HIV
1. HIV Transmission and Prevention
Primary Transmission Routes:
Sexual Contact: Accounts for of all transmissions. Risk per exposure ranges from . Risk is elevated by concurrent STIs, advanced clinical stage, higher viral load, and vaginal bleeding.
Parenteral Transmission:
Sharing contaminated needles (risk: per episode).
Occupational exposure: for needlestick injuries and for blood splashes on mucous membranes.
Mother-to-Child (Vertical) Transmission: Risk is without antiretroviral therapy (ART) but drops to < 1\% with proper viral suppression.
Prevention Strategies:
Utilization of PrEP (Pre-Exposure Prophylaxis), PEP (Post-Exposure Prophylaxis), and TasP (Treatment as Prevention).
U = U: Defined as "Undetectable = Untransmittable," meaning individuals with undetectable viral loads cannot sexually transmit the virus.
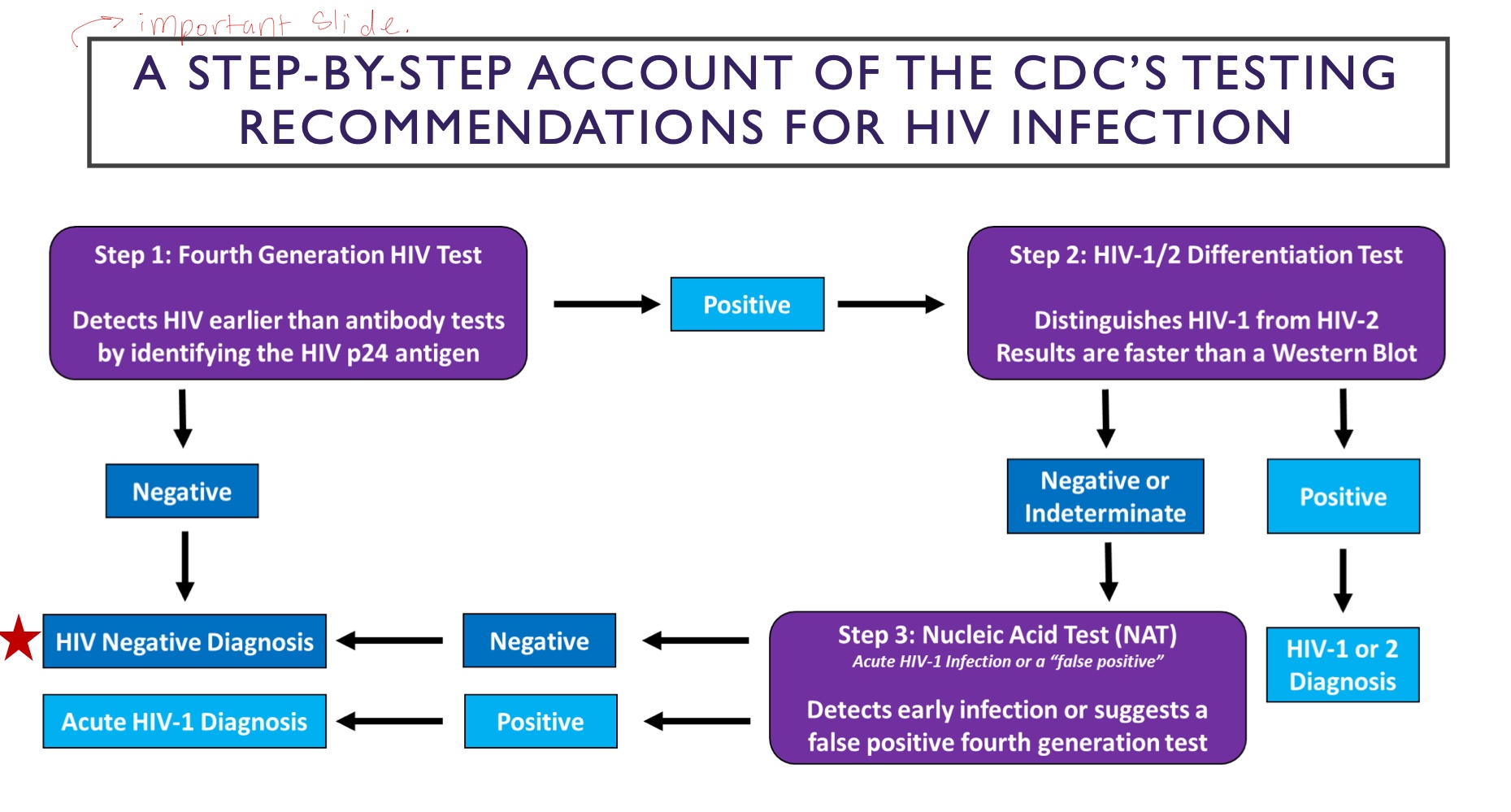
2. Screening and Diagnostic Testing
Screening Guidelines: Recommended for all individuals aged years. Pregnant individuals must be screened regardless of perceived risk.
Diagnostic Methods:
Nucleic Acid Test (NAT): Detects the virus approximately days post-exposure.
Antigen/Antibody (Ag/Ab) Test: Detects HIV within days.
Antibody Test (EIA): Detects antibodies within days.
Temporal Concepts:
Eclipse Phase: The initial period (approximately days) where the virus is undetectable by any test.
Window Period: The interval before anti-HIV antibodies are detectable, roughly days.
3. The HIV Life Cycle and Drug Targets
Characteristics: HIV is an enveloped single-stranded RNA virus. HIV-1 is prevalent in the U.S., while HIV-2 is specific to West Africa.
Seven Stages of Infection:
Binding (Attachment): HIV binds (gp 120) to CD4 receptors. then binds to the co-receptor CCR5/CXR4. Drug Target: CCR5 antagonists.
Fusion: Envelope fuses with the cell membrane. GP41 fusion to CD4 cells.Drug Target: Fusion inhibitors (e.g., enfuvirtide).
Reverse Transcription: Viral RNA is converted to DNA. Drug Target: NRTIs and NNRTIs.
Integration: Viral DNA enters the host nucleus via integrase. Drug Target: Integrase inhibitors (e.g., dolutegravir).
Replication: Host machinery produces HIV protein chains.
Assembly: New viral components gather at the cell surface.
Budding: Protease cleaves long protein chains to create mature, infectious virus. Drug Target: Protease inhibitors.
Acute HIV sundrome
HIV enters the body and infects a large nuber of CD4+ cells
This phase is characterised by very high viral load and significant drop in CD4 cellcount, leading to flu-like symptoms that may include fever, headache, fatigue, and lymphadenopathy. take 1-4 wells post exposure and lasts 2-4 weeks
clincial latency:
2-4 wekks after HIV exposure, the immine system beinds to respond , but the virus continues to replicate, leading to a gradual decline in CD4+ cells and an increase in viral load until the immune response is overwhelmed.During this time, individuals may remain asymptomatic, but their immune system is becoming increasingly compromised, setting the stage for opportunistic infections and other complications associated with AIDS.
4. Markers of Disease Progression
CD4 Cell Count: The primary indicator of immune function. Normal ranges are . Declines dictate the need for opportunistic infection (OI) prophylaxis.
Viral Load: Measures HIV RNA copies in the plasma to monitor treatment success.
Disease Phases: Progression typically follows: Acute Infection \rightarrow Clinical Latency \rightarrow AIDS.8-10 years
AIDS diagnosis:
CD4 cells < 200 cells/mm3 or presence of OI or AIDS defining illness
5. Opportunistic Infections (OIs)
Infections that exploit the weakened immune system of HIV-positive patients:
Candidiasis: Oropharyngeal or esophageal; occurs when CD4 < 200 \text{ cells/mm}^3.
Orophargeneal candidisis: painless, creamy white, plaque like lesions in the mouth or throat, which can cause difficulty swallowing and may lead to systemic infection if left untreated.
Esophageal candidiasis: genetaally presents with retrosternal buring pain or discomfort along with odynophagia, which can significantly impact nutrition and quality of life. Timely antifungal treatment is essential to alleviate symptoms and prevent complications.
Pneumocystis Pneumonia (PCP): Caused by ; presents at CD4 < 200 \text{ cells/mm}^3.
Toxoplasmosis (TE): Often results in encephalitis; occurs at CD4 < 100 \text{ cells/mm}^3.
Mycobacterium Avium Complex (MAC): Disseminated infection occurring at CD4 < 50 \text{ cells/mm}^3.