Respiratory
URTI - more viral
LRTI - acute bronchitis & pneumonia
Acute Bronchitis
Definition - inflammation of the bronchi
Clinical features
Cough - dry —> productive (clear/white/yellow sputum)
Wheeze
Dyspnoea
Mild fever
Diagnosis
Clinical
CXR if suspect pneumonia
Management
Pain relief
Abx if bacterial infection
Asthma
Bronchiectasis
Definition - dilation of bronchi
Aeitology
Chronic inflammation
Post-infection - TB, pneumonia
Immunodeficient - HIV
Connective tissue disorders - Marfan’s, RA, SLE
Congenital - CF (must exclude)
Clinical features
Persistent cough with purulent copious sputum
Chest pain, dyspnoea, haemoptysis
Coarse crackle on early inspiration —> lower zones
Wheeze
Diagnosis
HRCT — bronchial dilation, bronchial wall thickening
Management
Bronchodilators
Chest physical therapy
Postural drainage
Smoking cessation
Immunisation - influenza, pneumonia
Chronic obstructive pulmonary disease (COPD)
Definition - lung disease that has 2 types - chronic bronchitis + emphysema
Risk
Interstitial Lung disease
Diseases that cause inflammation & fibrosis to the pulmonary interstitium
Pulmonary Fibrosis
Definition - progressive scarring of lung tissue
Causes:
Idiopathic pulmonary fibrosis
Sarcoidosis
Asbestosis
Hypersensitivity pneumonitis
Risk factors
Male
50-70 years old
Smoker
Clinical features:
Dry, non-productive cough
Dyspnoea
Clubbing
Inspiratory bibasilar crackles
Investigations
HRCT — honeycombing
Biopsy
Spirometry
Management
Meds
Surgery — transplant
Lung cancer
Lung cancer is initially classified histologically as being either small cell lung cancer (SCLC) or non-small cell lung cancer (NSCLC) due to the different features, management and prognosis see in the two groups.
SCLC accounts for around 15% of cases and generally carries a worse prognosis.
NSCLC can be broken down into
adenocarcinoma
this is now the most common type of lung cancer. The increased in the proportion of lung cancer cases caused by adenocarcinoma is thought to be have been caused by the increased use of low-tar cigarettes
often seen in non-smokers: amongst 'never' smokers adenocarcinoma accounts for 62% of cases compared to 18% caused by squamous cell
squamous
cavitating lesions are more common than other types of lung cancer
large cell
alveolar cell carcinoma
not related to smoking
++sputum
bronchial adenoma
mostly carcinoid
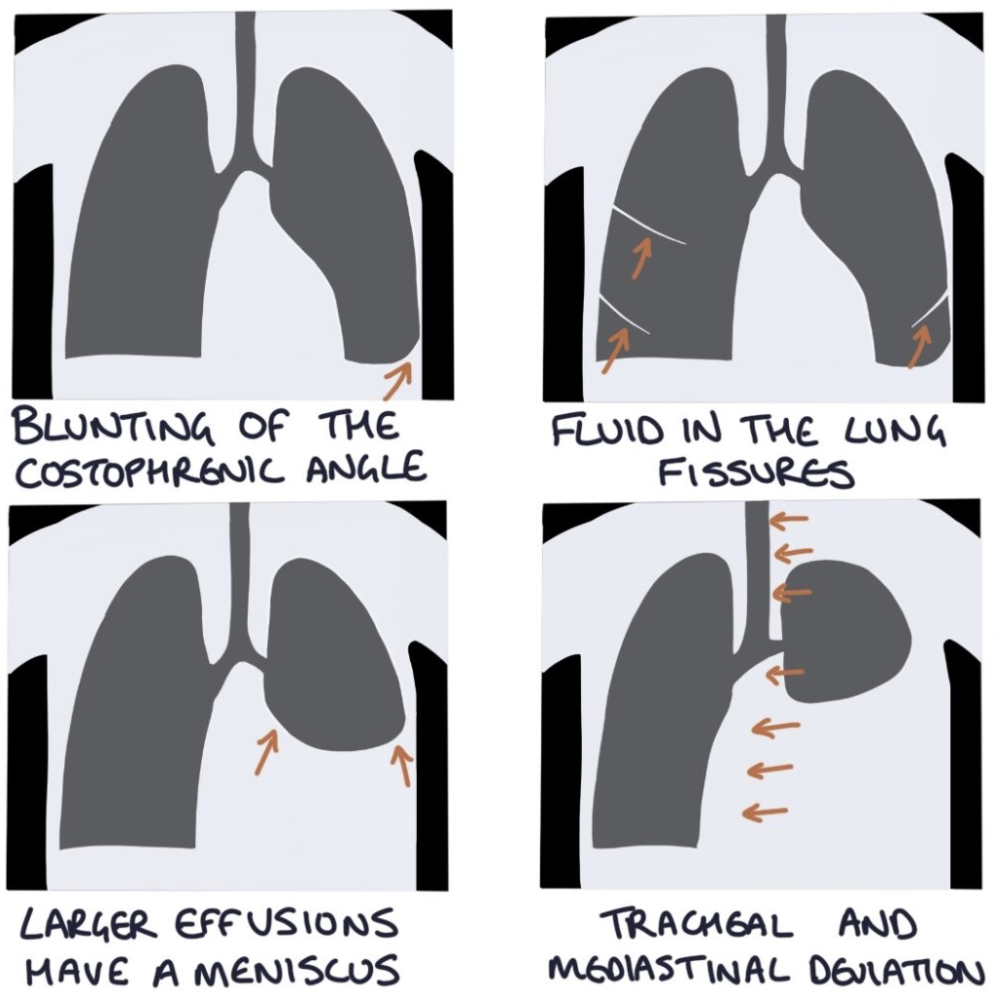
Pleural effusion
Definition - accumulation of fluid in pleural cavity
Exudative > transudative = protein
Causes:
Exudative
Infection e.g. pneumonia
Malignancy
RA
TB
Transudative
Congestive heart failure
Clinical features:
SOB
Dull percussion
Reduced breath sounds
Tracheal deviation
Investigation — CXR
Management
Conservative
Aspiration
Chest drain — non-recurrence
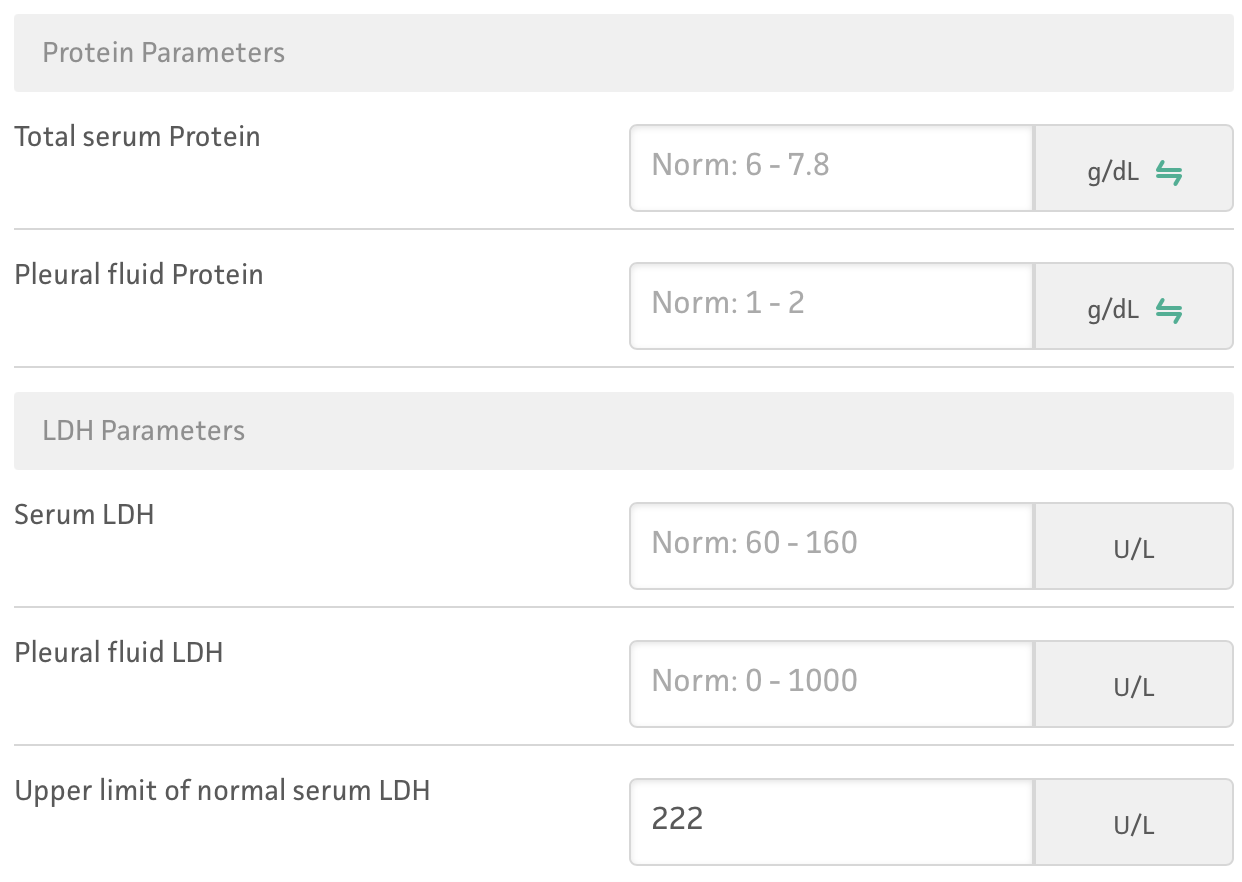
Light’s Criteria establishes exudative effusion
Pleural fluid protein / serum protein greater than 0.5
Pleural fluid LDH / serum LDH greater than 0.6
Pleural fluid LDH greater than 2/3 of the normal upper limit of the serum LDH
Pulmonary embolism (PE)
Definition - blood clot obstructing the pulmonary artery
Cause - DVT
Risk factors:
Immobility/ long haul travel
Recent surgery
Presentation:
Dyspnoea
Pleuritic chest pain
Cough — haemoptysis
PERC Rule to rule out PE
Wells Score used when PE is suspected
Diagnosis
CXR - to rule out other pathologies
Likely PE — CTPA
Unlikely PE — D-dimer —> +ve —> CTPA
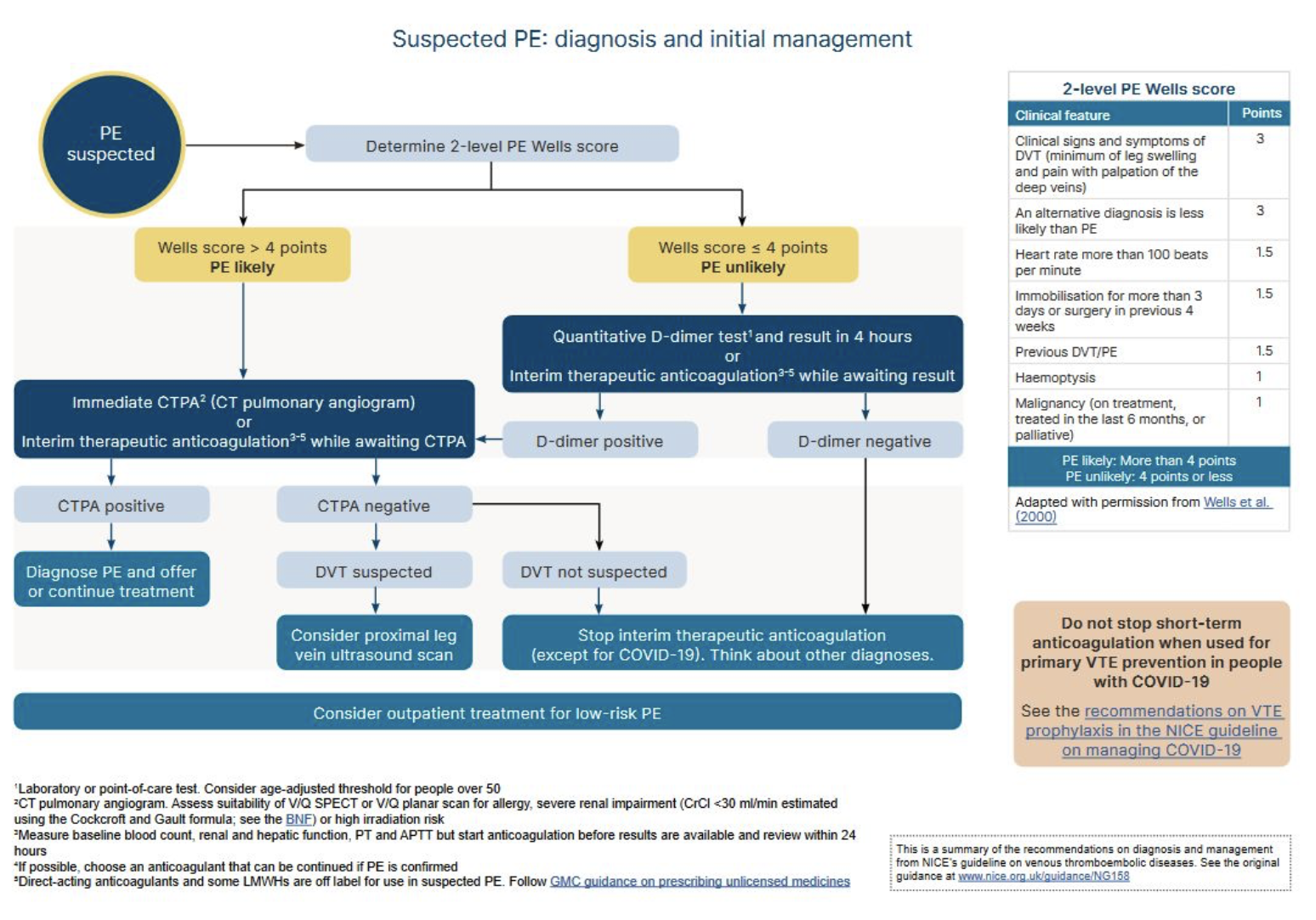
D-dimer is raised in VTE
Management
Supportive — O2, analgesia, hospital admission
Apixaban/rivaroxaban — LMWH
Massive — thrombolysis, unfractioned heparin
Long-term
DOAC - “-ban“
Warfarin (vitamin K antagonist) - antiphospholipid syndrome
LMWH - pregnant
Continue medication for 3 months
Pneumonia
Obstructive sleep apnoea
Examination
Unilateral reduced chest expansion —> collapse/pneumonia
Percussion
Resonant = normal
Dull = consolidation, collapse, effusion (pneumonia/effusion)
Hyper-resonant = pneumothorax
Auscultation
Inspiratory stridor = URTI
Wheeze = asthma / COPD
Coarse = pneumonia / pulmonary oedema
Inspiratory fine crackles = pulmonary fibrosis