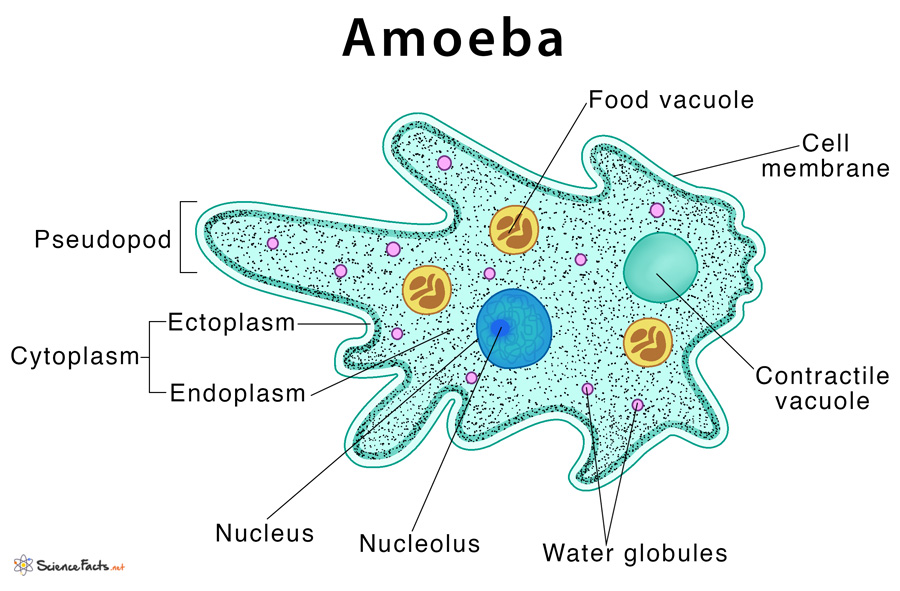
Amoeba - Lobosea
SUBPHYLUM SARCODINA
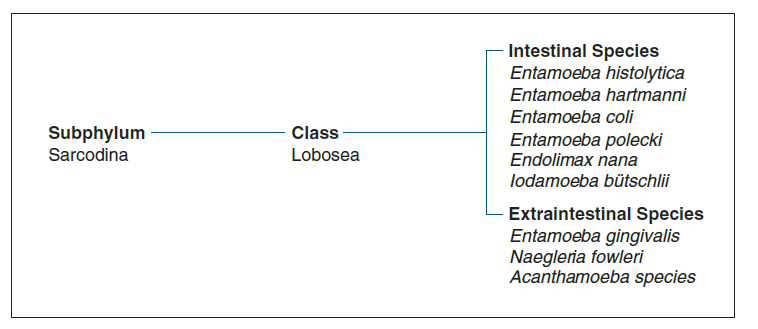
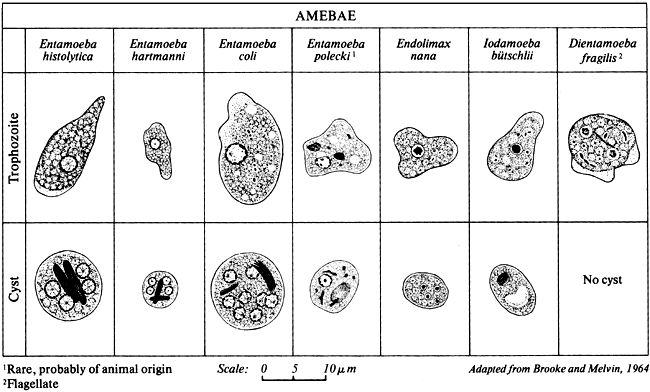
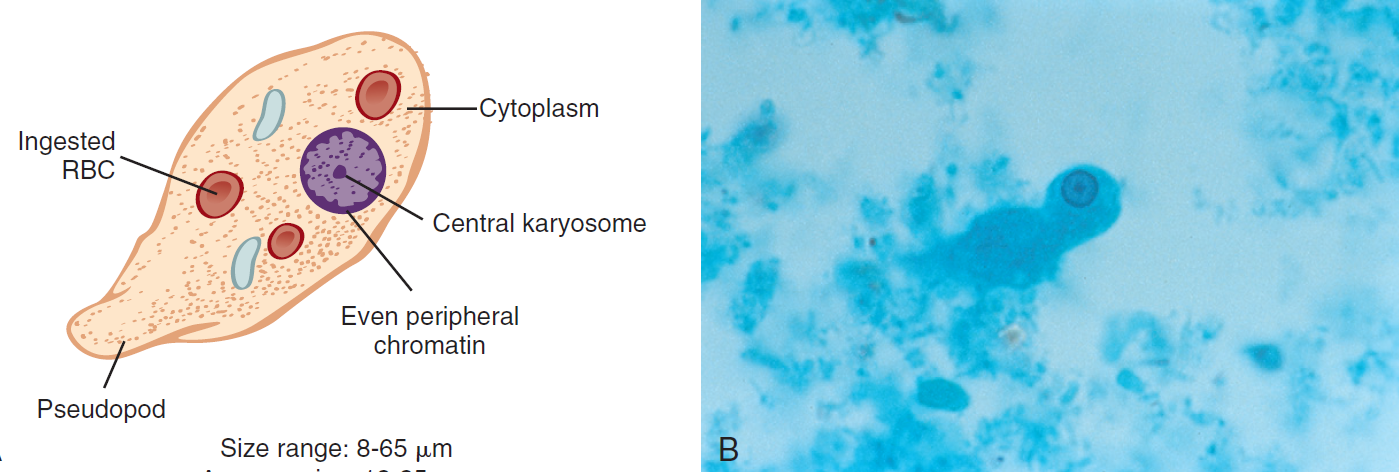
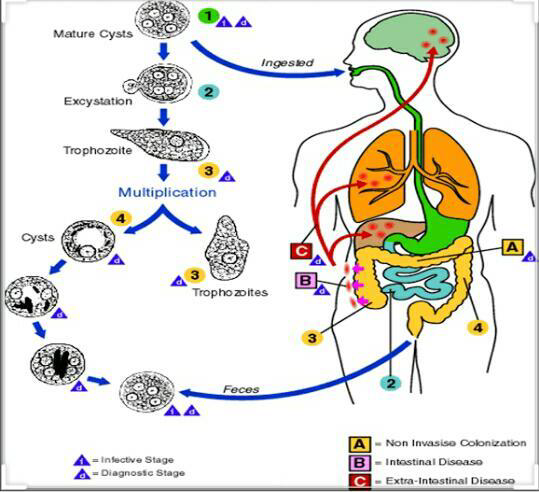
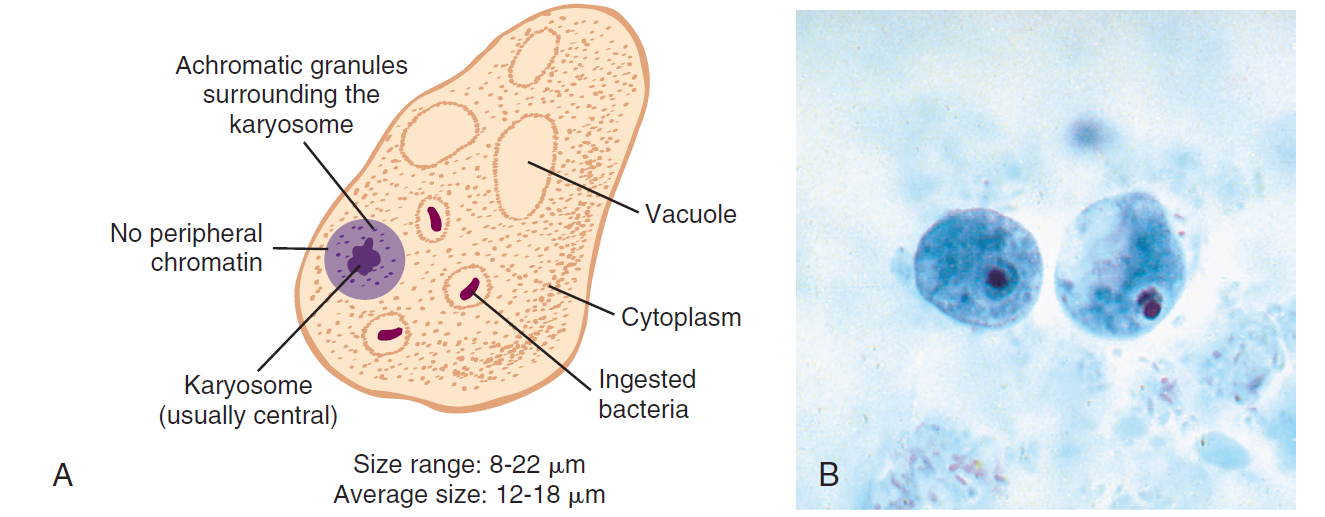
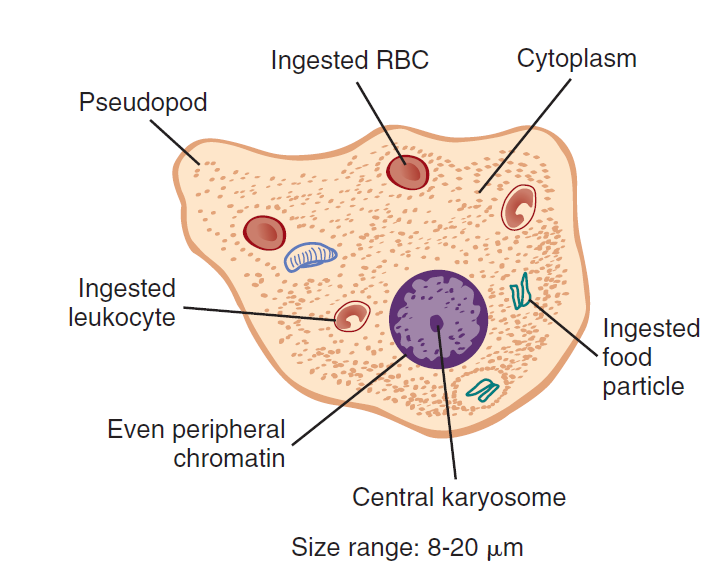
Entamoeba histolytica
Direct life cycle
multiplies by binary fission
associated diseases:
Intestinal amebiasis
amebic colitis
amebic dysentery
EXTRAINTESTINAL AMEBIASIS
“lyse” tissue destruction
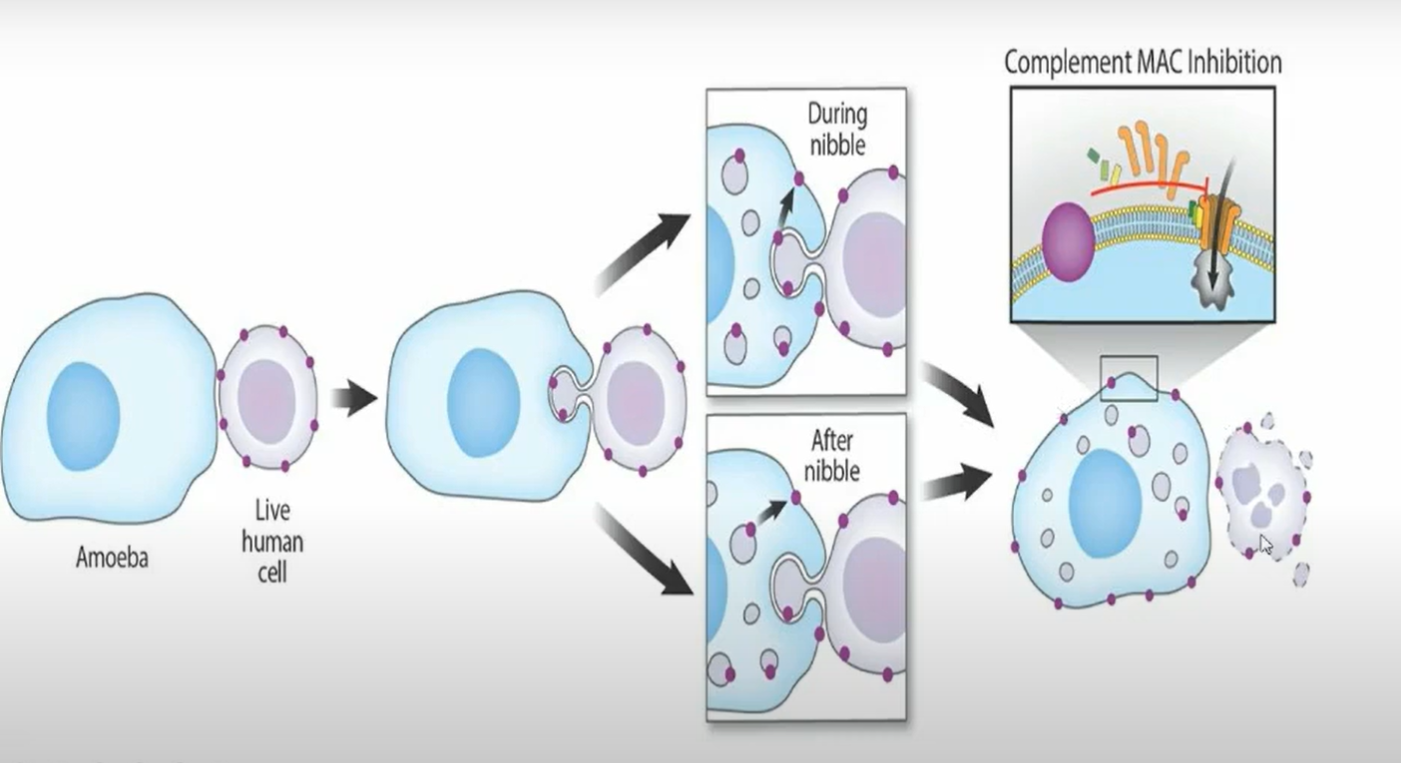
IS
CYST
MOT
ingestion of food/water with cyst
Phoretic Vectors
cockroach and flies
Location
Large intestines
MORPHOLOGY
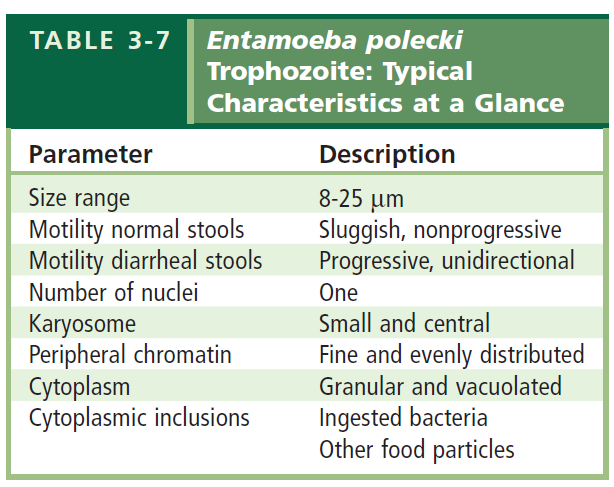
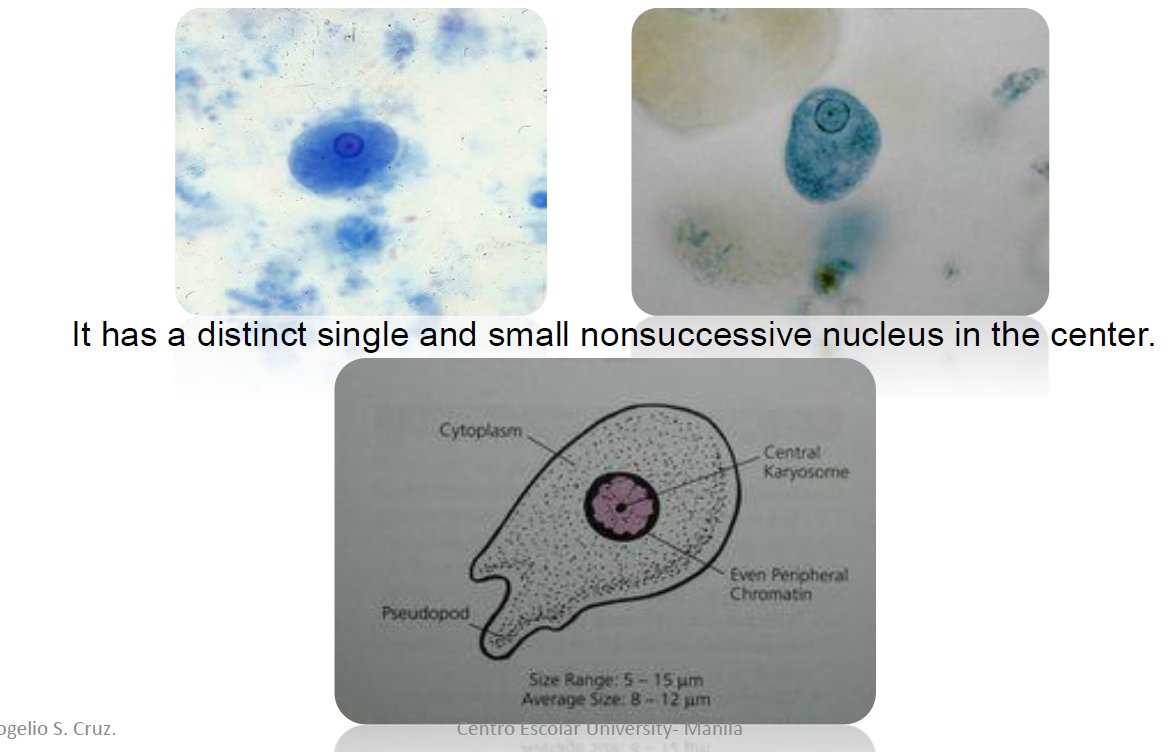
TROPHOZOITES
8-65 microns (12-25 microns)
Motility:
progressive
finger-like pseudopods
Nuclei:
one
Karyosome:
small and central
Peripheral chromatin:
fine and evenly distributed
Cytoplasm:
finely granular
Cytoplasmic inclusion
ingested RBCs
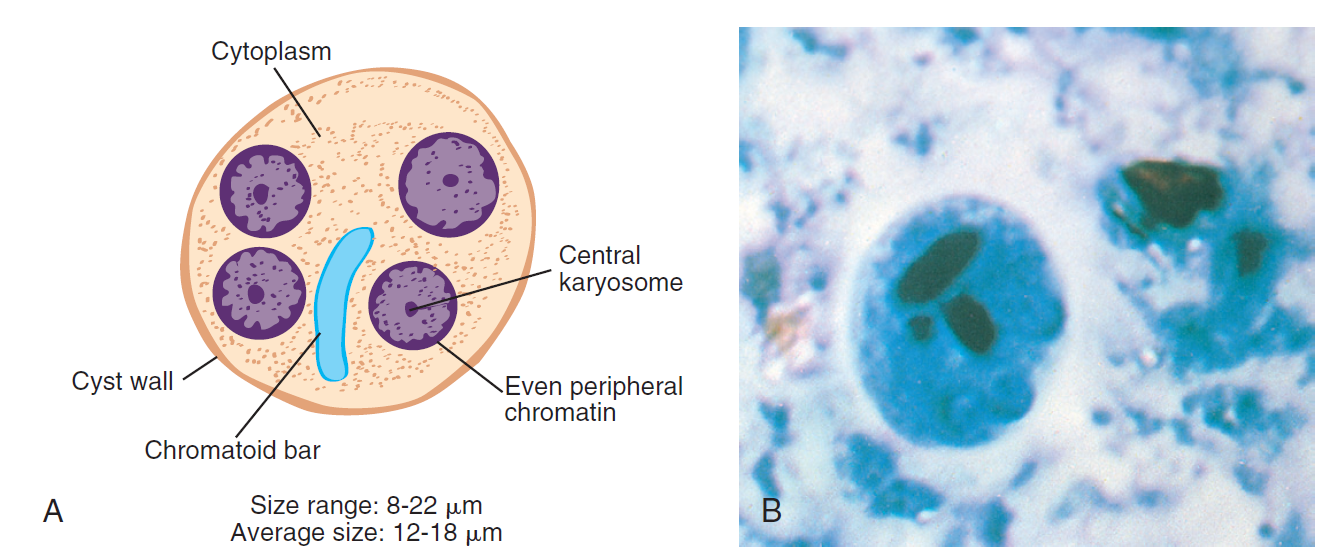
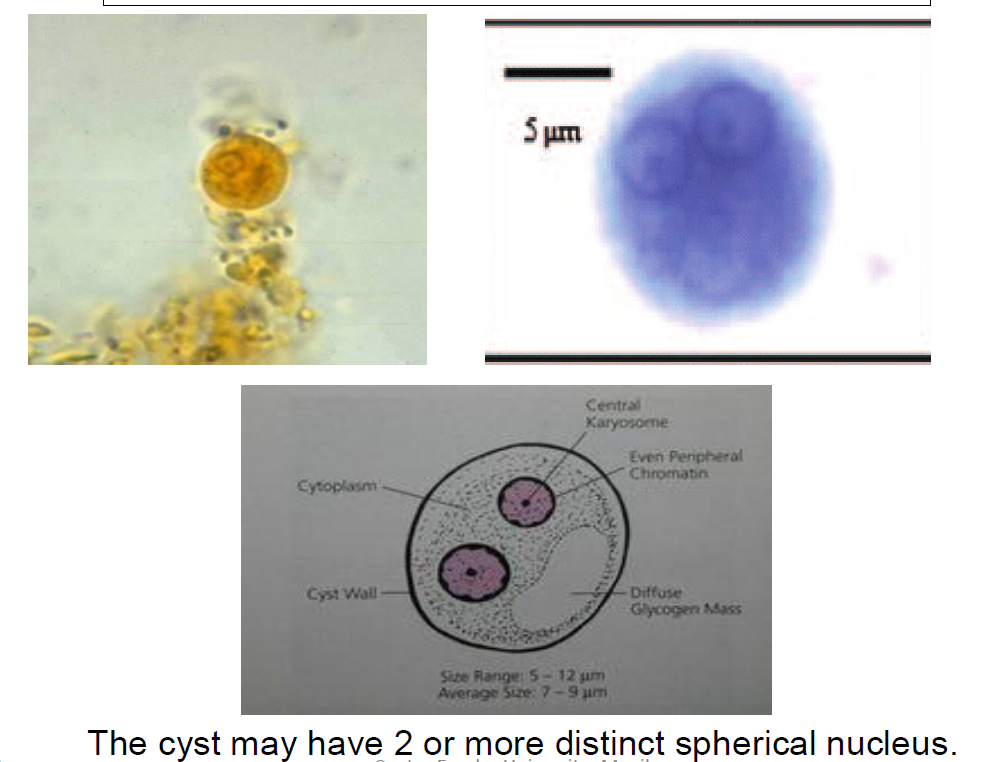
CYST
8-22 microns (12-18 microns)
smaller than trophs
Shape:
spherical to round
Nuclei:
one to four
Karyosome:
small and central
Peripheral chromatin:
fine and evenly distributed
Cytoplasm:
finely granular
Cytoplasmic inclusion
Chromatoid bars, rounded ends in young cysts
Diffuse glycogen mass in young cysts
Laboratory diagnosis
Standard and alternative methods
ELISA (Enzyme-linked immunosorbent assay)
IHA (indirect hemagglutination)
GDP (gel diffusion precipitin)
IIF (indirect immunofluorescence)
Life Cycle
survival in a feces contaminated environment for up to 1 month is common
Epidemiology
infection is as many as 10% of the world’s population
considered a leading cause of parasitic deaths after malaria
Clinical Symptoms
only known as pathogenic intestinal amoeba
Asymptomatic
Symptomatic
Treatment
Paramomycin
Diloxanide furoate (Furamide)
Metronidazoles (Flagyl)
Prevention and Control
Improved sanitation
help reduce the likelihood of transmission
Entamoeba hartmanni
MORPHOLOGY
TROPHOZOITES
5-18 microns
Motility:
non-progressive
finger-like pseudopods
Nuclei:
one
Karyosome:
small and central
Peripheral chromatin:
fine and evenly distributed
Cytoplasm:
finely granular
Cytoplasmic inclusion
ingested bacteria may be present
CYST
5-12 microns
smaller than trophs
Shape:
spherical
Nuclei:
one to four
Karyosome:
small and central
Peripheral chromatin:
fine and evenly distributed
Cytoplasm:
finely granular
Cytoplasmic inclusion
Chromatoid bars, rounded ends in young cysts
Diffuse glycogen mass in young cysts
Laboratory Diagnosis
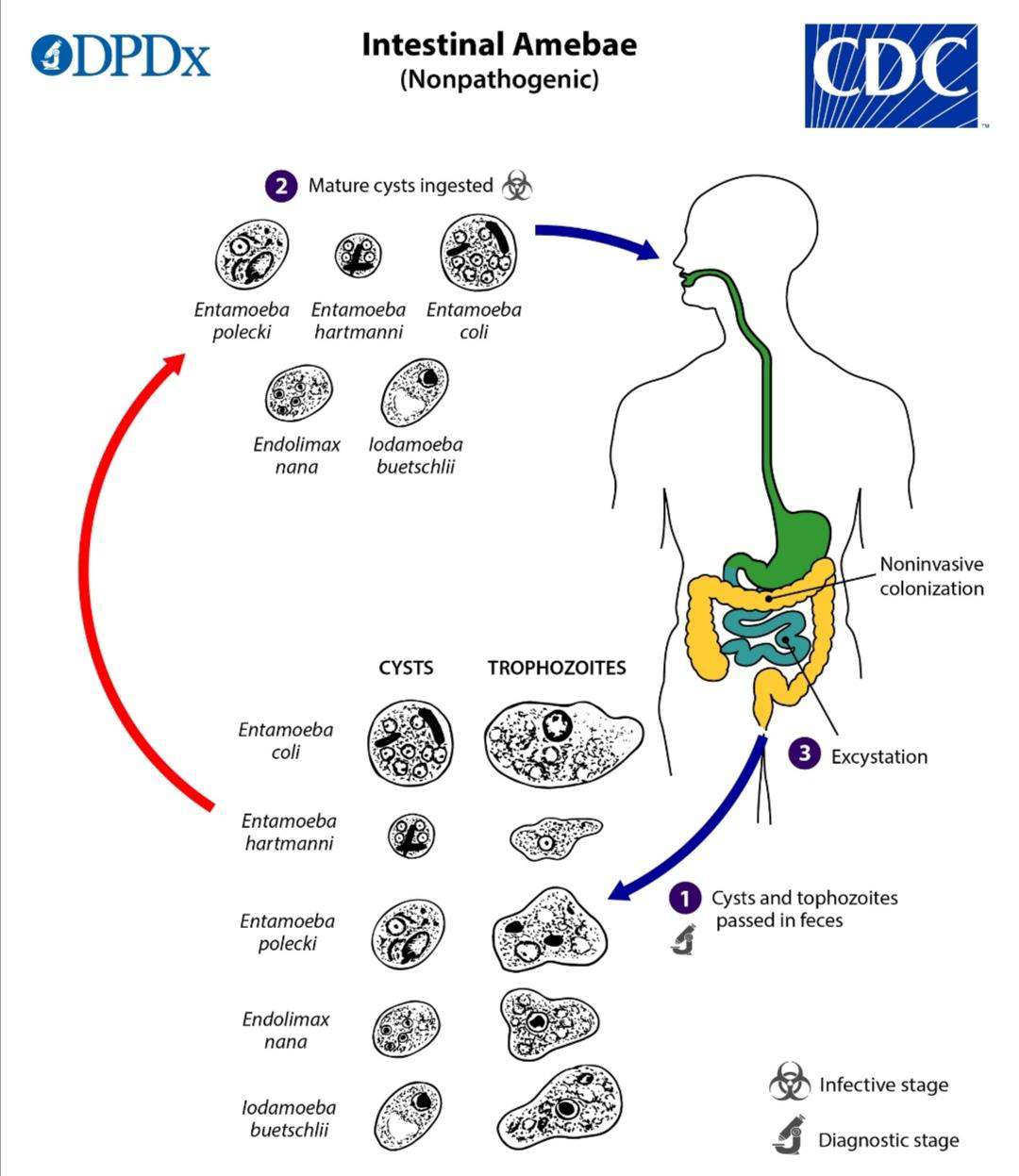
NONPATHOGENIC
examining the stool
advisable to not base solely on the sizes of the amoeba as it may mislead results
ingestion of infected cysts
ASYMPTOMATIC
Prevention and Control
Good sanitation and good hygiene practices
Protection of food and water from vectors like flies and cockroaches
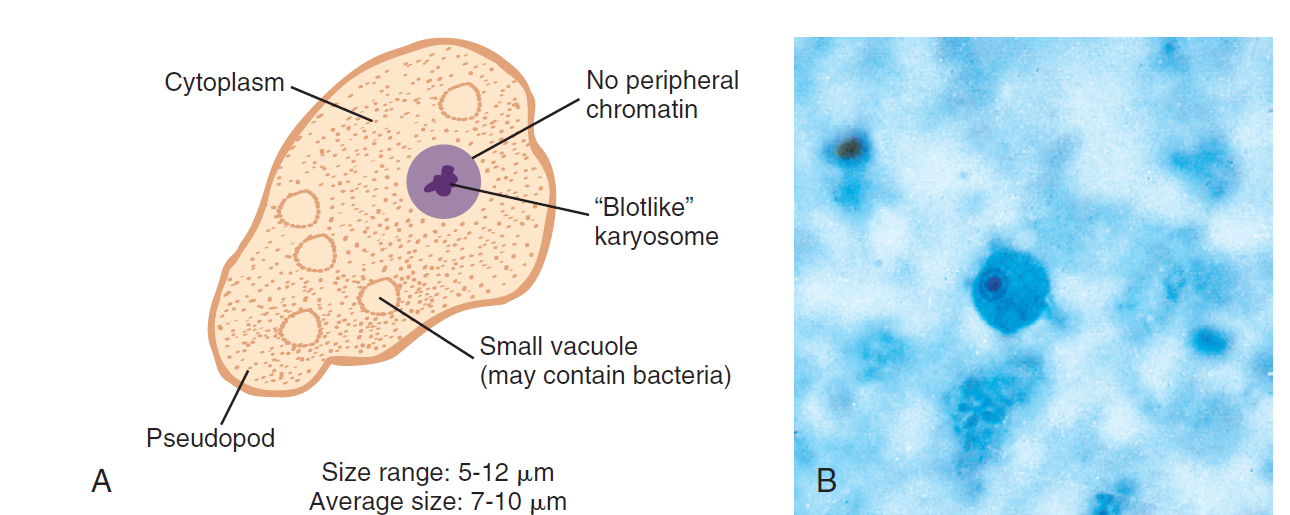
Endolimax nana
NONPATHOGEN
most common of the smaller intestinal amebae
usually encountered with about the same frequency as in E. coli
colonizes the colon
MOT
Fecal-oral via cyst
MORPHOLOGY
TROPHOZOITES
5-12 microns
Motility:
sluggish/slowly
nonprogressive
blunt pseudopods
feeds bacteria and food debris
Nuclei:
one
Karyosome:
large, irregular, blotlike
Cytoplasm:
granular
vacuolated
Cytoplasmic inclusion
bacteria
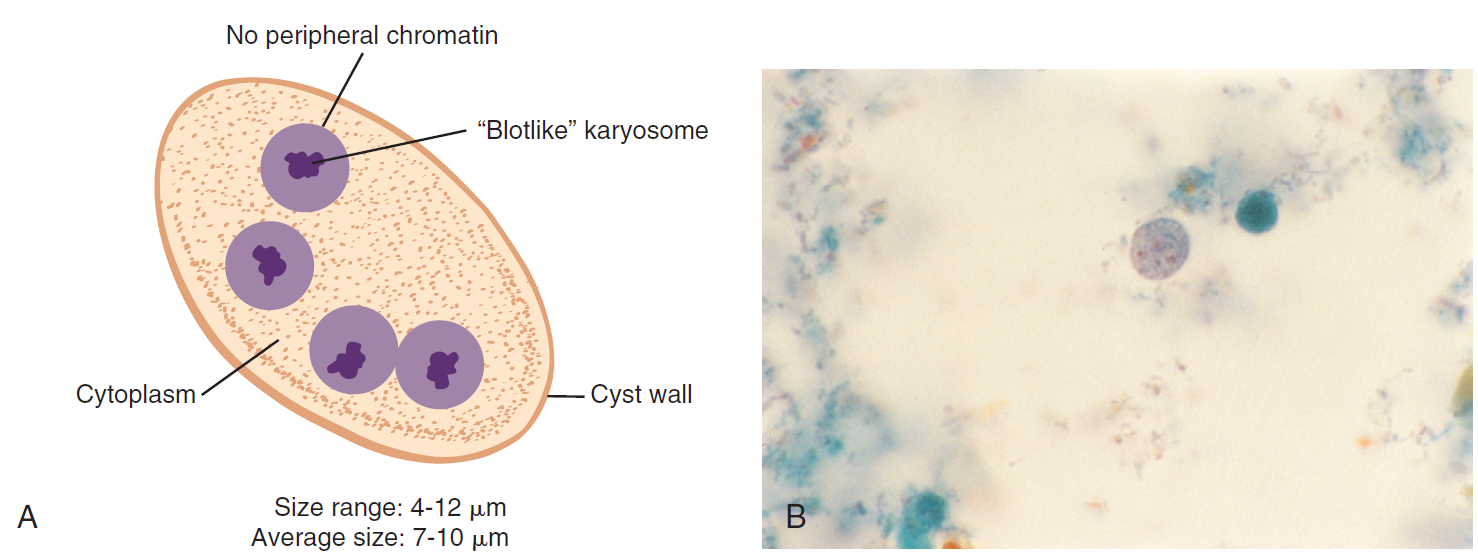
CYST
forms as feces dehydrates
7-10 microns (4-12 microns)
smaller than trophs
Shape:
spherical, ovoid, ellipsoid
Nuclei:
one to four (most common)
with large endosomes
Karyosome:
large
blotlike
usually central
Cytoplasm:
granular
vacuolated
Cytoplasmic inclusion
Chromatin granules
Nondescript small mass
Diffuse glycogen mass in young cysts
Life Cycle
Intestine
organisms passed in feces
Epidemiology
are with poor hygiene
substandard sanitary conditions exist
Clinical Symptoms
Asymptomatic
Prevention and Control
improved hygiene
disposal of fecal waste
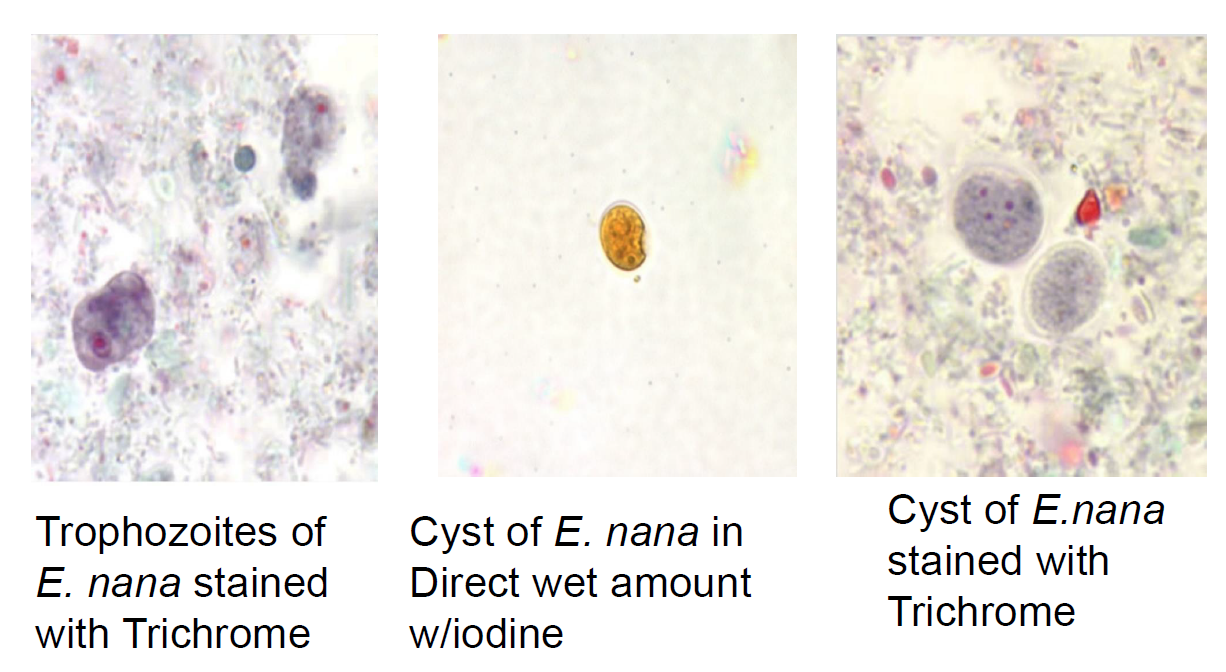
Laboratory Diagnosis
examination
concentration, permanent stained smear
Iodamoeba butschlii
MORPHOLOGY
TROPHOZOITES
8-12 microns
Motility:
sluggish/slowly
usually progressive
Nuclei:
one
Karyosome:
large
usually central refractive achromatic granules may be present
Cytoplasm:
coarsely granular
vacuolated
Cytoplasmic inclusion
bacteria
yeast cells, other debris
CYST
5-22 microns
Shape:
ovoid, ellisoid, triangular, other shapes
Nuclei:
one
Karyosome:
large
eccentric achromatic granules
on one side present
Cytoplasm:
coarsely granular
vacuolated
Cytoplasmic inclusion
well defined glycogen mass may be present
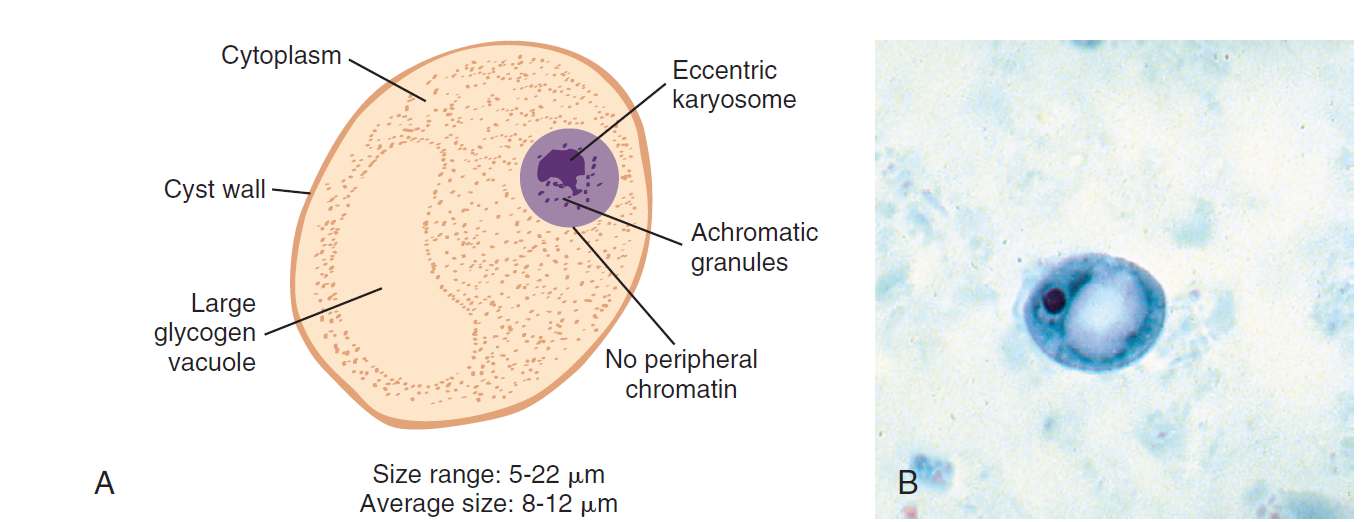
Laboratory diagnosis
Iodine wet preps
glycogen picks up the iodine stain
remain unstained following trichrome staining
aids on identification
Epidemiology
found worldwide and has higher prevalance in tropical regions
Entamoeba gingivalis
MOT
mouth-to-mouth (kissing)
droplet contamination (contaminated drinking utensil)
MORPHOLOGY
TROPHOZOITES
resemblance to E. histolytica
8-12 microns
Motility:
active
varying pseudopods appearance
Nuclei:
one
Karyosome:
centrally located
Peripheral chromatin:
fine and evenly distributed
Cytoplasm:
finely granular
Cytoplasmic inclusion
leukocytes
epithelial cells
bacteria
CYST
UNKNOWN stage
Life Cycle
lives around the gum line of the teeth in the tartar and gingival pockets of unhealthy mouths
trophozoites inhabit tonsillar cryps and bronchial mucus
like E. histolytica— can be found in the sputum and pulmonary abscess
multiplied by binary fission
not survive following contact with stomach juices
also recovered in vaginal and cervical specimen from women using IUD
spontaneous disappearance following removal of IUD
Clinicala symptoms
no symptoms
recovered in patients suffering from pyorrhea alveolaris
thrives under disease conditions but do not produce symptoms
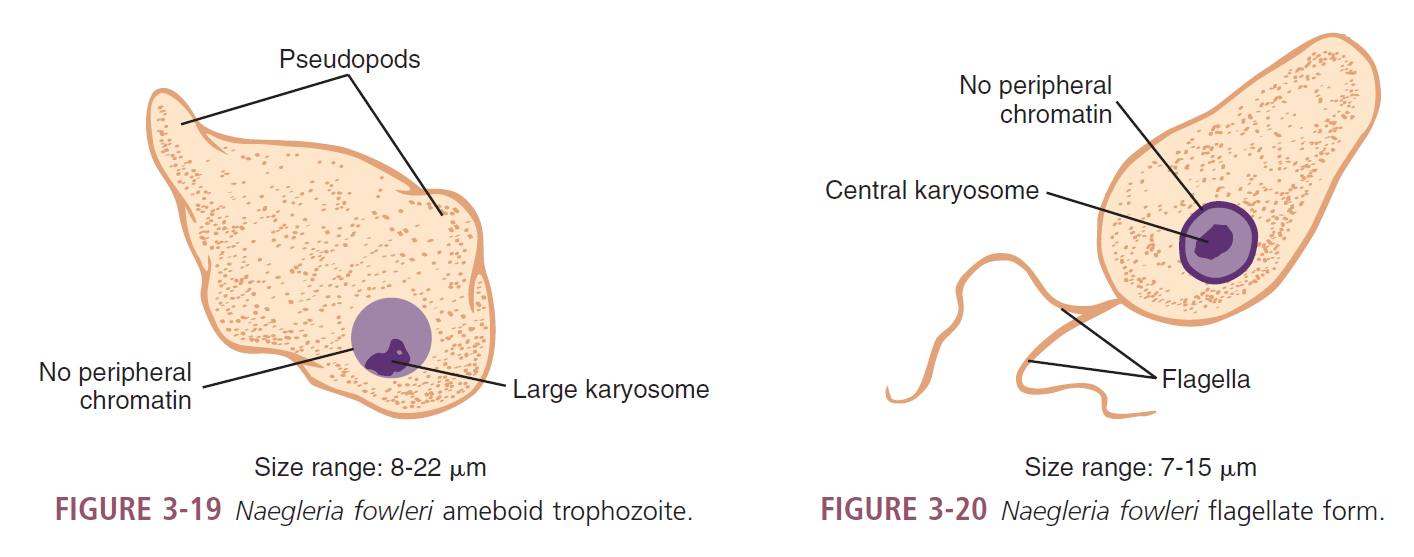
Naegleria fowleri
Causative agent of Primary Amoebic Meningoencephalitis (PAM)
Thermophilic organisms (up to 30°C)
Multiplies through promitosis
intracellular mitosis
nuclear membrane doesn’t break down
three known morphologic forms
ameboid trophozoite
flagellate (protozoa) forms
cysts
N. australiensis
pathogenic in mice
may infect humans
MOT
Oral and Intranasal
while swimming in contaminated lakes, pools, and rivers
often migrate in the brain
inhaling dust infected by N. fowleri
Diagnosis
Cerebrospinal Fluid (CSF)
spinal tap
Culture
non-nutrient medium with Page’s saline seeded with living Escherichia coli
PCR
ELISA
MORPHOLOGIC FORMS
CYST
9-12 microns
thick cell walls
uninucleated w/ rounded chromatoidal bars
TROPHOZOITE
FLAGELLATE
7-15 microns
flagella
whiplike structures; locomotion
2 at broad end
Motility
spinning or jerky
directional
does not divide
AMOEBOID
8-22 microns
only form recognized in humans
single pseudopod
Nucleus
one
karyosome
large central
without peripheral nuclear chromatin
broad anterior end; posterior end is tapered
motility
sluggish
done by blunt pseudopodia
cytoplasm
granular
often contains vacuoles
Epidemiology
found in warm bodies of water
contaminated dust
Primary Amebic Meningoencephalitis
ameboid trophozoites invade the brain causing rapid tissue destruction
symptoms
fever, headache, sore throat, nausea, and vomiting
stiff neck and seizures
smell and taste alterations and blocked nose
Kernig’s sign
diagnostic sign for meningitis
patient is unable to stretch his/her legs because of hamstring stiffness
Postmortem brain tissue samples has the typical ameboid trophozoites
Treatment
always result to death unless detected and treated early
PROMPT Amphotericin B in combination with rifampin or miconazole
damages the cell wall of Naegleria
Prevention and Control
posting off-limits sign on contaminated water sources
educating community
Chlorinate swimming pools and hot tubs
immediately repairing of possible sources of contamination like cracks
Life Cycle
replication
simple binary fission
ameboid trophozoites → flagellate trophozoites (after being transferred to water from a tissue culture)
flagellate trophozoites do not divide but lose flagella and convert back to ameboid
cyst
only exist in external environment
external environment
amebic trophozoites → cysts and flagellates → amebic trophozoites
human contact
swimming in contaminated water
enters through
nasal mucosa and often migrate to the brain
causing rapid tissue destruction
inhaling infected dust
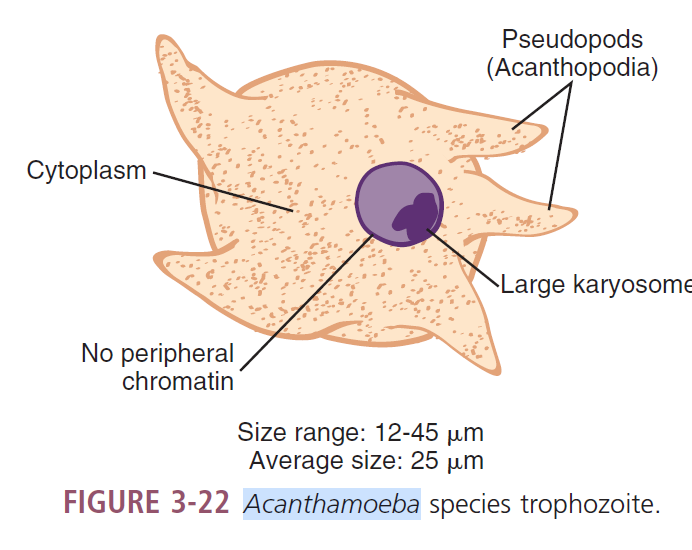
Acanthamoeba spp.
most common
A. castellani
MORPHOLOGY
TROPHOZOITES
12-45 microns (25 microns)
Motility
sluggish
spine-like pseudopods
acanthopodia
Nucleus
one
Karyosome
large
Cytoplasm
granular and vacuolated
CYST
8-25 microns
round-shaped
double cell wall
Cytoplasm
disorganized
granular
Laboratory Diagnosis
Cerebrospinal Fluid (CSF)
Brain tissue
Corneal scrapings
infections of the eye
may be cultured on non-nutrient agar plates with gram-negative bacteria (E. coli)
bacteria as the source of food
produce a set of marks (tracks) on the agar
histologic examination
calcoflour whits
primarily used for fungi;
stain
Indirect immunofluorescent antibody staining
Life Cycle
humans may acquire in one of two ways
Aspiration or nasal inhalation
Trophozoites enter via lower respiratory tract or through ilcers in the mucosa or skin
Hematogenous spread
through the bloodstream & invade CNS (serious CNS infections)
Direct invasion of the parasite in the eye
2 groups are at risk:
contact lens wearers
Acanthamoeba keratitis
trauma to the cornea
contaminated saline
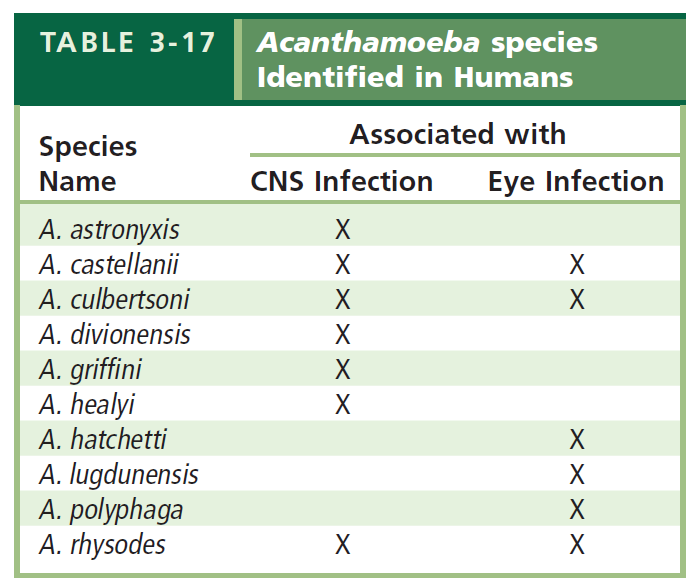
Granulomatous Amebic Encephalitis (GAE)
Location
lungs
hematogenous spread to the brain
CNS Infection
Symptoms
headaches, seizures, stiff neck, nausea, vomiting
Granulomatous lesions
in the brain
may contain both Acanthamoeba trophozoites and cysts
other areas of the body
kidneys
pancrea
prostate
uterus
Acanthamoeba keratitis
infections of the cornea of the eye
Symptoms
severe ocular pain
vision problems
Infected tissue
may contain trophozoites and cysts
perforation of the cornea may result
subsequent loss of vision
Treatment
begin treatment immediately
itraconazole
ketoconazole
miconazole
propamidine isethianate
rifampin
Prevention and Control
avoid using homemade non-sterile saline solutions for contact lens
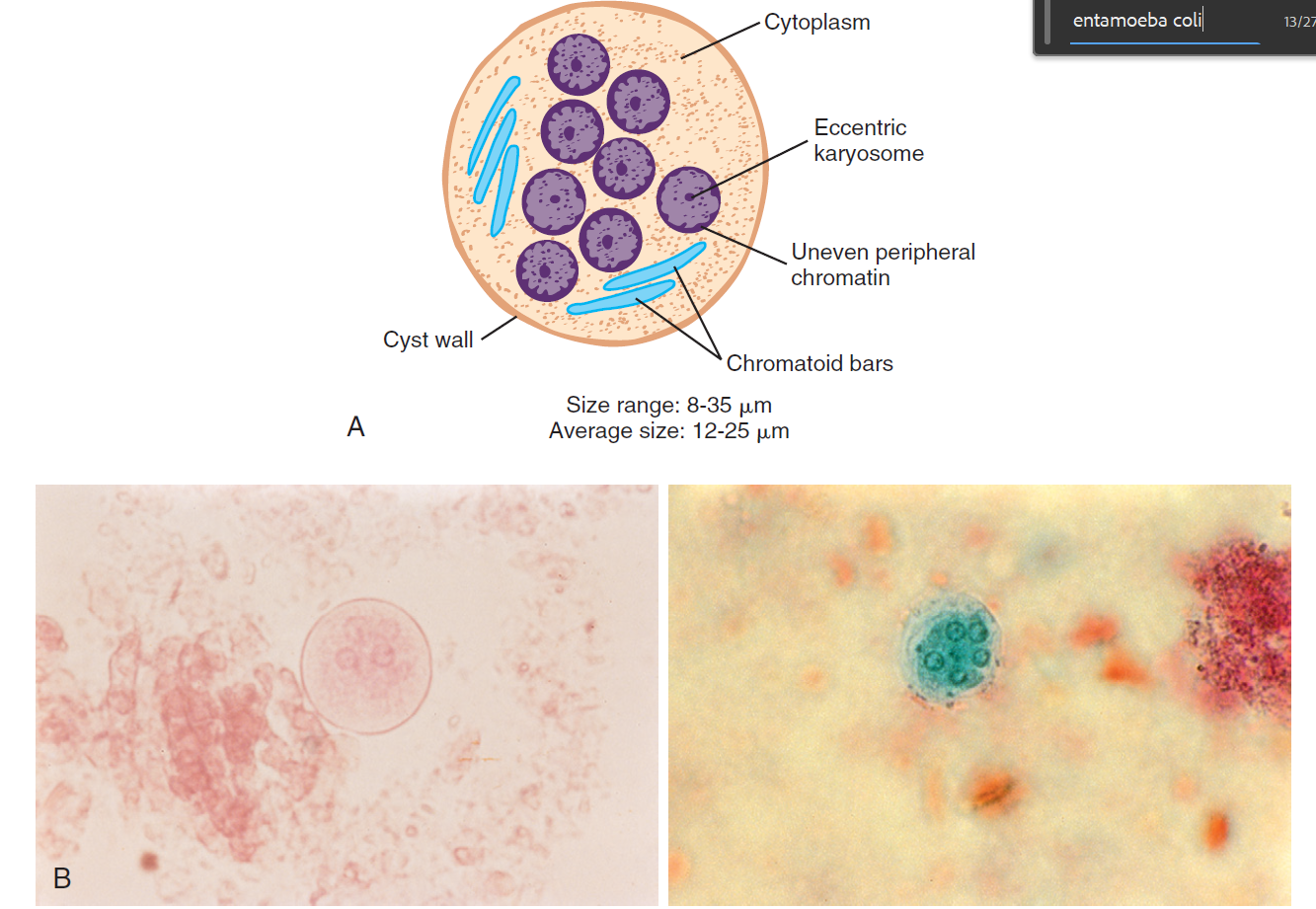
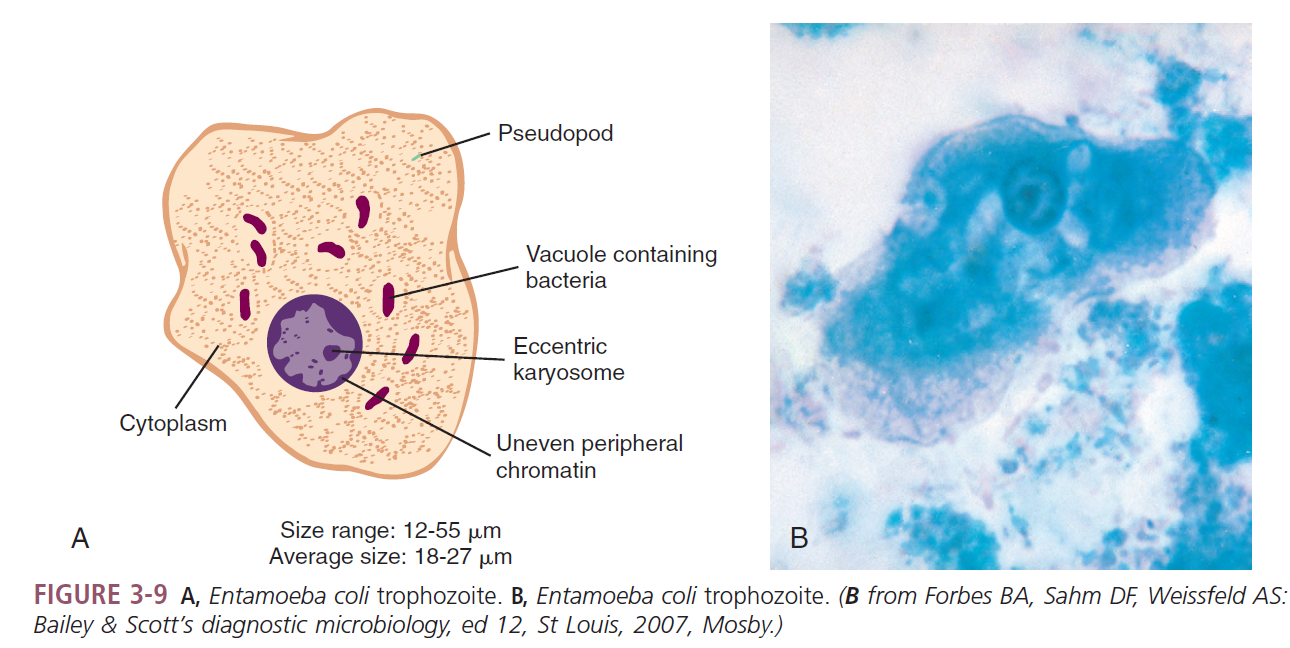
Entamoeba coli
MORPHOLOGY
CYST
10-35 microns (usually, 15-25 microns)
splinter-like chromatoidal bars
mature cyst with 8 nuclei
Peripheral chromatin
coarsely granular, may be clumped and unevenly arranged
Karyosome
large, may or may not be compact and/or eccentric
Glycogen
diffuse, may be absent in mature cysts
TROPHOZOITE
15-50 microns (20-25 microns)
moves in several directions at the same time
sends out several pseudopods at the same time
pseudopods trusted out slowly
Endoplasm
contain bacteria, yeasts, and cell detritus
stained nucleus contains a thicker nuclear membrane with layer of variously sized chromatin granules unevenly distributed along the inside border of nuclear membrane
Karyosome:
large, eccentrically located
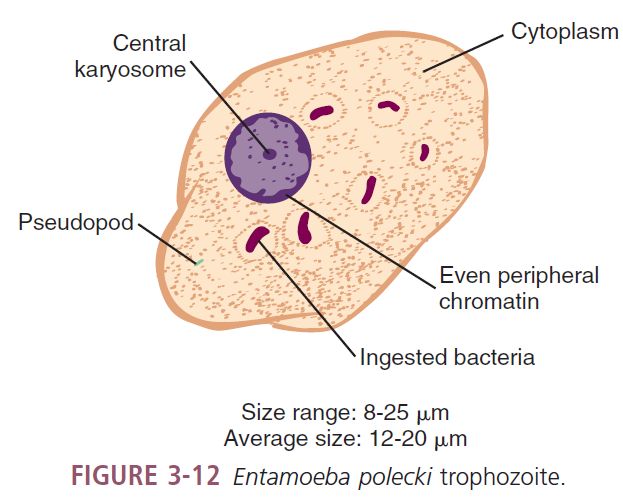
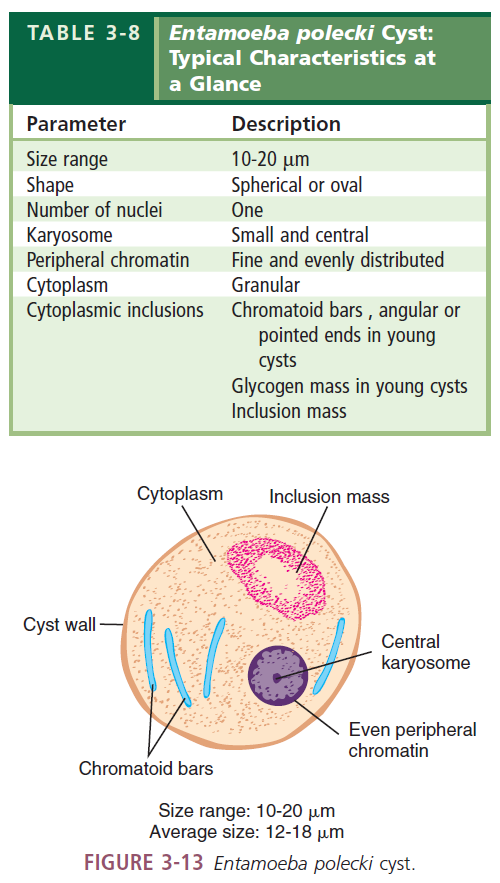
Entamoeba polecki