0.0(0)
Explore Top Notes Note
Note Studied by 93 peopleNoteStudied by 19 peopleNoteStudied by 44 peopleNoteStudied by 194 peopleNoteStudied by 322 peopleNoteStudied by 13 people
Studied by 93 peopleNoteStudied by 19 peopleNoteStudied by 44 peopleNoteStudied by 194 peopleNoteStudied by 322 peopleNoteStudied by 13 people
Chapter 8: Probability and Random Variables
Key Biogeochemical Cycles to Know for AP Environmental Science
drugs
AP World 2.6 - Environmental Consequences of Connectivity
AP PSYCH 2.9 Sleep and Dreaming
Module 3
Week 11 | Day 1 | PSYA02
Week 11 | Day 1 | PSYA02
Neuropsychology In Context
- WWI & WWII left a lot of brain-injured soldiers and people had to find more specialized ways to help them
- Educational testing: already wide use of standardized tests (Binet’s test)
- Basic research: experimental studies made the theories behind neuropsychology assessment stronger
- Neuroimaging: impressive advances in the ability to image a brain meant less need for tests to identify injured areas (eg. they don’t need to do a test, we can just do a scan of your brain)
- Historically: World War Soldiers have brain injuries, how does this affect their thinking skills and where is the injury?
- Present: Impact on thinking skills, what is the consequence and how can we help?
Cognitive Training
Basic approach: ‘Trainee’ completes structures cognitive tasks, typically adaptive or performance over a period of time/sessions
- Grounded in a cognitive theory
- Adaptive design is key to neuroplasticity
Neuroplasticity: the ability of the nervous system to respond to intrinsic or extrinsic stimuli by reorganizing its structure, function, and connections
- Commonly invoked mechanism for the efficacy of cognitive training
- Training is typically specific to cognitive ability, which may be a barrier to generalized rehabilitation programs
- Cognitive training can be thought of as a restorative approach
Near vs Far Transfer:
- Near Transfer: training on one task generalizes to performance on another, highly similar task (eg. training on one working memory tasks improves your performance on another working memory task)
- Far Transfer: training on one task generalizes to performance on another, dissimilar or loosely similar tasks (eg. working memory task training improves academic functioning or other real-world skills)
Cognitive Training Example
- “What happens if we train cognitive training paradigm while patients are in for substance abuse?”
- Training did not have any impact on reduced substance abuse relapse
- Basically, this means that even if you train using games (like Lumosity), it may help better performance in similar games but not transferable to real-life skills
Cognitive Rehabilitation
- The main function is to support the patient’s ability to function in their day-to-day life
- Treatment target: Depends on the patient's goals that depend on the patient's willing to participate in treatment
- Several approaches to cognitive rehabilitation:
- Not trying to restore cognitive deficit, but instead emphasizing their strong points
- Restoration of cognitive deficit
- Modification of environment
- Implementation of supports
- Systems-type interventions (eg. family support)
- Examples of compensatory approaches
- Internal: raising awareness of potential cognitive errors
- Eg. mega-cognitive monitoring in Goal Management Training
- External: lists and record keeping to support memory
- Eg. memory organizer in Learning the Ropes for Living with MCI
- Internal: raising awareness of potential cognitive errors
Cognitive Rehabilitation Example:
- Go slow but try to make no mistake in doing that task
- Gradually go faster
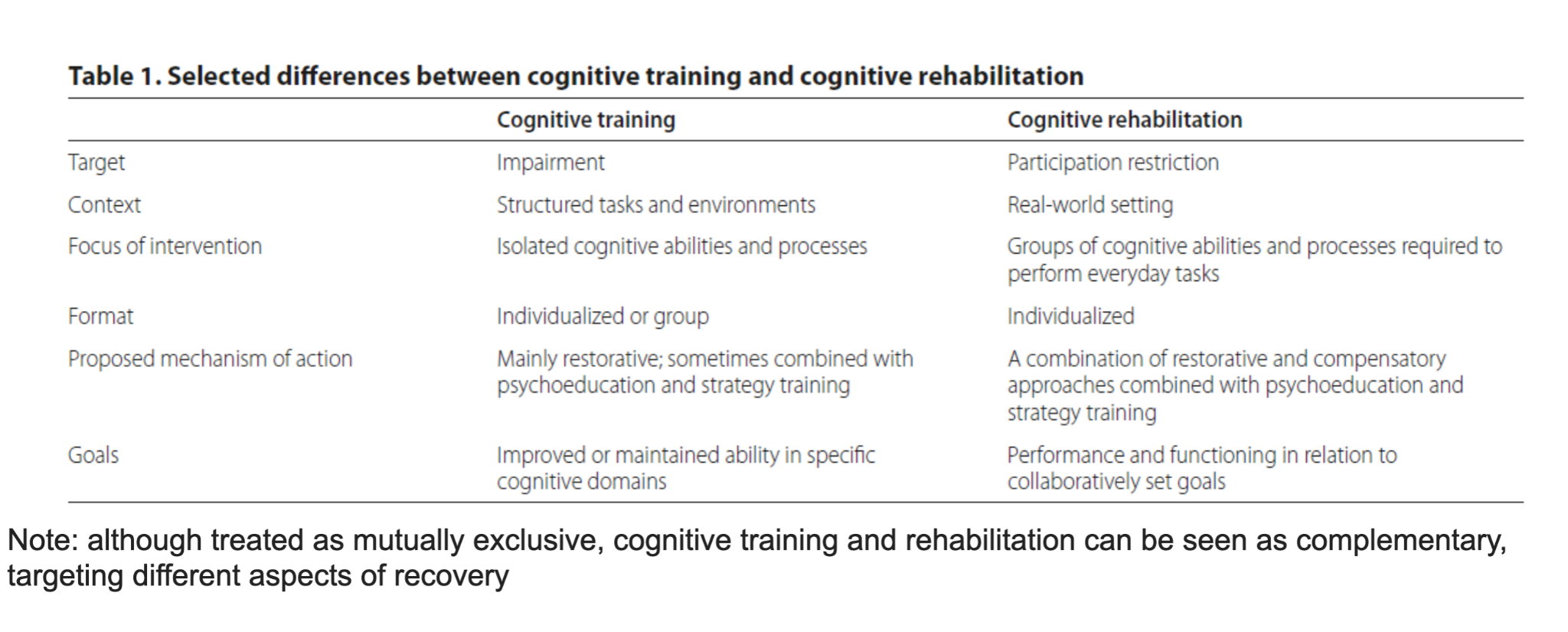
Rehabilitation vs Training
Holistic Approaches
- Emphasizing multiple domains of functioning
Complementary, Not Incompatible
- Cognitive training and rehabilitation both offer approaches to provide treatment or intervention to individuals with varying levels of cognitive difficulties
- The primary differences are in their target outcomes and approaches, but can often be completed in combination (not mutually exclusive approaches
- Newer models emphasize holistic, integrative approaches
- As a newer area of clinical practice, continuous improvement, adaptations, and research will continue to shape current approaches
- Ngl I have no idea what I wrote for this it’s just from the lecture pls review
0.0(0)
Explore Top NotesNoteStudied by 93 peopleNoteStudied by 19 peopleNoteStudied by 44 peopleNoteStudied by 194 peopleNoteStudied by 322 peopleNoteStudied by 13 people
Chapter 8: Probability and Random Variables
Key Biogeochemical Cycles to Know for AP Environmental Science
drugs
AP World 2.6 - Environmental Consequences of Connectivity
AP PSYCH 2.9 Sleep and Dreaming
Module 3