positive relationships with others Being well-adjusted + positive relationships with others → healthy living | Being well-adjusted → easier to build positive relationships with others Being well-adjusted → better mental and physical health | Being well-adjusted → better health Having positive relationships with others → better health |
What is the sense of community belonging and how is it linked to health outcomes?
Community-belonging: the degree to which an someone is or perceives to be connected to their community
Community belonging is strongly related to community-level capacity for healthy behavioural change through:
Exposure to health-related behaviour norms and attitudes in the community
Psychosocial mechanisms like self-esteem, social status, and social control
Access to material and other types of community resources
What are the buffering effects of gender roles on health?
Buffering effects: women are less susceptible to socio-economic impacts on health than men
May be because of their gender roles within families and communities
What is the morbidity paradox?
Morbidity paradox: women report poorer health but live longer lives than men
What is the feminization of aging?
Feminization of aging: because women live longer than men, they make up a disproportionately large share of the older population, particularly in advanced age groups
What are the differences between the differential exposure hypothesis and the differential vulnerability hypothesis?
Differential exposure hypothesis | Differential vulnerability hypothesis |
Women have more health problems because:
| Women have more health problems because they react differently than men to the material, behavioural, and psychosocial conditions that affect health |
Critical thinking questions
We now know that our membership in social networks has a major impact on our health-related beliefs, values, and behaviour. How might this discovery be used to address some of the big issues currently confronting health promotion, notably obesity and low levels of physical activity?
Canada and Australia have aimed at creating multicultural societies, whereas the US and France have pursued policies of assimilation. How might the different policy approaches to ethnic and racial diversity affect the health of the relevant populations?
Some studies show that older women in Canada report worse self-reported health, greater distress, more perceived pain and lower levels of happiness than older men. What accounts for the difference?
Due to the feminization of aging → they make up a disproportionately large share of the older population, particularly in advanced age groupsGender inequalities in income and rates of paid-unpaid work + having children → reduces women’s access to material resources and the psychosocial benefits of paid work → has negative impacts on their health and well-being
“Body image is a subjective experience of appearance. It’s an accumulation of a lifetime’s associations, neuroses and desires, projected on to our upper arms, our thighs. At five, children begin to understand other people’s judgement of them. At seven they’re beginning to show body dissatisfaction. As adults 90% of British women feel body-image anxiety. . . . Many young women say they are too self-aware to exercise; many say they drink to feel comfortable with the way they look; 50% of girls smoke to suppress their appetite . . .” (Eva Wiseman. Uncomfortable in our skin: the body image report, The Guardian, Sunday 10 June 2012) Is socially-driven anxiety harming girls and women?