Dysphagia Exam 1
Tongue (lingual or glossal)
Function: used to manipulate food, articulate speech sounds, and expectorate (spit out) material from the oral cavity
muscular hydrostat- biological structure found in animals and is used to manipulate items such as food, locomotion. This consists of muscles w/ no skeletal support.
The tongue is a muscular hydrostat.
Muscles of the tongue are divided into two groups: intrinsic and extrinsic
there are four paired for intrinsic and 4 extrinsic
intrinsic: both origin and insertion located within the body of the tongue. Contraction of these muscles causes deformation of body of the tonge
extrinsic: either origin or insertion within the body of the tongue with other point on another structure such as the jaw or palate. Contraction of these muscles reposition the body of the tongue w/in or outside the oral cavity.
Intrinsic muscles include vertical, transverse, superior longitudinal, and inferior longitudinal.
vertical intrinsic muscle: fibers that are aligned vertically. Contraction flattens the tongue.
transverse: fibers align horizontally. Contraction narrows and elongates the tongue.
vertical and transverse lingual muscles are interdigitated (intertwined).
superior longitudinal muscle: fibers are aligned along the length of the tongue. Contraction shortens and pulls tip upward.
inferior longitudinal: fibers aligned length of tongue. Contraction shortens and pulls top downward.
extrinsic muscles of tongue: hyoglossal, genioglossus, palatoglossal, styloglossal
hyoglossal: courses between tongue and hyoid bone. Contraction depresses the tongue.
genioglossus: courses between the tongue, mandible and hyoid bone. Posterior contraction protrudes the tongue, anterior contraction retracts the tongue. Contraction of all fibers causes lingual depression.
palatoglossus: courses between the tongue and soft palate. Contraction retracts and elevates the tongue.
styloglossus: courses between the tongue and the styloid process. Contraction causes elevation and retraction.
styloid process: bone in the skull located near the ear.
Epithelium and covering of tongue
tastebuds (papillae): raised protrusions on the surface of the tongue and contain sensory receptor cells for taste.
mucosa: pink layer of mucus that is soft and moist and is located under tongue
lingual frenulum: fold of mucosa that connects tongue to floor of the mouth.
Sensory innervation: general and special sensation
general innervation: pressure, touch, vibration, temperature (located throughout the body)
special innervation: dedicated organ with special receptors for a particular stimulus type (tongue, ears, eyes, nose).
tongue has both general and special sensation
general anterior two thirds of tongue innervated by CN V and posterior 1 third by CNIX
special: anterior two thirds of tongue innervated by CN VII and posterior 1 third by CN IX
posterior lingual movement/propulsion: the rapid forceful movement of the tongue that propels into the throat or pharynx
Dysphagia: difficulty swallowing which may impact the safety and/or efficiency. Reduction in safety (apiration), efficiency (prolonged mastication, multiple swallows, residue).
Stages of normal swallow: oral, pharyngeal, esophageal
oral phase: bolus moves from oral cavity into the oropharynx; voluntary process.
pharyngeal phase: bolus moves from oropharynx or pharynx into the esophagus; involuntary process.
esophageal phase: bolus moves through the esophagus and into the stomach; involuntary process
Anatomy:
Maxilla: forms the upper jaw and most of the hard palate. Strengthens the oral cavity. 16 permanent teeth (8 on each side), infants only have 10 teeth.
mandible: lower jaw, large horseshoe shaped structure, 16 permanent teeth
temporomandibular joint: the mandible articulates with the left and right temporal bones along the sides of the skull to form the joint. Located under the external auditory meatus. enclosed by fibrous capsule and lubricated by synovial fluid.
hyoid: attachment points for the muscles. Do not articulate with any other in the body. Attached by ligaments to the styloid process.
the hyoid has 2 greater horns, 2 lesser horns, and a body.
Cartilages:
epiglottis: flap in the throat that protects airway from food and liquid
epiglottic petiole: by the base of the epiglottis.
Laryngeal Cartilages: thyroid, cricoid, epiglottis, arytenoid, cuneiform, corniculate
paired: arytenoid, cuneiform, corniculate
unpaired: thyroid, cricoid, epiglottis,
thyroid: lamina, prominence, superior cornu, inferior cornu, oblique line
Soft Tissues: Tongue, velum, aryepiglottic folds, posterior phrayngeal wall
spaces: sulci (oral cavity), anterior sulcus, lateral buccal sulcus, sublingual sulci ( floor of mouth)
pocketing: residue of food especially in lateral buccal sulci
valleculae: area between the base of tongue and epiglottis
pyriform sinus: area just superior to the cricopharyngeus
laryngeal vestibule: opening into the airway above the true vocal folds
glottis: opening between the true vocal folds.
PES/UES: pharyngeal esophogeal sphincter or upper esophageal sphincter
comprised of two muscles: thyropharyngeus and cricopharyngeus.
PES/UES functions include: 1. prevent air from entering esophagus 2. to prevent reflux of esophagus contents into pharynx to guard from aspiration
located behind cricoid cartilage but extends above and below it. It is located at c5-c6.
Cranial Nerves:
CN V- trigeminal: innervates the temporalis, masseter, medial lateral pterygoid, anterior belly of diagatric, mylohyoid, tensor veli palatini
functions of CN V: motor (opens and closes jaw, lateralization of jaw, mastication) sensory (sensation of face, palate, anterior 2/3 of tongue).
Implications of CN V: impaired mastication/bolus preparation, reduced awareness/sensation of anterior spillage, reduced superior hyoid excursion
CN VII: Facial: innervates buccinator, posterior belly of digastric, stylohyoid, submandibular and sublingual glands.
Functions of CN VII: motor (raise eye brows, wrinkle forhead (LMN), smile/pucker, puff cheeks, superior hyoid movement) sensory (taste to anterior 2/3 of tongue)
Implications of CN VII: lateral sulcus residue (pocketing), anterior spillage, reduced salivation, reduced superior hyoid movement.
CN IX: glossopharyngeal: innervates stylopharyngeus and parotid glands.
functions of CN IX: motor (stylopharyngeus contraction) sensory (sensation and taste to posterior 1/3 of tongue, sensation to faucial pillars/palatine tonsils/posterior pharyngeal wall, gag reflex).
Implications of CN IX: impaired taste, reduced salivation, delayed onset of swallow.
CN X: vagus: innervates the larynx (superior laryngeal nerve, recurrent laryngeal nerve) and pharynx
functions of CN X: motor (vocal quality, pitch elevation, cough, palatal elevation, pharyngeal contraction/cricopharyngeal relaxation) sensory (sensation to larynx, pharynx, trachea)
implications of CN X: reduced vocal fold adduction, aspiration, impaired sensation to aspiration, pharyngeal residue, nasopharyngeal regurgitation.
CN XII: Hypoglossal: innervates intrinsic lingual muscles (superior longitudinal, inferior longitudinal, vertical, transverse), extrinsic muscles (genioglossus, hypoglossus, styloglossus, palatoglossus)
innervation for CN XII: motor (lingual movement/symmetry, lingual strength, appearance (atrophy, deviation, fasciculations)) sensory (n.a)
Implications of CN XII: impaired bolus prep/manipulation/control, AP (anterior posterior) transit, oral/lingual residue)
Liquid coming out of the nose, breathing quality, silent aspiration, on MBS indicates which nerve?
Vagus nerve
slow oral and A and P transit, food residue
hypoglossal CN XII
difficulty with mastication, not aware of spillage
trigeminal CN V
dry mouth, pocketing, weakness to one side of face while smiling.
CN VII
reduced taste, dry mouth, delayed onset of pharyngeal swallow
glossopharyngeal CN IX
Palate: soft and hard
hard palate: comprised of 2 paired bones of skull 1. maxillae-forms majority of hard palate(anterior 2/3) 2. palatine- forms posterior 1/3 of palate. Hard palate is covered in mucosa (superficial layer is keratinized or waterproof).
function of hard palate: static immoving structure, allows tongue to apply pressure to it. Speech and swallow roles. sensory function includes providing feedback about tongue position during speech and swallowing and bolus position during swallowing. sensory information for hard palate is carried by the maxillary branch of trigeminal nerve CN V.
Rugae: ridges produced by folding walls of an organ. play a role in bolus positioning in oral cavity.
soft palate: a posterior muscular extension of the hard palate. It is comprised of tensor veli palatini, levator veli palatini, musculus uvulae, palatoglossus, palatopharyngeus.
tongue and velum are both muscular hydrostats
motor innervation of soft palate: motor (tensor veli palatini is innervated by CN V and manibular nerve while all else is innervated by pharyngeal plexus which is CN IX and X) sensory (soft palate innervated by CN V and faucial arches by glossopharyngeus CN IX).
Function of soft palate: dynamic function 1. respiration (location of airflow) 2. resonance (location of sound flow) 3. deglutition (location of bolus flow). CN V-V2 (maxillary nerve) carries sensory information of soft palate to the brain.
Respiration —> Positions of soft palate: up/elevated and posterior: air can be forced through the oral cavity, down/depressed and anterior: during quiet breathing allows for air to flow to oral and nasal cavity
Resonance —> speech sounds /m/ /n/ /ng/ block oral cavity needing depressed velum, all other sounds velum is elevated.
Deglutition —-> location of bolus: velum is depressed before swallow during chewing allowing for nasal breathing and retronasal olfaction. velum is up during swallow to prevent nasal regurgitation or food entering nasal cavity. Helps to build pressure in pharynx to move bolus downward.
velar elevation and retraction occur via contraction of levator veli palatini and musculus uvulae
velar depression and anterior movement occurs via contraction of palatoglossus and palatopharyngeus.
tensor veli palatini- dilates eustachian tube to aerate middle ear. (dilates during swallowing to equalize middle ear pressure).
Pharynx: throat
Spaces:
Pharyngeal cavity: air filled space that includes nasopharynx which is behind the nasal passages, the oropharynx behind the oral cavity, and laryngopharynx which is behind the larynx.
pharynx: includes natural pockets that serve as reservoirs where food and liquid briefly collect.
Functions of pharynx: 1. respiration: open passage allows for gas exchange between the lungs and oral or nasal passage. 2. digestion: food and liquid need to move throughout the pharynx to reach the esophagus and stomach
pharyngeal spaces: connect nose and mouth to the air way and food way.
pharyngeal muscles: paired
constrictors: “c” shaped walls: posterior right lateral and left lateral open anteriorly, horizontally aligned fibers (creates smaller diameter of oropharynx and laryngopharynx). The constrictors are superior, middle, and inferior.
Function of constrictors: constrict from top to bottom to aid in sequentially moving bolus downward to the esophagus. Aid in bolus efficiency.
Location/attachments: arise from the posterior midline part of the pharynx and coarse anetriorly toward the structure to which they attach. superior: attaches to buccinators bilaterally via pterygomandibular raphae. Middle: coarse anteriorly and attach to the greater horn of the hyoid bone bilaterally. Inferior: coarse anteriorly and attach to oblique line of the thyroid cartilage.
Other muscles:
longitudinal pharyngeal muscles: long narrow muscles that run vertically form structures above the pharynx and through the pharynx.
function: hyolaryngeal elevation via pharyngeal shortening (airway protection)
sapingopharyngeus, palatopahryngeus, stylopharyngeus (shorten pharynx): when they contract they elevate and shorten the pharynx. they are interdigitated (attached to) the pharyngeal constrictors, they aid in elevation of the constrictors.
contraction of the constrictors and longitudinal muscles to shorten and constrict the pharynx.
pharyngeal constrictors help with epiglottic inversion and thus airway protection.
Innervation of pharyngeal muscles: motor (all muscles except the stylopharyngeus are innervated by the pharyngeal plexus (CN X and CN IX). The stylopharyngeus is innervated by the glossopharyngeal nerve CN IX. Sensory (nasopharynx-glossopharyngeal CN IX, oropharynx and laryngopharynx by Pharyngeal plexus.
Normal Swallow Stages
oral stage: lip closure, tongue control, bolus preparation/mastication, bolus transport/lingual motion/anterior-posterior AP transit.
Muscles of the oral stage:
temporalis: CN V
Masseter: CN V
Buccinator: CN V
pterygoid: CN V
What are the main goals of swallowing?
bolus efficiency: moving ingested bolus into the esophagus in timely manner without significant residue, effort, or repeated swallows.
airway protection: preventing ingested material from entering the larynx or trachea.
when is the swallow triggered?
MBS: initial hyoid burst
FEES: arytenoid cartilage approximation
EVENTS:
Posterior Lingual Propulsion: quick forceful lingual movement that propels a bolus posteriorly into the pharynx.
BE: primary driving propulsive force for bolus transit during swallowing. The bolus is pushed against the hard palate via midline of the tongue while also contained by mid tongue.
AP: epiglottic inversion: base of tongue retracts and helps move the epiglottis into a horizontal position.
Swallow Trigger BE and AP: triggered by sensory stimulation to oropharyngeal region.
Velar Elevation BE: velum elevates in posterior direction, making contact with posterior pharyngeal wall. swallow triggers any time in pharynx. younger = earlier older= later
Laryngeal Vestibule Closure BE AP: first line of airway defense during swallowing.
hyolaryngeal excursions: hyoid bone and larynx move up and forward. position of epiglottis is higher and closer to the tongue.
arytenoid adduction and forward movement AP: during swallow arytenoids adduct and pivot anteriorly toward the base of the epiglottis. This prevents penetration from posterior commissure (posterior space between the vocal folds). If penetration occurs (enters the laryngeal vestibule) adduction and forward pivoting help prevent aspiration.
aryepiglottic bunching AP: prevents aspiration as bolus travels down laterally on either side of the larynx. Occurs via aryepiglottic muscle and indirectly via passive epiglottic inversion driven by other structures.
epiglottic inversion AP: via base of tongue, passive movement of epiglottis by another structure (the tongue). pharyngeal movement: helps move broader, free end of the epiglottis into inverted position near the arytenoids.
Laryngeal Elevation BE: UES traction/stretching. Clearing force behind tail of bolus traveling down pharynx. Occurs via sequential contraction of superior, middle, then inferior constrictors (pharyngeal stripping wave) about 400msec and via the longitudinal pharyngeal muscles shorten length of the pharynx.
Upper Esophageal Sphincter: opens to allow the bolus to move from pharynx to the esophagus via relaxation of the sphincter muscles. Relaxation occurs via inhibition of the pharyngeal plexus and some branches of ansa cervicalis of cervical plexus (spinal nerves).
UES further opened by laryngeal excursion.
BE allow bolus passage to esophagus
AP indirectly protects the airway

GERD: gastroesophageal reflux is backflow of gastric contents from the stomach into the esophagus. severe or frequent and it becomes GER-D
10-48% of americans which is about 60 million people
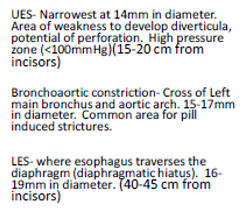
Esophagus: tube like structure, collapsed at rest, portion of upper digestive tract, conducts food from pharynx to stomach (peristalsis), 25cm or 10inch length 1inch or 2.5cm in diameter C5-C6.
The esophagus is divided into three parts: cervical (proximal), thoracic(mid-distal), and abdominal (distal).
cervical: left of midline behind trachea, cricoid cartilage to thoracic inlet, made up of striated muscle.
thoracic: thoracic inlet to diaphragm, mix of smooth and striated
abdominal: LES, at or just below the diaphragmatic hiatus, made of smooth muscle
UES: proximal 1/3 striated muscle, transition zone straited and smooth, distal 2/3 smooth muscle
how many laryngeal cartilages are there?
6
what cranial nerve is involved during the esophageal phase
cranial nerve x or 10 or vagus
penetration occurs when the food/liquid/secretions enter what area?
laryngeal vestibule
in a healthy swallow the ___ makes a posterior inferior fold to make contact with the arytenoid cartilages?
epiglottis
a client has food or liquid caught in the vallecula, is this cause for concern and have they aspirated? if not, at what point would it be considered aspiration?
not yet a concern, they have NOT aspirated. Below the vocal folds is considered aspiration.


At what level is the UES located?
C5-C6

true
during normal swallow, which is the only stage not to involve airway protection?
velar elevation
what are the three functions of the pharynx?
constriction, elevation, shortening
Name two functions of saliva?
breaks down food, maintains pH, starts digestion process, prevents tooth decay
what are the two muscular hydrostats?
tongue and soft palate
CN ____ might be affected if you see silent aspiration on a MBS
10
all muscles of the pharynx EXCEPT ____ muscle are motorically innervated by the pharyngeal plexus?
stylopharyngeus