Language Disorders
Communication Development: An Introductory Review
Most childhood language disorder or delay do not have a know cause
Sender and a receiver that are using some form of shared system
When there is no shared system there is a communication breakdown.
There can be multiple shared systems in one convo, like speaking and texting.
Communication: Sharing information between 2 or more people.
Language: symbolic communication; spoken, written, signed words. A code that stands for something else.
Acquired: someone develops a language disorder sometime after birth, they already have had a system established.
Developmental: one has had a language disorder since birth.
Speech: Sounds that produce words; spoken language.
Needs a symbolic and code-based system along with the respiratory system, phonatory, articulatory, and resonance to produce spoken language.
Stages of Communication
0 to 7 months → Preintenional: actions are treated as communication without the child purposely using the action to communicate. The communication is based on a biological response. This state is a response to the state of your body. You do not think you are trying to communicate a message, but that message still communicates some type of message.
Parents however assign communication intentionality to the unintentional message.
Infant learns that most of the time when they cry they get their needs met or attention.
7 months → Pre-symbolic Intentional: purposeful communication without the use of language, including eye contact, gestures, and vocalizations “prelinguistic”. This means before language but is intentional.
This can also include gestures and vocalization.
There is a grey line between pre-intentional and pre-symbolic intentional.
12 months → Symbolic Intentional: purposeful communication using language, including words while still using pre-symbolic forms. Now infants are also using symbols, word approximation, or words. However non-symbolic communication is still being used.
Comprehension: (understanding) Receptive language.
Both can be either written or spoken or signed, etc.
Comprehension both proceeds and exceeds production. To be able to meaningful express a word you need to be able to understand it first.
Production: (expressing) Expressive language.
Domains of Communication
Form: the behaviors used to communicate
These include written and spoken, and how individual sounds and words are produced.
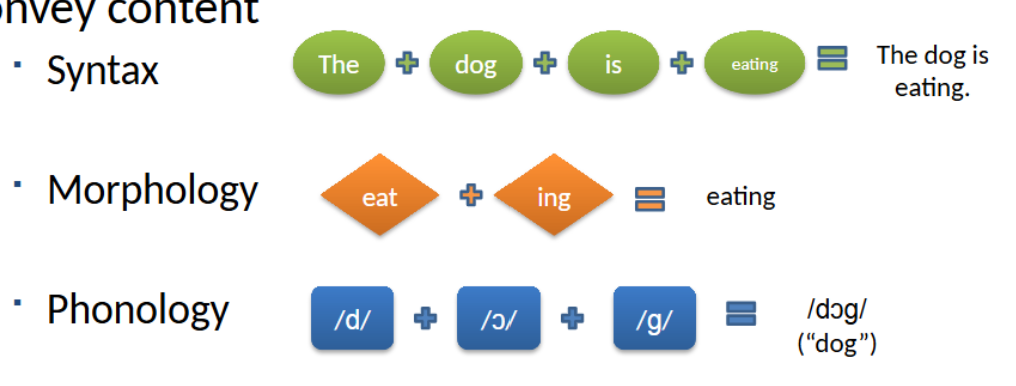
How gestures, sounds, words, and sentences are organized and arranged to convey content.
1) Syntax: how words are organized. Increase in utterance length, sentence modalities, and complex syntax.
2) Morphology: The smallest units that carry meaning.
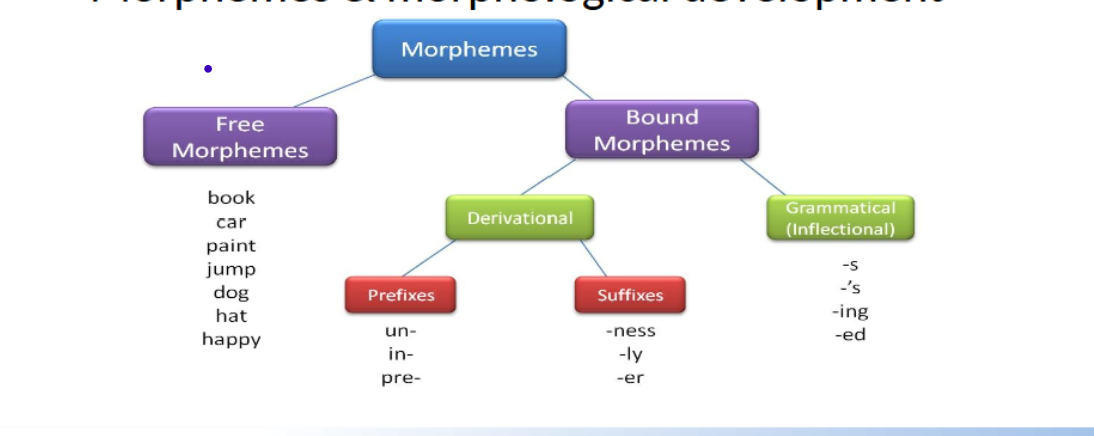
Morphosyntax: grammar
3) Phonology: sound structure of syllables and words (phonemes). Phonological development.
Speech segmentation: being able to understand and hear each individual sound in a word.
Phonemic inventory: the sounds you understand and can produce
Content: The meaning of what is communicated, the message we are trying to get across.
4) Semantics: the meaning of words, lexicon, and the mental dictionary or mental vocabulary.
Acquiring a receptive and expressive lexicon.
Word learning opportunities.
Organizing lexicon for word retrieval.
Use: the reason or function for communicating
5) Pragmatics: function, reason, or meaning for why you are communicating. What is the purpose, what are the needs and wants? The function of communication; is how personal and social needs are met.
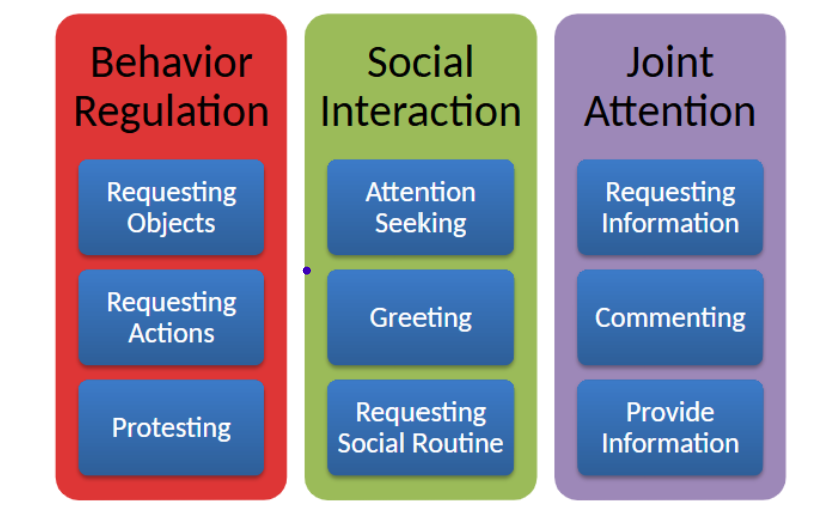
We need to be able to communicate for a variety of functions.
Pragmatics also involves turn-taking and conversation.
Reciprocal is a big part of communication as well.
Pragmatics is social context-dependent, relational, and situationally dependent.
How and why do children learn language?
Nature and nurture: knowledge that is innate or predetermined, which then further knowledge is gained through experience.
Kids learn best in the context of everyday activities, especially the early language development.
10-14 months is when kids say their first words
First words need to be a close approximation to adult form and similar pronunciation. Is not imitation they can do it on their own, and the word is generalized
At 2 years of age they use two word combinations this usually is when they have 50 words in their vocabulary
Assessments
Assessment: systematic process of gathering information about an individual’s background history, skills, knowledge, perceptions, and feelings.
May be multidisciplinary
Testing is only part of assessment
Need to develop a good communication profile with strengths and weaknesses.
Purpose:
(1) Identifying skills in a particular area of communication that a person has or lacks
(2) To guide the design of interventions to enhance a person’s skills in a particular area of communication
(3) To monitor a person’s communicative growth and performance over time
(4) To qualify a person for special services
Application:
(1) To determine whether a person’s performance indicates the presence of a disorder
(2) To identify specific short- and long-term goals and specific learning targets to identify strategies and contexts for addressing these goals
(3) To determine progress made as a result of interventions, to assess whether specific outcomes have been reached, and to monitor progress after discharge
(4) To determine whether a person meets the eligibility requirements set by a particular program or institution for coverage of educational therapeutic services.
Scope and sequence of assessment:
(1) Screening and referral
(2) Designing and administering the assessment protocol
(3) Interpreting assessment findings
(4) Developing an intervention plan
(5) Monitoring progress and outcomes
Screening: Test or task to conduct a check or performance to determine the need for a full evaluation. This does not determine a diagnosis. Do not need screening to have a full evaluation.
Informal: parent noticing kid isn’t talking
Formal: SLPs or teachers doing official screening on developmental milestones
Screen for speech, voice, fluency, and language.
Referral: When a professional’s help is formally requested.
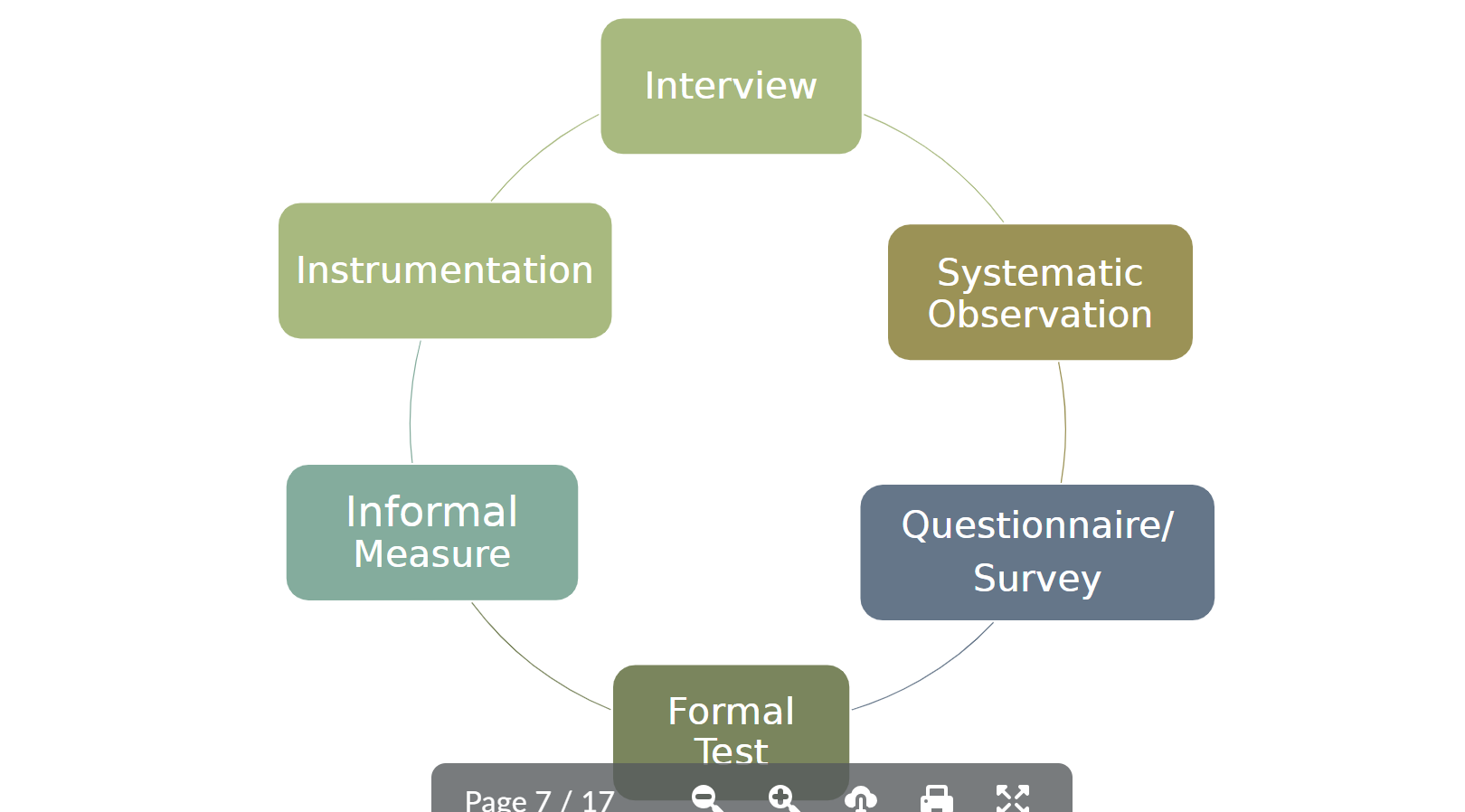
Interviews: w/ child, client or caregiver
Systematic Observation: how the patient behaves naturally on a daily basis
Informal measurements: gaining more necessary information that you might need.
Formal Tests:
Norm referenced: Used to compare performance with that of a same-age peer. Normed on a random sample of a specific developmental age.
Criterion-referenced: Used to determine level of achievement in a particular area. level of achievement.
Important Qualities of Norm-Referenced
no tests are perfect
Standardization: means it is administered and scored in a uniform and consistent manner. The test is given in the same way. There needs to be a set of criteria that is included.
ALL norm-referenced tests have to be standardized
ALL standardized tests are not norm-referenced
Normative Sample: the peers being used as the sample to compare the test takers’ scores to. Test developers use the normative sample data before making the test scores.
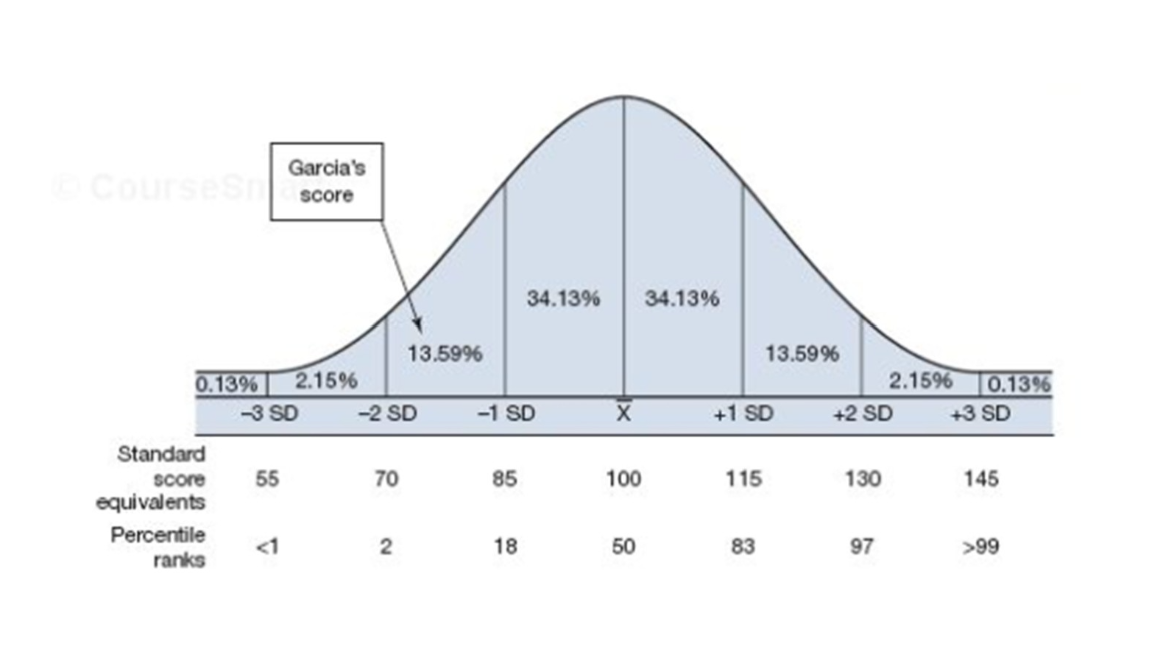
Standard Scores: based on principles of the normal curve and standard deviation.
1 sigma/standard deviation = 68% of the data falls within 1 standard deviation from the mean.
2 sigma/standard deviation = 95% of the data falls within 2 standard deviations from the mean
Diagnostic Accuracy: sensitive and specificity
See video - test characteristics: how accurate was that test?
How likely will this test return as a true positive or true negative
Increasing sensitivity decreases specificity
A bad disease you want to make it more sensitive and to decrease sensitivity for things like pregnancy.
Accommodations and Modifications
modifications: modifies test or the information given. In standardized tests you can’t use those scores or submit scores
accommodations: only if the person needs it, but it can used on normative tests, and the normative tests have scores for accommodations
On norm-referenced tests extended time is allowed or not
Time for example might be a determining factor for if someone has a disorder or not and this may allow them accommodations other places in life
Standard Normal Distribution
Derived from mathematical models of probability regarding how scores will range from a skill or aptitude that is assumed to be normally distributed within the population
Raw score: tells us whether the items are correct or incorrect, it is a simple counting of items. The raw score is how you derive the standard score and percentile rank. Raw scores don’t care about meaning and are not reported.
Normal Curve: what is typical or expected
Mean
Standard deviation
Percentile rank: same as or above x% of the population
Standardized norm tests typically have a mean of 100 and a standard deviation of 15
The two most important scores are percentile (rank) and standard score.
Criterion-referenced tests: can be compared to various things
Could be based on developmental milestones
Require the establishment of a clear standard performance
Require design of specific tasks
Must provide clear guidelines for interpretation
Difference - this test can be standardized, but it is not based on a norm from a set of peers. It can be standardized by administering the test and can do a standardized procedure to get a score, but the score is not standardized since there is no curve.
To find the developmental milestones, the same test wasn’t given, it was determined a different way, and then this test is created off of those milestones
Formal: someone has created it, and it can be officially bought, but it is still based on a developmental milestone
Informal: one that is made in the clinic by one SLP. These are done when your looking for more information in a specific area.
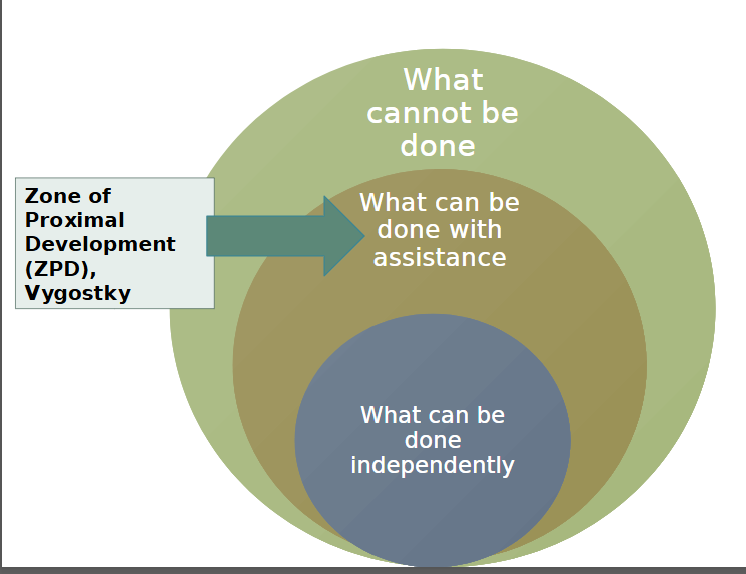
Dynamic assessment: looks at what they can do right now, and what their full potential can be
Analyzes how much and what types of support or assistance are needed to bring an individual’s communicative performance to a higher level
Want to make sure they don’t have a language disorder just because they haven’t been exposed to the information
A person might need additional exposure help but not LD help.
Test, teach, retest: this is the most common dynamic assessment and can be done in 15 minutes or more drawn out depending on the situation
What can the child do with assistance?
Then slowly decrease the support to move toward independence
Kids without a language disorder are going to learn new things within 10 minutes, but individuals with a LD aren’t going to pick it up as quickly
Interpreting Assessment Findings:
Diagnosis: differential diagnosis. Information needs to show up in more than one source. Find what type of language disorder. Having a particular disorder or not.
Determine the severity of the disorder: very mild, mild, moderate, severe, and very severe
Characterizing the client’s prognosis: improving, plateauing, or declining.
Developing an Intervention Plan:
Identify treatment goals: what you will be working on. Have goals in mind to know what to work for.
Describe the possible length and frequency of treatment
Describe treatment contexts and activities.
At the end of an assessment report write up a paragraph of recommendations with the things above.
Monitoring progress and Outcomes
Assessment doesn’t stop when the diagnosis is made
An ongoing process that monitors progress and outcomes for the client
Purpose: monitor a client’s progress during treatment, modify the treatment plan as progress is made, and determine when a client should be discharged from treatment.
Evidence-Based Practice
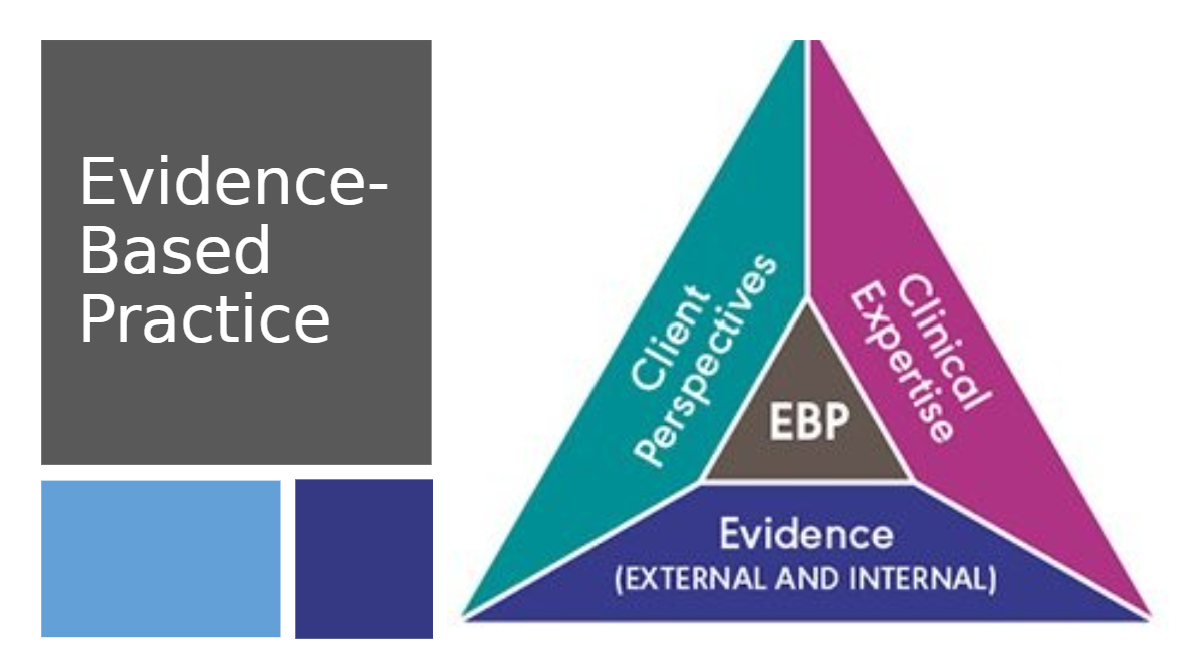
Evidence-Based Practice (EBP): Client perspectives, clinical expertise, and evidence (external and internal).
Very rarely is it an equilateral, typically imbalance in one area or the other.
It is a dynamic moving triangle.
We try something brand new and different if there is limited external evidence, or if the external information the client is not improving. Doing something new is still based on sound external evidence.
Fidelity: doing the intervention the way it was designed
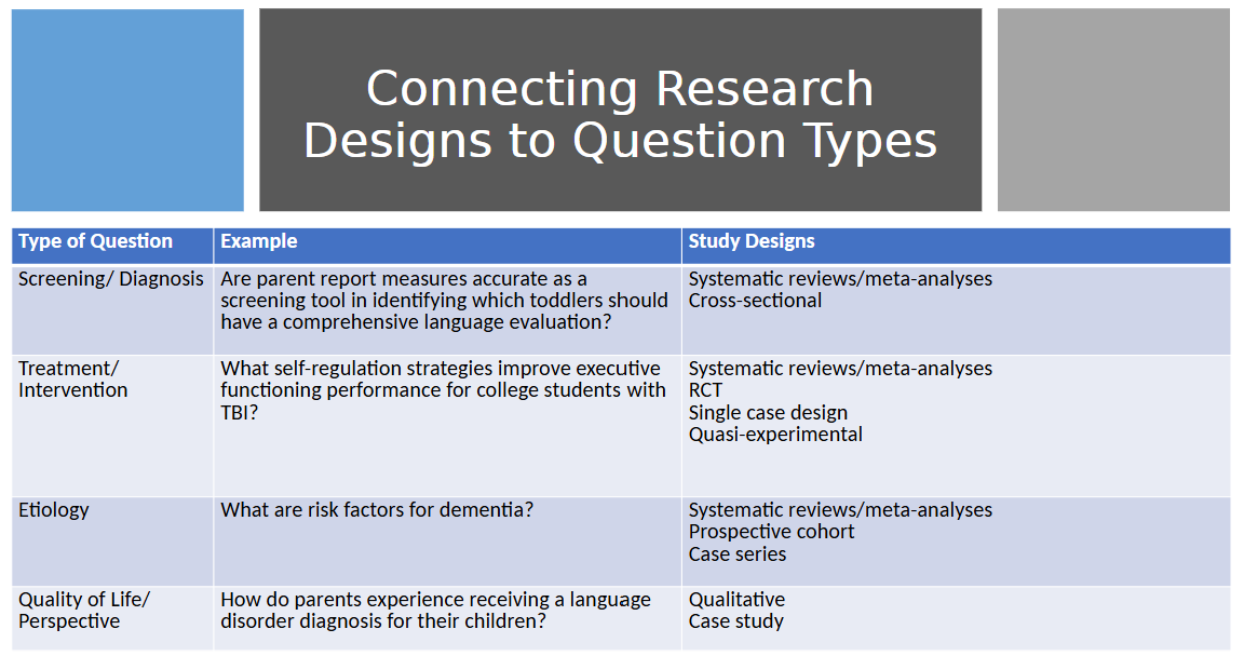
Types of clinical questions:
screening/diagnosis
Therapy/Intervention/Treatment
Etiology - what causes certain things
Quality of Life/Perspectives
PICO Question: help us guide what we are looking for in the reading
P: Population/People/Patient/Profile
I: Intervention/instruction
C: Comparison (can sometimes be left out)
O: Outcome
PICO Question Template: For this specific person (or this communication profile), will this intervention or this other possible comparison intervention, be more likely to result in this desired outcome?
Develop a list of “Search Terms”
Extract key words from your PICO Questions
Consider synonyms or related terms
Include relevant study designs (as applicable)
Create a search string by using AND OR
Ex. Children or Child and autism spectrum disorder or autisic
Ex. Traumatic brain injury or TBI or Concussion
Find Evidence
Library databases (ERIC, PubMed, PhsychInfo)
Google Scholar
ASHA Journals
Appraised or synthesized evidence:
ASHA Evidence Maps
The Cochrane Library
What Works Clearinghouse (US Dept of Ed)
Evaluate the Evidence
Treatment research question for clinical decision-making:
“Does the picture really show that people who got this treatment showed enough improvement, as compared with people who did not get this treatment, that I should adopt it as my approach?”
When choosing evidence in a clinical sense you can look directly at the results to see if it works or not
Combine the high-quality evidence with your expertise as a practitioner and with the client’s performance and values
Use of external evidence is “not a rigid prescription but a dynamic part of a client-centered approach”
All three components should be considered and integrated in making decisions
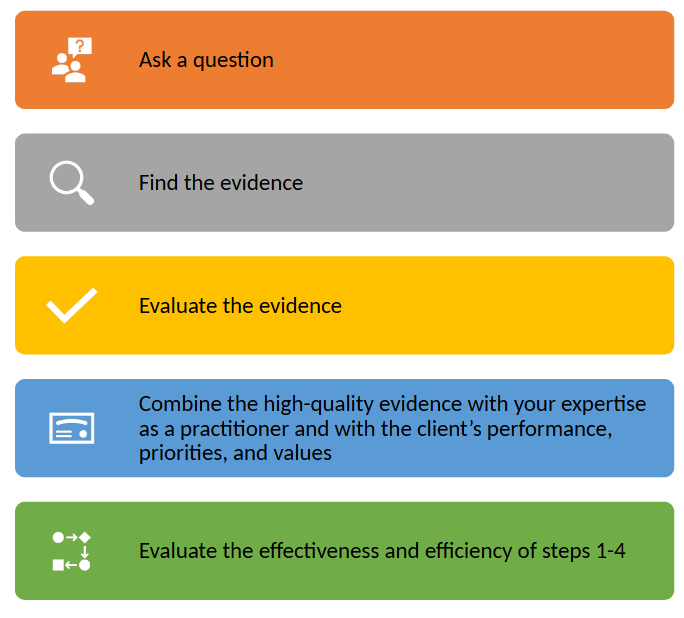
Evaluate the Effectiveness and Efficiency of Steps 1-4
Reflect on:
Did I ask a good question?
Find evidence efficiently?
Evaluate it correctly
Combine it well with my own knowledge and with client’s specific information
Evaluate:
Did I implement the intervention correctly and as well as I could? (fidelity)
What evidence do I have that my client improved? (progress monitoring)
Study Designs
Meta-analysis and systematic reviews: systematic summary of scientific literature
Experimental variable(s) altered/manipulated, controlled comparison
RCT: Single-case design (e.g., multiple baseline/multiple probe, alternating treatments)
Quasi-experimental: variable(s) altered/manipulated
Two group (nonrandomized) comparison
Non-experimental quantitative (or observational or descriptive): variables are measure but not altered/manipulated
Cross-sectional prospective, prospective cohort, case series
Qualitative: in-depth perspectives and/or experiences of individuals; variables are not altered/manipulated.
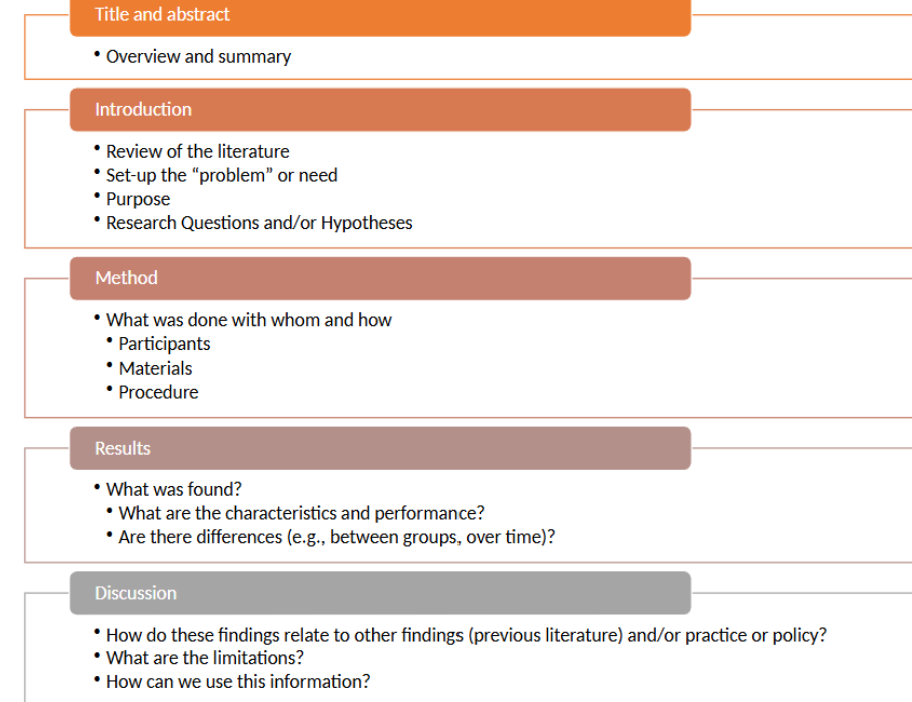
An Approach to Answering Treatment Questions from Research Articles
Review title and abstract
Purpose and research question(s)
Does the purpose address, contribute to, and/or align with your PICO question?
Participants (toward the beginning of method section)
Is there a sufficient match with client/population/profile?
Results: look for main table or graph (in results section)
Were there differences between groups (or between baseline and intervention)?
Did this intervention “work” (i.e. produce desired outcomes)?
Measurement (in the method section)
How did the researchers measure the outcomes?
How does the measurement represent the intended skills (validity)?
Intervention procedures (in method section)
What did they do (are detailed intervention procedures included and what are they)? Fidelity checklist?
What context did they conduct the intervention?
Principles of Intervention
treatment and intervention are interchangeable
intervening with communication needs that interfere with someone’s daily communication that they want to improve
Want to use the words in your head to communicate and be understood
Intervention: refers to the implementation of a plan of action to improve one or more aspects of an individual’s communicative abilities
it is systematic, it has a scope and sequence
Qualities: Effectiveness, Efficient, Feasible
It is based on performance and then where the treatment goes
Effective - things need to work
Look into assessment and see if it works
Start with external science and then check and see if it works for this person
Efficient - the least time-intensive that works. This could be a lot of time or not
Feasible - does it work for this particular person?
Purposes of Intervention: 3 primary purposes
Prevention - prevent a disorder or outcome of a disorder
Remediation - There is a know concern that we improve the trajectory on, we help increase their skills to meet their daily life needs. Altering the course of a disorder, improving, and building skills.
Compensatory - providing improved performance in certain areas. Using strategies to aid in a specific area, sometimes this can actually change how you do certain things. What are the things we can do to help the individual
Intervention Planing:
Goal setting: what are you working on with this individual, what is the target for this person, they let you know what you are working towards. The thing that we want to improve.
Procedure: The act of what you need to do to reach those goals. It is a systematic plan that aligns with goals.
Goal (behavioral objective) components
behavior - things that are measurable and observable. Behavior is the everyday things people do, talking, gesturing, storytelling, etc. If it is challenging call it challenging or interfering behavior. It won’t be understanding as something that is behavior because you can’t measure that
Condition - situation or context in which they are doing the behavior
Criteria - the way that the behavior is being measured and at what level
Ex. Jenning is running 2 times a week for 2 miles outside. Running is a behavior, the condition is outside, and the criteria is 2 times a week for 2 miles.
S - specific (specific enough that we know what the goals are)
M - measurable (way to know when we achieve it or to track our progress)
A - Attainable (is it possible for this person, is it something that is within reach for them)
R - Relevant (are there benefits for this person and is it important to them?)
T - Time-Based (when will this goal be done? When do we need to check back in on the goal)
Three Phases of Intervention Planning: Context, strategies, activities, and materials
Phase 1: Setting long-term client-centered goal(s), the anticipated outcomes of therapy (very broad)
Phase 2: Setting short-term goals that will lead to the desired long-term goals (maybe over a month, what are your checkpoints?)
Phase 3: Setting session-level goals that are written in measurable observable terms (goals that can be achieved in 1 session)
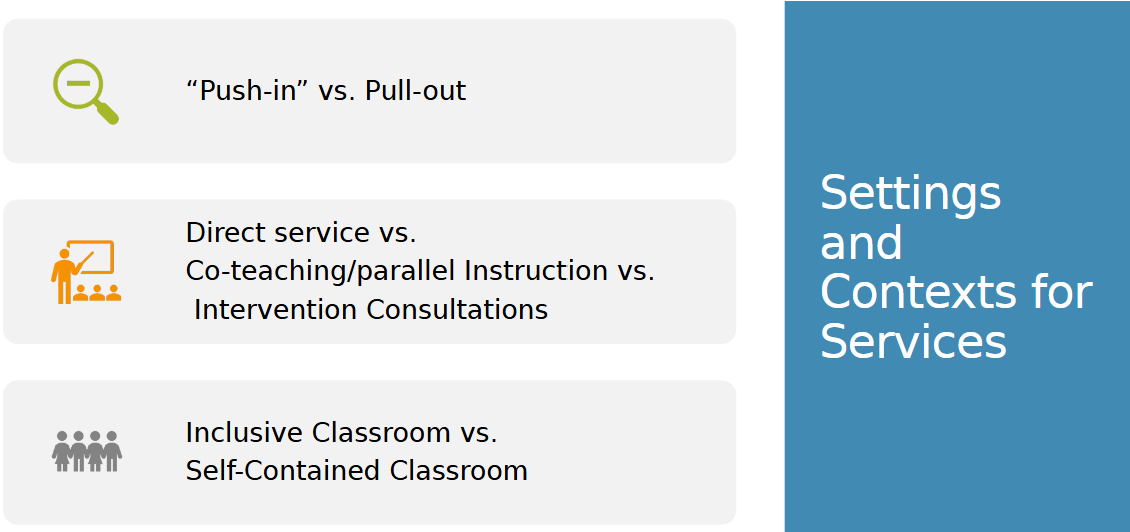
Direct service: I am directly providing intervention to you
Collaborative delivery: 2 or more people working together. more than one discipline working together. This could be co-teaching, etc.
Consultation: when you as the SLP are providing support for someone when you are not present with the client.
Acquisition: learning how to do the skill
Fluency: Learning to do the skill smoothly and at natural rates
Maintenance: Using the skill after instruction has stopped
Generalization: Applying the skill whenever and wherever it is needed
Instruction & Learning Process: Intruction/guidance, opportunities to practice, and then feedback.
Unit 2
Slide 1:
Overview of Child Language Disorders
Slide 2: Focus Questions
What is an LD?
How are they classified?
What are the prevalent types?
Slide 3: Intro
Indicators:
Kids who have delays in prelinguistic skills can be an indicator of a language delay, then intervention/prevention can be provided and help the kids provide
Kids are slower to meet milestones or there is something atypical about the way they acquire language
A delay is when kids are just acquiring language at a slower rate, but they are still doing it in order
You need to look at the whole picture
Future Impacts/Challenges
Current: can’t express needs or wants in the moment, which can cause frustration etc.
Future: it can impact academic skills, peer relationships, daily living and employment
THIS is why we need to intervene early to reduce the impact on their lives later
Slide 4: What is an LD?
Some Impaired comprehension and/or use of spoken, written, and/or other symbol system.
Can impact expressive or receptive language or both, often there is some impact on the other even if one is more obvious than the other
May impact: form (phonology, morphology, and syntax), content (semantics), and/or function (pragmatics)
Hit on what is most impactful for the person and the big picture
Slide 5: Common Signs - Preschool
Slide 6: Common Signs - Elementary
Slide 7: Common Sings - Adolescence
Slide 8: Considerations
Slide 9: Terminology
Slide 10: Prevalence and Incidence
Slide 11: Classification
Slide 12: Etiology
Slide 13: Manifestation
Slide 14: Severity
Slide 15: Types
Slide 16: Specific Lang. Impairment
Slide 17: Autism Spectrum Disorder
Slide 18: ID
Slide 19: TBI
Slide 20: Questions
Foundational Language Intervention Strategies for Early Communicators
Language disorder: if the characteristics affect the function of their life
The foundation for all language learning is responsive interactions
Teaches the child that their communication is important
And that their interests they are communicating are important
Supports engagement and builds secure relationships
Promotes reciprocal interactions: sender and receiver, the foundation for all conversations
The more a child communicates the more practice they get
Tune in, Talk More, Take Turns
Serve and return interactions (ping-pong match)
The child showed an interest and the adult responded in a supportive way
(1) Share the focus: notice when they are showing interest. Notice serves.
(2) Support and encourage: say a word of encouragement. Helping and playing with a child.
(3) Name it: name what they are seeing, saying, or doing. Build an understanding of the world and what to expect from it
(4) Take turns back and forth: waiting is crucial, give the child a chance to return the serve
(5) practice endings and beginnings: Watch when they are no longer interested and want to move on to something new. Allows the child to take the lead
Notice — RESPOND — Pause
Notice the child’s communication
Physically engage through imitation and/or “next step”
Verbally imitate and/or comment on the child’s focus of attention
Pause after your response
Notice: Leading by following — follow the child’s interest
Notice what the child is looking at
Notice what the child is reaching for
Notice what the child is doing
Notice what child is saying
Respond by talking about:
What the child is doing/looking at/reaching for
What the child is communicating
Language is most meaningful when it’s related to what child is doing or in response to what child communicating
Respond: imitating actions — helps child realize he has the power
The child draws a circle on the paper, you draw a circle in the same way
Child taps on a drum you…
The child pretends to eat play fruit while saying “mmm” you…
Respond: commenting
Add words to what the child is doing
Add words while you imitate actions or after you imitate actions
Helps make a bridge between your words and their actions, making it easy for them to learn language
Avoid lengthy narration and remember to pause to allow the child to take a turn
Respond: Expansions
An expansion is when you add more words on top of what the child communicated
Child points to a duck → you point and say “duck!”
Child says “muh” during snack → You…
Child says “in” when putting blocks away → you could say “putting blocks in the basket”
Pause: Balanced Communication Turns
Take turns communicating with child
allow time for child to communicate
play a game of “communication catch”
Child communicates
You respond (and wait)
Child communicates
Your respond (and wait)
Take another turn if child doesn’t take a turn after you pause for 5 seconds
Early Communication Intervention
IDEA Part C: EI (early intervention) services are designed to support the family to meet the developmental needs of its infant or toddler (birth to 36 months)
IFSP: Individualized Family Service Plan
The only part that is optional to be required by the state
All 50 states run part c programs
If they choose to have it then they must follow federal protocol
Designed to build the family’s capacity to meet the developmental needs of their infant and toddler
It is coaching and teaching caregivers
Law and evidence line up well
For infants and toddlers (below 3 yrs) current evidence is showing parent-implemented services versus clinical direct intervention are either have equal outcomes or the parent intervention outcome is slightly better.
When they are younger it is about the family, when they transition it is about the education
It is an entitlement program, must provide services no matter what
6 components of EI services:
Screening/Evaluation/Assessment
states get to determine what their requirements are for it to be a developmental/language delay
Done in a multiple disciplinary ways
Interdisciplinary: all together at the same time
Transdisciplinary: One primary doing the testing and others either watching and taking notes or gets debriefed after.
Goal setting and intervention
Primary services Provider model: transdisciplinary, one main provider goes and provides services with support from other professionals.
Consultation with and Education for team members, including families and other professionals
Service coordination
Help connect family with resources and support that they need that go beyond services.
Transition planning
Starting planning for school once they get close to their 3rd birthday
Advocacy
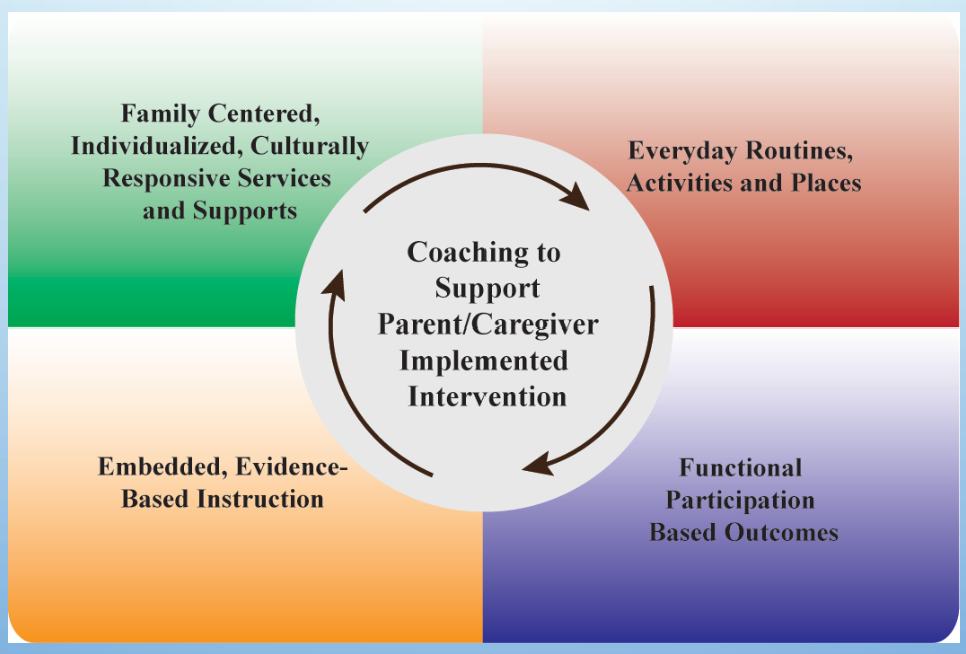
4 Guiding Principles for EI Services
Family-centered and culturally and Linguistically responsive services
Not showing how to parent, just providing services that fit family’s needs
Developmentally Supportive and Promote Children’s participation in their natural environments
Where would the child be participating if they didn’t have a language delay
Location: Home, preschool, park, library, etc.
Routine/Activity: don’t create contextualized activities, incorporate them into daily life
People: who are the people the child normally interacts with?
Materials: don’t bring in foreign items
Not the things that make a difference
Comprehensive, coordinated, and team-based
Based on the highest quality evidence available
best quality service delivery in their natural environment and intervention strategies
Foundations of Family-Guided Routines Based Intervention (FGRBI)
Working with the parents in a collaborative model
caregiver: parent, teacher, grandparent — someone who sees the child regularly
Collaborative intervention model
Principles and Practices in Early Language Intervention:
All children are communicators regardless of age or ability level. All children behave in ways that signal their state, interests, attention, and needs.
Need to know their current communication and what they are already doing.
Early language impairments place children at risk for problems in social development and reading.
All children with language impairments can benefit from intervention in natural environments regardless of their developmental limitations or severity of impairments of form, content, or use.
Most children with language impairments require intervention and support to increase their communication rate (frequency/how often they communicate — toddles in an interactive environment communicate every 2-3 minutes), diversity (what functions?), and complexity (moving along language acquisition in production) at every stage of development.
Most children with language disorders will need systematic teaching to learn, generalize (use in everyday life in multiple scenarios), and maintain (keep using skills in everyday life — maintaining that skill) new language and communication skills across the toddler and preschool years.
Children’s progress in using communication functionally in everyday activities, not their diagnoses, should determine the methods, dosage (how much/how often), contexts, and duration of intervention.
Early Communication Intervention:
Begins with supporting social foundations of communication (joint attention, engagement, play)
Teaches prelinguistic communication skills as needed
Provides a mode for expressive communication
Builds comprehension (receptive) as well as production
Continues through the transition to spoken language
A wide range of strategies can improve children’s language and communication skills — contingent responding, turn-taking, modeling new forms and functions in context, recasting and expanding child communication acts, providing meaningful feedback in response to children’s attempts, and prompting.
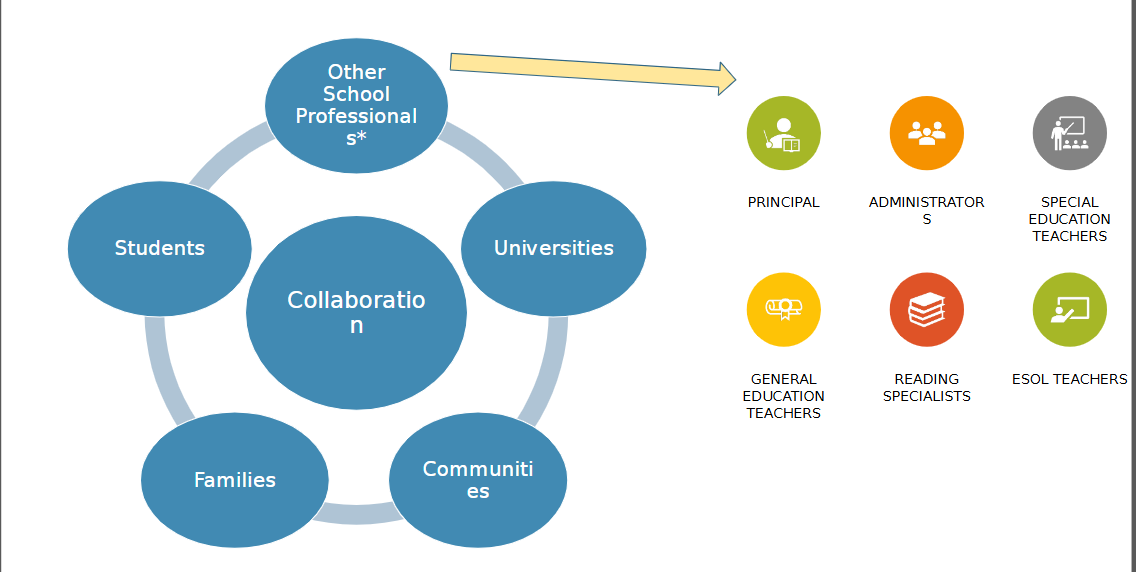
Teaching and supporting partners (parents, caregivers, teachers, and peers) are essential to successful child communication intervention. Effective early intervention depends on the participation of partners who respond to communication, who teach new forms and functions of communication in context, and who can modify how they respond and what they model as children develop new skills. (collaboration)
Full participation in home and classroom learning opportunities is a critical component of early language intervention. Thus, making adaptions to promote participation, and providing support and training to partners to support learning in natural environments is part of early communication intervention.
Early Communication Intervention Priorities for Selection Targets (Behavior): need to be done in the following order!
Increase the frequency of communication.
increase the frequency of their current form.
Expand to new functions.
need to expand beyond expressing needs and wants, want to make sure intervention includes social communication.
Extend to new forms (increase length, grammatical features, and sentence structure).
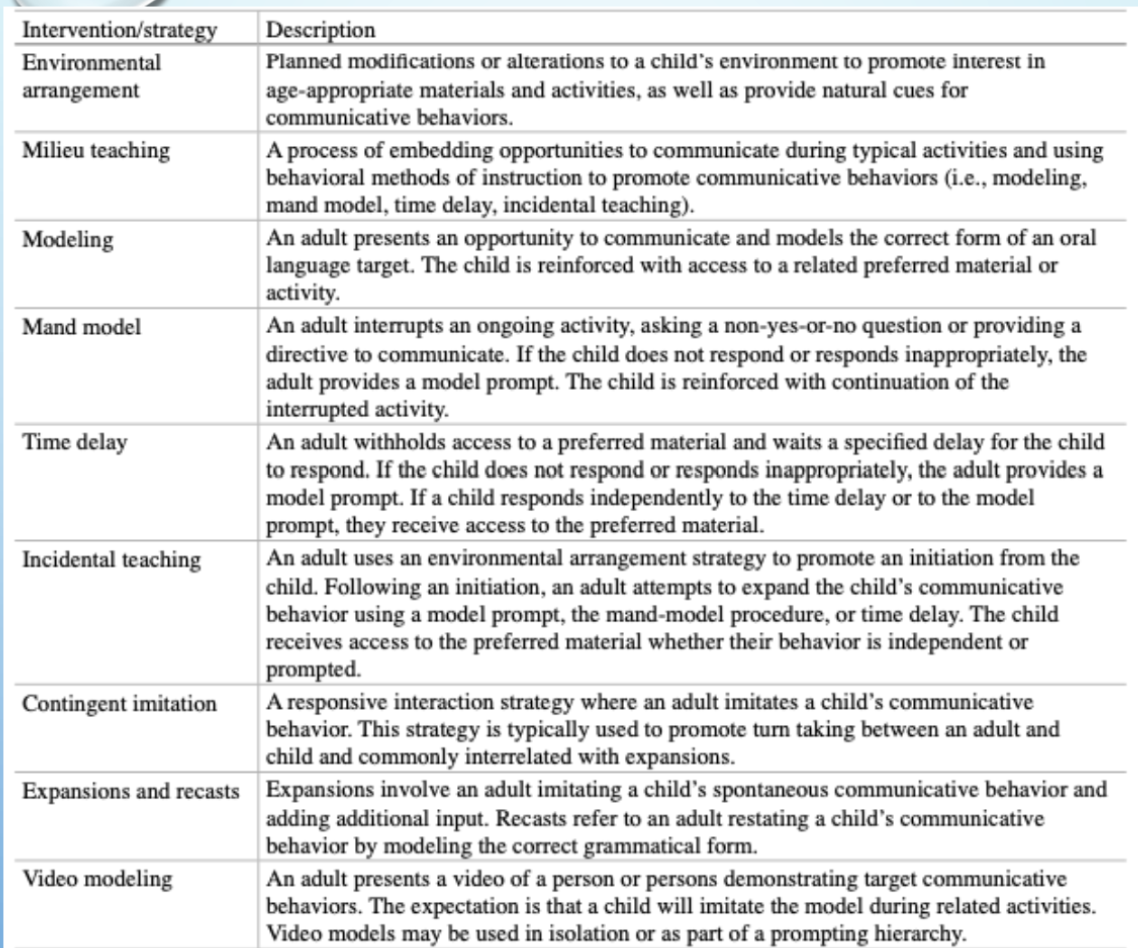
Contingent imitation: The caregiver imitates what the child does — showing that the child’s language is powerful and also serves as a return.
Expansion: take what they said and add a little more to it, this shows the next steps of language.
Recasts: focused on adding the correct words or grammatical features.
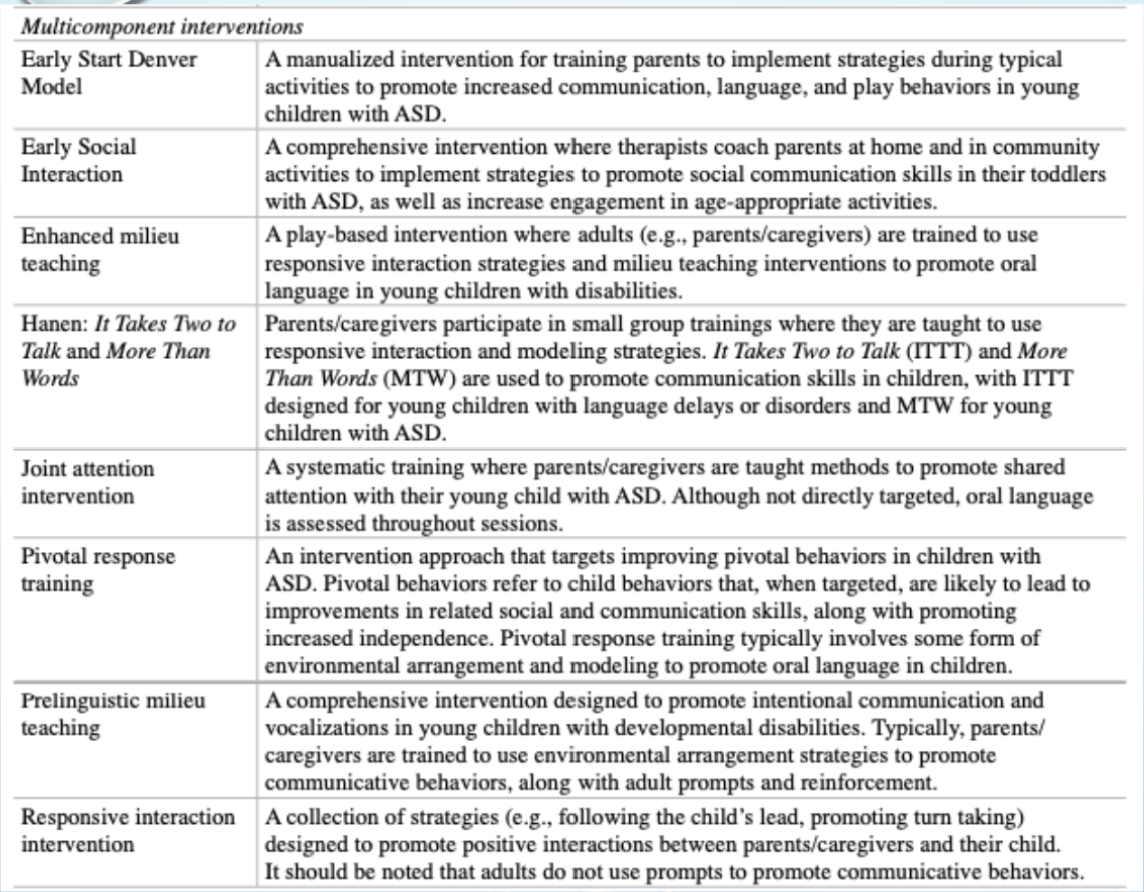
Enhanced milieu teaching: play-based that incorporates environmental arrangement
setting up the environment to give the child multiple things to communicate about. The goal is for the environment to prompt the child to communicate (For example: insight out of reach).
Prompting: least to most prompting — wait after first form of communication, then go to next level support (“do you want paper towels or bubbles” — put what they want last), then last you can use say “bubbles”, then say “bubbles!” Give them a chance to say it twice and if they don’t then give it to them an say “bubbles!”.
Prompts are limited and layered throughout the session.
Autism
If you’ve met one person with autism, you’ve met ONE person with autism
Official diagnostic is autism spectrum disorder or ASD
DSM (diagnostic and statistical manual of mental disorders)
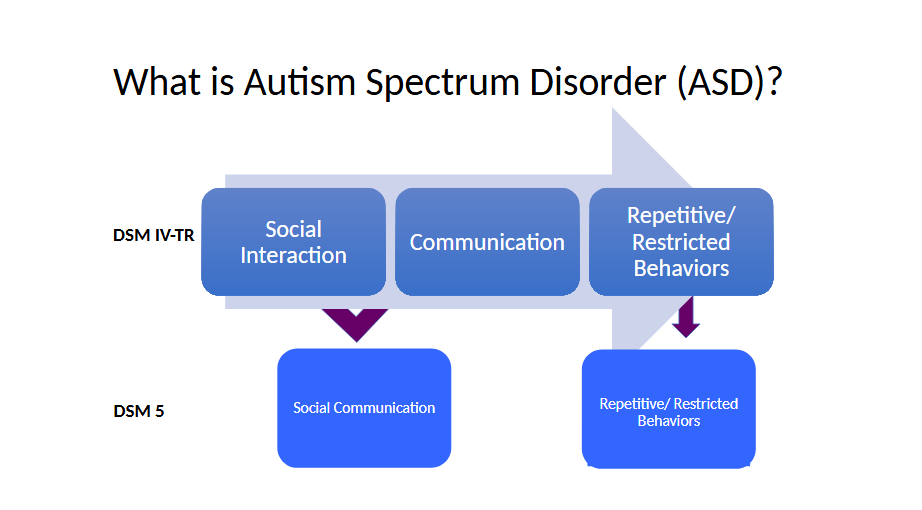
Three main parts (prior, not current) social interaction, communication, and repetitive/behaviors
Now two main parts: social communication and repetitive/restricted behaviors
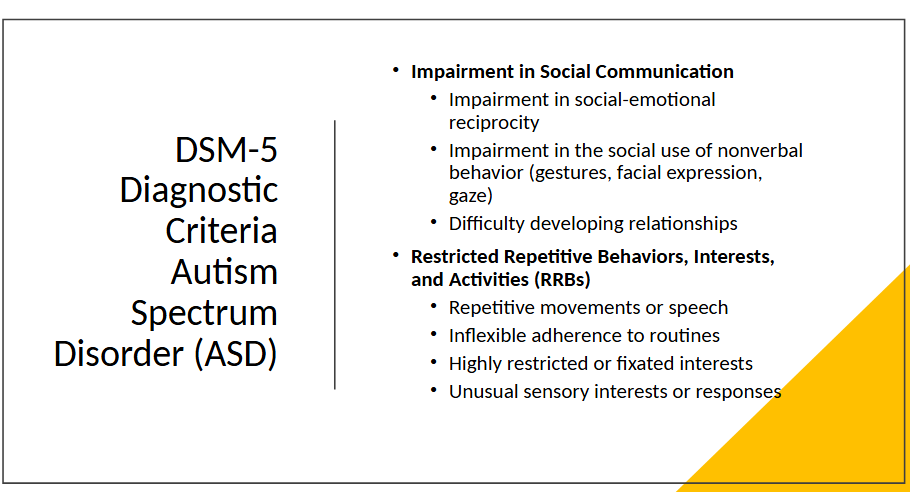
Three areas of social communication impairment and all three must be met to be diagnosed with autism
Impairment in social-emotional reciprocity
Impairment in the social use of nonverbal behavior (gestures, facial expression, gaze)
Difficulty developing relationships
For restricted or repetitive behaviors you must have two of the four to be diagnosed with autism (RRBs)
Repetitive movements or speech
inflexible adherence to routines
highly restricted or fixated interests
unusual sensory interests or responses
Must be present from early childhood and have a functional impact on their life
Person-first:
“person with autism”
“child with ASD”
places the person first, disorder doesn’t identify the person
generally more preferred by family members and professionals
Family members of child with autism or are more co-dependent prefer person-first
Identity-first:
“autistic person”
“autistic child”
The disorder is inseparable than the person and is an important part of the person’s identity
generally more preferred by autistic adults
Ask what terminology they prefer.
Social Communication Disorder
persistent difficulty with verbal and nonverbal communication that cannot be explained by low cognitive ability
Difficulty in acquisition and use of spoken and written language as well as problems with appropriate responses in conversation
Limits effective communication, social relationships, academic achievement, or occupational performance
ASD Basics
Developmental Disability; neurodevelopmental disorder
1 in 36 children
present across all racial, ethnic, and socioeconomic groups
4 times more common in boys than girls
lifelong disorder:
Symptom presentation changes throughout life
importance of early diagnosis
need for sustained support
Levels of support: 1, 2, or 3, not high or low functioning it is about how much support then need
Range of intellectual abilities: can be highly gifted or have a intellectual disability
differences in learning the meaning of words:
everything and everybody has a name or a label
things can have multiple labels
words can have multiple meanings
make incorrect associations and/or interprets word literally
differences in use of language:
echolalia
act of repeating or echoing words or sentences that others have said
3 major types:
immediate
delayed
mitigated
Metaphorical language
repetitive questions and sentence forms
differences in level of understanding:
may repeat words and phrases that are beyond level of comprehension
some language is understood at very high level when related to an intense interest
difficult to understand the true ability of those who are nonverbal
Differences in early interaction and communication skills:
individuals with ASD may have
School Based Services: Roles, Responsibilities, and Context of SLPs in Schools
Statistics: (caseload surveys) 91% of school-based SLPs provided intervention for language disorders
Serve more children with spoken language disorders than any other childhood communication disorder
Critical Roles: SLPs have integral roles in schools and are essential members of school faculties
work across all levels
serve a range of disorders
ensure educational relevance
provide unique contributions to the curriculum
highlight language/literacy
provide culturally competent services
Legal mandates
free appropriate public education (FAPE)
Individuals with Disability Education Action (IDEA)
Least Restrictive Environment (LRE)
Section 504 - allows for accommodations which is not interventions. With an accommodation you are able to participate fully
The Family Educational Rights and Privacy Act (FERPA)
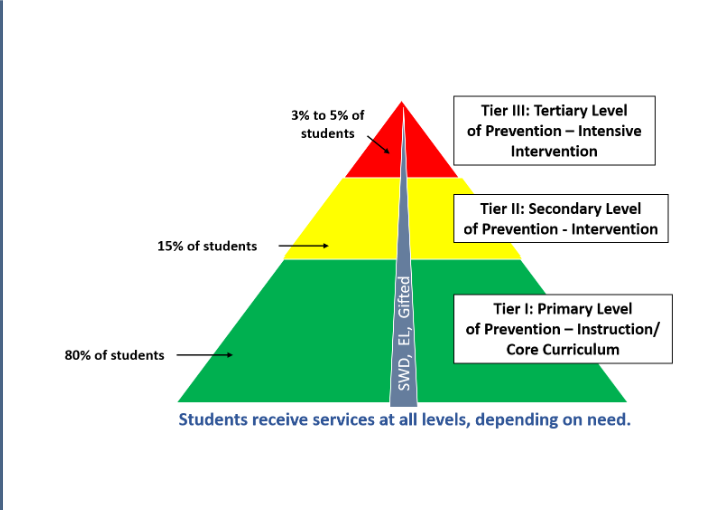
Prevention and RTI: Response to Intervention (RTI)
In theory, it has a lot of strengths, but how RTI is implemented, it then has some problems
prevent failure and provide an alternative method for identifying students with learning disabilities
High quality instruction matched to student needs
Learning rate over time/level of performance
make important educational decisions
Special Education Eligibility Categories:
Include direct and related services - the eligibility catergories do not dictate specific services, the needs dictate the servicces
Autism
Deafblind
Deaf/Hard of Hearing (D/HH)
Emotional and Behavioral Disorder
Intellectual Disabilities
Orthopedic Impairment
Other Health Impairment
Significant Developmental Delay (ages 3-9)
Specific Learning Disability
Speech Language Impairment
Traumatic Brain Injury
Visual Impairment and Blindness
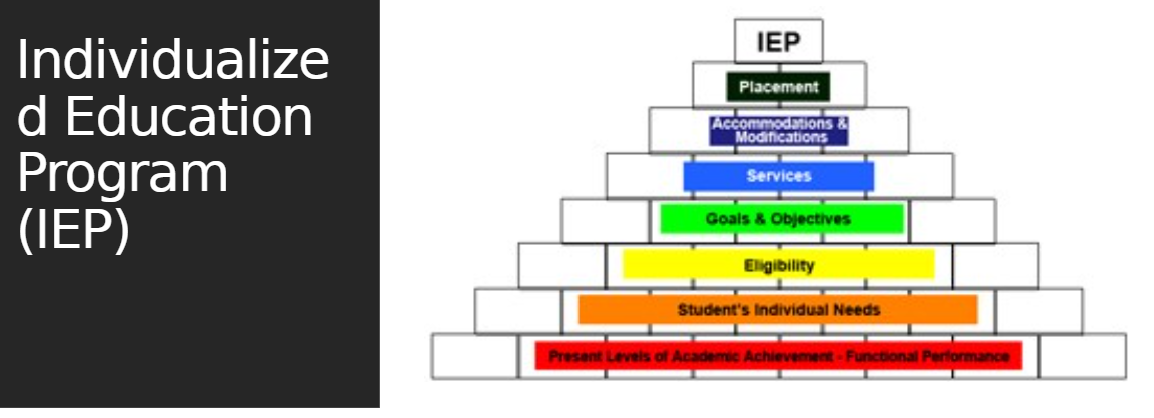
Determining Eligibility (for “speech lang. impairment” in Georgia)
Determining eligibility for speech-language impaired special education services includes three components:
The Speech-Language Pathologist determines the presence or absence of speech-language impairment based on Georgia rules and regulations for special education
Documentation of an adverse affect of the impairment on the child’s educational performance
The team determines that the child is a child with a disability and is eligible for special education and appropriate specialized instruction needed to access the student’s curriculum
Eligibility shall be determined based on the documented results of at least two or more measures or procedures, at least one of which must be formal, administered in the area of impairment, documentation, and adverse affect.