Mid-Term Notes
Bones
Functions of Bones
Structural Support → soft Tissue and muscles and organs
Growth Center for Cells → Red blood cells and platelet in bone
Movement → Muscles are attached, contract to move and bones facilitate movement
Protection → Protective cage for more delicate parts (ie. Skull and Brain)
Reservoir of Minerals → body can call upon in order to regulate the level of calcium and phosphorus in the body
Anatomical Terms
Plantar → Towards the sole of the foot
Dorsal → Uppermost surface of the foot
Plantar flexion → point your toes
Dorsiflexion → bringing top of foot closer to shin
Opposition → Thumb comes towards other fingers
Reposition → returns to normal anatomical position
ABduction → Moving body segments away from the body
ADduction → moving body segments TOWARDS the body
Supination → rotating the wrist so the palm faces up
Pronation → rotating the wrist so the palm faces down
Inversion → ANKLE → standing on outer edge
Eversion → ANKLE → standing on the inner edge
External Rotation → twisting body part outwards from midline
Internal Rotation → turning body part inwards towards midline
Protraction → moving anteriorly
Retraction → moving posteriorly
Circumduction → combo of flexion, extension, abduction, adduction
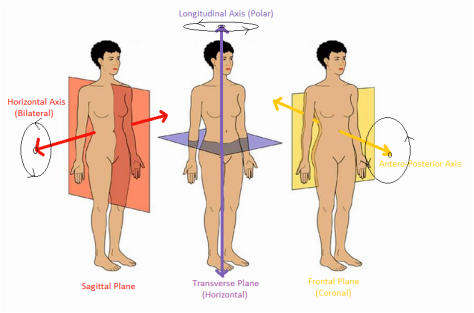
Axis and Planes
Types of Bones
Long Bones → found in hands, arms, legs, SAME SHAPE
Short bones → most common in wrist, shaped roughly as a cube and contain mostly spongy bone
Flat Bones → flat thin and are found at the roof of the skull and in the ribs
Irregular Bones → Include odd looking bones (Vertebrae or sphenoid bone)
Sesamoid Bones → are unusual, small and flat bones wrapped within tendons that move over a bony surface, Patella
Axial vs Appendicular Skeleton
Axial Skeleton
80 bones
are comprised of the spine, much of the skull and the rib cage
most of the abdominal group origins are on the axial skeleton
THEY HELP STABALIZE AND SUPPORT
Appendicular skeleton
126 bones
all movable limbs and girdles
6 Main regions:
Pectoral girdle: clavicles and scapulae
Arms are Forearms: humerus, ulna, radius
Hands: carpals, metacarpals, phalanges
Pelvis: left and right hip bones
thighs and legs: left and right femur, patella, tibia, fibula
Feet and ankles: tarsals metatarsals, phalanges (Medial, intermediate, distal)
Bones need to Know
Calcaneus - largest of the Tarsal bones in the foot
Mandible - Only moveable bone in the skull, it is the strongest
Atlas - C1, it is what the skull rests upon, it is the first cervical vertebrae
Temporal Bone - Weakest bone in the head, this is where the ear rests
Sacrum - This is the tail bone, turned in for men, out for women
Bone Landmarks
Ridge, bump, groove, depression on the surface of the bone that serves as a guide to the location of other body structures (where ligaments can attach)
Long Bones
Long Bones are made up of different types of live tissue that make it so can move and strengthen. They are:
o Cartilage: Smooth movement when protecting the bone. This is what disintegrates so people would need a knee replacement.
o Periosteum: Connective tissue, these are fibres and ligaments and tendons to connect bone to bone OR bone to muscle.
o Medullary cavity: inside the shaft of the bone. (Called the diaphysis). This is the where the red and yellow bone marrow, (red is where blood cell form) CHILDREN HAVE MORE THEN CHANGES AS yellow bone marrow is fat (ADIPOSE) so as they gain fat they will also gain more yellow marrow)
o Compact Bone: Dense part of the bone, thickest part of bone à is responsible for bone structural integrity
o Cancellous or spongy bone: marrow is in the holes (Cavities of the it) THIS IS THE PART THAT STRENGTHENS WHEN IT IS EXERCISED,
o Diaphysis: Shaft of the long bone that is made up of the medullary cavity, part of the periosteum, and compact bone.
o Epiphysis: end of long bones
o Summary: Long Bones are like a sturdy building with different parts: cartilage for smooth movement, periosteum for connections, medullary cavity for marrow, compact bone for strength, and spongy bone for reinforcement.
The Neurocranium
o There are 8 cranium Bones
o This is the upper and back part of the skull
o This creates a protective casing around brain
o The Bones are the Frontal, Parietal, Temporal, Occipital
The Calvaria
o Uppermost part of skull
o Protective covering
o The Frontal, Parietal, temporal bone, occipital bone
o Parietal is largest, and temporal is the most fragile (DECREASED RESISTANCE, MAJOR BLOOD VESSELS OVER IT)
o can be displaced internally or fractured, medical emergency
o this is because of blows to the skull
The Facial Bones
o has 14 bones
o Mandible is only moving and strongest bone in the face
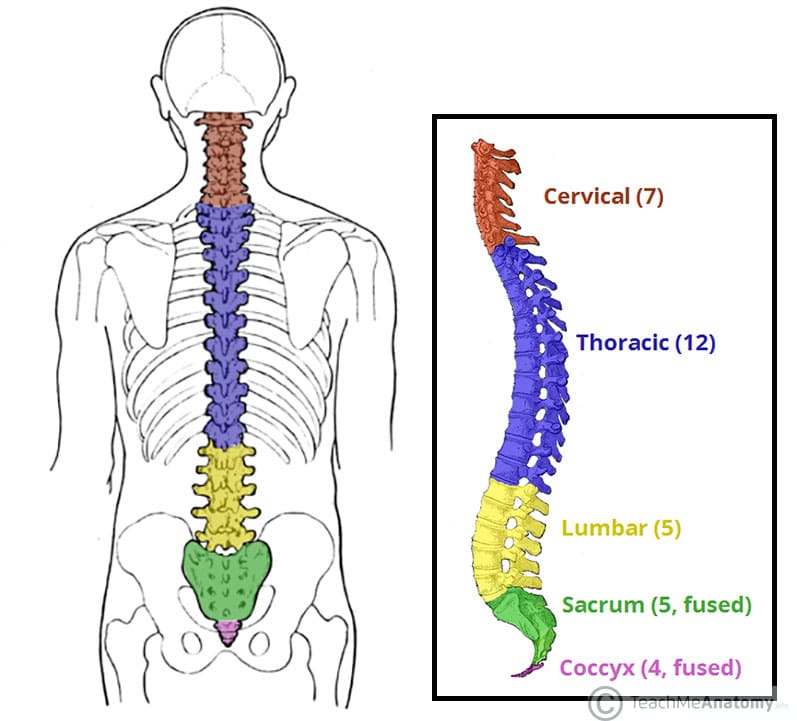
Vertebral Column
o They have fibrocartilaginous discs:
o Their functions are to:
o Provide strength, flexible support for the body, they are to keep the body upright
o Point of attachment for muscles of back
o Protects spinal cord and nerves
o Absorbs shock with out damaging the vertebrae
o There are 24, and then the sacrum
o Bears majority of the weigh of the body, So UNDER A LOT OF PRESSURE
o Protective canal for the spinal cord
Injures in the Spine
o Traumatic blow of the spine can fracture, dislocate, crush, compress the vertebrae
o Most have to do with the nerves in the spine of the spinal cord
o If severely damaged, then the spine may not be stable anymore so put a lot of pressure on the spinal cord which then damages the spinal cord
Ribs
o Made up of bone and cartilage
o Protects internal organs and they can twist so to protect chest area
Pelvic Girdle
o Pair of Os Coxae (Hip bones)
o Support for the bladder and the abdominal content
Male vs Female:
o Male sacrum tilts forward, more of a “heart shape” and ilia closer together
o Q-angle is greater in females
o Greater then 90 degrees for the female anterior view
Structure of Bone
o The body is repeatedly changing over the cells that are in your bone.
o They are doing this through:
o Ossification: The process of new bone production
o Osteoblast: Forms bone by laying down new minerals along the surface pf the bone, uses calcium.
o Osteoclast: they are large multinucleated cell; this breaks down the old calcium and bone this is partially responsible for the release of calcium into the blood stream. Estrogen breaks down osteoclast which means that it regulates it and allows osteoblasts to work better. This is much faster than osteoblast though.
o IN A REGULAR BODY THEY ARE WORKING EXACTLY EQUAL TO ONE ANOTHER, this is changing as people get older because of:
o Osteocytes: Signals the blasts/clasts
Bone Formation
Compact Bone
Long bones
1. Begins as cartilage
2. Hormones excite the osteoblasts which then release a gel like substance (Discharges)
3. Minerals would be deposited in the gel then harden in bone, this is with diffusion and osmosis then the minerals would calcify
Cancellous Bone
Flat bones of skull and ends of long bones
1. Begins as fibrous membrane
2. Gel-like substance forms a bundle of fibres
3. New bone forms out “outwards” from center of bundle
4. Convert “soft spots” at birth into bone
Bone Remodeling
o Don’t just grow from osteoblasts, there is a take and give system
o The osteoclasts take the old bone, and the osteoblast give new bone, this can make the bones thicker especially in children, which means that at before 35 there is more of growth then take then after there is no more added so even and then start to shrink
Structures and Functions of Bones
o IS A LIVING TISSUE
o There is blood flow through it
o This means that it is responsive to disease and self repairing (Broken bones can fuse again)
Inorganic
o Hydroxyapatite: calcium Rich and stiffens to strengthen the collagen together
Organic
o Mainly Collagen, (Long chains of proteins that is flexible and elastic fibers)
Composed of:
o Calcium Carbonate and calcium phosphate
o make up 60-70% of the weight of the bone and they prove much of the bone’s stiffness and resistance to pressing or squeezing force
o Collagen
o Gives bones the flexibility and contributes to resistance of stretching forces, age changes this and then the bone become more brittle
o Water
o Much smaller proportions of water then other body parts
Effect of Fitness on Bones:
o Become denser and more mineralized with long exercise
o Inactive shows exact opposite meaning there is a loss of bone dense and decreased bone weight
Long-term Effects
o Increased calcium stores
o Exercise is stress on bones which means that there is more stress, so bones get stronger
o Weight bearing exercises give more minerals in bone which includes collagen and calcium
o Increased stretch of ligament and tendons
o Become stronger and more flexible
o Muscles get stronger so the tendons must cope with the extra pull
o Ligaments must get stronger and more flexible so they can control the joints that the stronger muscles and tendons act on
o Increased thickness of cartilage
o Is on the ends of bone becomes thicker to deal with the extra wear and tear and shock absorption from an increase in activity
o Increased production of synovial fluid
o Joints are being used more so through exercise the membrane produces more fluid to keep joints lubricated
Brain Injuries
Concussion
o Injury to the brain
o Mechanism:
o Violent shaking/jarring of the head
o Brain is bouncing against the inside of the skull
o Symptoms:
o Confusion
o temporary loss of normal brain function
o Headache that won’t go away
o There is no such thing as a minor concussion or just shaking it off
o You have to rest to heal
CTE
o Chronic traumatic encephalopathy
o is a progressive brain condition
o thought to be caused by repeated blows to the head and repeated concussions
o Associated with contact sports
Rib Injuries
o Bruises, torn cartilage, and bone fractures
o Common causes: falls, car crashes, contact sports
o Heal on their own in about 6 weeks
o Can’t breathe deeply so there is an increase on your risk of developing pneumonia
o Could lead to a collapsed lung
Dislocation
o Separation of two bones where they meet a joint
o Most common: shoulder and fingers, also can be in knees (Very rare), hips and elbows
o Sometimes can be put back in the proper place by itself but if not, you have to have a trained healthcare worker manually put it back in
o May take months to heal depending on severity
Femur Fracture
o Can cause a significant blood loss in person and loss of bone marrow which greatly affects the creation of red blood cells
o Young People: have it due to car crashes (High-energy collisions), person and car or car and car or gun shot or very high fall
o Old People: lower force incident, fall from standing as they could have weaker bones
o Repair: you must put screws and plates into the bone to let it fuse and allow for the things to heal as there is so much bone so they can’t just hold itself together
Joints
What is it
o A point of connection between 2 bones
o Strands of connective tissues called ligaments, and they hold the bones together and ensure stability of joints
o They are classified by their structure OR function
Function Classifications
o Motion capabilities
Synarthrosis → allows no movement under normal conditions
amphiarthrosis → allows limited movement
Diarthrosis → allows for a freely moveable joint
Structural Joint Classification
o Fibrous joint
o Allows no movement (Skull joints ends of bone)
o Bound tightly together by connective tissue
o Cartilaginous joint
o Allows limited movement
o Body of one bone connects to the body of another by the means of cartilage
o Vertebrae disks
o Synovial joint
o Allows large range of movement
o Bony surfaces are separate by fluid and cartilage
o HIP JOINTS OR SHOULDER JOINTS
o THREE TYPES:
o Uniaxial: rotates around one axis
o Biaxial: moves around 2 perpendicular axes
o Multiaxial: around all three perpendicular axes
Types of Synovial Joints
1. Ball and socket joint
2. Hinge joint
3. Pivot joint
4. Condyloid joint (Ellipsoid joint)
5. Saddle-shaped joint
6. Gliding (Plane) joint
Ball and Socket Joint
o MULITAXIAL ROTATION (IN ALL PLANES)
o Most moveable joint
o Allows for circumduction (So flexion, extension, adduction, abduction…)
o Round bone fit into a cup
o HIP AND SHOULDER JOINTS
Hinge Joint
o Uniaxial
o Has one surface that s convex and one that is concave (the weird hole in the humerus that allows the ulna to be inserted into it)
o FINGER AND ELBOW JOINTS (AND KNEES)
Pivot Joint
o Uniaxial
o Allows for pronation and supination
o HEAD OF RADIUS AGAINST ULNA
Condyloid Joint
o Kinda like ball and socket but shaped differently
o Biaxial (Flexion, extension, abduction, adduction)
o Usually, an oval surface and ovular convex and one is concave
o WRIST AND KNUCKLE JOINTS
Saddle Joint
o Biaxial
o Bones are together as in sitting on a horse
o CARPOMETACARPAL JOINT OF THE THUMB
Plane Joint
o Uniaxial
o Bones surfaces involved are nearly flat
o Comes in groups of bones
o They just glide alone each other and rotate along each other
o FOUND IN WRST AND ANKLES
o THE ACROMIOCLAVICULAR JOINT OF THE VERTEBRAE
Common Injuries of the Joints
o Cartilage damage à arthritis (hard rubbing)
o Sprains à foot especially (This is more with ligaments and muscles)
o Dislocation and separation à mostly in shoulder* but can also happen in knee hips and fingers
o *Shoulders à there are 2 types partial and complete
o Common: Humerus slips anteriorly out of the glenoid fossa (Cavity)
Symptoms: swelling, numbness, pain, weakness, bruising, capsule and or rotator cuff tears, brachial plexus injury
Muscles
There are more then 600 muscles in the body
o Move in and out
o To stabilize
o They are having to move together
o There is voluntary or involuntary from nerve system (3 groups of function and structure)
o Smooth: involuntary, eating
o Skeletal: voluntary, breathing, moving
o Cardiac: involuntary, heartbeat
o Muscle is attached to bone through a tendon
o Origin: the proximal location, the part that is more stationary
o Insertion: the distal end, the part that moves the most
o In contraction: insertion moves towards the origin
o Muscle makes up 40% of your total body weight
Muscle Tissue
o Just a collection of cells
o Shortens during contraction (tension is created moving)
o Achieved through tendons à tough bands that move the bones with the force of the muscle
o Three types
o Skeletal
o Uses of tendons
o Most prevalent
o Conscious control and striated → BECAUSE OF ORGANIZATION OF SARCOMERES AND MYOFILAMENTS (light is actin and dark is myosin and actin or only myosin)
o Cardiac
o Only in the heart
o Striated (not as much as skeletal) is directed by the autonomic nervous system
o Pumps blood from heart to body
o Smooth
o Surrounds internal organs and hair follicles
o Spindle-shaped fibers in dense sheets (CANNOT STRENGHTEN)
o Contracts more slowly but remained contracted for longer periods of time
Properties of Muscle Fibres – KNOW
o Irritability: response to stimuli
o Contractability: Shorten in length
o Elasticity: Stretch and return to original position
o Extensibility: extend in length
o Conductivity: transmit nerve impulses
Agonist and antagonist
o All arranged in opposing pairs
o Always pull is one muscle will pull one direction then the other muscle when “relaxing”
o Agonist: primary responsible for movement (the one doing the work)
o Antagonist: the one that counters it is the agonist muscle (would lengthen)
o Stabilizer: provide support and holds the joint in place so that the movement may occur
Break down of the Muscle
o Muscle à Bundle (Fascicle) à Muscle fibres (millions make one fascicle) à Myofibril (One tube that can extend or flex) à Filaments (Where the Actin and Myosin is)
o Actin is the light, and the dark is the myosin when the muscle is striated
o Epimysium: Surrounds the entire muscle → connective tissue
o Endomysium: covers full bundle of fascicles that are held together by perimysium à connective tissue
o Sarcomeres: compartments in myofibrils that are the actin and myosin
o They are individual but when organizes end to end they make up myofilaments
Actin and Myosin
o Myosin
o Have a head (wants to stick into the actin) and a tail
o Head would attach and contact and pull in in a canoe motion
o That is what converts the ATP to ADP, which is usable, by removing a Pi molecule when attaching
o You get the ATP from food
o Actin
o Has binding sites for the myosin head
o Two proteins:
o Troponin: where the calcium goes (when bound they open up the spots to bind)
o Calcium: trigger for muscle contraction after nerve impulse
o Allows for actin and myosin to interact
o Relaxation is caused by re-uptake of calcium ions required for adenosine triphosphate
o ATP is used to detach
o As you work more = more use of muscle = more ATP used = more need = food need
o Tropomyosin: cordlike structure that covers binding sites (so you are not always contracting)
o Work like a swivel locking mechanism à only allow for binding once the calcium is released by the sarcoplasmic reticulum
o This is the excitation-contraction coupling à this protein filament interact at the molecule level that allows them to slide across one another, this is all about the nerve and muscle’s interaction together à leads Sliding Filament Theory, which is the allowing the synchronized action across the muscle
ATP ROLE
ATP is the energy source behind the release of calcium
ATP is also used to DETACH myosin from actin
ATP must be replaced through food metabolism for process to continue
Thin and Thick Filament
o Thin: Actin
o Thick: Myosin
Sliding Filament Theory
o The muscles pull they don’t push
o A limb can push but only because of a muscle pulling on bone
o Contract if the load is light or heavy
o It will remain the same length if the load is equal to the muscle strength
o Contract due to actin sliding over myosin
o ATP turns into ADP which allows it to bind
o Order of movement:
o Motor nerves active muscle fibres from brain by sending action potential
o Head attaches
o Cross bridges (repeat like canoe) à (attach, rotate, detach, and reattach in rapid succession) → space between the actin and myosin
o The actin filament moves, and sarcomere shorten à I band shortens and H-zone shrinks (A-band stays the same)
o Optimal joint angle is 90-120 degrees
o Optimal number of cross bridges (Weird space between) à ALLOWS FOR MAXIUM FORCE
o Large: few cross bridges (sarcomeres are too far apart)
o Small: cross bridges interfere with each other (sarcomeres too close together)
The Neuromuscular System
The Nervous System: Controls skeletal muscle and is activated à conscious control à bigger muscle is more nerves (from the peripheral (PNS))
The Motor Unit
o Made up of the motor neuron (and its axon) and the muscle fibres it activates
o Nerves have a wave impulse (no jerky motion)
o A single nerve impulse with contraction à muscle twitch
o One neuron can be responsible for many muscles fibres
o It is the basic functional entity of muscular activity
o Even though the motor neuron can be attached to many muscle fibres they must all be the same type of muscle
o Each muscle can have more then one motor unit
o Delicate and precise movement
o Many (1500-3000) motors per muscle
o Few (8-50) muscle fibres per unit
o Unrefined and powerful movement
o Few (600-2000) motors per muscle
o Many (1500) muscle fibres per units
o Larger body mass = motor units contain more muscle fibres
All or None Principle
o Can be categorized into small or large unites
o Large: produce large (gross) movement
o Small: fewer muscle fibres so there are finer motor movement
o Smaller because they have fewer muscle fibres than fast twitch motor units (EYES)
o Single motor units in the quad can simulate 300 to 800 muscle fibres
o For maximal muscle fore to be produced all motor unites within that muscle group must be recruited à all to contract or it does not contract à must be at the same time fire and contract
o ALL OR NONE PRINCIPLE à all motors units need to comply à when a motor unit is simulated to contract, it will do so its fullest potential
Activation Threshold
o Has a specific threshold that it must be reached for activation
o Weak nerve impulse = weak threshold (smaller muscle that has it)
o Stronger nerve impulse = stronger muscle = stronger threshold
o This is because of the actin and myosin working together à This is part of the excitation-contraction coupling
o As resistance increases, more motor units must be activated by stronger more intense impulse
o If you need to pick up something heavy then you need more of an contraction which means more of an impulse needed to work them
Link Between the Muscular and Nervous System
Junction Point: EXAM
o Nervous system → impulses originating in the brain and spinal cord
o Both system of the central and the peripheral nervous system working together
o Muscle twitch: single nervous impulse and resulting contraction
o The motor neuron, its axon, and the muscle fibres all stimulate together
o Neuromuscular junction: nerves transmit messages directing the muscle to move
o ACETYLCHOLINE is released when there is a contact point between the nerve and the muscle
o This chemical is then received to ACh receptors which then releases the calcium from the sarcoplasmic reticulum
o Then the chemical is detected by receptors on the surface of the muscle contraction (By activating the movement of troponin) Such as à contract smooth muscle, slow heart rate, and dilate the blood vessels
o Area where nerves and muscle meet and pass on message
o There is a space between the 2 that is extremely small that is in between the nerve and muscle called the synapsis
o This is the principle of energy transfer: electrical energy to the surface of muscle fibres
Excitation-Contraction Coupling
o Muscle contraction as a whole
o Begins with electrical signal from spinal cord, down the nerves at the neuromuscular junction, to the contact point of the motor nerve with the muscle fibre. Once the signal has transmitted across the synapse the muscle is contracted with the release of acetylcholine.
1. Electrical signal that begins starts in the spinal cord and moves along the axon to the junction
2. Then the signal is moved down to the muscle fibre through the tubular membranes and by the release of acetylcholine
3. Calcium ions are then released into the sarcoplasm reticulum
4. The interaction of calcium of the protein troponin and tropomyosin moves to have actin and myosin interact
Muscle Fibre Types
o Fast Twitch
o Type II
o Appearance is white/clear
o Fast contraction à cannot be sustained for a long period of time
o Anaerobic à does not need oxygen
o Large fibres (Think of someone ripped)
o Slow Twitch
o ST or Type I
o Appears red
o Slow contraction à can be sustained for a long period of time
o Aerobic
o Fatigue resistant
o Small fibres (Think of someone who is lean)
o YOU CAN NOT SWITCH ONE TYPE OF FIBRE TO ANOTHER BUT YOU CAN IMPROVE THE FIBRES WITH THE TYPE OF TRAINING YOU DO
Myoglobin
o Difference in fibre type are main do to the extent to which a particular muscle relies on oxygen in the production of energy
o Myoglobin = protein
o They store oxygen and delivers it to the muscles, thus allowing energy production to sustain over a long period of time
o More aerobic processes the more it can sustain longer-term activity
o Slow Twitch: high in myoglobin à endurance
o Fast Twitch: Low in myoglobin à concentrated and shorter burst of energy
o Faster is white because there is less myoglobin and oxygen à there are capillaries in the muscle so to allow the blood to get to the muscles à gain energy form the sugar glycogen instead of oxygen
Nerve-Muscle Interaction and Adaptation
o INTRA-MUSCLE COORDINATION à all in the same muscle
o the ability to activate all motor units simultaneously
o this is impossible so we try to be as efficient as possible à normal is about 60%, athlete is 85%
o MUSCLE FORCE DEFICIT à difference between assisted and voluntarily generated maximal force à at some point you cannot do the action anymore as you are so tired and the muscle need to rest à this is because of vigorous exercises
o Trained athletes though have a larger number of muscle fibres and larger muscle mass à more limited in further strength gains à they are very strong so can’t get any stronger
o INTER-MUSCLE COORDINATION à in different muscles
o The ability to activate different muscles to produce a movement
o Especially the interplay between the agonist and antagonist
o They must be synchronously activated and relaxed
o The greater the participation of muscles/groups the higher the importance of the inter-muscle coordination
Muscle Adaptation to Strength Training
o Biological adaptation à performance improvement through strength training à increased strength
o Performance capacity of a muscle is determined by several factors:
o Fibre diameter
o Intra- and inter- muscle coordination
o Nerve impulse frequency
o Muscle and tendon elasticity
o Energy stores
o Capillary density
o Non-trainable factors:
o Muscle fibre type
o Structure of muscle fibres
o Different factors adapt at different rates
DOMS
Delayed Onset Muscle Soreness
result of microscopic tearing deep within the muscle fibers
Causes:
starting a new exercise program
dramatically increasing duration or intensity
can last from several hours to several days
Not the same as immediate acute pain of a pull or strain or pain/fatigue during an exercise → this gradually happens after you are resting again
swelling can occur
minimized with proper warm up/cool down; need to gradually increase intensity in workout
TO TREAT: Ice, stretch, rest and recover
Reflex Arch
The receptor
o Receives the initial stimulus (pinprick to the skin/loud noise)
2) The sensory nerve
o Afferent – carries impulse to the spinal column or brain (AWAY)
3) The intermediate nerve fibre
o Adjustor – interprets the signal and issues an appropriate response
4) The motor nerve
o Efferent – carries the response message from spinal cord to muscle or
organ (TOWARDS)
5) The effector organ itself
o Carries out the response
o Ex: skeletal muscle – moving hand away from danger
Proprioceptors
specialized receptors within tendons, muscles and joints → Allow from the e-c coupling and sliding filament theory also allow for nothing to get injured
provide sensory info about the contraction, position of body posture and balance → control is with the afferent input
two types: Muscle spindles and the tendon organs
Muscle Spindles
essential in all movement
auto adjust to demands place on them→ are parallel to main muscle fibre and send constant signals to spinal cord
intrafusal muscle (thinner and shorter but behave in same way)
they help maintain tension and sensitive to change in muscle length
HAS 1 EFFERENT AND 2 AFFERENT NERVE FIBRE
sense the change in length and responds to lead to the proper motor response
Golgi Tendon
sensory receptors that terminate where tendons join to the muscle fibre
aligned in series with the muscle such that any muscle stretching also stretches the GTO → uses to detect increased tension exerted on tendon
there is change detected then there is signal sent on the afferent nerve to the CNS WHICH IS CONNECTED TO the same muscle fibre as the same muscle
This prevent injury which allows the muscle to relax
IN ORDER TO EXERT GREATER FORCE, NEED TO OVERCOME OBSTACLES PRESENTED BY THE GOLGI TENDON ORGAN
this means that if you want to try to push yourself you need to over come this nerve saying to stop
Three path ways
Groups of Muscles
Anterior (QARP)
→ The quadriceps group
→ The rotator cuff group
→ The abdominals groups
→ The pectoral muscles
Posterior (CHaRGE)
→ the erector spinae group
→ The rhomboids
→ The gluteal (the “glutes”)
→ The hamstring group
→ The calf muscles
Gastrocnemius
Intersection: Posterior surface of calcaneus
Origin: lateral and medial condyles of the femur
Purpose: plantarflexes foot at ankle, flexes leg at knee joint
Soleus
Intersection: Posterior surface of calcaneus
Origin: head of fibula and medial boarder of tibia
Purpose: foot plantar flexion
Together they do plantar flexion of the foot
Clinical
Three Metabolic Pathways
| ATP-PC | Glycolysis | Cellular Respiration |
Energy Source | Creatine Phosphate | Glucose | Mitochondria |
Oxygen | Anaerobic | Anaerobic | Aerobic |
ATP Molecules | 1 | 2 | 36 |
Duration of Activity | 10-15 second | 15 second to 3 minutes | 120 seconds and beyond |
Number of Chemical reactions | 1-2 (ATP à Creatine or creatine à ATP) | 11 | Glycolysis, Krebs cycle, and electron transport chain |
By-products | None | Lactic acid | Water and carbon dioxide |
Types of Activity | Power surges and speed events | Intermediate activity | Prolonged activity |
Types of Exercises that rely on the system | Sprints, jumping, weightlifting | 200-800 metre runs; shift in hockey; swim | Marathons |
Advantage | Very quick surges of power | Quick surge of power | Long duration; complete breakdown of glucose |
Limits of energy system | Short duration; muscles store small amount of ATP and Creatine Phosphate | Buildup of lactic acid causes pain and fatigue | Slow, requires large amount of oxygen |
Type of Joint
UNDER THE JOINT IN THE BONE SECTION
Treatment of Injuries
Shoulder Dislocation
Femur Fracture
CTE
Concussion
ALL ABOVE
Age of Bones
Epiphyseal Plates and Lines
o Growth Plates: Allows for growth and is at the epiphyseal part of the plate, they are made up of a layer of cartilage, so this vanishes creating:
o Epiphyseal lines: This is because theses plates have fused (Ossified) so the growth has finished and is not possible (They fuse at around the age of late teens early 20s)
Older the 35 is when they start to go into a thinner part in the bones → they don’t grow as much → become arthritic
Asian, African, Caucasian
Maxillary Bone
They are the left and right parts of the bones that form the roof of the mouth → 16 upper teeth in adults
There are different arches in different races:
Hyperbolic: African
Parabolic: European
Round: Asian
Nose and Cheek bone
Nasal opening
African: more flaring
Asian: cheek Bones angled more forward
European: neither of those things
Male vs Female
o Male sacrum tilts forward, more of a “heart shape” and ilia closer together
o Q-angle is greater in females
o Greater then 90 degrees for the female anterior view
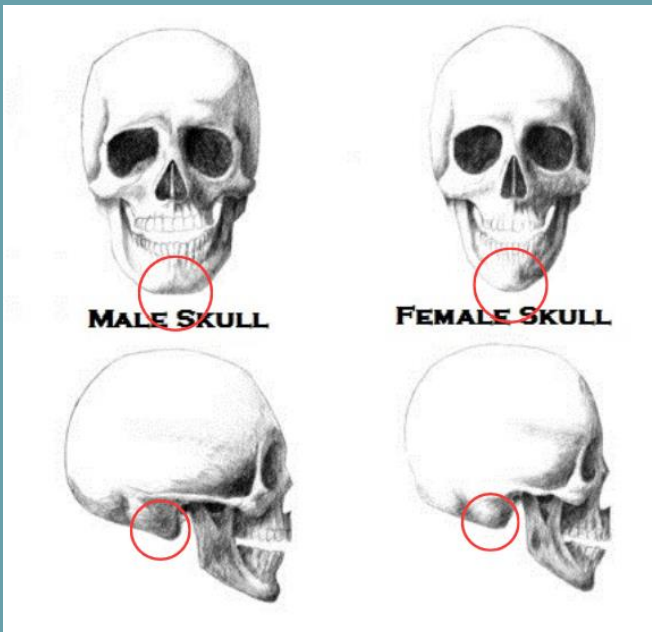
Skull Of Male Vs Female
Chin
F: Round
M: Square
Mastoid Process
F: Small
M: Large
External Occipital Protuberance
F: Small (Not Prominent)
M: Large (Prominent)
General Anatomy
F: Gracile
M: Robust
Forehead
F: Vertical
M: Receding
Brow Ridge
F:Slightly developed
M: Prominent
Muscle Lines
F: slightly developed
M: Prominent
Orbital Margins (Eye sockets)
F: Sharp
M: Rounded
Angle of Ascending Ramus (jaw line)
F: Obtuse
M: close to 90 degrees