BIO 207 Exam 3
Wednesday, June 5, 2024
Lecture 25- Immune System- Innate Immunity
General Host Defenses [Brock 21-24] (first line of defense)
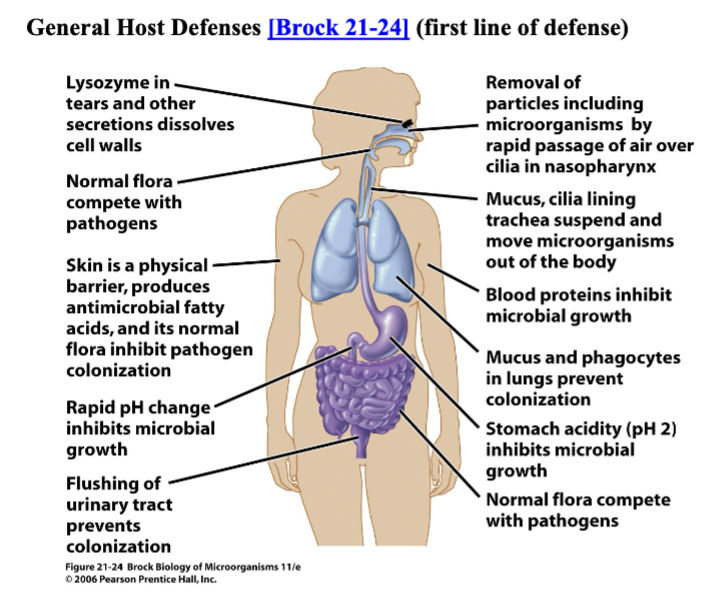
- Skin & Mucosal Surfaces
- organism must penetrate, adhere, grow
- there is tissue specificity for most infectious agents
- tight junctions in epithelial tissue seal off "inside" [figure 23.27]
- mucus limits direct access to epithelial cells
- breaks in epithelium allow microbes to bypass these barriers
- organism must penetrate, adhere, grow
- Normal Flora
- young are more susceptible before stable adult flora develops
- diet, drugs can alter normal flora
- Antimicrobial Secretions
- lysozyme & other enzymes kill bacteria in saliva and tears
- defensin proteins insert in microbial membranes [table 23.2]
- blood proteins sequester nutrients
- fatty acids on skin lower pH
- Physical Removal
- cilia/mucus movement
- urine flushing
- Stomach Acid
Components of the Immune System (participate in 2nd and 3rd lines of defense)
- Blood & Lymph Systems
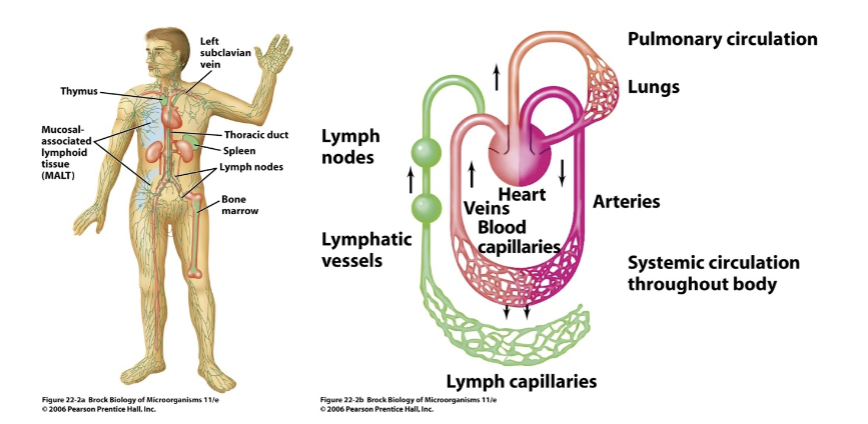
- interconnected circulatory systems [Brock 22-2a] [Brock 22-2b]
- blood is closed loop powered by heart
- lymph is a drainage system returning tissue fluid to blood
- series of collecting vessels starting with microscopic capillaries
- interconnected circulatory systems [Brock 22-2a] [Brock 22-2b]
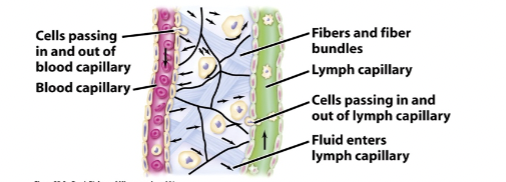
- fluid drains into lymph from surrounding tissue [Brock 22-2c]
- powered by skeletal muscle
- one-way valves keep lymph moving to chest
- white blood cells move in and out (extravasation)
- collect in lymph nodes [Brock 22-2d]
- kill bacteria, remove debris
- interact with other cells of immune system present there
- Organs/Tissues [figure 23.25]
- primary- where lymphocytes develop
- thymus & bone marrow
- secondary- where lymphocytes collect
- spleen, lymph nodes, tonsils, adenoids, appendix
- SALT, MALT, GALT- skin, mucus, gut-associated lymphoid tissue
- M cells in skin, tonsils, adenoids, intestines monitor flora [figure 23.28b]
- primary- where lymphocytes develop
- Blood cells (~45% of blood volume) [figure 23.18] [Brock T22-01]
- erythrocytes- red blood cells (not part of immune system)
- enucleated
- carry oxygen
- platelets- involved in clotting
- erythrocytes- red blood cells (not part of immune system)
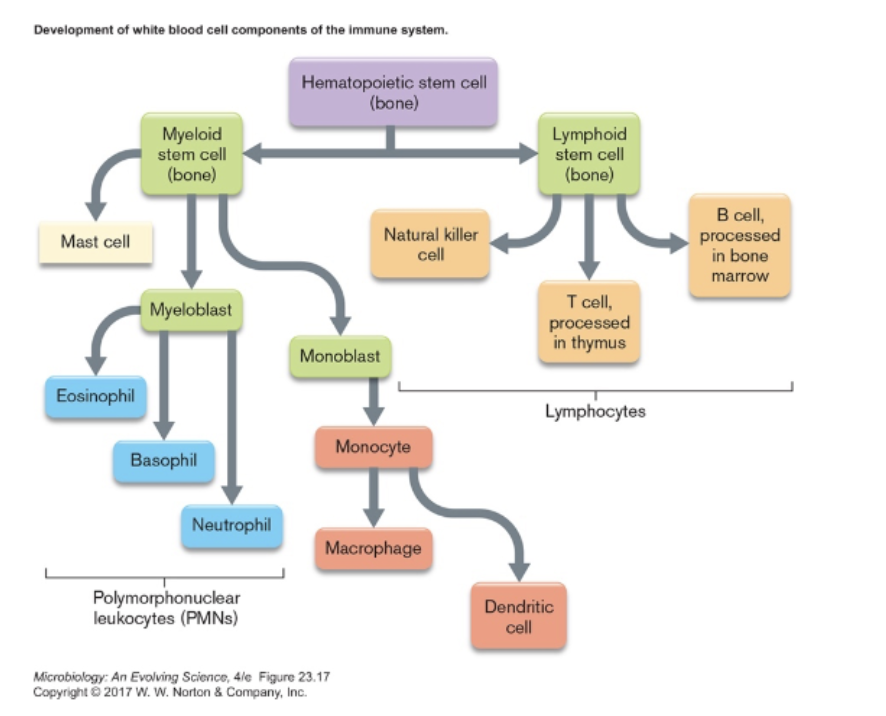
- leukocytes- white blood cells [figure 23.19] [figure 23.20] [table 23.1]
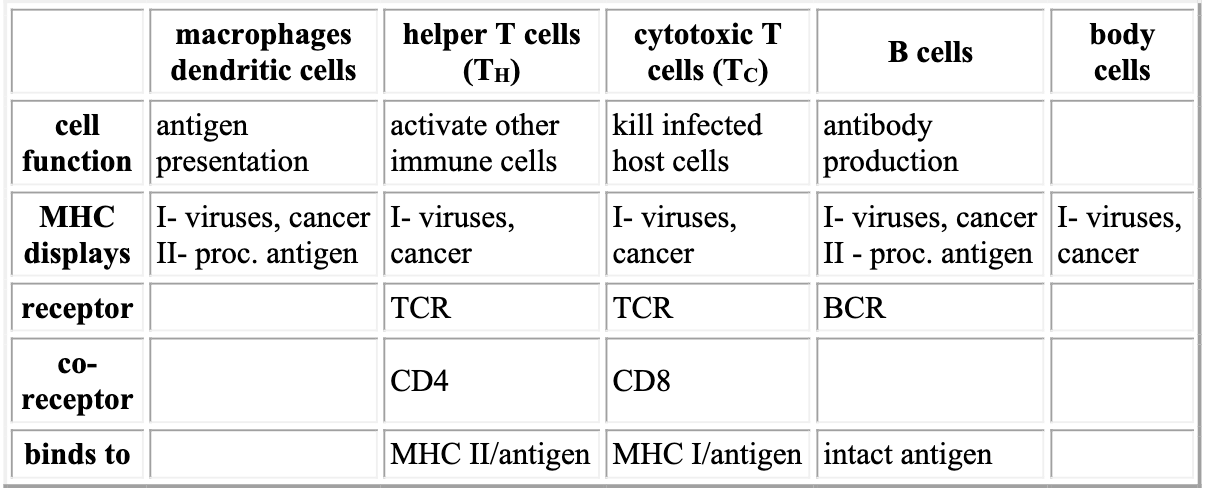
- monocytes, dendritic cells, macrophages- phagocytic, antigen-presenting cells (APCs)
- engulf foreign cells, viruses, proteins
- break these down & display foreign peptides on their surface
- monocytes circulate in blood
- dendritic cells & macrophages attach to different tissues [figure 23.22]
- polymorphonuclear leukocytes (PMNs or granulocytes, in blood)
- neutrophils- phagocytic cells, migrate to site of infection
- can use Neutrophil Extracellular Trap (NET) to kill cells [figure 23.21]
- eosinophils- anti-protozoan secretions
- basophils- inflammation mediator
- mast cells- mediate inflammation throughout body, not in blood [figure 24.11]
- lymphocytes (mostly in spleen and lymph nodes)
- natural killer cells- kill infected or cancerous cells [figure 23.23]
- T cells- central to adaptive immunity
- B cells- part of adaptive immunity, produce antibodies
- monocytes, dendritic cells, macrophages- phagocytic, antigen-presenting cells (APCs)
- leukocytes- white blood cells [figure 23.19] [figure 23.20] [table 23.1]
- Plasma proteins, soluble in fluid portion of blood (~55% of blood volume)
- fibrinogen- clotting
- antibodies
- complement
- iron sequestration & other antibacterial proteins
Innate Immunity (second line of defense)
- Inflammatory Response [figure 23.32] {anim 23.01}
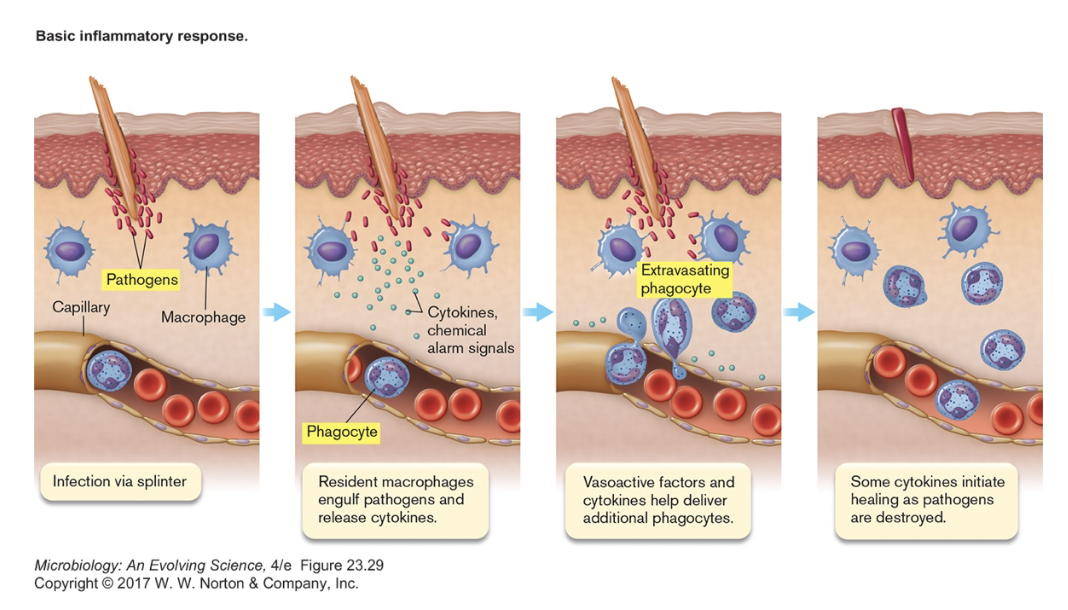
- a non-specific response to wounds & infection
- signs described 2000 years ago
- redness (rubor) heat (calor) pain (dolor) swelling (tumor)
- Detection [figure 23.33] [table 23.3]
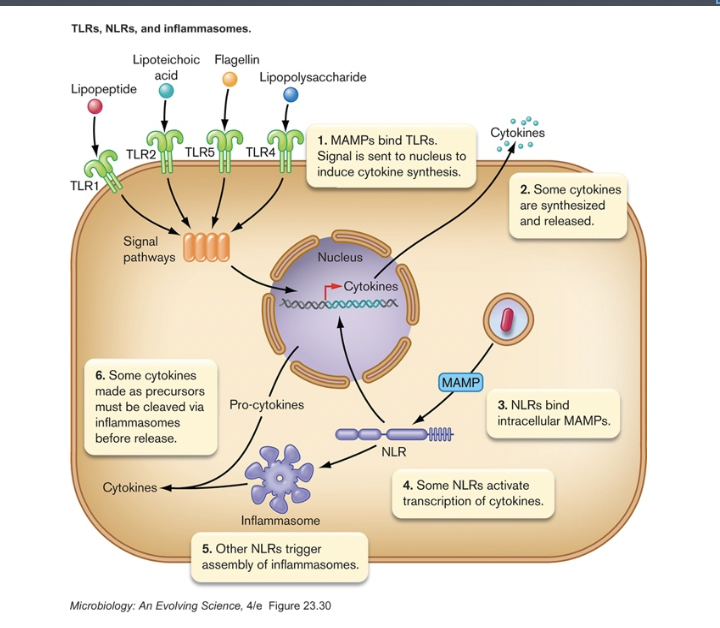
- triggered by unique signals of invader (MAMPs, microbe-associated molecular patterns)
- bind to Toll-like receptors (in membrane) or Nod-like receptors (in cytoplasm)
- cause transcription and release of cytokines [table 24.4]
- Clotting
- clotting factors released by platelets
- attempt to contain infection
- Phagocytosis [figure 23.20] [figure 23.36] {anim 23.02}
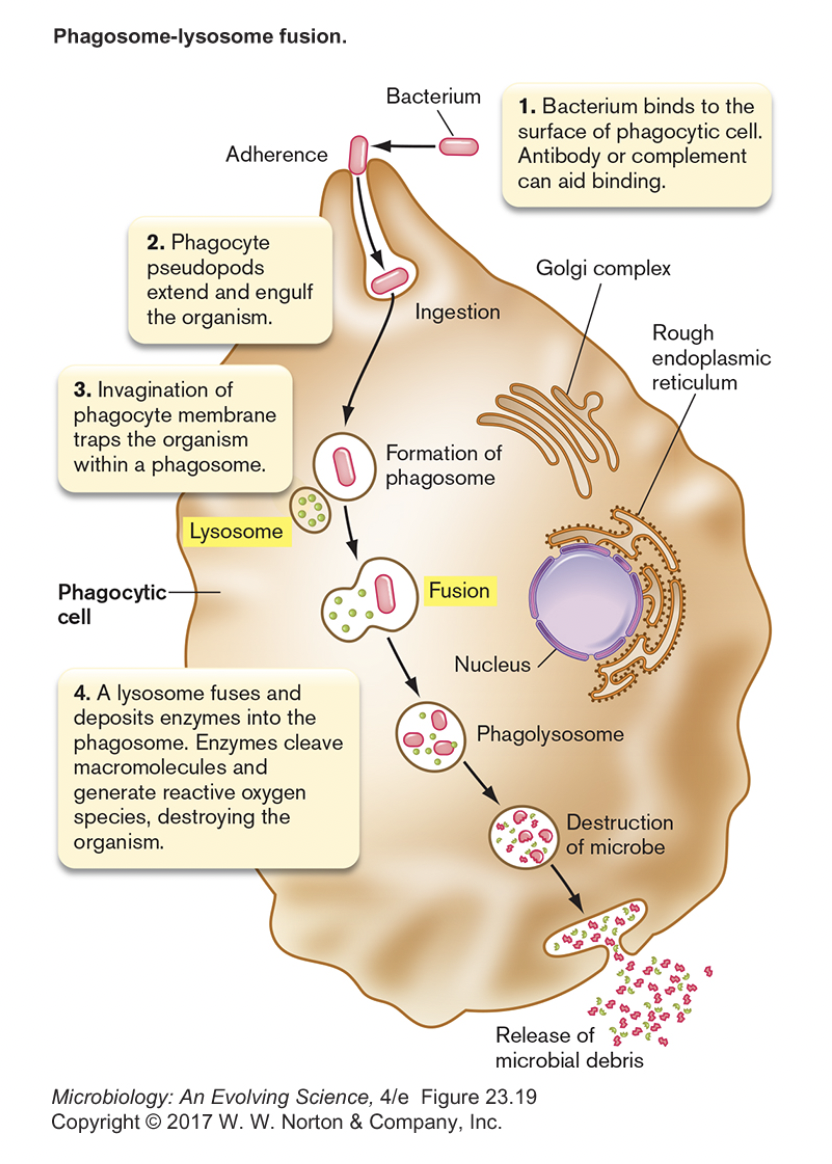
- phagocyte (macrophage) engulfs microbe
- invader is recognized because it does not have self-antigen (CD47)
- some pathogens can avoid because of capsule
- antibodies can increase phagocytosis (opsonization) [figure 23.37]
- microbe is killed/digested in phagolysozome
- multiple pathways used
- some pathogens resistant to digestion
- peptides from invader may be displayed on phagocyte surface (antigen presentation)
- peptide release can stimulate/attract other leukocytes
- macrophages also release (and are activated by) cytokines [table 24.4]
- phagocyte (macrophage) engulfs microbe
- Extravasation brings neutrophils from nearby capillaries [figure 23.35]
- cytokines cause local endothelial cells to make selectins
- selectins/integrin/ICAM-1 retain passing neutrophils from circulating blood
- bradykinin from damaged host cells loosens connections between endothelial cells
- allows neutrophils to squeeze out
- attracted to wound by chemokine gradient
- triggers mast cells in tissue to release histamines
- causes vasodilation (blood volume increases), bringing more cells
- vessel wall permeability increases, leading to edema (fluid buildup)
- triggers prostaglandin release → pain
- aspirin and related pain relievers prevent prostaglandin synthesis
- allows neutrophils to squeeze out
- Inflammation summary
- benefits of inflammation
- increased blood volume brings in more antimicrobial agents
- increased temperature makes phagocytes more efficient, may inhibit bacteria
- clot may isolate area of infection
- downside of inflammation
- may release nutrients & promote bacterial growth
- microbe can gain access to further tissue via blood vessels
- high fever can harm host
- chronic inflammation damages host tissue
- benefits of inflammation
Complement System [figure 23.40]
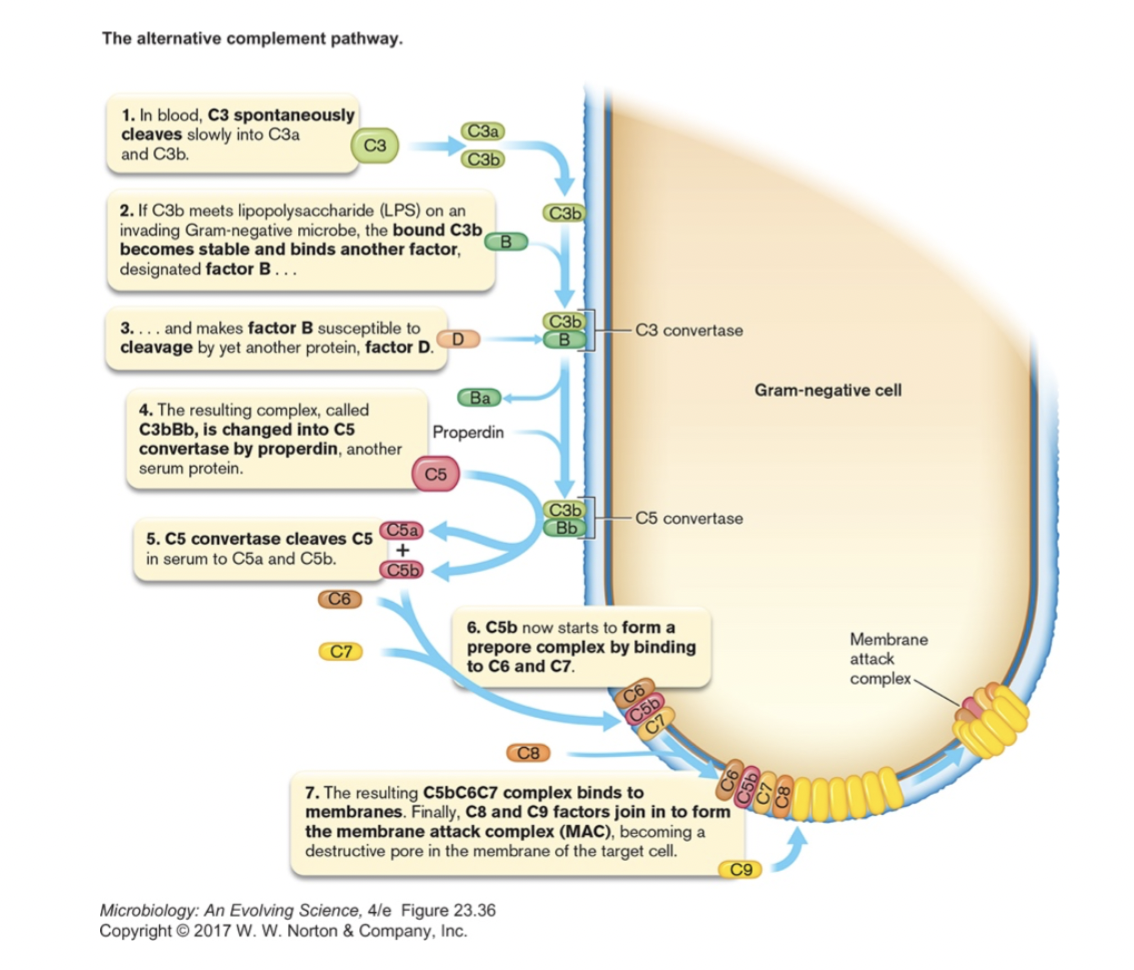
- serum proteins that can work with or independent of antibodies to kill bacteria
- cascade of protein interactions leads to pores forming in bacterial membrane
Lecture 26- Immune System- Adaptive Immunity 1
Immunoglobulin Superfamily Proteins
- Antibodies = secreted proteins that bind antigen
- have the following structure in common [figure 24.8b] [figure 24.9]
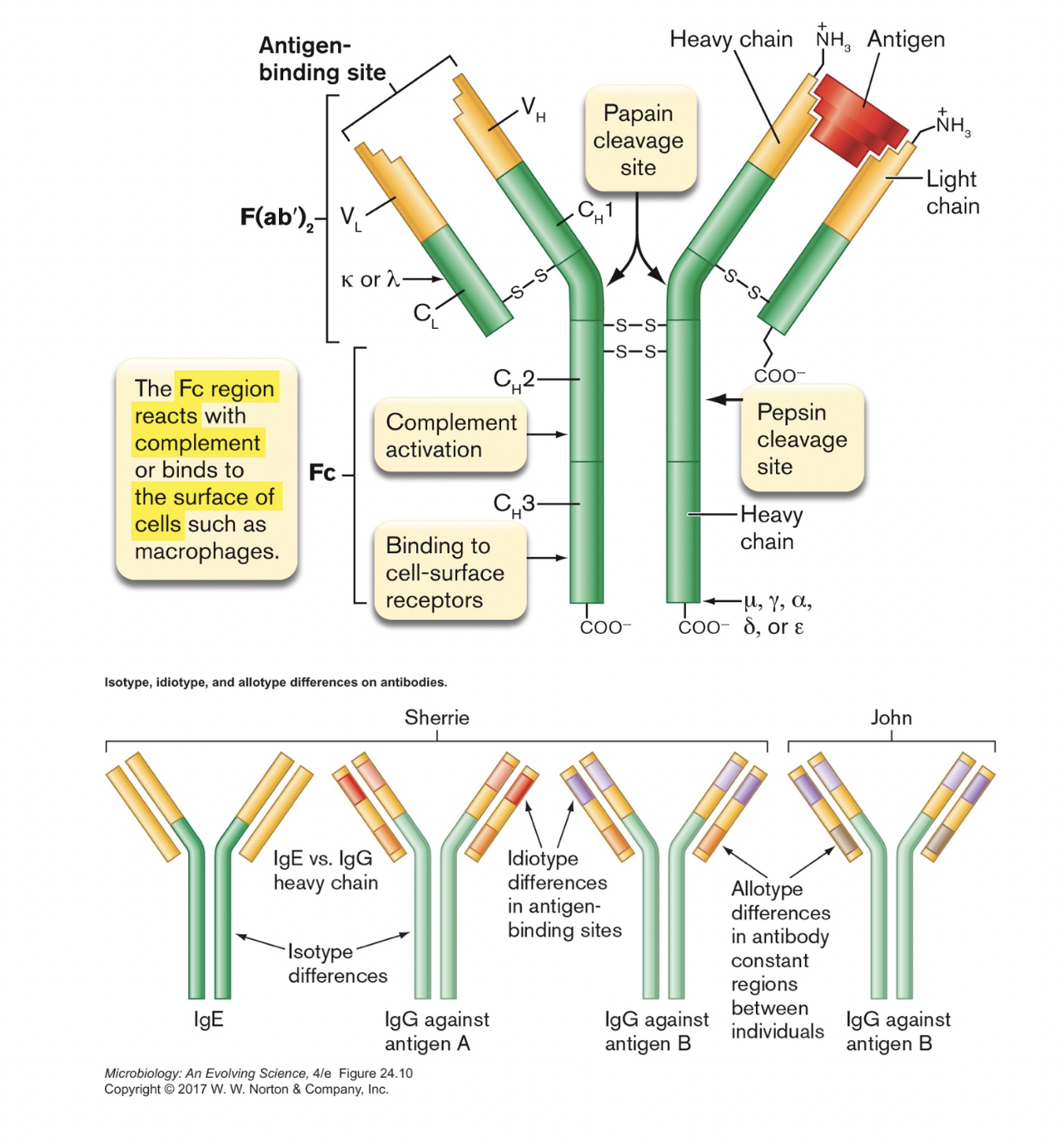
- four polypeptide chains, 2 light & 2 heavy, held together by disulfide bonds
- each chain has constant (C) and variable (V) regions
- C regions are the same for that individual/chain (allotype) and class (isotype)
- i.e., all IgG light chain C regions in an individual are the same
- V regions are unique to each antibody (idiotype)
- antigen binding domains are formed by V regions of 1 H and 1 L chain
- on a given antibody, all binding domains bind the same antigen
- antigen= whatever antibody binds to, usually protein (carbohydrate,lipid,DNA)
- epitope = the specific part being bound [figure 24.2]
- four polypeptide chains, 2 light & 2 heavy, held together by disulfide bonds
- five different classes of antibody (in humans) [table 24.2]
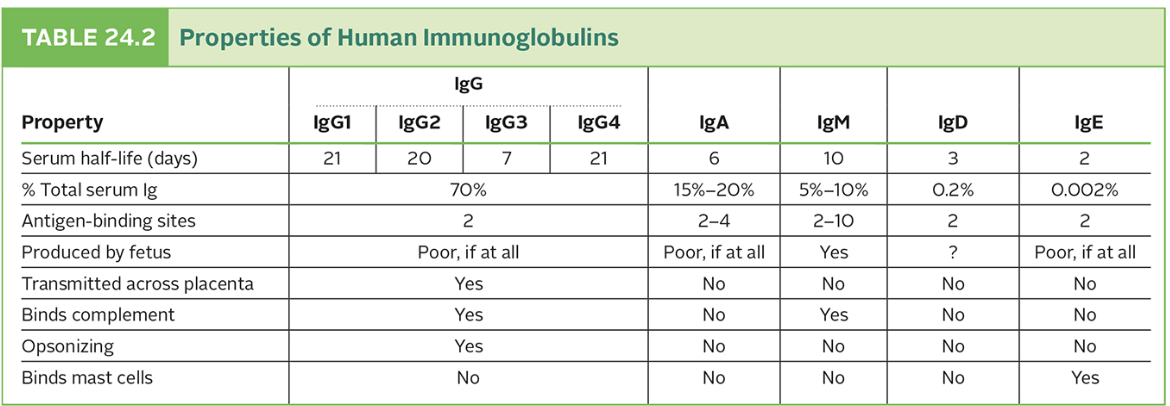
- IgG [figure 24.8b]
- IgG is bivalent, will bind 2 of the exact same antigen
- IgG is found in blood serum
- classic Y-shape
- IgM
- five antibody proteins held together [figure 24.10a]
- longer constant domain
- generally the first Ig made in immune response
- IgM monomers in B cell membrane bind antigen, help bring it in for presentation
- IgA
- two antibodies held together [figure 24.10b]
- common in body secretions (tears, breast milk, mucus, etc.)
- IgE
- longer constant domain (has C H 4)
- binds to mast cells
- important in allergic reactions
- IgD
- helps antigen bind to B cells
- IgG [figure 24.8b]
- Major Histocompatibility Complex (MHC) proteins exist in plasma membrane of host cells
- unique to individual, help determine "self" (HLA type)
- important in transplant rejection
- two types, both will bind and display antigens [figure 24.19]
- binding of antigen depends on shape of two variable regions
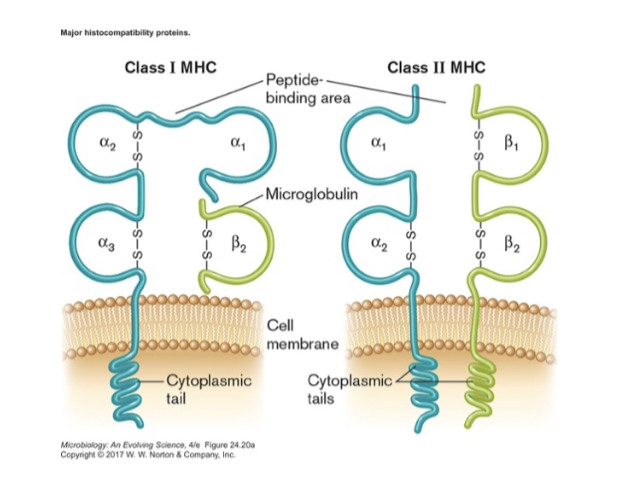
- Class I- all nucleated cells
- alerts immune system that cell is infected
- Class II- B cells and antigen-presenting cells (APCs)
- tells other immune cells that APC has found a foreign antigen
- Class I- all nucleated cells
- unique to individual, help determine "self" (HLA type)
- T cell receptor (TCR) is (structurally) similar to MHC but only found on T-cells [figure 24.21]
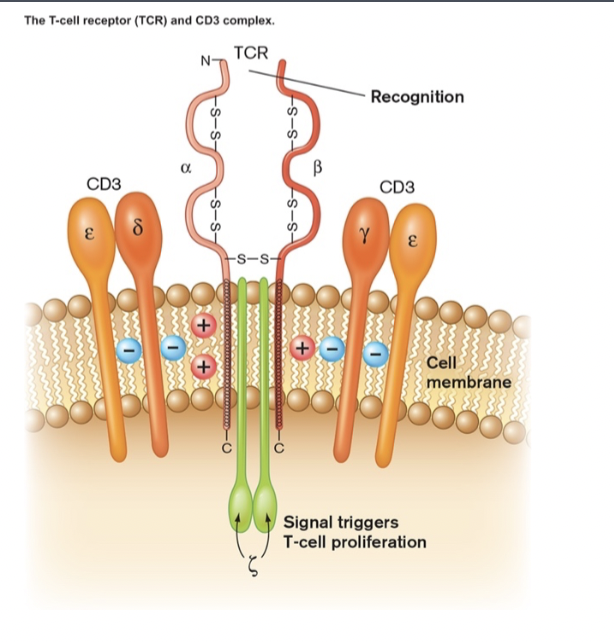
- each T cell has roughly 100,000 copies of one particular type of TCR
- each type of TCR will bind only one antigen (with limited cross-reactivity to others)
- variable region is different in each cell, ensuring a range of TCR binding specificities
- each T cell has roughly 100,000 copies of one particular type of TCR
- B cell receptor (classic antibody sitting in membrane of a B cell) and antibodies also belong to this family of proteins [figure 24.14]
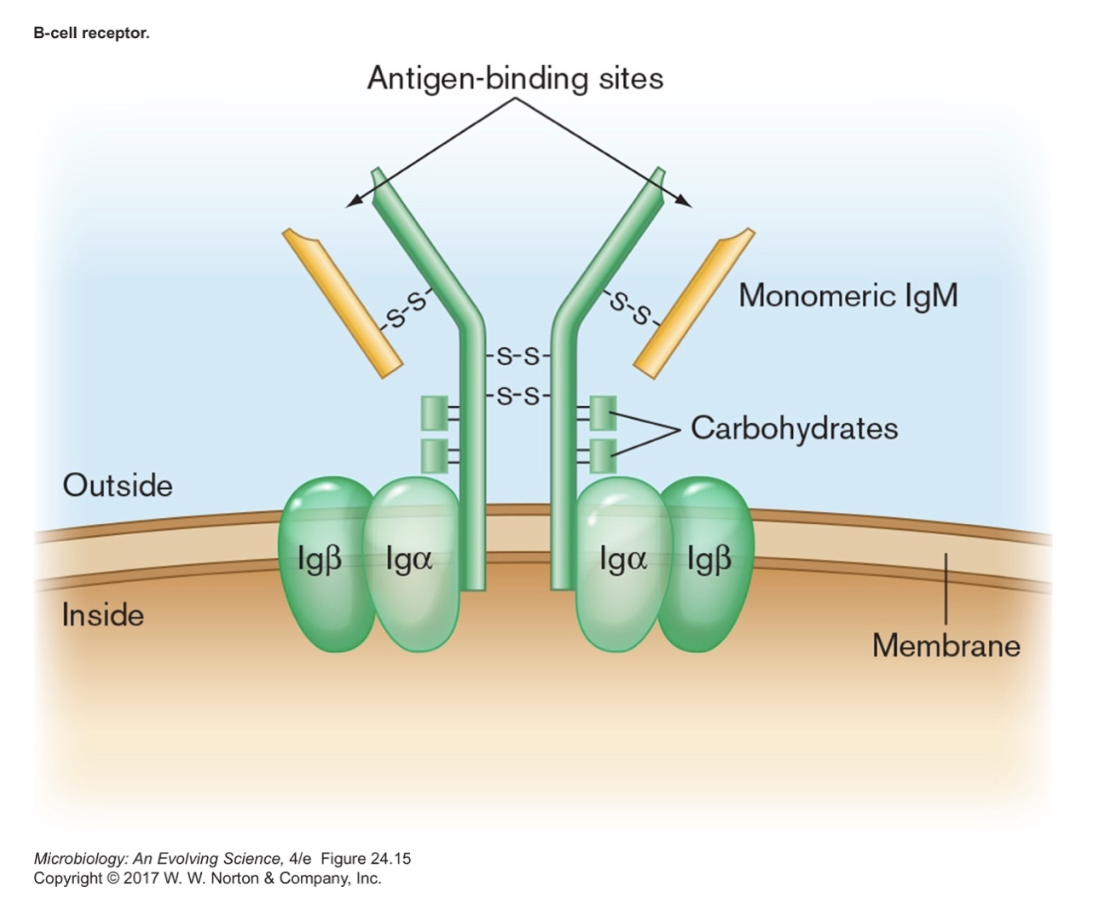
- antibodies are secreted by activated B cells (see below)
- BCR has extra domain in tail to insert into membrane
- Receptor interactions
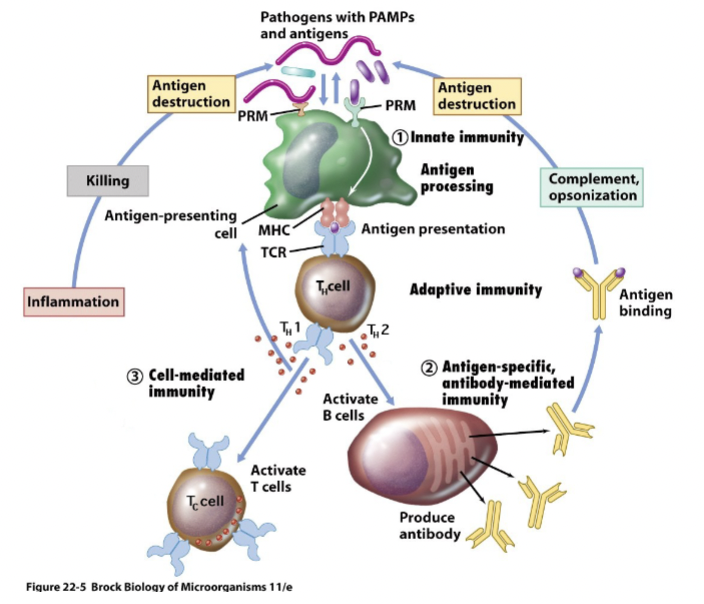
Adaptive Immunity (third line of defense)
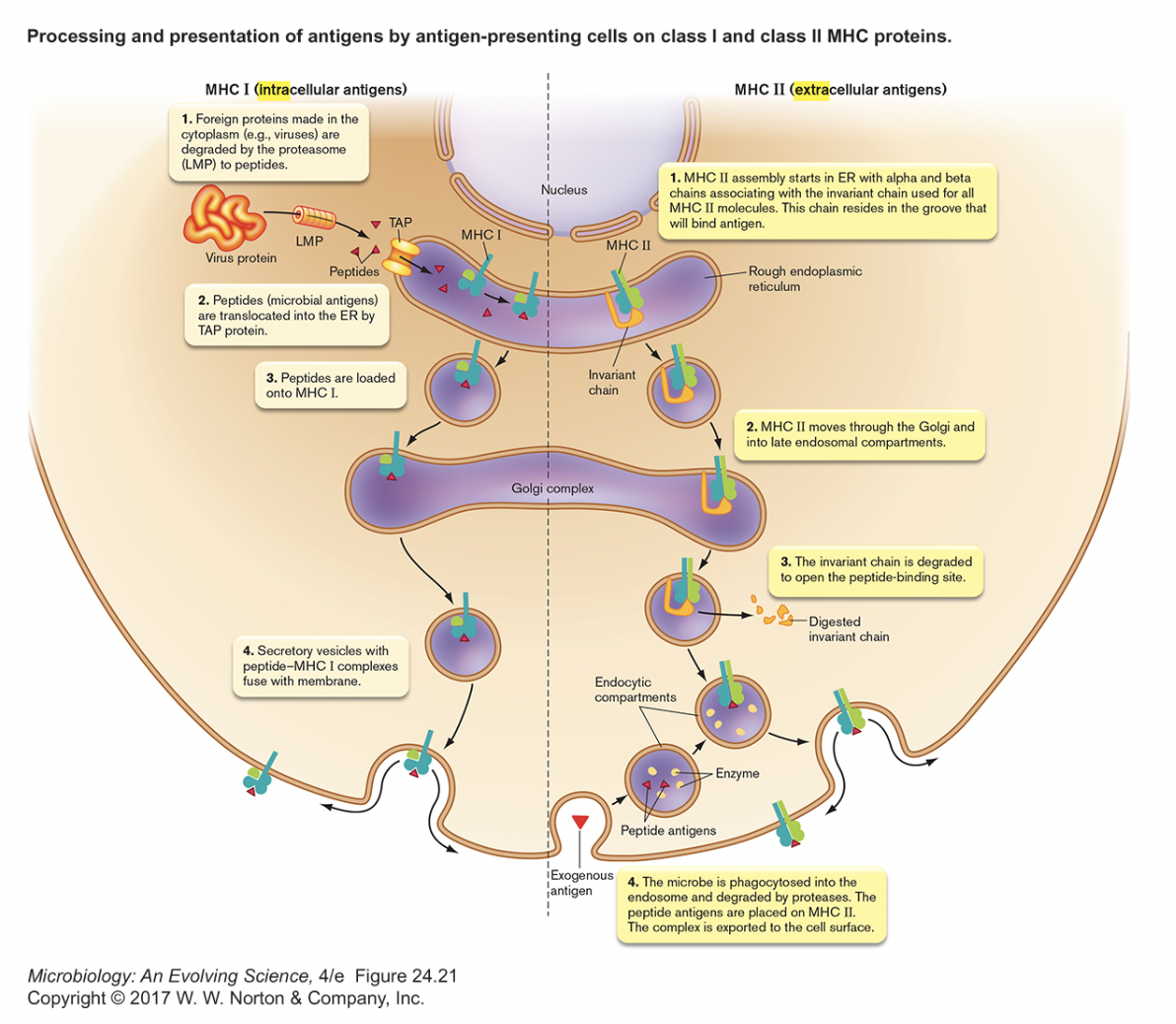
- Antigen Presentation [figure 24.20]
- to some degree all cells are capable of "antigen presentation"
- all cells display internal antigens in class I MHC
- if antigens are foreign (viral or cancerous) → activate T C (cell-mediated immunity)
- only "true" APCs (dendritic cells, macrophages, B cells) process external antigens
- take in, break down and display antigens on surface of APC in class II MHC
- immunogenicity of antigen depends on
- exceeding minimum size (5-100 a.a.?)
- molecular complexity (proteins > carbohydrates > lipids & nucleic acids)
- form (soluble or insoluble)
- dosage (not too high, not too low)
- route of introduction (injection better than ingestion)
- self/non-self (self should not provoke immune response)
- response is only to small part of immunogen (4-6 a.a.)
- called antigenic determinant or epitope
- a single protein has hundreds of potential epitopes
- immunogenicity of antigen depends on
- take in, break down and display antigens on surface of APC in class II MHC
- to some degree all cells are capable of "antigen presentation"
Tuesday, June 11, 2024
Lecture 26- Immune System- Adaptive Immunity 1
Adaptive Immunity (third line of defense)
- Activation of T-helper (TH 0) cells [figure 24.22] {anim 24.01}
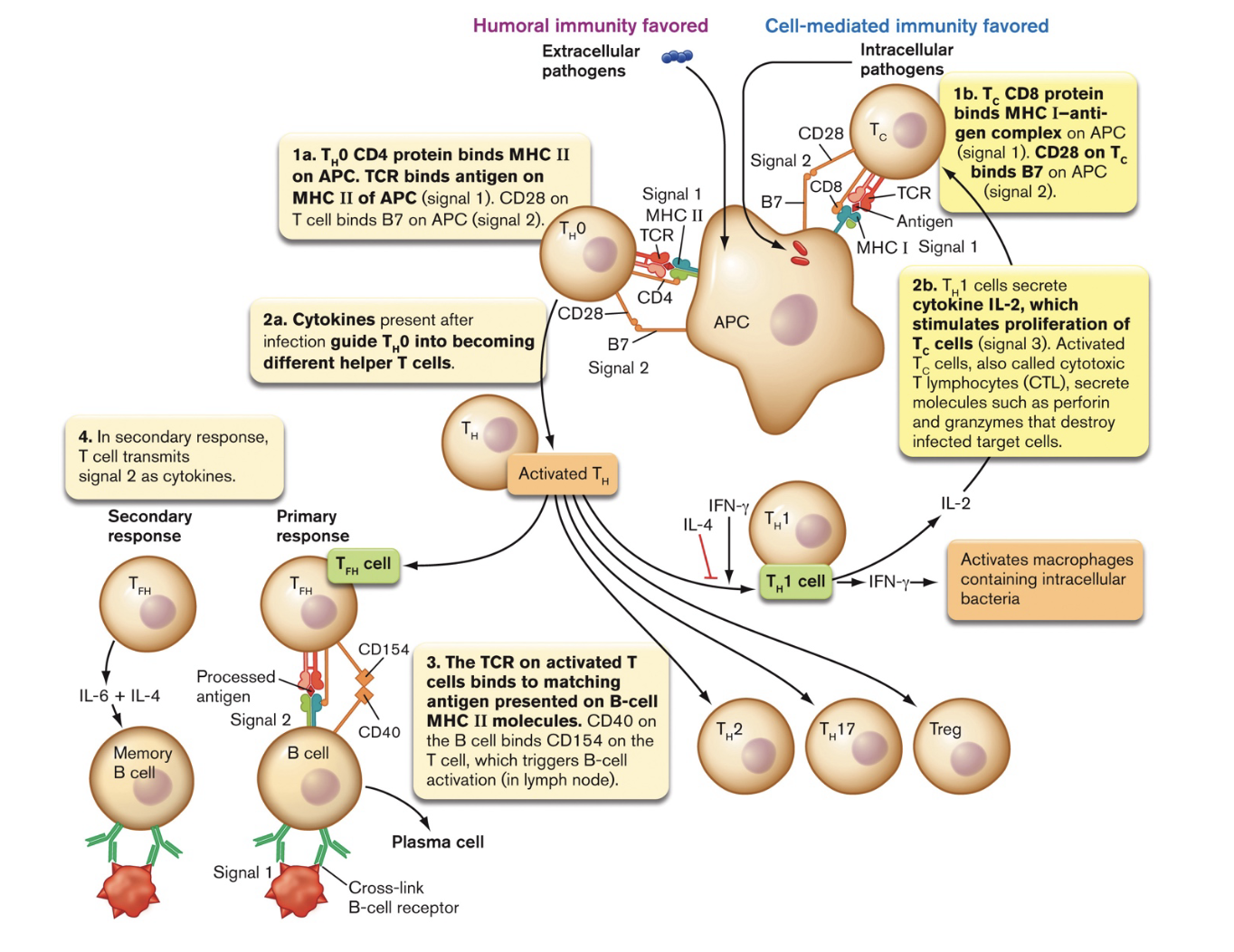
- a naive T-helper cell (T H 0) recognizes the foreign antigen/class II MHC via its T-cell receptor (TCR) and CD4 co-receptor
- binding of B7 & CD28 serves as confirmation signal
- APC releases cytokines, triggering development of T H 0 [table 24.4]
- a naive T-helper cell (T H 0) recognizes the foreign antigen/class II MHC via its T-cell receptor (TCR) and CD4 co-receptor
- Cell-Mediated Immunity
- effective against virally infected cells or cancerous host cells
- operates via activated cytotoxic T-cells (TC )
- TC cell recognizes the foreign antigen/class I MHC on APC via its T-cell receptor (TCR) and CD8 co-receptor
- binding of B7 & CD28 serves as confirmation signal
- IL-2 secreted by T H 1 induces proliferation of T C cells
- activated T C kills infected host cells
- TC cell recognizes the foreign antigen/class I MHC on infected cell via its T-cell receptor (TCR) and CD8 co-receptor [figure 24.24a]
- in this case, no binding of B7 & CD28
- signals to TC cell that it is binding to an infected cell, not an APC
- binding results in secretion of cell killing proteins [figure 24.24b]
- perforin- protein which inserts in infected cell membranes, makes pore
- granzymes- proteins which trigger apoptosis, programmed cell death
- TC cell recognizes the foreign antigen/class I MHC on infected cell via its T-cell receptor (TCR) and CD8 co-receptor [figure 24.24a]
- proliferation is selective, i.e., only T C cells with TCR fitting foreign antigen are activated
- activation will only occur if APC is also activating nearby T H 1
- activated T H 1 will also bind to macrophages via TCR and secrete cytokines that activate macrophages and promote inflammation [Brock 22-13b]
- Humoral Immunity
- effective against any pathogen outside a host cell (viruses, bacteria, protists, etc.)
- operates via differentiated B-cells
- can happen two ways [figure 24.16]
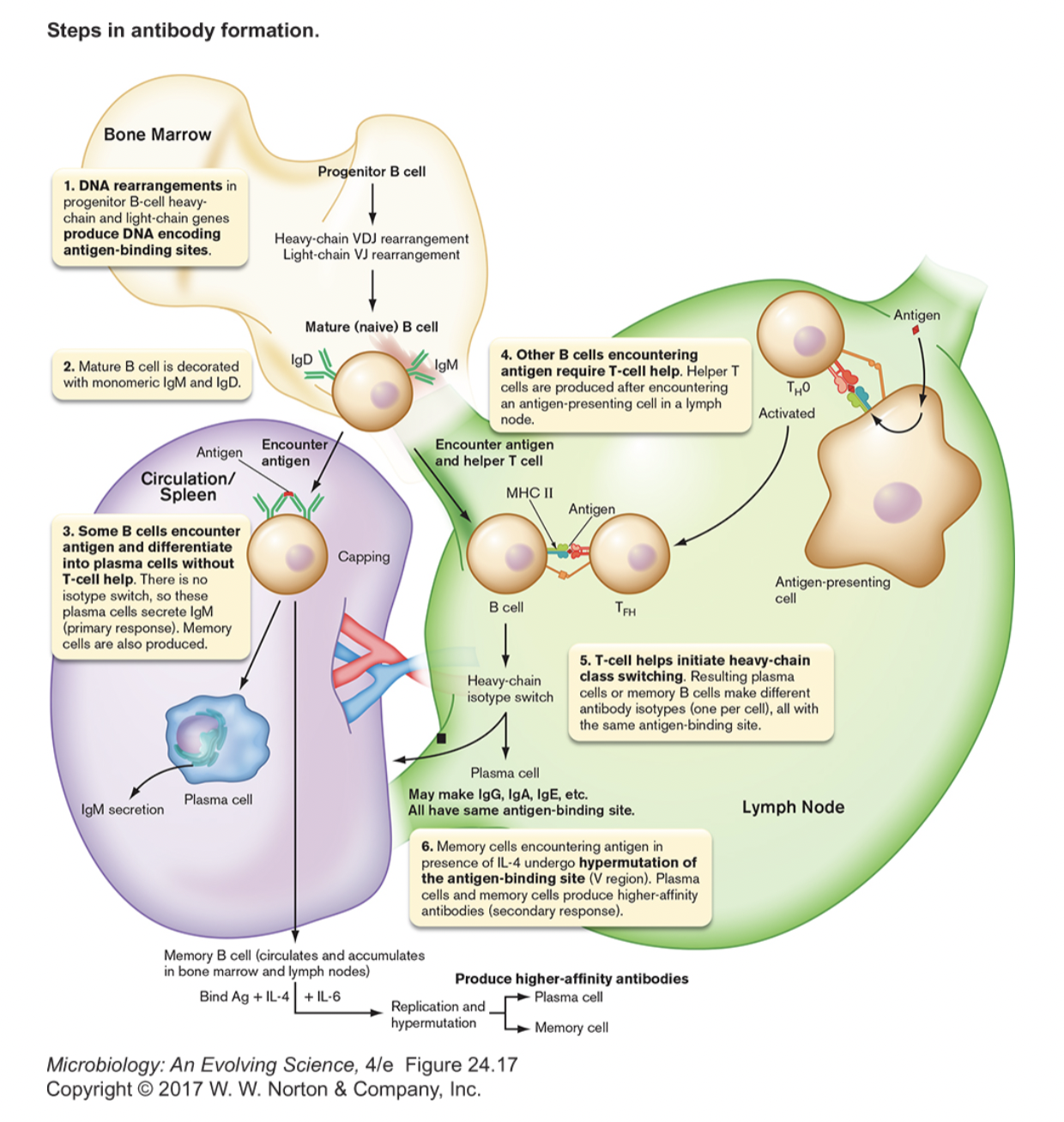
- direct encounter of antigen [figure 24.15]
- antigen binding to B-cell receptor (BCR) causes clustering (capping)
- B-cell differentiates into plasma cells (secrete IgM) and memory cells
- interaction with T FH / TH 2 [Slon5, figure 24.3] [Brock 22-14]
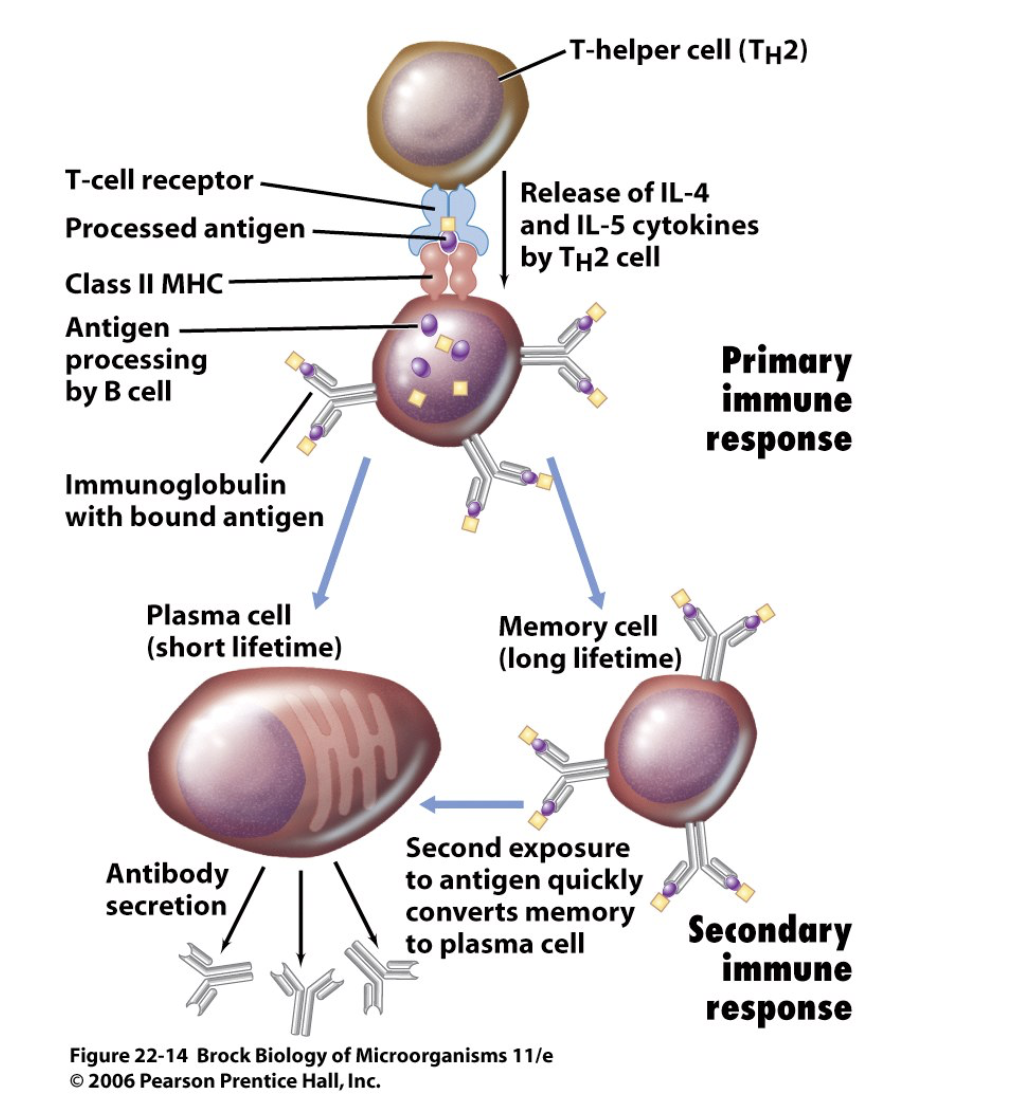
- B cells can act as APCs and display antigens in class II MHC
- TFH / TH 2 cell recognizes the foreign antigen/class II MHC on B cell via its T-cell receptor (TCR) and CD4 co-receptor
- binding of CD154 & CD40 serves as confirmation signal
- TFH / TH 2 cell releases cytokines that initiate B cell differentiation
- class-switching of heavy chains occurs (all classes possible) [figure 24.18]
- new cells all recognize same antigen (clonal selection)
- plasma cells- secrete antibodies
- memory cells- long lived B cells
- don't secrete antibodies
- exist to ensure faster, stronger response to second exposure
- higher number of B cells specific for that antigen after first exposure
- don't require TH activation to convert to plasma cells, just binding to BCR
- hypermutation of variable region may give even higher affinity antibodies
Lecture 27- Immune System- Adaptive Immunity 2
Review [figure 24.3] [Brock 22-5] {anim 24.01}
- APCs & Helper T-cells
- Cell-Mediated Immunity
- Humoral Immunity
- What the immune system can do
- respond to anything, even if never encountered before (antibody/receptor diversity)
- strengthen its response upon encountering something (clonal proliferation and memory)
- discriminate between self and non-self (clonal deletion)
What Happens When a Virus Infects a Person?
- Exposure to the virus
- Virus enters those cells with the proper receptor, begins replicating
- new viruses produced → free (extracellular) virus particles
- but also some viral antigens will be displayed on surface of infected cell by MHC I
- Macrophages and other APCs (including B cells) will engulf free virus particles
- APCs typically encounter virus in spleen, lymph node, other specialized tissue
- display viral antigens in MHC II and MHC I
- A few TH 0 cells will have a TCR that fits the combination of MHC II/antigen on APC
- TH 0 cells bind to APC via TCR and CD4
- causes APC to release cytokines, causing that specific T H cell to proliferate
- can differentiate into T H 1 and/or TH 2 depending on cytokines present
- in either case, more copies of T H with TCR recognizing that particular viral antigen
- activated T H cells will release cytokines as well
- Separately, a few T C cells will have a TCR that fits MHC I/antigen on APC
- TC cells bind APC via TCR and CD8
- activated T H 1 cells induce proliferation of that specific T C cell
- therefore, more copies of T C with TCR recognizing that viral antigen
- TC cells migrate to site of infection
- TC cells bind to virally infected cell via TCR and CD8
- causes TC cell to release proteins that kill the infected cell
- Separately, a few B cells will have a BCR that fits free virus
- B cells will engulf virus particles and display viral antigens in MHC II
- TH 2 cells bind to B cell via TCR and CD4
- activated T H 2 cell induces differentiation of that specific B cell
- makes plasma cells make lots of antibody specific for that viral antigen
- and makes memory cells for that viral antigen are defense against future infection
- Eventually, infection is brought under control by
- TC cells killing virally infected cell
- antibody neutralization of free virus
- Review Lecture 26 notes and then come back to this ^^^ and review it
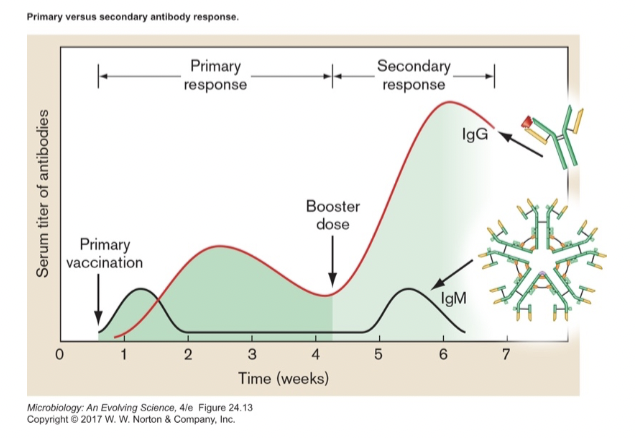
- Reinfection leads to rapid secondary response [figure 24.12]
Function of Antibodies [antibodies]
- Virus or toxin neutralization [figure 24.7]
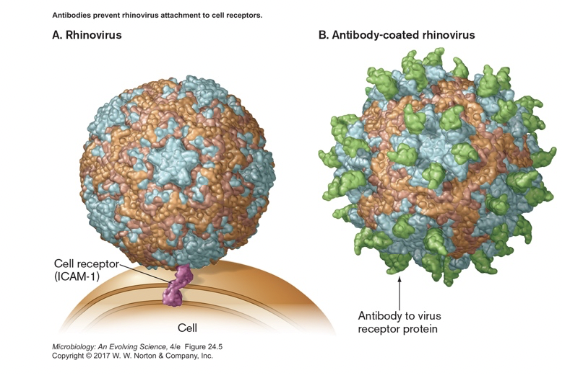
- bind to viral surface or toxin
- prevent intended interaction of virus or toxin with host
- Agglutination/Precipitation [Slon4, figure 24.8]
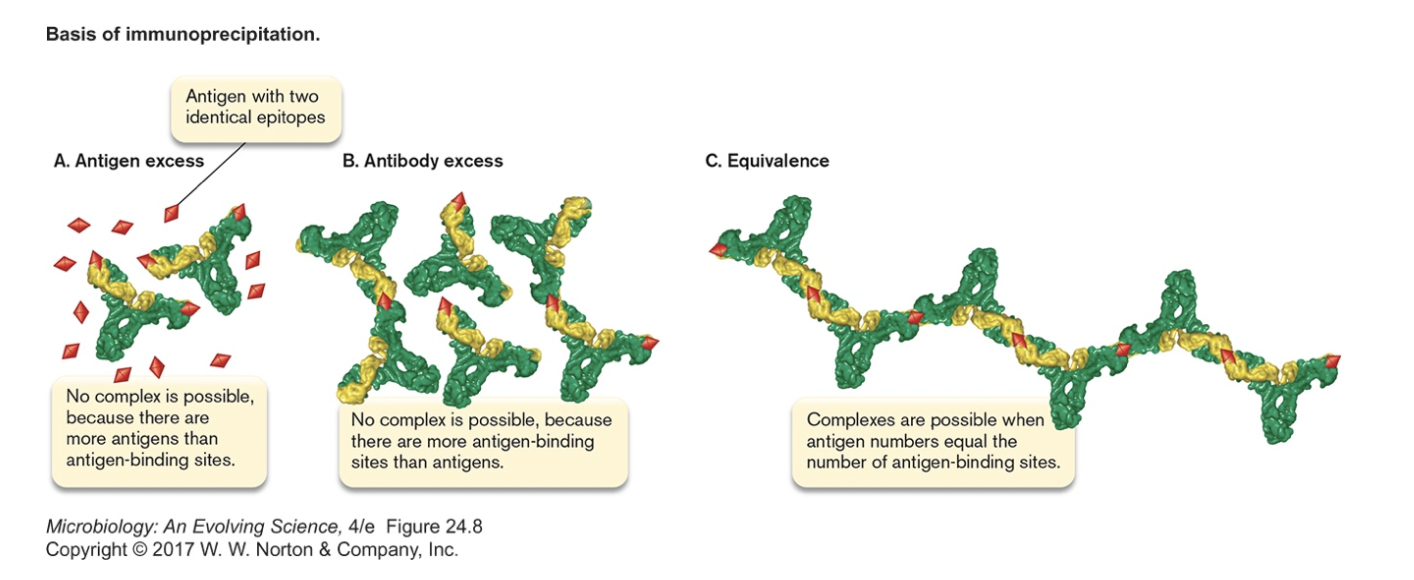
- clump antigens together
- if soluble antigen, may cause it to precipitate
- Activate complement system of proteins [figure 24.27]
- antibody bound to bacterial cell surface triggers binding/cleavage of complement proteins
- cleaved complement proteins cause inflammation
- other fragments of complement proteins insert into membrane
- pores form, cell dies
- doesn't work for Gram positives
- Opsonization [figure 23.37]
- antibodies and complement on cell surface "flag" cell for phagocytosis
- works for all bacteria
- can also clump cells or toxin molecules leading to easier phagocytosis
- antibodies and complement on cell surface "flag" cell for phagocytosis
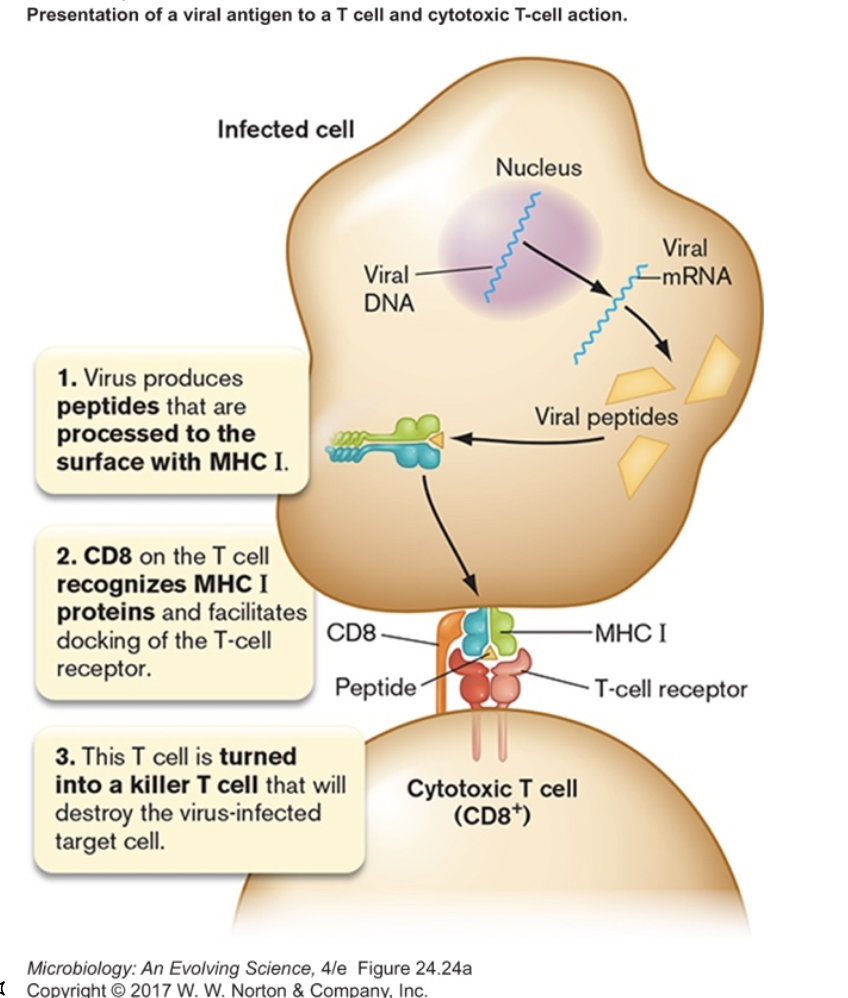
Generation of Antibody Diversity
- Each B cell produces only one kind of antibody
- Ability to respond to anything out there depends on millions of different B cells, millions of different antibodies
- Antibodies are proteins, does this mean there are millions of different antibody genes?
- NO, diversity is created by uniquely splicing DNA segments in each B cell [figure 24.17]
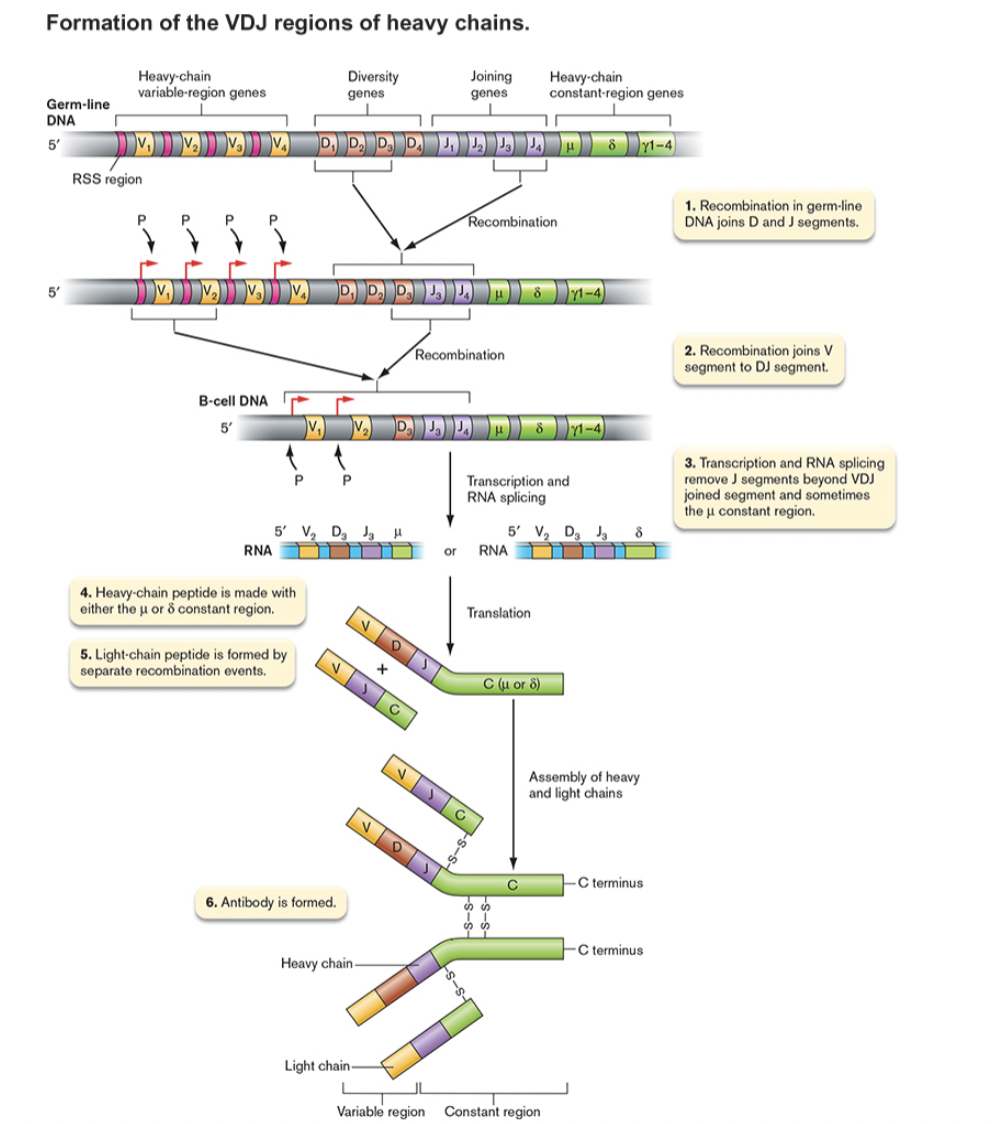
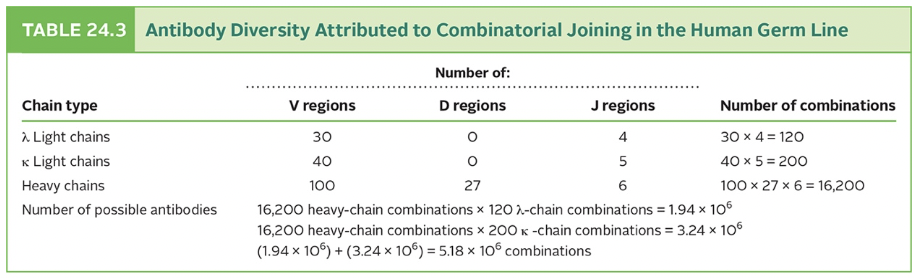
- multiply the segments to realize the possibilities [table 24.3]
- remember that C region determines class, is not involved in antigen binding
- 320 light chains x 16,200 heavy chains = > 5 million binding specificities
- even more variation because of
- imprecise joining of segments
- high mutation rate during B cell proliferation
- multiply the segments to realize the possibilities [table 24.3]
- Similar processes result in TCR diversity
Immunization & Vaccines [Brock T22.3]
- Natural active immunity (disease exposure)
- infection leads to immune response, boost in memory cells (takes weeks)
- second exposure results in stronger, faster response
- Artificial active immunity (vaccination) [table 24.1]
- vaccination leads to immune response (takes weeks)
- whole organism- killed or attenuated
- subunit- natural, modified or recombinant
- hapten + carrier molecule- when antigen is too small on its own [Slon5, figure 24.6]
- second exposure (or booster) results in stronger, faster response
- vaccination leads to immune response (takes weeks)
- Natural passive immunity (maternal immunity)
- antibodies are received from mother through placenta, breast milk (instant protection)
- no host immune response, no boost for later exposure
- Artificial passive immunity (antitoxins)
- injection of antibodies from another individual or animal (instant protection)
- used against toxins
- no host immune response, no boost for later exposure
Immune Disorders
- Allergies can be an overreaction of the immune system [figure 24.30] [table 24.6]
- Autoimmune diseases- the immune system attacks self-antigens [figure 24.32] [table 24.7]
- Superantigens can activate T cells indiscriminately and destabilize the system [figure 24.26]
Clonal Selection in recognition of self and non-self
- Each B & T cell makes a unique antibody or TCR
- When binding to antigen, proliferation occurs [figure 24.13] [Brock 23-8]
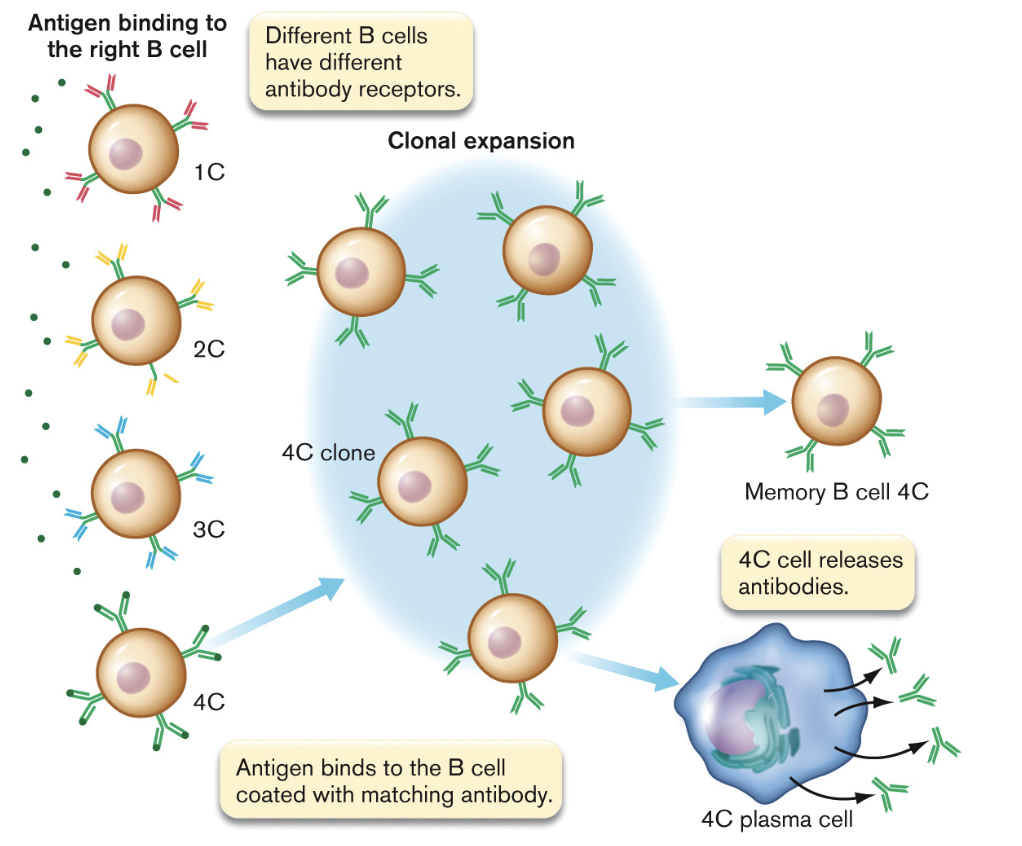
- a clonal line is expanded
- descendent cells produce identical antibody or TCR (except for mutation)
- During embryonic/neonatal development, those B & T cells that bind antigen (presumed to be self) are deleted [Brock 23-9]
- B cells mature in bone marrow; T cells mature in thymus
- it is thought even in adults, those tissues are kept free of "new" antigens
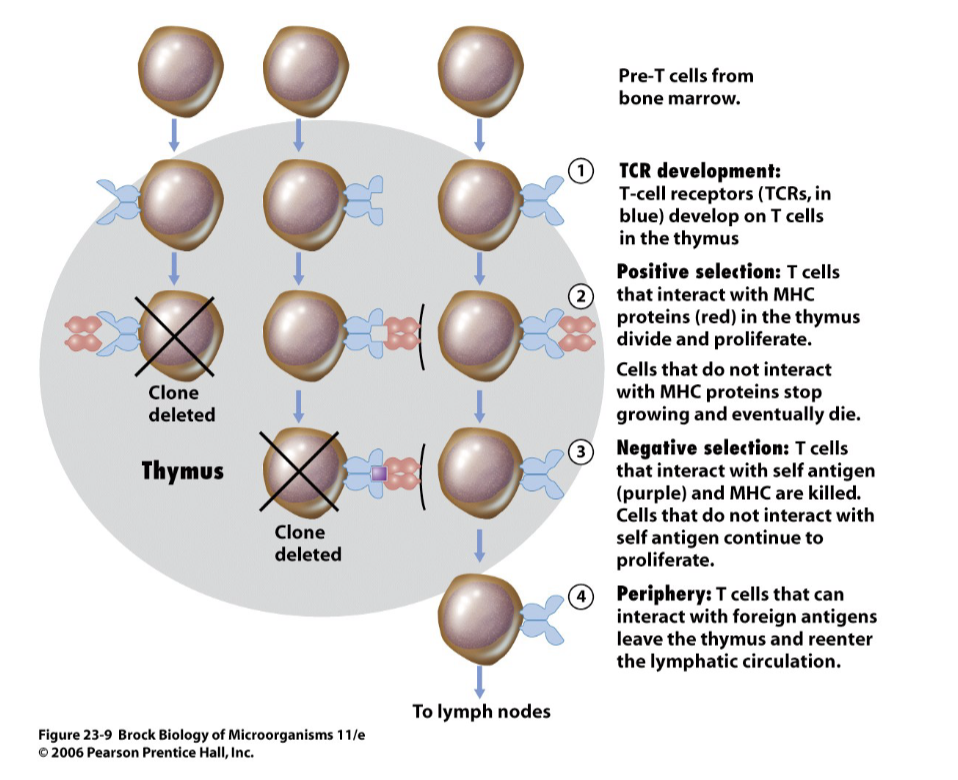
- if maturing cell does not react with MHC, it dies
- if maturing cell does react with antigen, it dies
The devastating effect of HIV
- HIV uses CD4 and a co-receptor to get into cells
- HIV can only replicate inside CD4+ cells
- therefore, HIV attacks macrophages, dendritic cells, and T H cells (immune system cells)
- usually infects mostly macrophages and dendritic cells early in infection
- switches over to mostly T H cells late
- TH cell count drops as HIV kills CD4+ cells
- uninfected adult has 600-1200 CD4+ cells per microliter of blood
- <400 CD4+ cells per microliter means the immune system is weakened
- <200 CD4+ cells per microliter is taken as a definition of having progressed to AIDS
- Without TH cells, cannot amplify T C cells or B cells and entire immune response collapses
Lecture 28- Diagnostics
Know Thine Enemy
- Quick detection and identification of pathogens is critical to effective treatment
- starts with epidemiological surveillance worldwide
- continues with tests performed in the clinic/doctor's office [table 28.3]
- test results determine treatment
- also indicate prognosis for complications, recovery
- and includes reporting to city/county/state health agencies
- Start with the usual suspects
- note symptoms of illness
- take case history
- onset of illness
- travel, occupation and hobbies contribute to exposure
- Narrow down based on known pathogenesis of microbes
- tests ordered to identify (or rule out) various agents
- based on most likely and most dangerous
- can be influenced by "what's going around" (epidemiological reports)
- Proper sampling & handling [figure 28.2]
- must take sample from site of infection
- may be swab, blood, fluid or stool collection
- include precautions to prevent contamination [figure 28.4] [table 28.1]
- must not contaminate with normal flora (if possible)
- must be mindful of oxygen tolerance of suspected pathogens [figure 28.3]
- must take sample from site of infection
Identification by Microscopic Observation
- Staining/morphology is rarely definitive (for bacteria)
- however, the appearance of some organisms in conjunction with symptoms and location sampled can often be presumptive (enough to start treatment)
- Specialized staining techniques can highlight microbes in tissue figure [figure 28.5]
Identification by Growth and Biochemical Tests
- Proper plating/media [figure 28.6]
- media should be enriching, if not selective
- failing that, a differential medium can distinguish between species
- must maintain temperature and oxygen conditions
- Identification by metabolic fingerprint, the results of multiple biochemical tests [table 28.2]
- based on flow charts for identification [figure 28.9] [figure 28.11]
- now worked into strips/kits [figure 28.8] [crystal 30]
- or even automated [figure 28.7]
Immunological Methods
- Current infection can be detected by using lab antibodies to detect antigen in patient
- Past infection can be inferred by detecting patient antibodies in blood using lab antigen
- antibody titer can be a signal of time of infection [Brock 24-11]
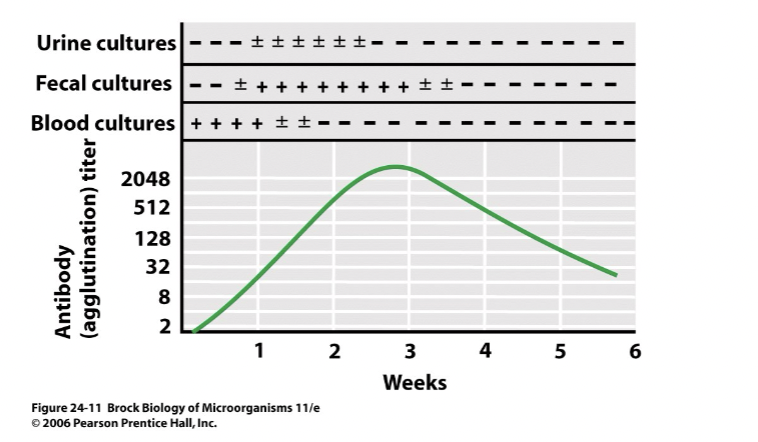
- draw blood, spin out cells
- dilute serum by factors of 2
- look for reaction against lab antigen
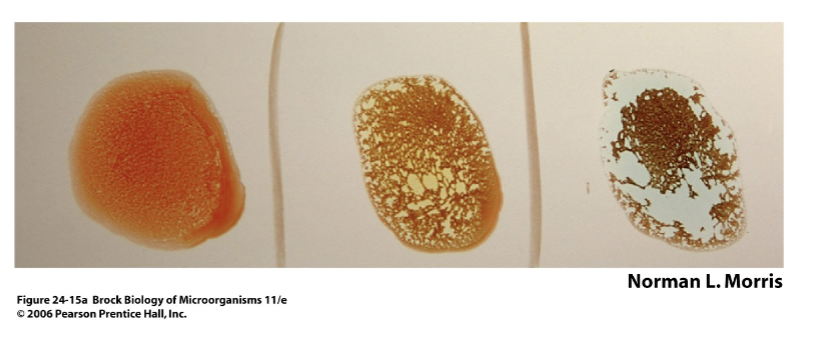
- Precipitation/Agglutination [Slon4, figure 24.8] [Brock 24-14a]
- at equal concentrations of antibody and antigen, bridging will occur
- will precipitate soluble antigen and agglutinate (clump) cells
- is the basis for blood typing [Brock figure 24.15a] [Brock, figure 24.15b]
- allows rapid detection of some infectious agents (or specific strain for epidemiology)
- Fluorescent Microscopy
- direct method (useful in identifying cells) [figure 24.21] [Brock 24-18a]
- antibodies are conjugated to fluorophore
- conjugated antibodies are allowed to bind to cell suspension from patient
- will bind if antigen is on cell surface
- can be examined by light microscopy
- This method tests for antigen in patient
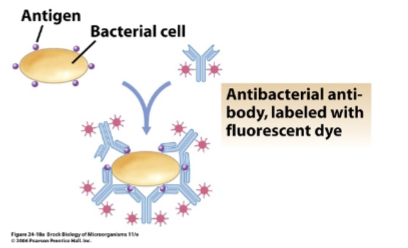
- antibodies come from lab and you’re binding to cells from patient
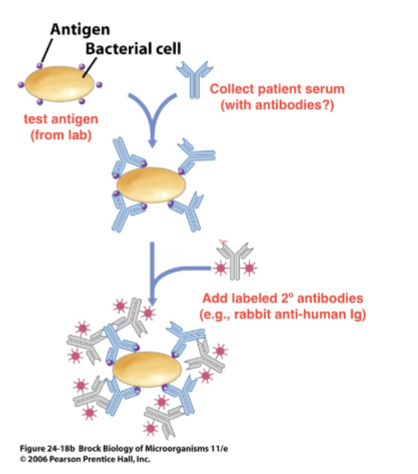
- indirect method (useful in detecting past exposure) [Brock 24-18b]
- serum from patient is collected
- serum is mixed with test antigen
- if antibodies present, will bind cells
- if not, serum is washed away
- secondary antibody with fluorophore added to cells
- 2º ab must be from other species
- 2º ab binds to any ab from 1st species in Fc region
- e.g., 2º ab = rabbit anti-human IgG
- if you don’t have antibodies, they won’t bind to anything
- can be examined by light microscopy
- This method tests for antibodies in patient serum (past exposure)
- Use of 2º ab saves time & trouble adding fluorophore to serum antibodies; labeled 2º ab binds to many different serum ab
- cells come from lab and you’re binding to anitbodies from patient
- can be used in combination with a cell sorter (FACS machine)
- laser activates fluorescently labeled cells (labeled antibody bound to surface antigen)
- charge difference is used to separate cells
- direct method (useful in identifying cells) [figure 24.21] [Brock 24-18a]
- Immunoelectron Microscopy
- antibodies are conjugated to gold bead
- gold is dense enough to block electron beam
- conjugated antibodies allowed to bind to cell section
- will bind wherever antigen is
- antibodies are conjugated to gold bead
- Enzyme-Linked Immunosorbent Assay (ELISA)
- similar to above but detection based on colorimetric enzyme reaction
- because of enzyme, more sensitive than fluorescent methods
- must conjugate enzyme to constant region of antibody
- amazingly, does not affect antibody binding or enzyme activity
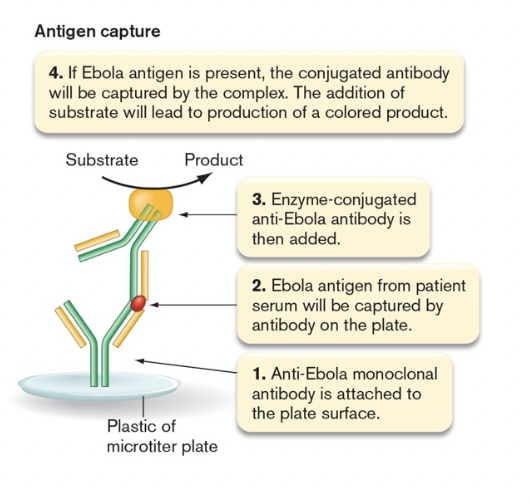
- direct ELISA- tests for antigen (antigen capture) [figure 28.20]
- unconjugated antibody stuck to well
- antigen allowed to bind
- enzyme conjugated antibody then added
- color based reaction carried out
- strength of color depends on how much antigen bound
- indirect ELISA-tests for antibody [figure 28.19]
- antigen stuck to microtiter well
- serum from patient passed over
- if antibodies present, will bind antigen
- if not, serum is washed away
- enzyme-conjugated 2º antibody added
- example- 2º ab = rabbit anti-human IgG
- color based reaction carried out
- strength of color depends on how antibody titer in patient serum
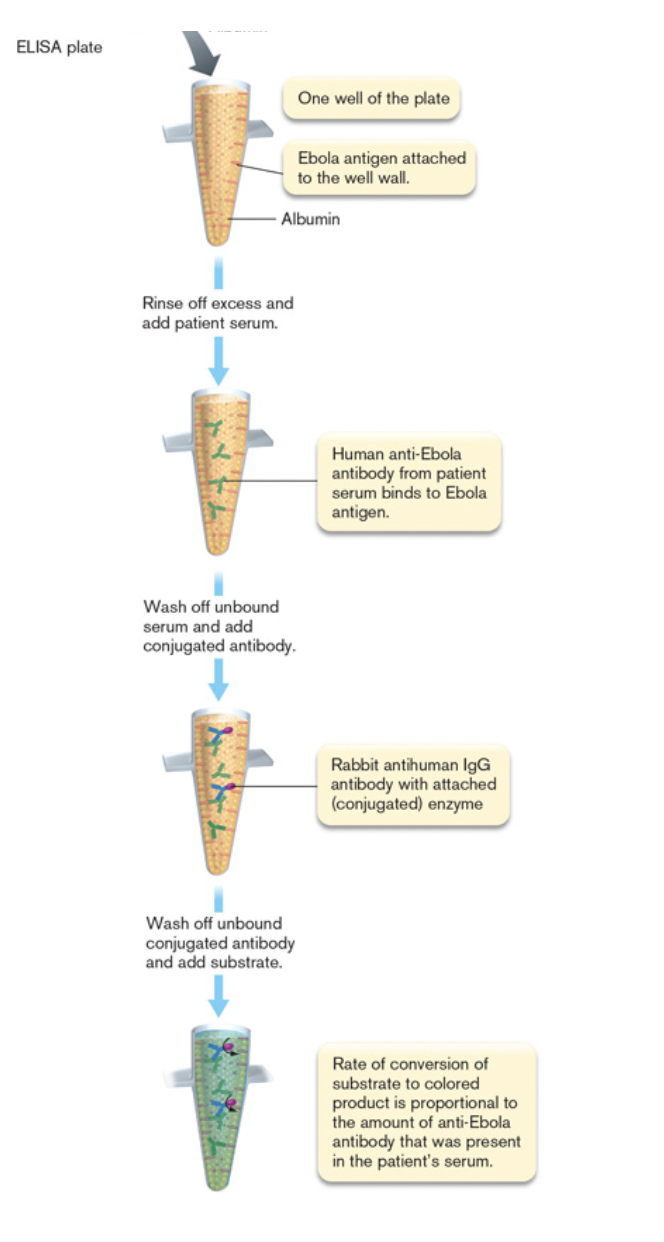
- similar to above but detection based on colorimetric enzyme reaction
Wednesday, June 12, 2024
Lecture 28- Diagnostics
Immunological Methods
- Immunoblot (Western blot)
- run proteins out on gel [Brock 24-27a-1]
- blot proteins onto membrane [Brock 24-27a-2]
- add unlabeled (primary) antibodies for specific protein [Brock 24-27a-3]
- add enzyme-conjugated (secondary) antibodies against first antibodies [Brock 24-27a-4]
- reaction will occur where antibody is bound [Brock 24.27b]
- Antibody-based rapid detection methods [figure 28.22] [table 28.4]
- advantage- fast, no culturing required, immediate treatment based on result
- disadvantages- false positives and negatives, no information about antibiotic resistance
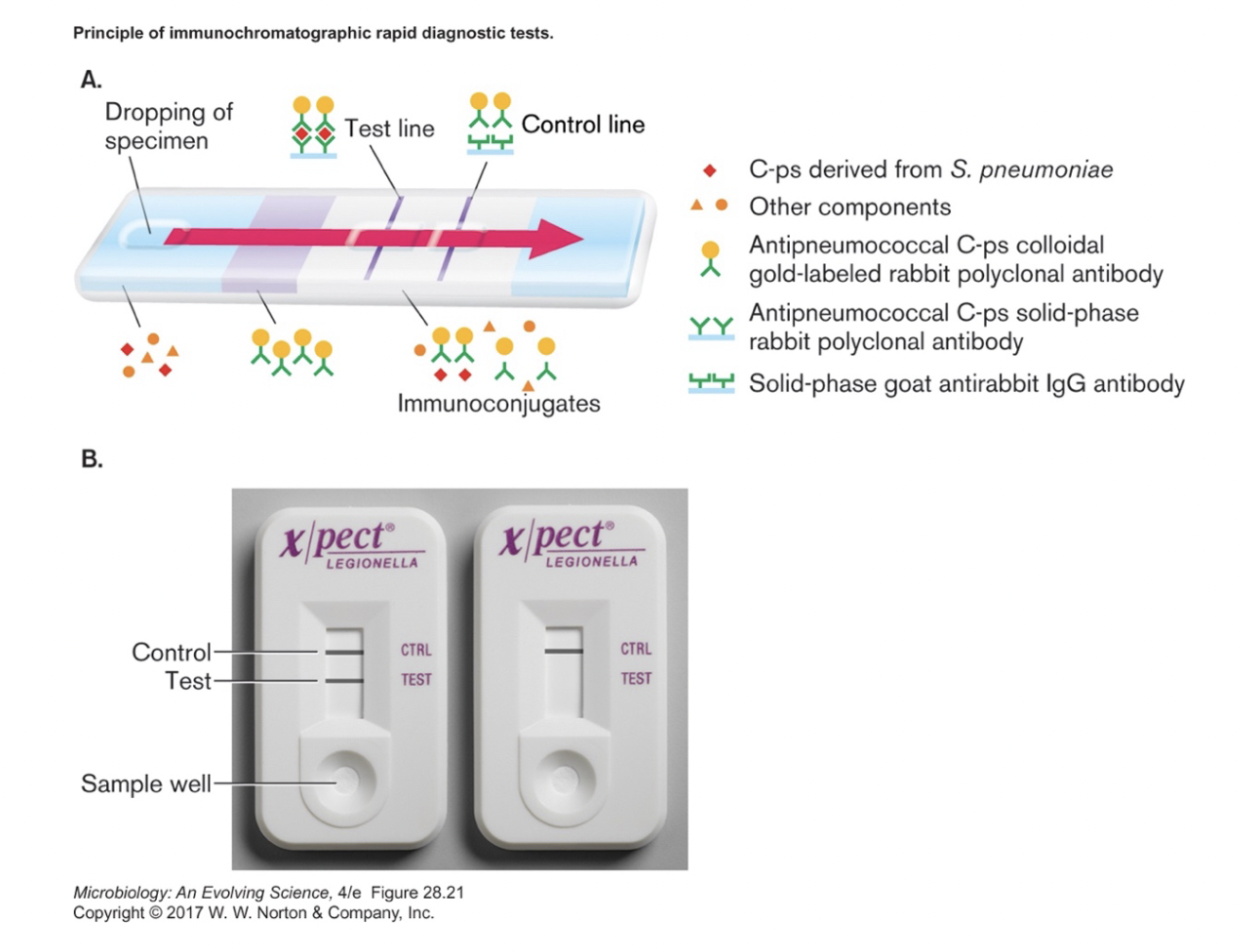
- blood, sputum or urine (with antigen) added to one end of filter strip
- capsular protein from Streptococcus pneumoniae in example above
- beta subunit of human chorionic gonadotropin in pregnancy test
- spike or nucleocapsid protein for rapid Covid tests
- capillary action carries fluid through region with labeled-antibody for particular antigen
- labeled antibodies are mobile
- will be carried along by fluid (with or without antigen binding)
- are from species 1 (rabbit in the example above)
- fluid passes line of immobilized antibodies for antigen
- labeled antibodies will stop on test line if bound to antigen
- fluid passes on to second line, immobilized antibodies for species 1
- must be from second species (goat in above example)
- serves as control, to ensure labeled antibodies were carried past test line
Nucleic Acid Methods (NAAT = Nucleic Acid Amplification Tests)
- PCR [figure 28.14]
- use primers for distinctive genes
- size of fragment can indicate species and strain, antibiotic resistance
- can be multiplex, i.e., include primer pairs for multiple genes
- sensitive and fast (no culturing)
- works well for bacteria and DNA viruses
- use primers for distinctive genes
- RT-PCR [figure 28.15]
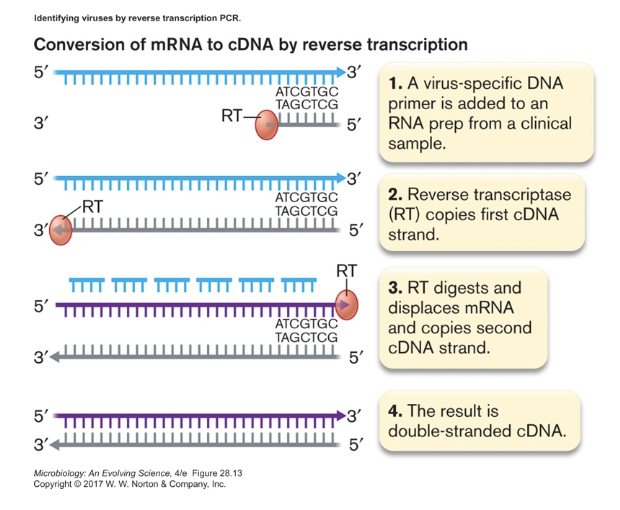
- used to detect RNA from pathogen, especially for RNA viruses (see end for Covid test)
- qRT-PCR (quantitative real time PCR) [figure 28.16b]
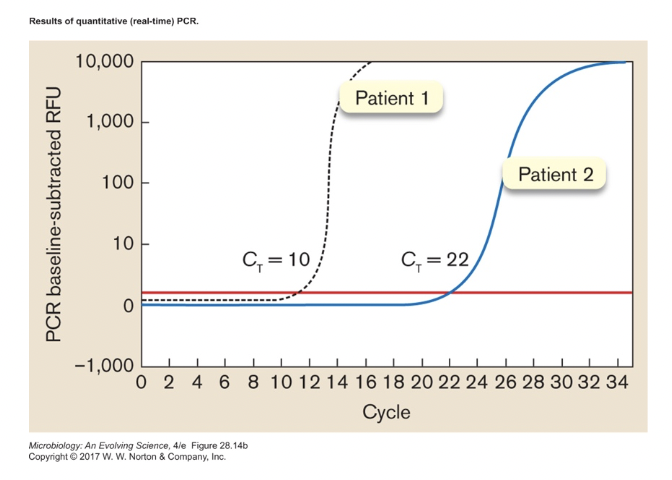
- follow increase in product, tells you how much starting template there was
- can track viral loads during infection
- tells you how much virus someone has in their system
Tests for SARS-CoV-2 [FDA] [CDC]
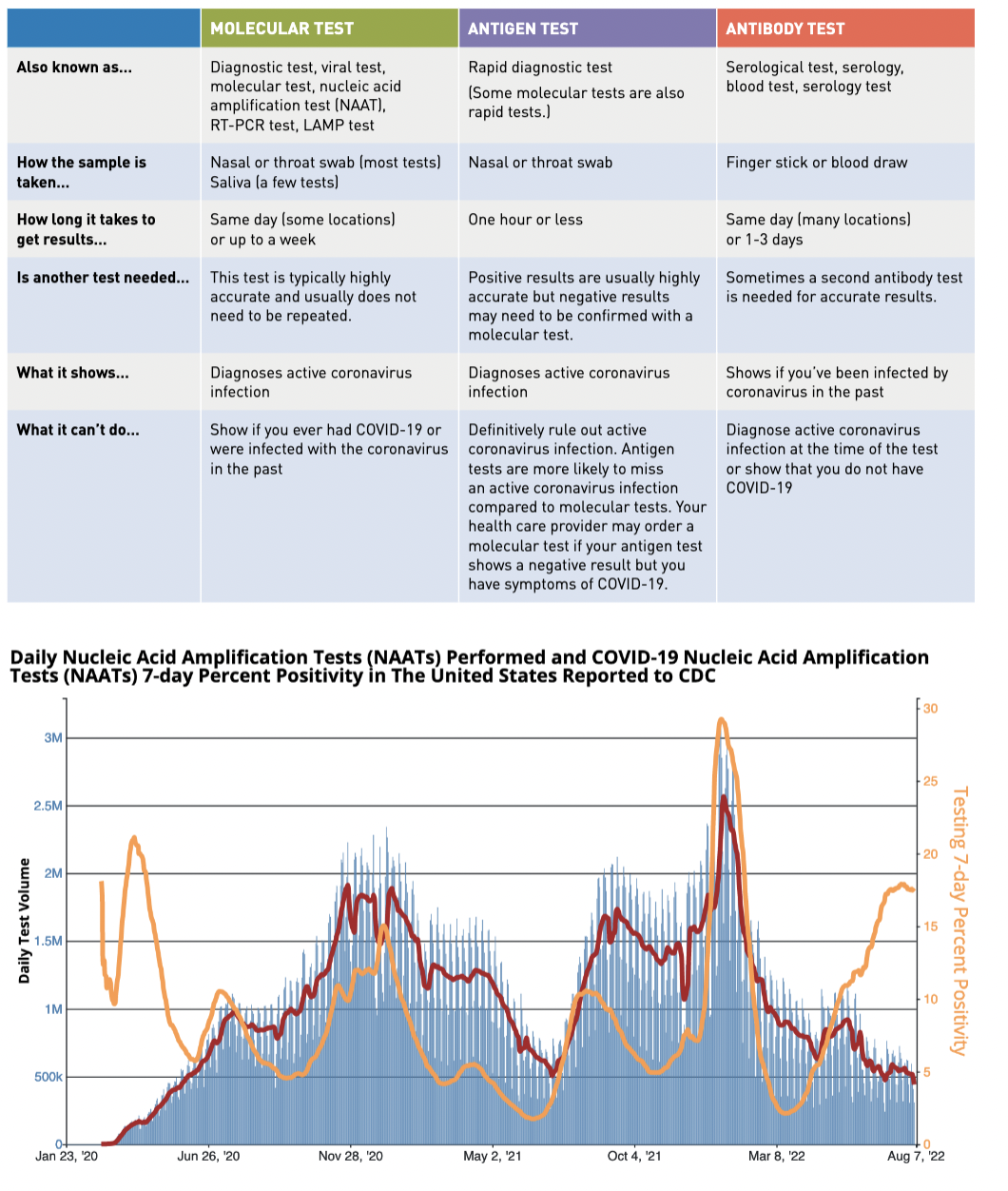
- Diagnostic tests- detect current infection
- start with a nasal/throat swab
- molecular tests- identify viral RNA in patient
- all are some version of RT-PCR
- requires lab equipment and some training of personnel
- sent to lab- more accurate; each machine can handle 500-1000 samples/day
- point of care- can get answer in 5-15 minutes, but no more than 100 tests/day
- how? abbreviated PCR
- less sensitive, danger is false negatives
- RNA may not be found right away, RNA may linger when patient not contagious
- speed of turnaround is key to usefulness
- all are some version of RT-PCR
- antigen test- identify viral proteins in patient
- simpler and faster, no equipment required to run test; cheaper
- less sensitive, problem with false negatives
- If positive, either result should be reported to public health for contact tracing
- USA current- ~465,000 PCR tests daily; ~2.8% positive: antigen test- ???
- but with end of Covid health emergency, no requirement to report testing to CDC
- Antibody tests- detects past infection (at least 2 weeks ago)
- starts with a blood sample
- detects IgM and/or IgG specific for the virus
- may help determine when person was infected or if they can donate plasma
- may provide data for epidemiological models
- if not specific enough (cross-reacts with cold viruses), false positives a problem
Lecture 29- Antimicrobial Drugs
General Characteristics of Antimicrobial Drugs
- Antibiotics = antimicrobial compounds produced by microbes [figure 1.22]
- source is typically fungi or soil bacteria
- Exhibit selective toxicity [figure 27.7] [Brock 27-20] [table 27.2]
- antibiotic must target something unique about pathogen
- May also have side effects
- typically = allergies, stomach upset, diarrhea, kidney and/or liver damage
- side effects are dosage dependent
- Effective range varies [Brock 20.15]
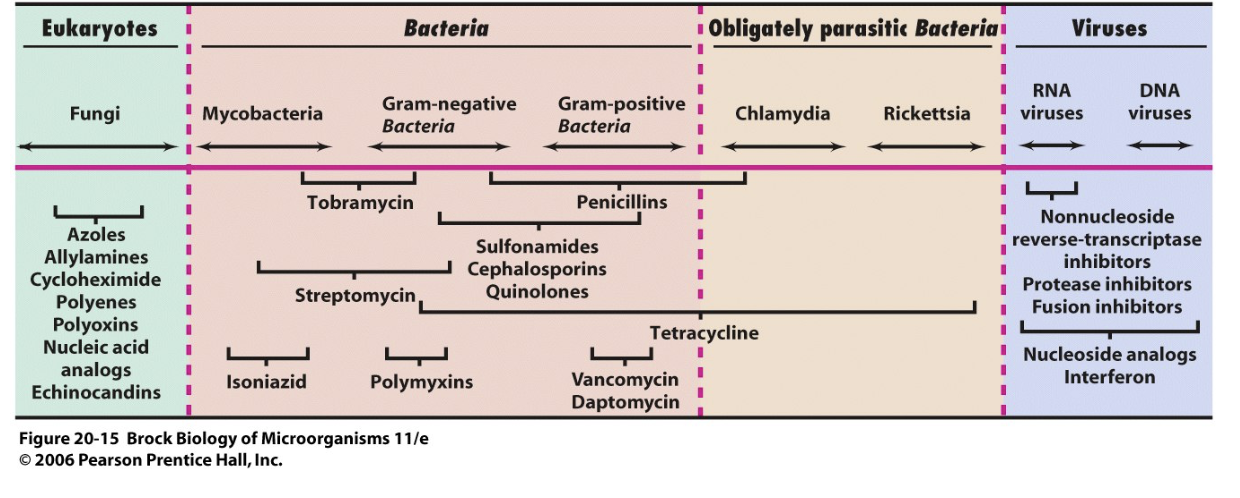
- drugs can be broad or narrow spectrum in terms of effectiveness against pathogens
- may kill pathogen (bactericidal) or limit its growth (bacteriostatic)
- Commercial antibiotics can be natural, synthetic or semi-synthetic
- growing the organism & purifying the drug (at scale) can be technical challenges [pen G]
- took ~ 15 years from discovery to introduction of penicillin
- first successful treatment of systemic infection (1942) used half available supply
- within two years, was being mass-produced [war1] [war2]
- best source strain = isolate from moldy cantaloupe in Peoria IL
- growth medium = corn steep liquor
- deep tank fermentation resulted in best yields
- how to introduce oxygen without contaminating the culture
- took ~ 15 years from discovery to introduction of penicillin
- natural drugs are often modified [figure 27.9] [Brock 20-20]
- to make them effective against more organisms
- to make them effective against resistant organisms
- to allow them to be taken in pill form
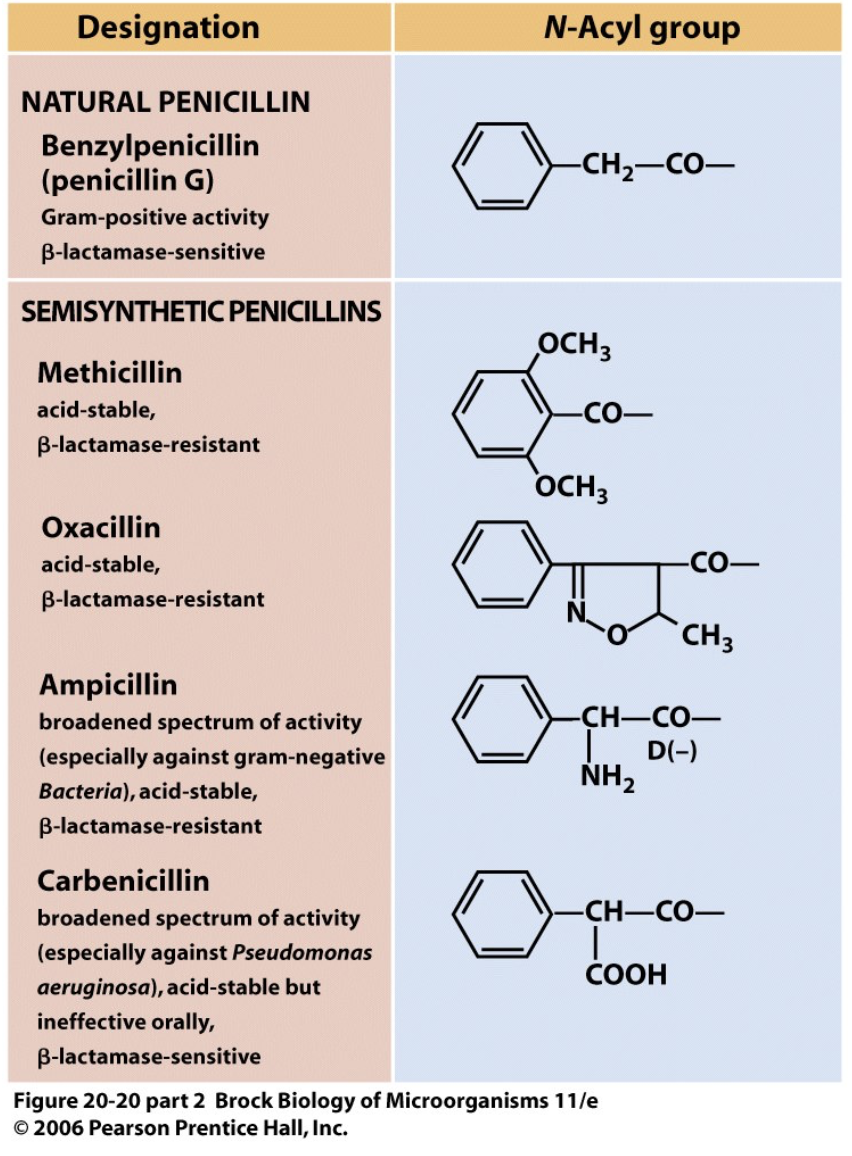
- natural penicillin is rapidly excreted
- probenecid given with penicillin to outcompete penicillin excretion
- synthetic penicillin makes this unnecessary
- growing the organism & purifying the drug (at scale) can be technical challenges [pen G]
- Mode of administration
- oral- must be acid tolerant, well absorbed
- most convenient
- topical- typically only for superficial infections
- injection- most direct, but also most difficult
- oral- must be acid tolerant, well absorbed
- Resistance [Brock T20-7] [figure 27.20]
- a predictable evolutionary result
- selection for resistance increases their numbers
- horizontal gene transfer spreads resistance genes
- should limit indiscriminate antibiotic use
- an increasing problem, especially in hospitals [figure 27.19]
- need to find new drugs or modify old ones
- mechanisms
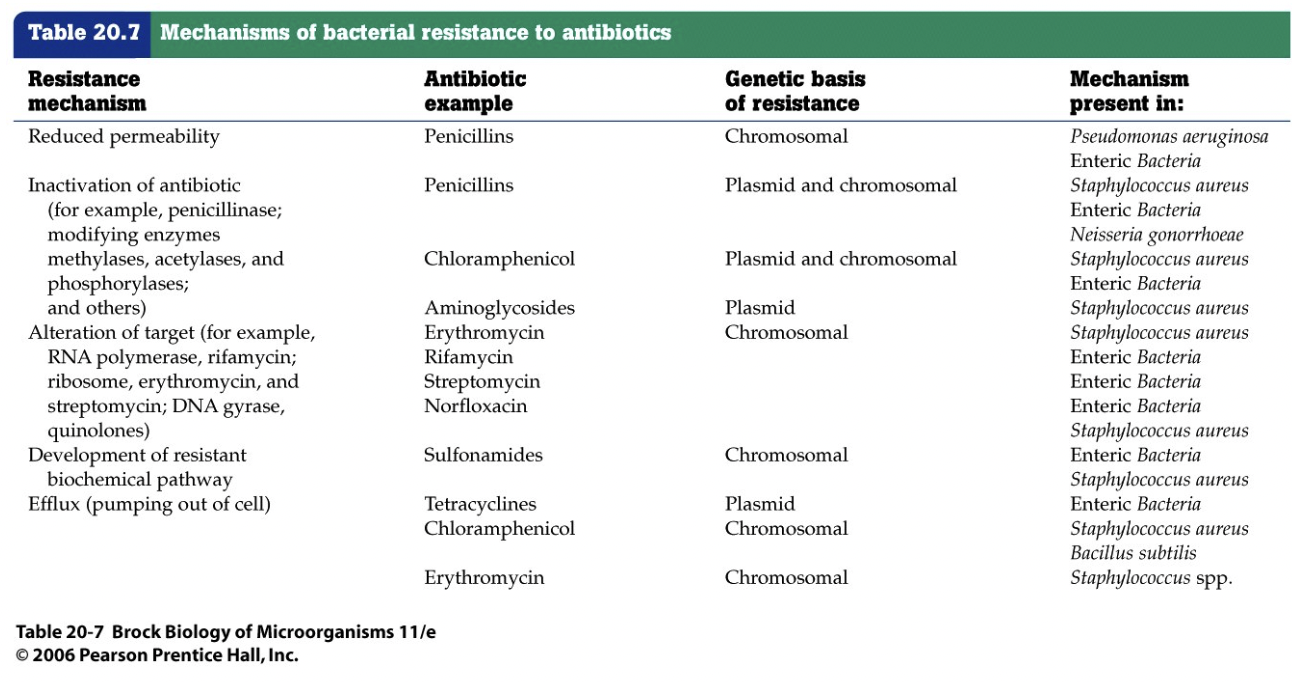
- reduced permeability of cell envelope
- alter pore proteins (for hydrophilic antibiotics)
- alter membrane lipids (for hydrophobic antibiotics)
- efflux pumps to transport drug out [figure 27.23]
- may add on to existing transport systems [figure 27.24]
- dumping water out of kayak that has hole in it as fast as the water is flowing in, kayak stays afloat
- inactivate antibiotic
- by cleaving it [figure 27.21]
- by modifying it [figure 27.22]
- mutate target of action
- avoid/alter target pathway
- usually sensitive is more favored than resistant because it grows faster and if the antibiotic hasn’t been encountered in quite some time, it’ll go back to sensitive
- reduced permeability of cell envelope
- determinizing effectiveness
- Kirby-Bauer method
- uses disk diffusion method [figure 27.5]
- compare diameter of zone of inhibition to standard [table 27.1]
- must maintain consistency of medium, temperature, etc.
- Minimum Inhibitory Concentration (MIC)
- determine by dilution [figure 27.3] or test strip [figure 27.4]
- what is the lowest concentration that prevents growth?
- in vivo levels don't match in vitro tests [figure 27.6]
- your body is flushing things out, breaking things down, and it doesn’t distribute evenly throughout your body/work as well in certain areas
- Kirby-Bauer method
- a predictable evolutionary result
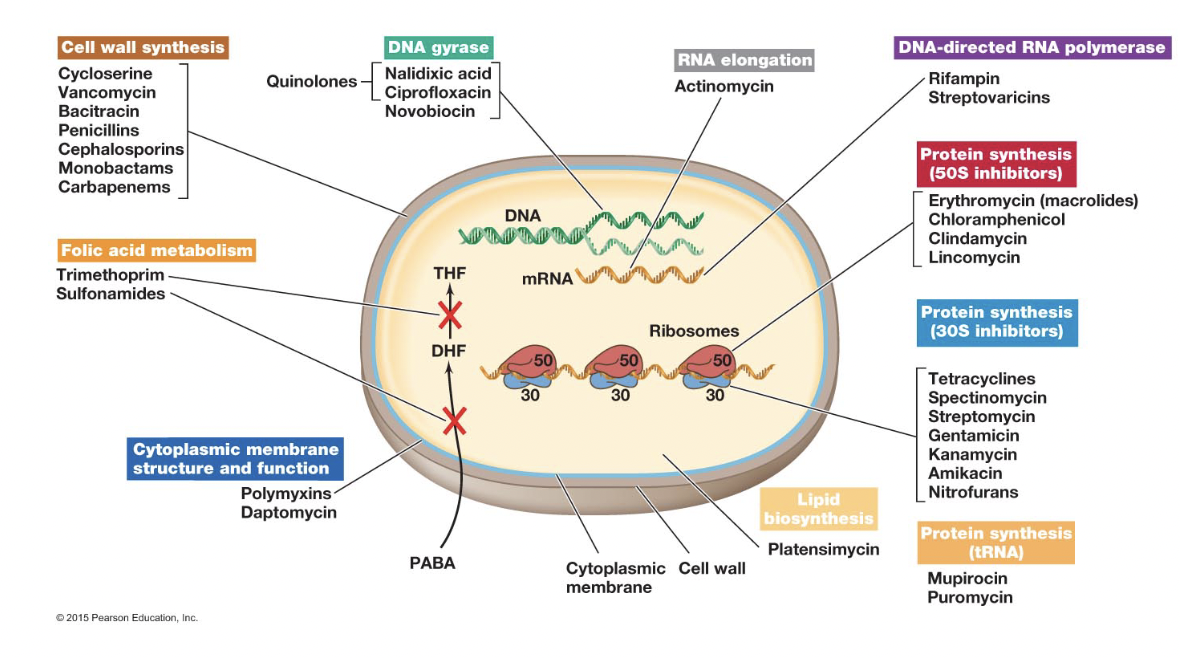
Cell Wall Synthesis [figure 27.8]
- Steps in peptidoglycan synthesis
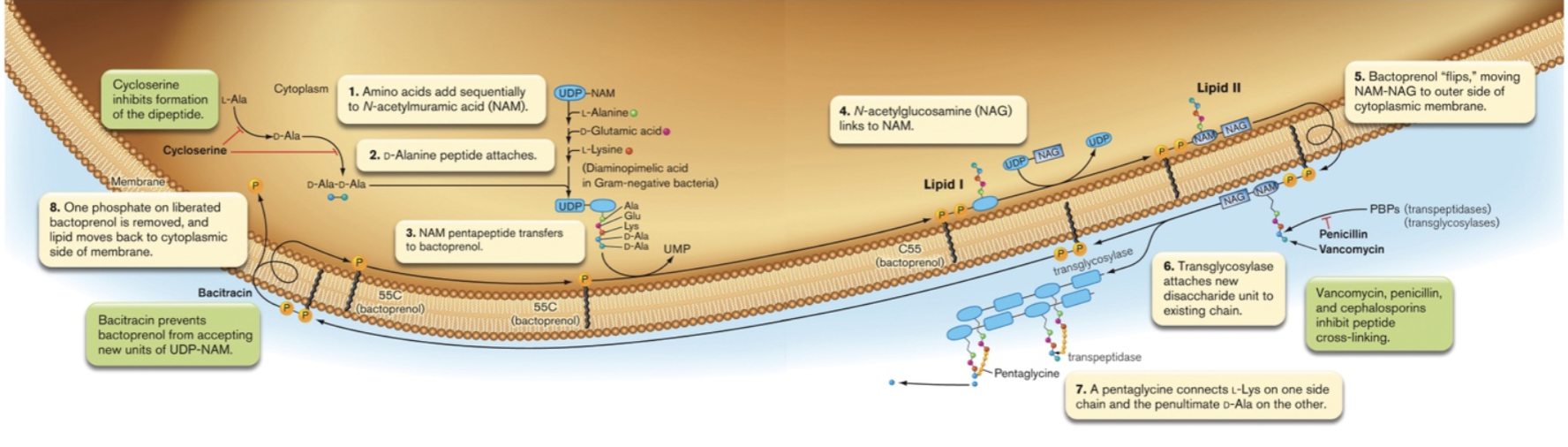
- synthesis of NAG & NAM-peptide precursors
- transport across cytoplasmic membrane by bactoprenol
- polymerization into existing wall by transglycosylases
- cross-linking chains by transpeptidases
- all of these steps needed to synthesize cell wall, any of them can be interfered with
- Beta-lactam antibiotics
- examples- penicillin, cephalosporin [figure 27.9] [figure 27.10]
- mechanism- resembles D-ala dipeptide, competes for binding to transpeptidase
- used against- Gram-positives, some Gram negatives (OM limits access to wall)
- resistance- enzymes which break down antibiotic
- Vancomycin [figure 27.11c]
- mechanism- binds to peptides, interferes polymerization and cross-linking
- used against- Gram positives, drug of last resort
- Cycloserine [figure 27.11b]
- mechanism- interferes with formation of D-ala dipeptide
- used against- Mycobacterium
- Bacitracin [figure 27.11a]
- mechanism- interferes with bactoprenol, peptidoglycan subunit transfer
- used against- Gram positives
Membrane Integrity
- Gramicidin [figure 27.12]
- a cyclic peptide with D and L amino acids
- mechanism- inserts into membrane, creates pores
- Polymixin
- polypeptide
- mechanism- acts like detergent to disrupt cytoplasmic membrane
- used- topically (also disrupts human cell membranes)
- Daptomycin
- non-ribosomal peptide (i.e., an enzyme, not ribosome, links amino acids together)
- mechanism- forms ion channel
DNA Synthesis and Structure
- Quinolones
- examples- nalidixic acid, ciprofloxacin
- mechanism- interfere with DNA gyrase
- used against - broad spectrum
- Sulfa drugs
- example- sulfanilamide
- mechanism- interfere with folic acid metabolism (analog of PABA) [figure 27.13]
- needed in synthesis of purines & pyrimidines
- bacteria make folic acid, we get it from food
- used against- broad spectrum
- resistance- bacteria take up folic acid
- Trimethoprim
- mechanism- interferes with folic acid metabolism
- used against- broad spectrum
- Base analogs [Brock 20-18]
- example- 5-fluorouracil, 5-bromouracil, AZT, 5-flucytosine
- mechanism- interfere with nucleic acid synthesis
- used against- viral or fungal polymerase that are more likely to incorporate analog
- resistance- mutations in polymerase decrease affinity for analogs
Transcription [figure 27.15]
- Rifamycin
- mechanism- interfere with elongation by RNA polymerase
- used against - broad spectrum
- Actinomycin D
- mechanism- bind to DNA, prevent initiation by RNA polymerase
- used- only in lab, is toxic to host cells
Translation [figure 27.16]
- Aminoglycoside antibiotics
- contain a cyclohexane ring and amino sugars
- examples- streptomycin, kanamycin, gentamycin, neomycin
- mechanism- interfere with 30S ribosomal subunit
- used against- broad spectrum
- toxicity- serious issues, due to impact on mitochondrial ribosomes
- some people more susceptible than others
- resistance - mutation in ribosomal proteins, readily develops
- Tetracyclines
- mechanism- binds 30S ribosomal subunit, prevents tRNA binding
- used against- broad spectrum
- toxicity- impact on bone development, proscribed for pregnant women
- resistance- mutation in ribosomal proteins, widespread
- Macrolide antibiotics
- contain lactone ring
- examples- erythromycin
- mechanism- blocks 50S ribosomal subunit, elongation
- used against- Gram positives, some Gram negative
- Chloramphenicol
- mechanism- binds to 50S subunit, blocks peptide bond formation
- used against- broad spectrum, but severe side effects limit use
- Oxazolidinones
- mechanism- prevents coupling of 30S & 50S subunits
- resistance- limited because multiple rRNA gene copies would have to mutate
- used against- mostly Gram positives
- Streptogramins [figure 27.17]
- mechanism- prevent elongation
Growth Factor Analogs
- Resemble growth factor, block its utilization
- Isoniazid
- mechanism- interfere with NAD metabolism, mycolic acid synthesis
- used against- only Mycobacterium incorporates mycolic acid into wall
- resistance- increasing
Antiviral Drugs [table 27.3] [figure 27.35]
- Base analogs [figure 27.33]
- have high host toxicity
- Viral enzyme inhibitors (very narrow spectrum, often specific to one virus)
- prevent uncoating [figure 27.32]
- example- amantadine blocks release of genome from capsid for flu virus
- neuraminidase inhibitor
- example- tamiflu & zanamivir prevent budding out of flu virus
- reverse transcriptase inhibitors
- example- delavirdine for HIV
- protease inhibitor [figure 27.34]
- example- viracept & lopinavir block cleavage of Gag polyprotein in HIV
- fusion inhibitor
- example- CCR5 inhibitors prevent HIV from binding to a co-receptor
- prevent uncoating [figure 27.32]
- Interferon
- mimic immune response
- needed at site of infection in high doses
Antifungal Drugs [Brock 20-24] [figure 27.37]
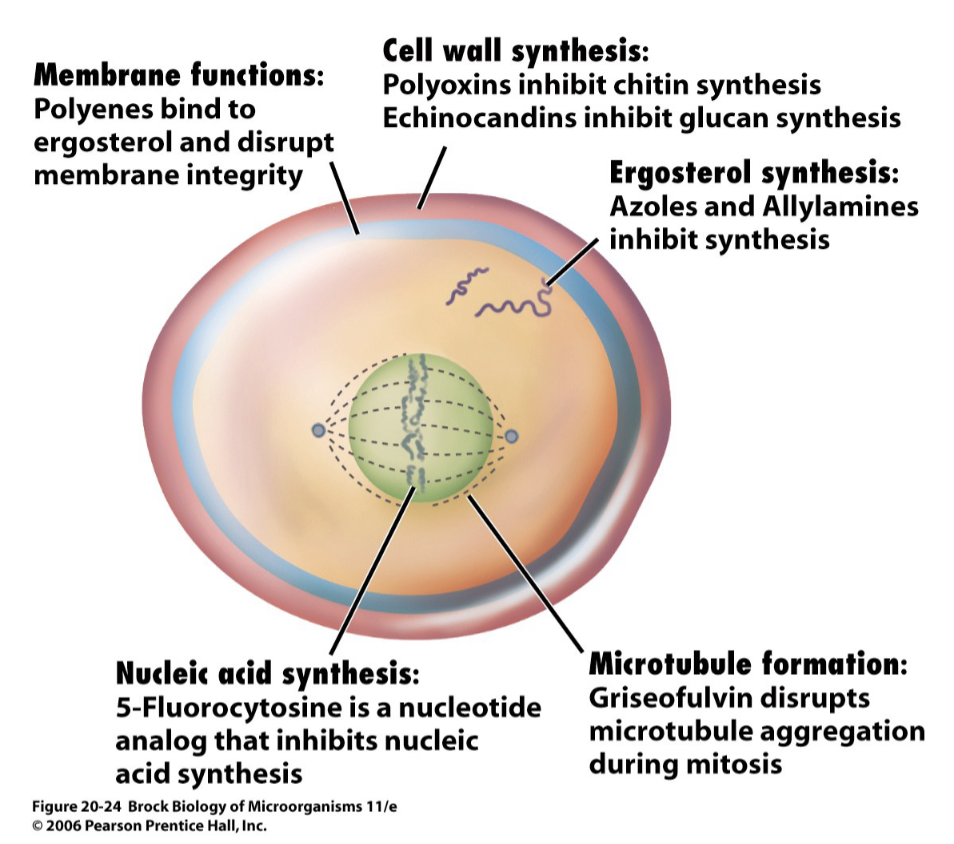
- Azoles & allyamines
- examples- ketoconazole, miconazole, lamisil
- mechanism- ergosterol synthesis inhibitors
- cholesterol equivalent for fungi
- used against- topical fungal infections
- Polyenes
- example- nystatin, amphotericin B
- mechanism- bind to ergosterol in fungal membranes, create pores
- used against yeast infections, systemic fungal infections
- Polyoxins
- mechanism- nucleoside analogs that inhibit chitin synthesis in cell wall
- Echinocandins
- mechanism- lipopeptides that inhibit glucan synthesis in cell wall
- Griseofulvin
- mechanism- disrupt microtubules
- used against topical infections
- Base analogs
Lecture 30- Epidemiology
Epidemiology
- Study of (infectious) diseases in populations
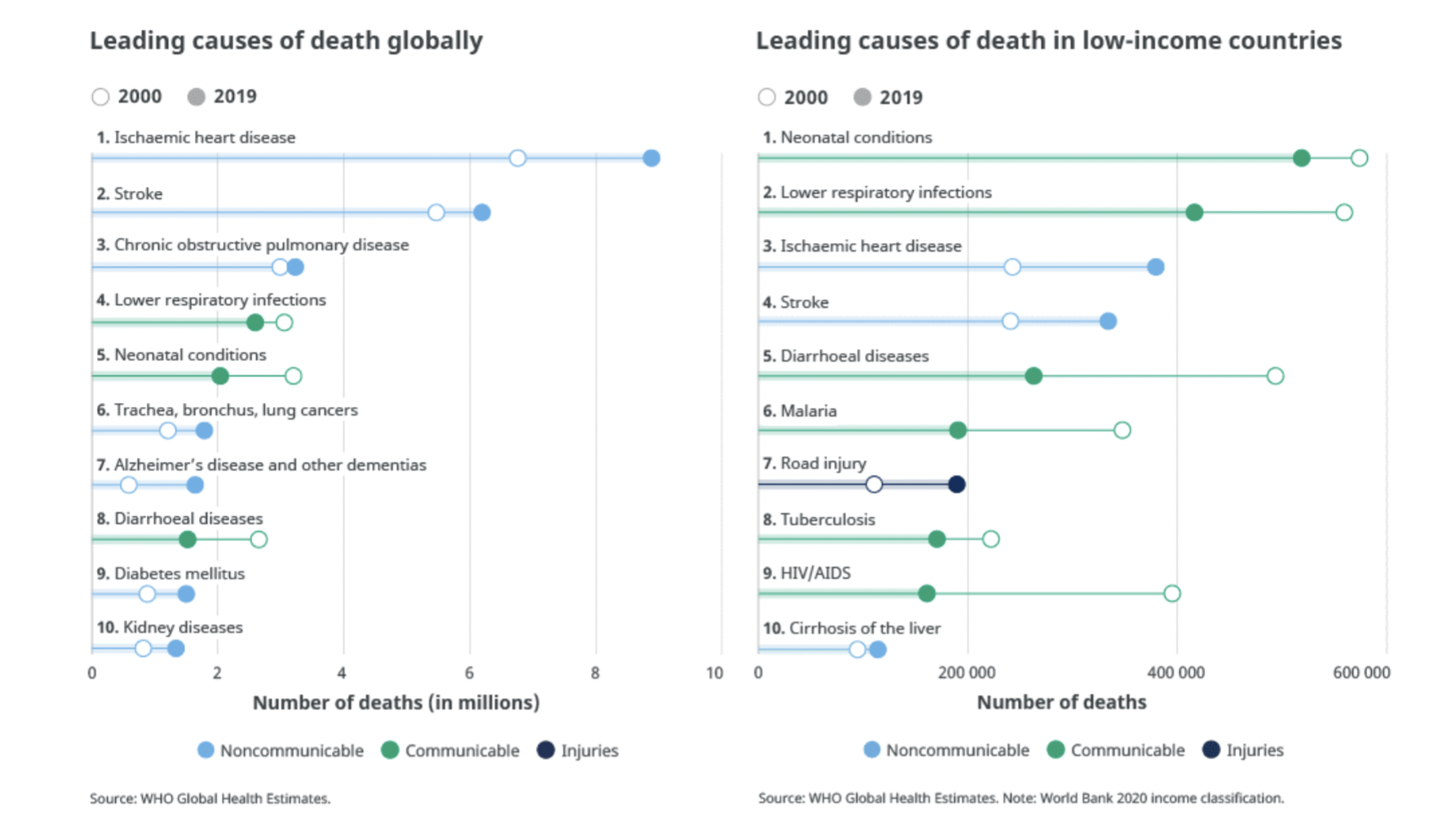
- infectious diseases caused 14.4 out of 55.4 million deaths worldwide 2019 (26%) [WHO]
- infectious diseases are on a long-term trend downward as a %age of deaths
- still more prevalent in low-income countries
- by comparison, Covid 19 has killed ~7 million in 4.5 years (~0.125m in last year)
- infectious diseases caused 14.4 out of 55.4 million deaths worldwide 2019 (26%) [WHO]
Individual Illness (addressed by medical system)
- Course of disease
- infection- disease agent is acquired
- incubation- agent is multiplying, disease symptoms not yet evident
- acute phase- height of disease
- decline period- symptoms subsiding
- convalescence- regaining strength
- Outcome determined by
- establishment of infection- point of entry, inoculum size
- virulence of agent- life cycle, virulence factors, strain
- host resistance- general health, age, nutrition, prior exposure
- treatment options- speed of diagnosis, availability and access to medicine
Epidemic Disease (addressed by public health system)
- Reservoir- where disease agent is found; origin of new cases
- humans
- may be incubatory, actively ill, convalescent, or healthy
- acute or chronic carrier
- other animals (zoonotic disease)
- may or may not show signs of disease
- soil/water
- humans
- Pattern of transmission [figure 25.6]
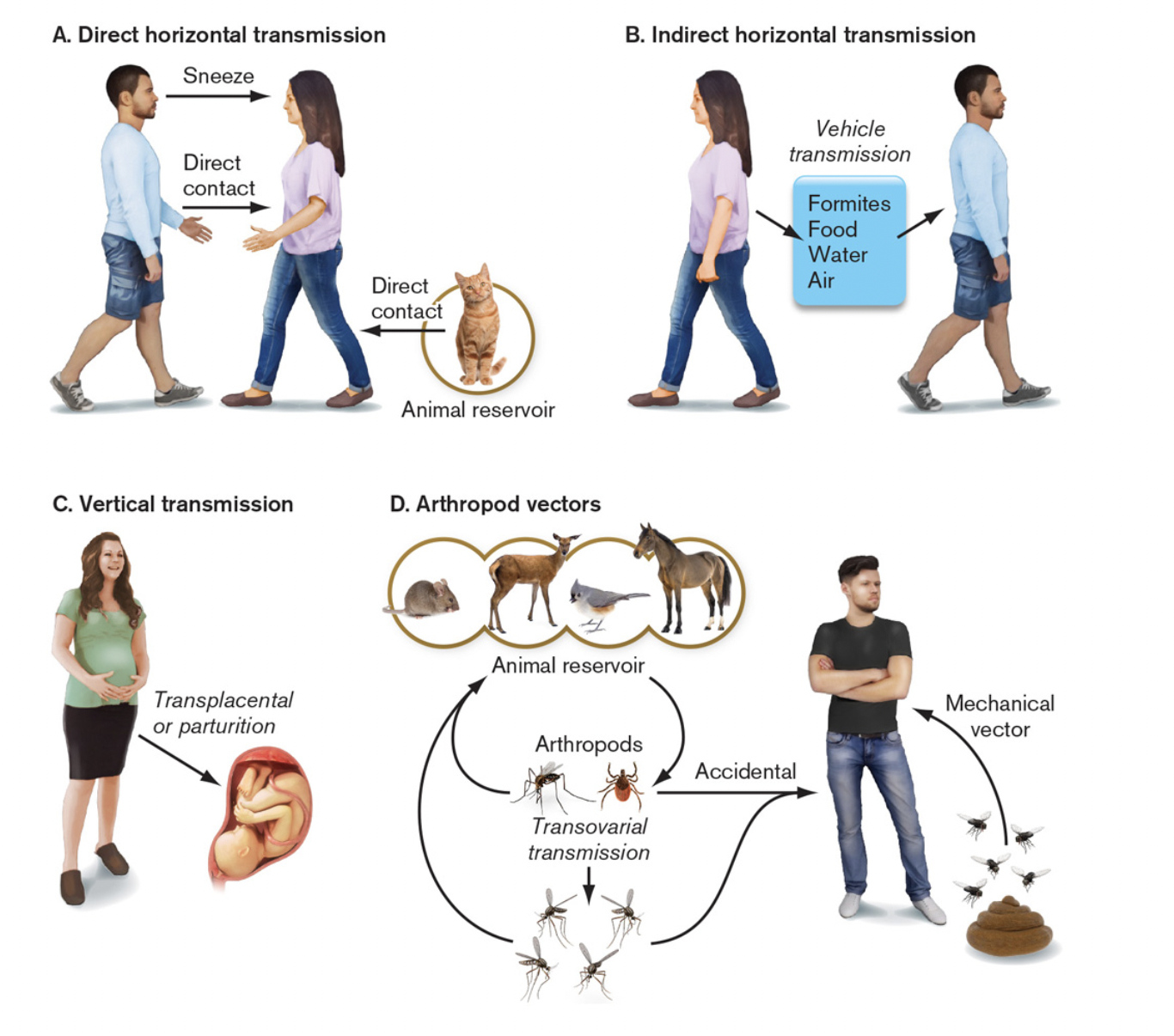
- direct- host to host
- physical contact- via touch, body fluids, etc.
- airborne- via droplets or dust
- indirect
- food & water- common source, contaminated before consumption
- vector-borne- living agent introduces pathogen
- fomites- inanimate objects, e.g., bedding, cups, utensils, surfaces, etc.
- direct- host to host
Thursday, June 13, 2024
Lecture 30- Epidemiology
Epidemic Disease (addressed by public health system)
- basic reproductive ratio (R0)- average number of new cases from each infected individual
- one person gets infected, how many people do they infect?
- if R0 is >1, someone is less than 50% likely to spread it to someone
- it assumes zero infection or immunity, no treatment for the disease
- but is not really a constant
- depends on mode of transmission, infectiousness and length of contagious period
- depends on density, susceptibility and behavior of victims (contact rate)
- depends on humidity, temperature and air movement
- R0 vs. Re = Re is the effective viral reproduction rate, accounting for above
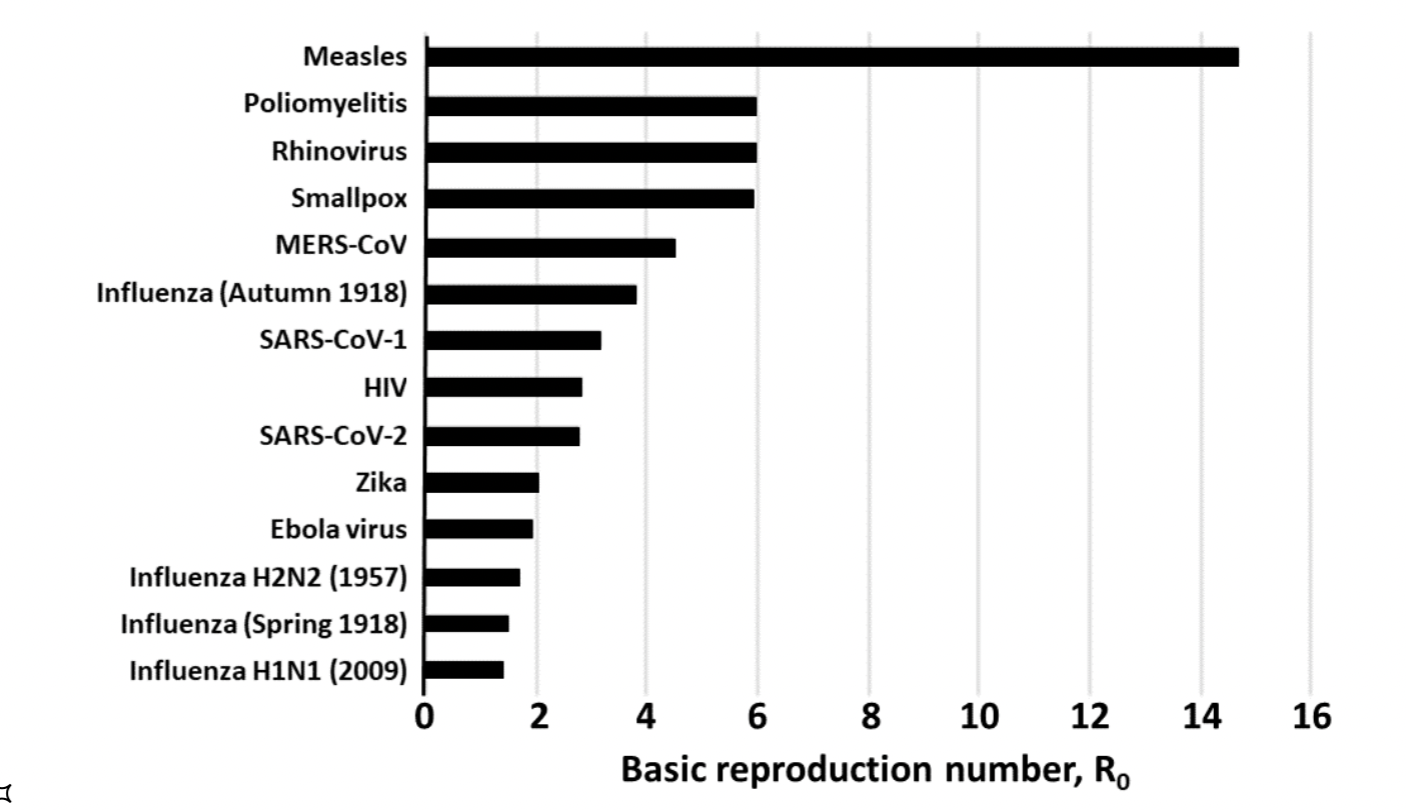
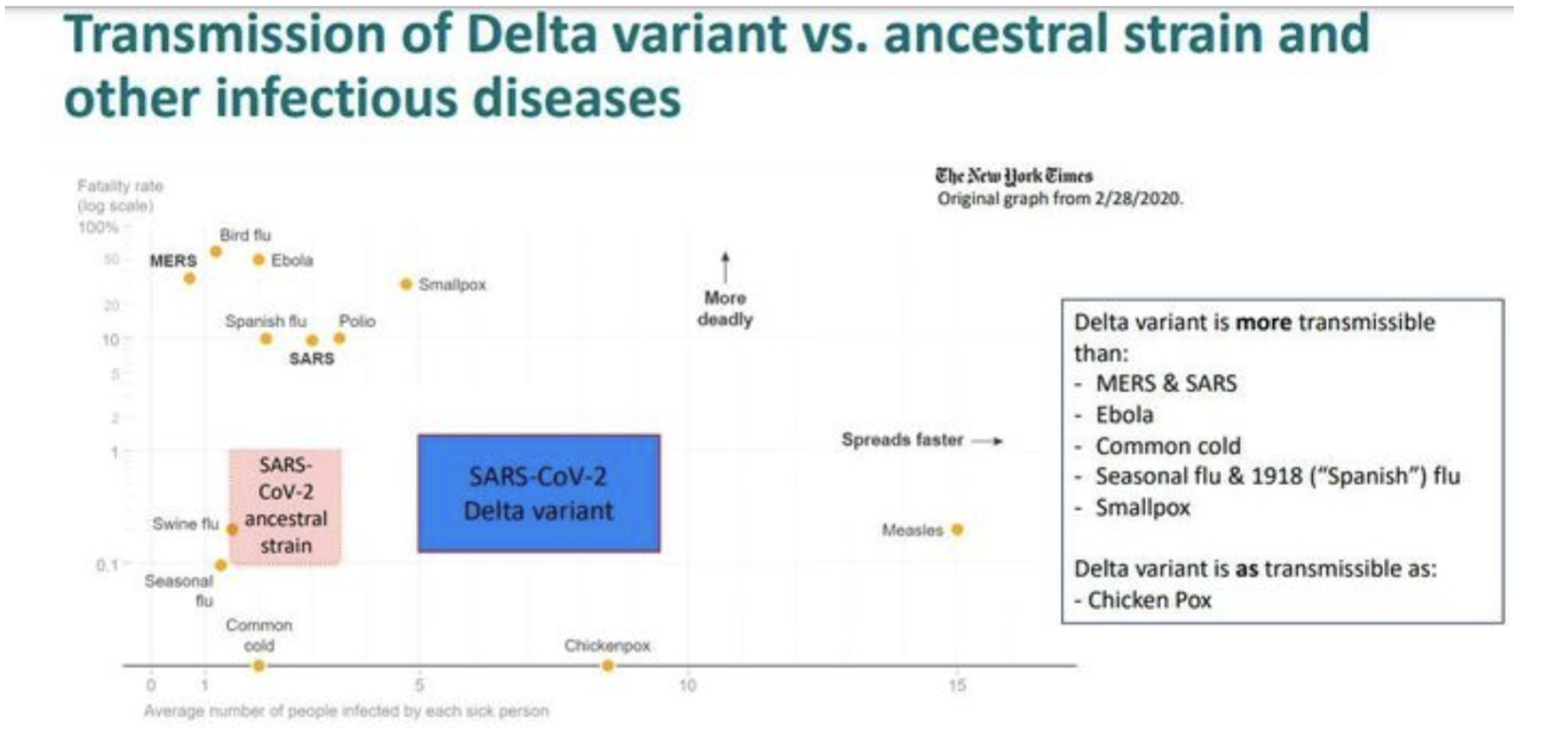
- R0 of some viral diseases [CEBM, Oxford] [delta] [omicron]
- seasonal flu: 1.4-1.6
- Ebola: 1.5-2.5
- 1918 flu: 2-3
- HIV: 2-5
- polio: 5-7
- smallpox: 5-7
- chickenpox 7-10
- measles: 12-18
- Covid 1.0: 2.3-3
- Covid a: 4-5
- Covid D: 3-6
- Covid O: 5.5-13
- cases may be seasonal due to several factors [Brock 28-18]
- due to biology of pathogen and behavior of susceptibles
- basic reproductive ratio (R0)- average number of new cases from each infected individual
- Incidence (number) and prevalence (proportion) [Brock 28-2] [figure 28.24a]
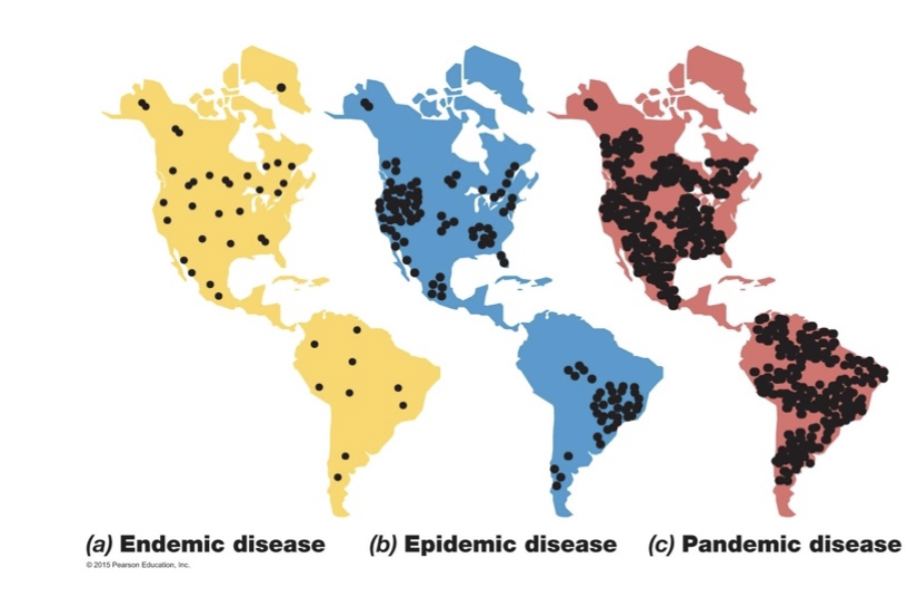
- sporadic- occasional occurrence at irregular intervals
- endemic- constant low level
- outbreak- localized increase
- epidemic- increase in incidence
- pandemic- widespread epidemic
- Reporting and Statistics [figure 1.10]
- diagnosis and testing- county, state, national labs
- surveillance- reporting networks [table 28.5]
- both known and emerging diseases
- morbidity- number of cases
- mortality- number of deaths
- CFR vs. IFR
- case fatality rate (CFR)- deaths/confirmed cases
- infection fatality rate (IFR)- deaths/infected (known or not)
- deaths attributed to Covid can vary somewhat
- but number of confirmed cases compared to total infected varies substantially
- availability and ubiquity of testing
- asymptomatic or mild cases that do not get tested
- consistency of diagnosis & reporting
- Covid-19 in US: cases- 111.8m; deaths 1.22m; CFR 1.1% [Worldometer]
- IFR 0.4% (my guess from 3 years ago)
- seasonal flu: CFR 0.1-0.2%; IFR 0.02%- 0.05%
- doesn’t measure other consequences (lung damage, myocarditis, brain fog, anosmia)
- Another way of looking at Covid [MarketWatch, 7/31/21]
- Evolution of new strains depends on...
- mutation rate of virus- more or less constant based on fidelity of RDRP
- selective advantage of the mutants- more or less random
- advantage to increased infectivity
- indirect advantage to decreased virulence (if it allows longer contagious period)
- number of infected individuals- allows for more chances for mutation
- Control [Brock 28-7]
- eliminating reservoirs
- sewage treatment
- treatment of infected individuals
- destroying infected animals
- minimizing transmission
- vector control- mosquito spraying & rodent killing
- chlorination of water
- food handling and preparation practices
- limiting contact between infected and susceptible individuals
- quarantine the infected/exposed- if you can identify quickly and enforce strictly
- limit all movement/contact (masking and lockdowns, if you can enforce that)
- vaccination of susceptible populations [Brock 28-8]
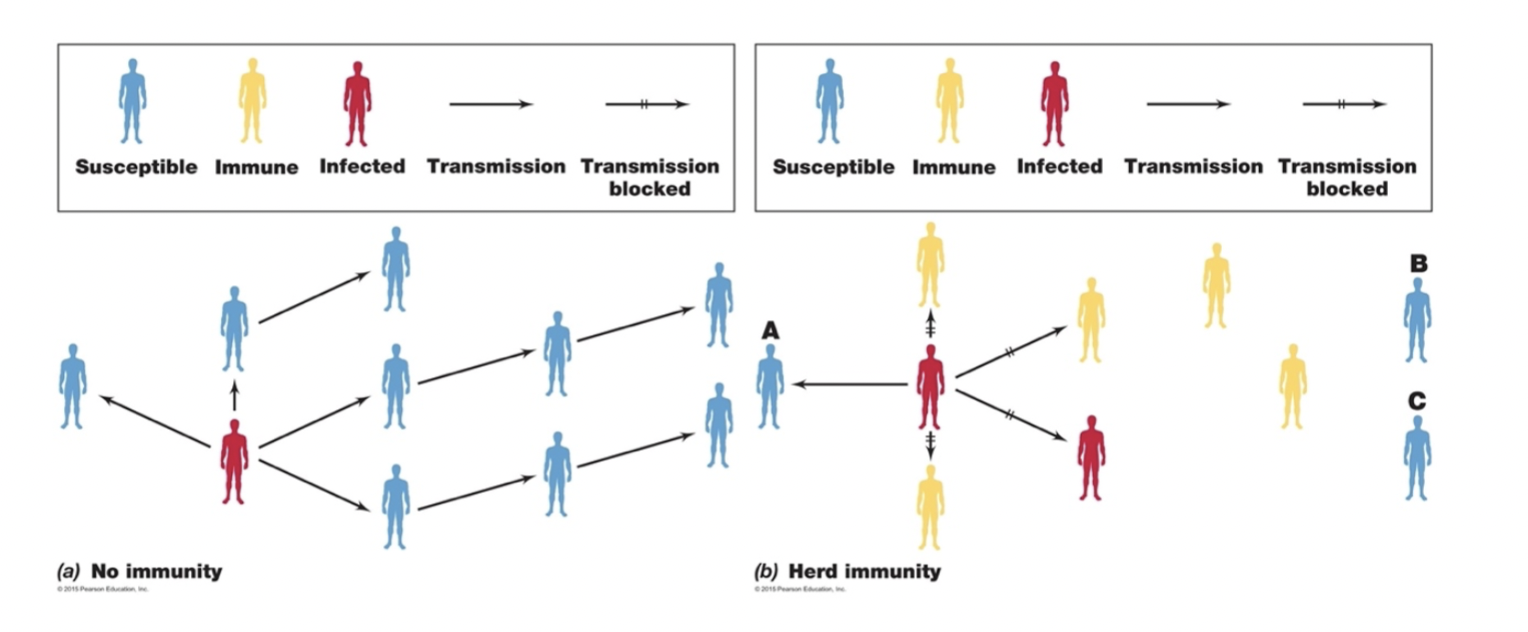
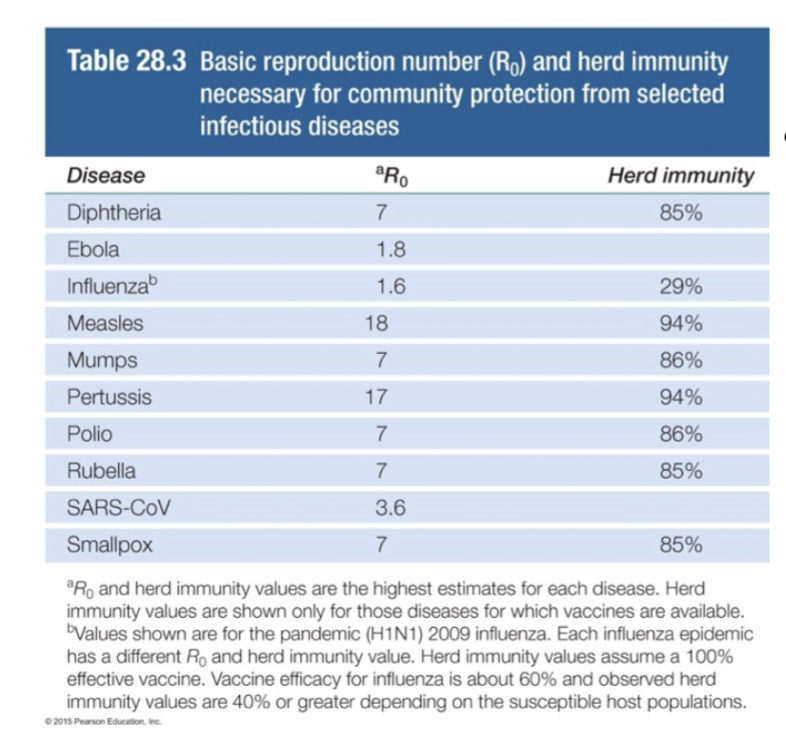
- herd immunity- disease spread is limited if percent immune in population is above transmission threshold [Brock T28-3] [Brock 28-4]
- threshold = 1-1/R 0 (so, 80%-88% for Covid D)
- herd immunity- disease spread is limited if percent immune in population is above transmission threshold [Brock T28-3] [Brock 28-4]
- includes immune due to vaccination and recovery
- eliminating reservoirs
- But...
- immunity can wane in vaccinated/recovered individuals
- how long? months? years?
- vaccinated vs. recovered?
- strain variation- change in pathogen makes population susceptible again
- “breakthrough” cases
- vaccines 90% effective, now 65% effective?
- immunity can wane in vaccinated/recovered individuals
Correlations with Virulence
- Virulence = ability to cause disease
- use animal models to estimate LD50 (dose resulting in 50% mortality) [figure 25.5]
- in many cases, virulence due to acquired traits [Brock T28-7] [figure 25.9]
- toxin production, adherence, protection from phagocytosis, nutrient acquisition
- attenuated (lower virulence) strains used to immunize
- Mode of transmission
- close contact- pathogen virulence is less
- carrier must be well enough to come into contact with other hosts
- vector borne- pathogen has higher virulence
- incapacitated host easier target for vector
- pathogen builds up to high numbers inside host to increase likelihood of transmission
- no selection for co-existence if pathogen can survive in the vector
- close contact- pathogen virulence is less
- Survivability of Pathogen
- high survivability outside host- pathogen has greater virulence
- low survivability outside host- pathogen has lesser virulence
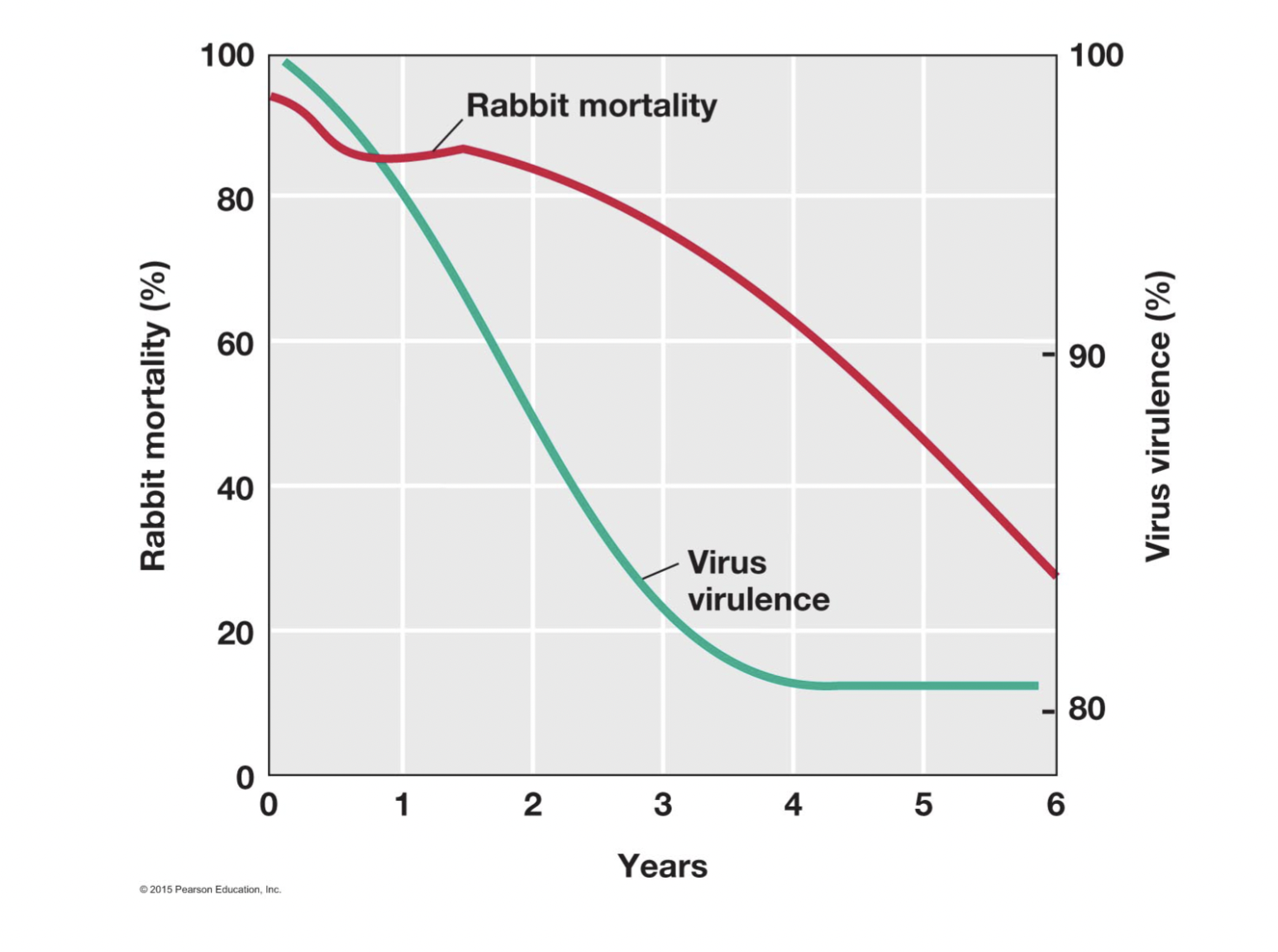
- Co-evolution of host and pathogen
- new disease- greater virulence
- established disease- lesser virulence
- shift from acute to chronic disease
- initial epidemic leaves resistant survivors
- example- myxomatosis virus in Australian rabbits [Brock 28-3]
Emerging and Reemerging Infectious Diseases [figure 28.30] [Brock T28-6]
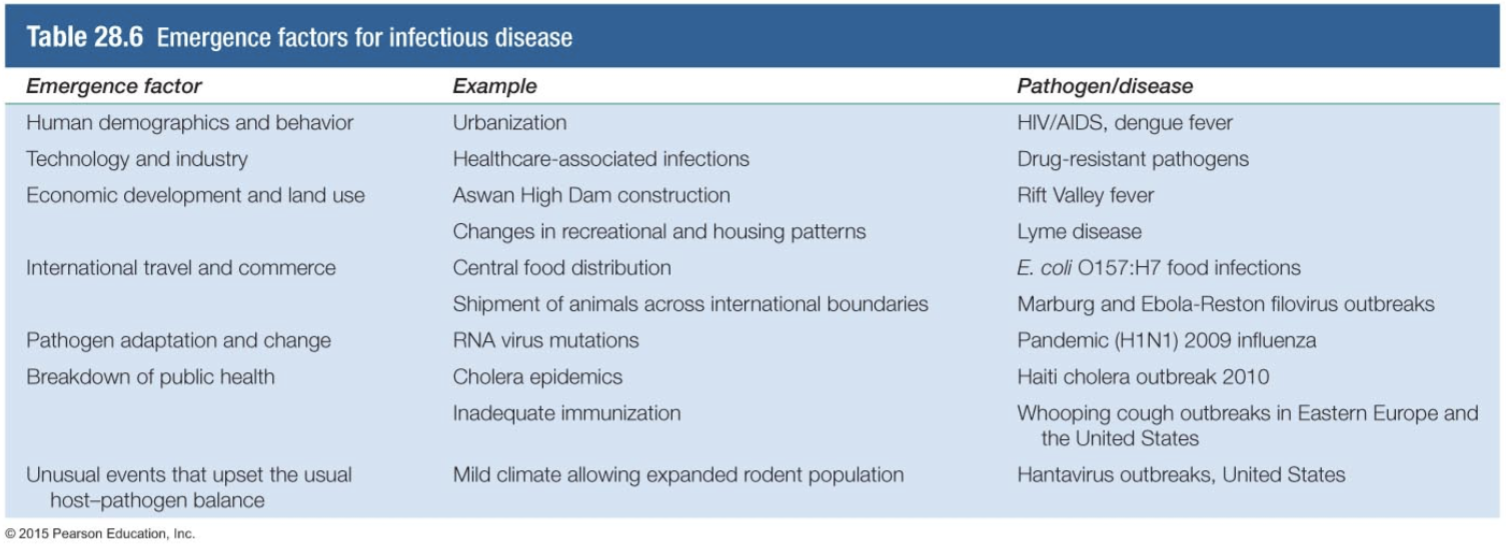
- Increasing population
- migration from tropics to temperate or rural to urban
- higher density increases exposure and efficiency of transmission
- Changing land use
- expansion of cities to edge of forest or jungle
- new habitats bring exposure to novel pathogens
- damming rivers for power and irrigation
- expansion of cities to edge of forest or jungle
- Industrialization of agriculture and food processing
- increased density of animals promotes disease
- centralized distribution magnifies failures
- Rapid global transportation
- Changes in behavior
- sexual behavior
- drug use
- food preferences
- Evolution of pathogens
- mutation --> drift and shift of recognized antigens
- selection for drug resistance
- Immunosuppressed individuals (e.g., AIDS patients, chemotherapy & transplant recipients)
- increase in susceptible individuals due to medical technology
- vulnerable to opportunistic pathogens
- provide an environment for rapid evolution
- Disruption of public health systems
- disaster
- economic neglect
- political unrest
- non-compliance with vaccination/quarantine
- Climate change
- change in range/survivability of disease vectors
- Bioweapons/biowarfare/bioterrorism? [figure 28.26] [Brock T28-8]
- Public response [Slon5, figure 1.9a] [figure 1.9b]
Lecture 31- Airborne Diseases
General Considerations
- Air is not a habitat
- organisms cannot grow in it
- organism is transiently present in droplet or as aerosol particle from infected host
- respiratory droplets traditionally defined as aqueous drops >5 μm diameter
- drops evaporate as they fall to ground [Wells curve]
- larger drops deposit organism on surface (hit ground before they evaporate)
- smaller drops evaporate to form droplet nuclei (aerosol) 1-4 μm diameter
- aerosols can remain airborne longer and travel farther
- a lot of debate, but IMO not any meaningful rules that come out of this
- organism must tolerate drying during passage from source to host
- Gram-positive bacteria have advantage over Gram-negative
- bacterial or fungal spores do better
- some viruses are better than others
- Outdoor Air
- lower overall numbers of microbes
- more bacteria from soil (spore-formers)
- more molds
- Indoor Air
- lower turnover rate, more crowded for people
- higher overall numbers
- preponderance of human respiratory bacteria
- a single sneeze, 100 m/sec (200 mph), 10,000-100,000 bacteria [Brock 26-1]
- Inhalation of spores/droplets is the mechanism of entry
- humans breathe 7-8 liters of air/minute, 10,000+ liters/day
- respiratory tract is the obvious site for infection
- but infection not necessarily limited to respiratory tract [Brock 26-2]
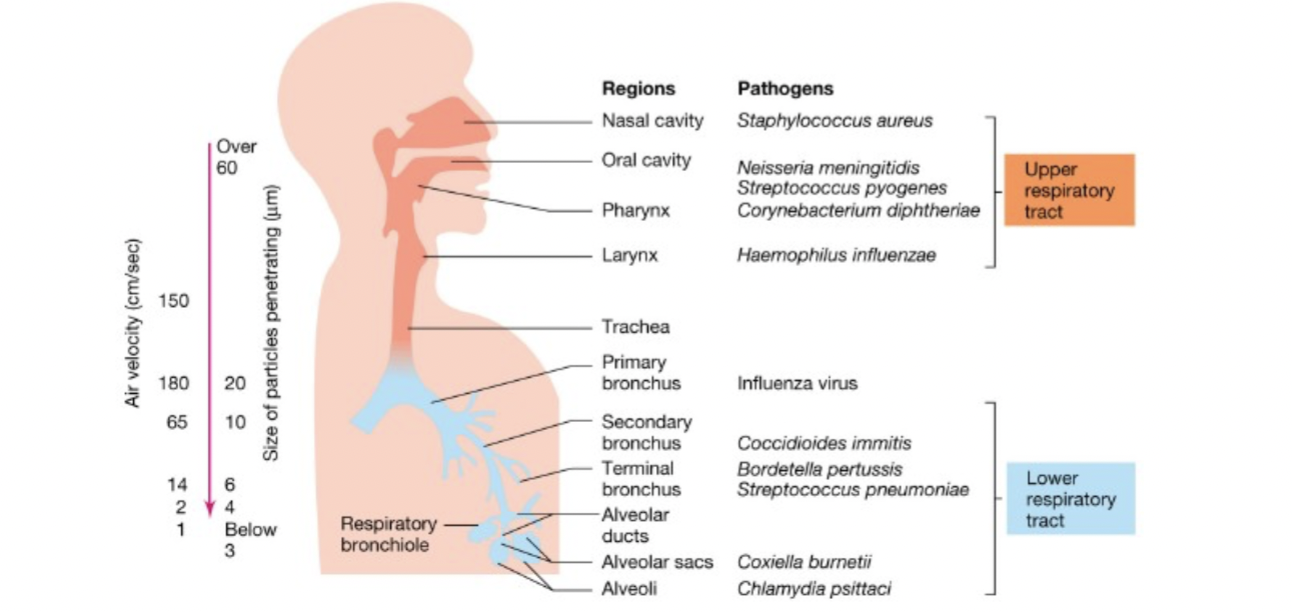
Bacterial Diseases [table 26.2]
- Mycobacterium tuberculosis- tuberculosis
- the organism
- Gram-positive bacillus
- mycolic acids in cell wall detected by "acid-fast" staining procedure [figure 18.21]
- tuberculosis (consumption)
- the most deadly, single-agent, infectious disease of humans
- one-quarter of world population infected, new cases = to 1% of population/year
- accounts for ~1.6 million deaths per year worldwide (1000 in U.S.)
- establishment of infection [figure 26.11]
- inhalation of droplets into lungs from person with active infection
- bacteria are phagocytized, but grow in macrophages [macrophage] [figure 25.32]
- change pattern of cytokine expression → less inflammation
- down-regulate receptors for inflammatory cytokines
- reduce MHC-I protein synthesis
- prevent programmed cell death of infected cells (initially)
- prevent autophagy
- immune cells and fibroblasts form granuloma around infected cells (tubercles)
- lesions change consistency (Ghon complexes show up in X-rays) [Ghon]
- disease most often (90%) stops here as a latent infection but can become...
- active infection
- symptoms- fever, fatigue, weight loss, cough with bloody sputum
- cough makes person highly contagious
- primary active infection occurs in some cases
- bacteria grow unchecked in lungs
- secondary active infection occurs if immune system is weakened (HIV, etc.)
- allows escape of bacteria from nodules
- bacteria can spread to form nodules throughout the body (miliary tuberculosis)
- symptoms- fever, fatigue, weight loss, cough with bloody sputum
- the most deadly, single-agent, infectious disease of humans
- test for previous exposure by skin test
- protein from M. tuberculosis is injected intracutaneously
- hardening and reddening of skin in 48 hours is positive test
- seroconversion = switching from negative to positive test result
- treated by four-drug combination: isoniazid, rifampicin, pyrazinamide and ethambutol
- administered for 6+ months
- treatment with multiple drugs right away makes it less likely drug resistance arises
- yet, multiple drug resistant cases have emerged in last 30 years
- MDR TB = resistant to two or more of the front-line antibiotics
- XDR TB = resistant to three or more second-line antibiotics
- incomplete or serial treatment allows resistant bacteria to become common
- eradicating antibiotic resistant bacteria is a combination of antibiotic keeping bacteria under stress and immune system killing bacteria
- Bacillus Calmette-Guerin (BCG) vaccine
- given to babies after birth with few side effects
- reduces infection 20%, progression from latent to active infection 50%
- protection lasts up to 20 years
- don’t use the vaccine, because it’d make the skin test useless
- the organism
- Streptococcus pyogenes
- the organism
- anaerobic Gram-positive cocci
- grow in long chains, do not produce spores
- much strain-to-strain variability in other toxins, virulence factors
- can be part of normal upper respiratory flora
- strep throat- sore throat, tonsillitis, tender lymph nodes, mild fever and malaise
- rapid diagnosis by latex bead agglutination, ELISA or fluorescent antibody staining
- confirmation by throat culture on blood agar plates
- inner ear infection (otitis media)
- mastitis- infection of breast tissue associated with breast-feeding
- impetigo- skin lesion
- scarlet fever- high fever, lethargy, sore throat, and a bumpy skin rash [strawberry tongue]
- caused by strain carrying toxin acquired via lysogen
- rheumatic fever- inflammation of heart, joints skin and brain
- can occur after case of strep throat
- some strains carry surface antigens similar to host antigens
- cross-reactivity of anti-streptococcal antibodies lets immune system attack host tissue
- glomerulonephritis- kidney failure
- antibody-antigen complexes clog kidney
- causes inflammation & severe pain
- depends of strain specific antigens
- necrotizing fasciitis- "flesh-eating" disease [figure 26.4]
- some strains secrete proteases and DNases when they penetrate mucus membrane
- immune response to these toxins causes much of the damage
- streptococcal toxic shock- drop in blood pressure, multiple organ failure, high fever
- due to superantigens overstimulating immune system
- the organism
- Streptococcus pneumoniae- pneumonia [figure 26.8]
- one of many agents to cause pneumonia
- also causes diseases of bone, inner ear and endocarditis
- capsule makes cells resistant to phagocytosis, allows it to invade lung tissue
- vaccine is a mix of capsular antibiotics
- Corynebacterium diphtheriae- diphtheria
- lodges in upper respiratory tract
- inflamed host tissue and bacteria make a "pseudomembrane"
- diphtheria toxin comes from lysogen
- Bordetella pertussis- whooping cough
- adheres via filamentous hemagglutinin antigen
- toxins cause tissue damage, symptoms
- Mycobacterium leprae- leprosy
- organism grows within macrophages
- nodular lesions under skin
- peripheral nerves killed, loss of motor function
- Neisseria meningitidis- meningococcal meningitis
- inflammation of spinal cord, brain tissue
- part of normal flora for some people
Viral Diseases [table 26.2]
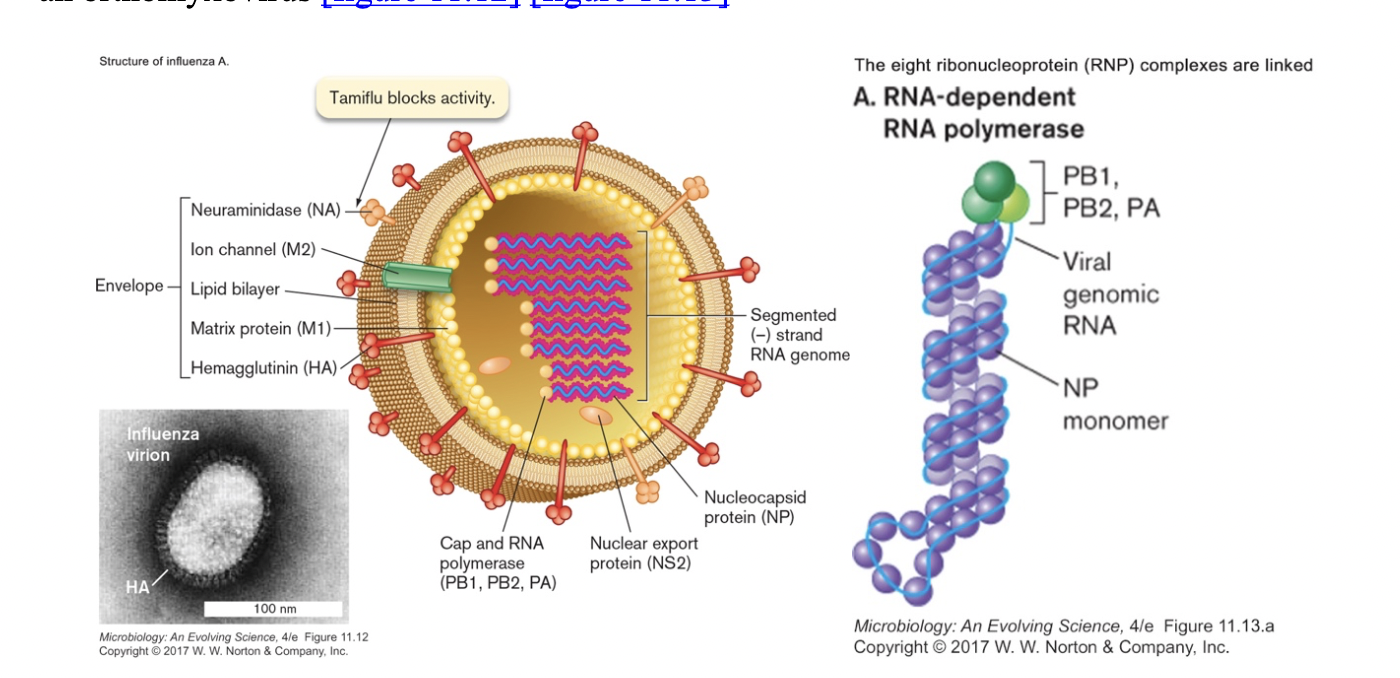
- Influenza virus- flu
- an orthomyxovirus [figure 11.12] [figure 11.13]
- four major types (A, B, C, D)
- named by type, place of origin, lab number, and year
- also named by the type of HA and NA proteins it carries
- animal it was isolated from, if not a person
- example- Influenza A/Sydney/5/97 (H3N2)
- segmented (-) strand RNA genome (8 pieces, 890 to 2341 bases long) [figure 11.15]
- an enveloped virus with two "spike" proteins
- hemagglutinin (HA)- attachment of virus to sialic acid on cell surface
- an enveloped virus with two "spike" proteins
- four major types (A, B, C, D)
will agglutinate red blood (and epithelial) cells
anti-HA neutralizes virus
- neuraminidase (NA)- helps in viral assembly/release
- eight other proteins
- RNA-dependent RNA polymerase (PB1, PB2, PA)
- nucleocapsid (NP)
- other structural proteins (M1, M2)
- interferon suppression (NS1)
- nuclear export protein (NS2)
- segments facilitate antigenic shift, mutations cause antigenic drift [figure 11.17]
- bird & swine flu are related viruses [figure 11.18]
- wild aquatic birds (ducks) appear to be a natural reservoir
- virus is avirulent in water fowl; shed in feces, transmitted via water
- pigs are the "mixing bowl" where human, avian and swine variants co-infect
- packaging of different segments allows new combinations
- outbreaks can then occur in domestic poultry or humans
- human to human transmission via aerosol droplets {anim 11.01}
- likely also by physical transmission (hand to mouth) from contaminated surfaces
- mask and hand-washing both effective at reducing transmission
- reproduces in epithelial cells of upper respiratory tract and lungs {anim11.02}
- molecular details of infection provide clues for drugs [figure 11.19] [figure 11.20]
- person may be contagious before they show symptoms
- likely also by physical transmission (hand to mouth) from contaminated surfaces
- outbreaks occur seasonally in winter (year-round in tropical climes)
- estimated 20% of unvaccinated children, 10% of unvaccinated adults infected/year
- 3-5 million severe cases annually, 250,000-650,000 deaths worldwide (36,000 in US)
- disproportionally among young, old and those with underlying health problems
- symptoms- fever, runny nose, sore throat, coughing, fatigue, muscle pain, headache
- secondary bacterial or viral infection (pneumonia) causes death
- immunity develops after infection
- strain specific, only lasts a few years
- new vaccines produced yearly against strains predicted to be most common
- decisions are made in February (September in S hemisphere) for following winter
- need time to gear up and produce enough doses
- antiviral drugs target virus-specific proteins [figure 27.32]
- amantadine- blocks M2, acidification in endosome, uncoating
- tamiflu & zanamivir- block action of neuraminidase, budding out of new virus
- show some effectiveness if given early in disease
- shaves one day off time to recovery
- lessens complications in elderly
- no prophylactic effect if given to healthy people
Tuesday, June 18, 2024
Lecture 31- Airborne Diseases
Viral Diseases [table 26.2]
- flu pandemics
- disease has been described back to ancient Greeks
- pandemic of 1918-20 H1N1
- origin not conclusive, possibly Europe, possibly China
- or US? first recorded cases in Haskell County, Kansas, January 1918
- Dr. Loring Miner, in a letter to the U.S. Public Health Service described a new strain of flu. He observed:
- flu pandemics
"violent headache and body aches, high fever, non-productive cough. . . . This was violent, rapid in its progress through the body, and sometimes lethal. This influenza killed. Soon dozens of patients—the strongest, the healthiest, the most robust people in the county—were being struck down as suddenly as if they had been shot."
- from there it spread to Camp Funston, Kansas
Pvt Albert Gitchell becomes the first recorded case on March 4, 1918
- US troops spread disease to New York and French ports by April
- spread throughout western front and western Europe generally
- released Russian prisoners of war bring it back to Russia in May
- reached China in June, Australia in July
- somehow got the name of Spanish flu, though mortality there no worse
- returning troops in Fall bring home a second wave, much deadlier
- estimated one-third of human population infected through four waves
- killed ~20-50 million worldwide, 675,000 in US (more than WW I & II)
- US troops spread disease to New York and French ports by April
195,000 in October 1918
- human population only 1.8 billion, so 1-3% of all humans died!
- disease course was different
- much higher mortality (CFR = 2.5% rather than 0.1%)
- higher mortality among 20-40 year olds than typically [w-curve]
- rapid pulmonary edema (immune system overreaction- cytokine storms)
- followed by rampant pneumonia (secondary infections killed most victims)
- made it difficult to determine actual cause of disease
viral cause not known until 1930!
- have tried to sequence & recover virus from preserved tissue, Norwegian miners, eskimos buried in permafrost
- virus seems to have jumped from chickens/ducks to humans and pigs
- was of the H1N1 subtype
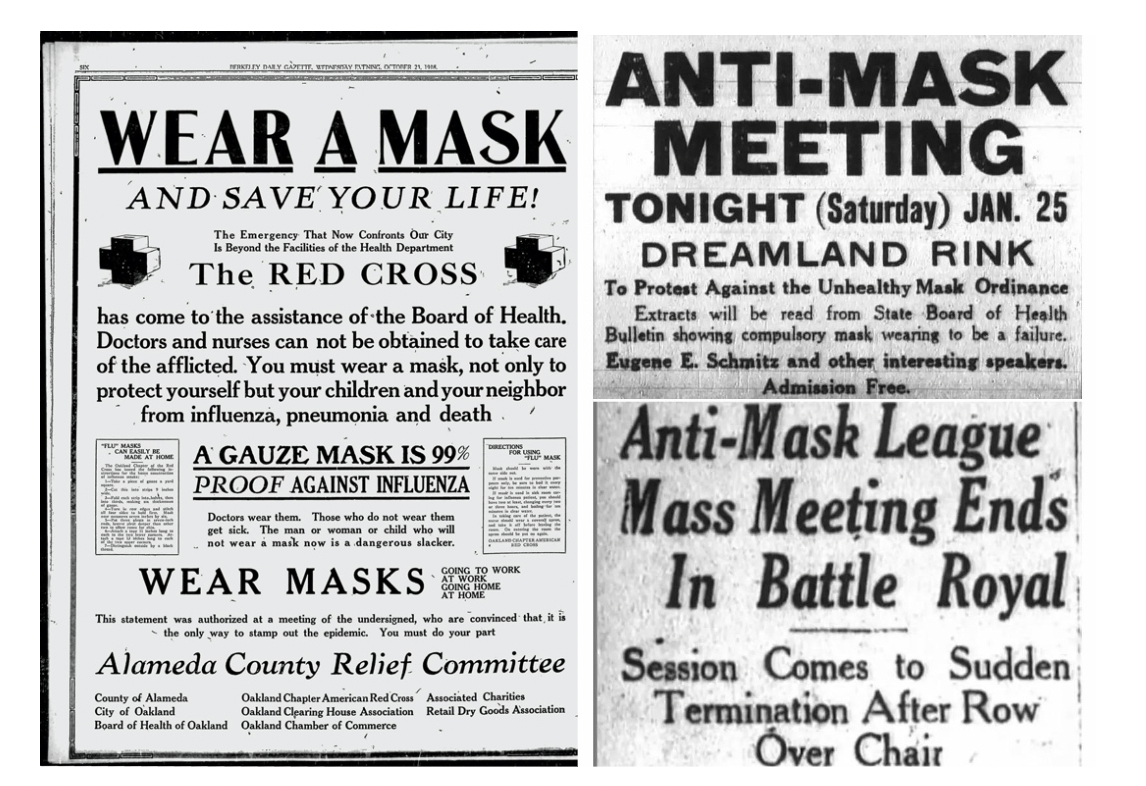
- lessons
- misinformation just spreads the virus
- quarantine in place
- super-spreaders: bond parades, world series games, armistice celebrations
- mask slackers will be mask slackers: anti-masking league in San Francisco
- have tried to sequence & recover virus from preserved tissue, Norwegian miners, eskimos buried in permafrost
- 1889-90 Russian flu (1 million deaths worldwide)
- 1957-58 Asian flu H2N2 (1-4 million deaths worldwide)
- 1968 Hong Kong flu H3N2 (1-4 million deaths worldwide)
- 2004 Bird flu H5N1
- 2009 Swine flu H1N1 (150-600,000 deaths worldwide)
- Severe Acute Respiratory Syndrome (SARS-CoV-1)
- 10% mortality in infected persons
- 2003 outbreak → panic of next flu pandemic
- Covid19 (SARS-CoV-2)
- 2019-2024 outbreak
- 705 million confirmed cases, 7.01 million deaths
- Respiratory Syncytial Virus (RSV)
- causes pneumonia in infants
- Rhinoviruses- cause the common cold
- many different viruses cause similar symptoms
- 3 per year?!!
- Rubeola virus- measles
- complications can cause death
- major worldwide vaccination campaign
- 1998- 30 million cases, 900,000 deaths
- 2002- 610,000 deaths
- Mumps virus- mumps
- infection of the salivary glands
- Rubella virus- German measles
- dangerous to fetus if contracted while pregnant
- Varicella virus- chicken pox
- new vaccine (1994)
- remains dormant in nerve cells
- reemergence = shingles
Fungal Diseases [table 26.2]
- Coccidioides immitis- coccidioidomycosis (desert southwest)
- Histoplasma capsulatum- histoplasmosis (Ohio & Mississippi river valleys) [figure 26.10b]
- Blastomyces dermititidis- blastomycosis (Great Lakes & midwest)
Lecture 32- Contact Diseases
Contact Diseases
- General considerations
- spread by person-to-person contact or indirect contact with contaminated objects
- includes contact with blood and bodily fluids
- or during birth
- causative agent cannot survive outside host very well
- spread by person-to-person contact or indirect contact with contaminated objects
- Staphylococcus aureus
- the organism
- Gram-positive coccus [figure 26.3a]
- non-sporeforming, resistant to drying
- part of normal flora for carriers (e.g., hospital staff)
- upper respiratory tract (nose and throat)
- skin
- diagnosis
- rapid immunological detection
- culturing
- serology
- skin infections
- boils [figure 23.31] and pimples- infection of hair follicles
- impetigo [impetigo]- crusty skin lesions
- scalded skin syndrome [figure 26.3b]- strains carrying exfoliative toxin
- a superantigen, cleaves skin protein → extensive blistering
- MRSA/VRSA- methicillin/vancomycin resistant Staph aureus [figure 17.21]
- mutation in penicillin-binding proteins
- wound and systemic infections also possible
- toxicities
- food poisoning- due to enterotoxin in food (e.g., potato salad at church picnic)
- fast effect (doesn't require growth of organism in body) since toxin is in food
- intestinal T-cell response
- increased fluid permeability
- severe diarrhea
- vomiting
- toxic shock syndrome- superantigen causes massive T-cell response
- symptoms
- inflammation
- low blood pressure
- sudden high fever
- vomiting
- diarrhea
- skin rash
- first gained publicity from deaths associated with super-absorbent tampons
- but also seen with contraceptive sponges
- wound dressings
- nasal packing
- drying out mucus layer favors S. aureus, can irritate epithelial tissue
- change tampons/sponges/bandages regularly
- symptoms
- food poisoning- due to enterotoxin in food (e.g., potato salad at church picnic)
- virulence factors
- coagulase- clots fibrin, walls off site of infection
- leukocidin- kills white blood cells, leads to pus
- hemolysins- are general cytolysins [figure 25.17]
- proteases- break down proteins
- lipases- break down lipids
- nucleases- break down DNA & RNA
- slime- biofilms, adherence, antiphagocytic
- protein A- binds Fc region of antibodies, lessens phagocytosis
- treatment- various antibiotics for infections
- the organism
- Helicobacter pylori - stomach ulcers
- Gram-negative spiral shaped bacterium
- grows in mucus lining of stomach
- only discovered in 1983
- accepted as cause of ulcers in 1994
- Barry Marshall drank culture and gave himself an ulcer
- cured it by antibiotics
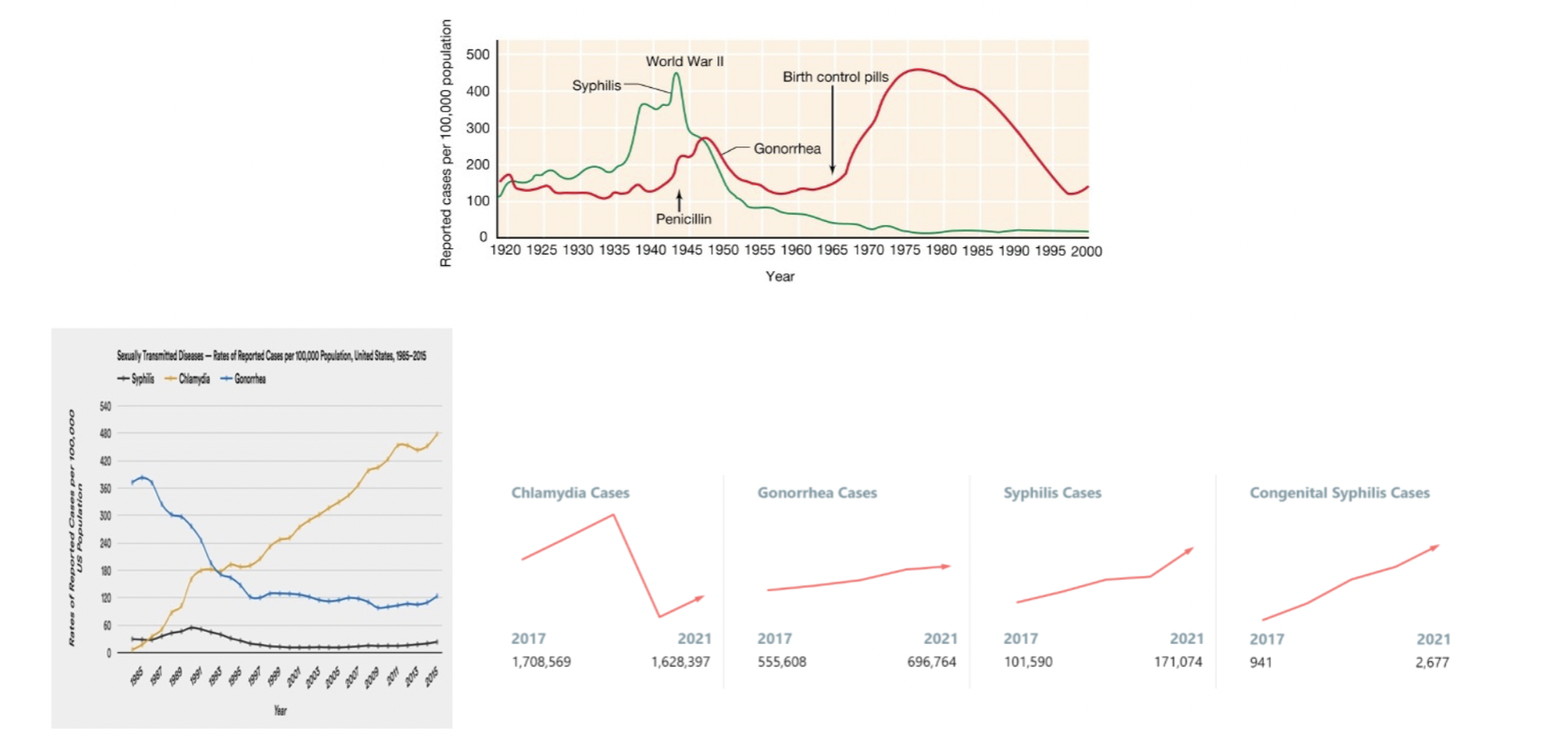
Sexually Transmitted (Venereal) Disease [table 26.5] [Brock 26-26] [CDC] [2019]
- A subset of contact diseases
- requires intimate contact between infected individual and next host
- inasmuch as sexual behavior is varied, different tissues can be infected
- Eukaryotic STDs
- Trichomonas vaginalis- protist causing trichomoniasis [Slon5, figure 26.23]
- infects urethra, vagina, prostrate & seminal vesicles
- generally asymptomatic in males
- leukocytes accumulate in response to infection in females
- yellowish-green discharge with "disagreeable" odor
- itchiness/tenderness/swelling & burning during urination
- very common
- 3-5 million cases/year in US
- 10-15% of STD cases in women
- diagnosis- microscopic examination of fluid discharge
- treatment- metronidazole
- infects urethra, vagina, prostrate & seminal vesicles
- Trichomonas vaginalis- protist causing trichomoniasis [Slon5, figure 26.23]
- Bacterial STDs
- Treponema pallidum- the "great pox", syphilis (together-love)
- spirochete bacterium [figure 26.25a]
- surging! ~200,000 US cases/year
- history
- brought back by Columbus?
- first "recognized" outbreak Naples, 1494 (Neapolitan disease)
- in army of Charles VIII (French disease)
- containing Spaniards from Columbus' crew (Spanish disease)
- also the Polish disease in Russia, the Russian disease in Siberia, the Christian disease in Turkey, and the Portuguese disease in India and Japan
- but described by Hippocrates in classical Greece?
- bones found in 13th century English friary- syphilis or leprosy?
- sequencing data indicate similarity to S American strains of yaws
- yaws and pinta are also treponemal diseases, but not sexually transmitted
- new strain, increase in virulence or Europeans especially susceptible?
- brought back by Columbus?
- Treponema pallidum- the "great pox", syphilis (together-love)
seems to be less deadly now then during Columbus' time
- first "new" disease after printing press, first recognized as sexually-transmitted
- symptoms
- primary
- chancre (hardened inflammation) at site of infection [figure 26.25b]
- primary
chancre is painless and heals without scarring in several weeks
- these days, obvious symptoms (should) lead to treatment and cure
- secondary
- skin rash 1-6 months after primary [figure 26.25c]
- generalized hypersensitivity reaction
- is when patient is most contagious
- tertiary
- 1-10 years after initial infection
- gummas- soft tumor-like growths
- joint and spinal deformities (tabes)
- personality changes and dementia
- cardiovascular complications
- congenital transmission to newborn
- Tuskegee experiment
- grows from effort of northern philanthropists and prominent black leaders to improve health & economic development of southern blacks
- Tuskegee institute teaches trade skills
- 1929- initiative with US Public Health Service to tackle syphilis
- grows from effort of northern philanthropists and prominent black leaders to improve health & economic development of southern blacks
estimated at 35% prevalence locally
treated with mercury & bismuth creams
toxic, <30% cure rate
arsphenamine (Salvarsan), an arsenic-based medicine, also was available but required expertise to prepare and administer
then private money runs out
- new study, 1932- follow 399 infected black men (and 201 uninfected controls) to observe long-term effects of untreated syphilis
- document racial differences in progression
- new study, 1932- follow 399 infected black men (and 201 uninfected controls) to observe long-term effects of untreated syphilis
men were recruited with free medical care, meals & burial insurance
never given true diagnosis, were told they suffered from "bad blood"
- hoping to make case for funding/treatment?
- bureaucratic survival of program?
provided training for medical interns, employment for nurses
careerist prestige for those involved?
- racism?
surely yes, in the attitude administrators had towards the participants
John Heller, director of the Venereal Diseases unit of the PHS from 1943 to 1948 -- "The men's status did not warrant ethical debate. They were subjects, not patients; clinical material, not sick people"
- inexcusably continued 25 years (until 1972!) after cure was known
Public Health Service denied information to patients
actively prevented treatment for patients drafted into army
40 wives and 19 children infected
- finally stopped by a leak to the press
- led to wholesale revision of studies involving humans, informed consent
- has also caused lingering distrust of public health institutions
- Neisseria gonorrhoeae- gonorrhea [figure 26.27]
- Gram negative non-sporeforming coccus
- infects genitourinary and other mucus membranes
- symptoms
- female- often asymptomatic
- can cause pelvic inflammatory disease, scar tissue, ectopic pregnancy, sterility
- disseminate during menstruation because of iron availability
- male- yellow discharge, painful urination
- systemic complications in both sexes (joints, heart, pharynx)
- congenital transmission to newborn → blindness
- female- often asymptomatic
- >700,000 confirmed US cases/year
- no acquired immunity
- oral contraceptives raise vaginal pH, favor Neisseria
- females are asymptomatic reservoir, so may be many more cases than known
- Chlamydia trachomatis- chlamydia/nongonococcal urethritis [figure 26.26]
- obligate intracellular parasite- reticulate vs. elementary bodies
- very common- 1.6-1.8 million US cases/year?
- many asymptomatic
- symptoms
- yellow or clear urethral discharge
- pain and tenderness in the genitals
- pain, burning, and itching during urination
- low-grade fever
- can lead to pelvic inflammatory disease, sterility in women
- Viral STDs
- Herpes simplex virus- herpes [anim 11.04]
- double-stranded DNA viruses
- HSV1- primarily epithelial tissue of mouth and lips
- cold sores & fever blisters
- spread via saliva, contact
- remains latent in nerve cells
- periodically reemerges
- HSV2- primarily epithelial tissue of genitourinary tract
- painful blisters on penis, vagina, cervix, vulva
- spread via sexual contact
- remains latent
- periodically reemerges
- HSV1 & 2 can infect "other's" area
- nucleotide analogs limit reemergence but do not cure
- HIV- AIDS [figure 26.28] [Brock T28.9] [anim11.03]
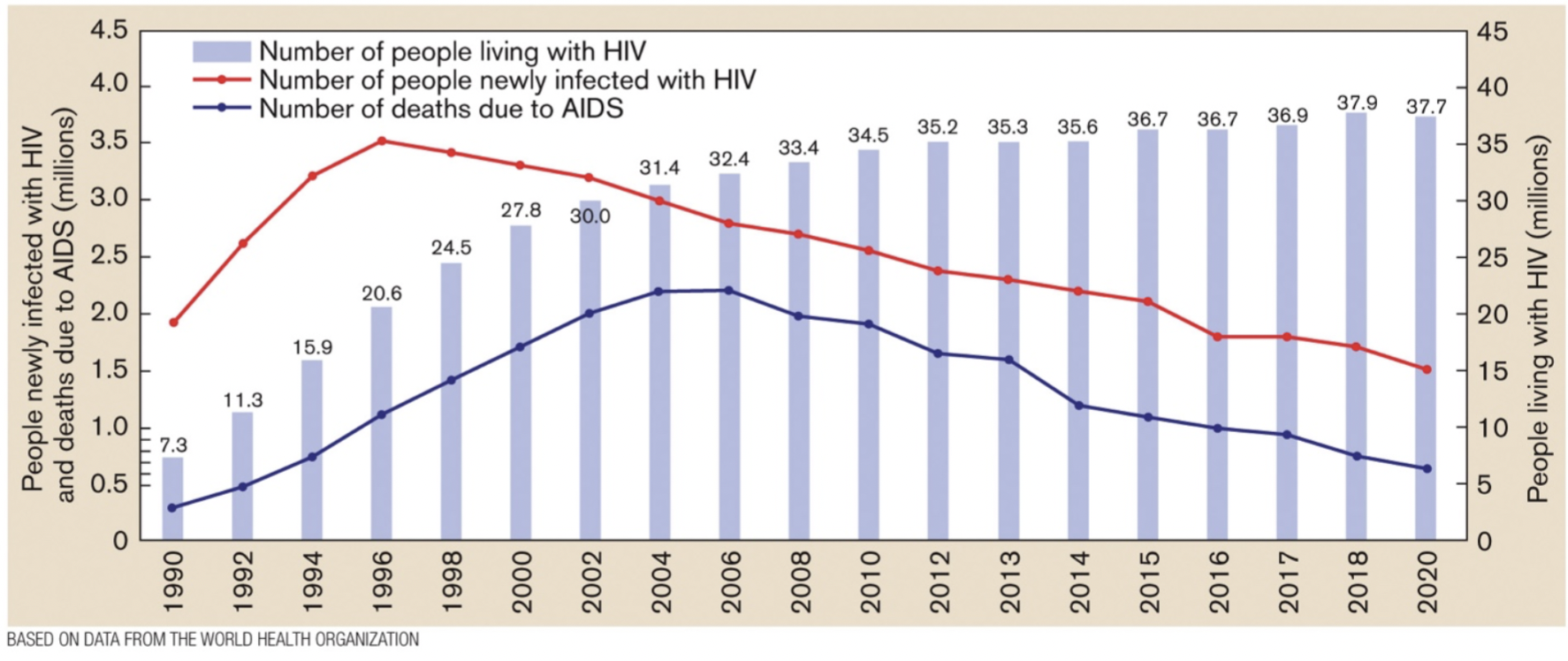
- retrovirus
- infects CD4 + cells (TH cells)
- many secondary infections develop [figure 26.28]
- managed by cocktail of base analogs, reverse transcriptase & protease inhibitors
- Herpes simplex virus- herpes [anim 11.04]