PS371 Unit 3 Notes
Substance-Related and Addictive Disorders
- Difference between substance use and disorder
- Substance use: moderate use with no impairment in social, educational, or occupational functioning
- 85% of Americans use caffeine
- Substance Use Disorders in DSM-5
- Pattern of substance use leading to significant impairment and distress
- Symptoms (need 2+ within a year)
- Taking more of the substance than intended
- Desire to cut down use
- Excessive time spent using/acquiring/recovering
- Craving for the substance
- Role disruption (e.g. can’t perform at work)
- Interpersonal problems
- Need at least 2 symptoms to meet criteria for disorder (can have multiple disorders for different substances)
- Different criteria for addiction and substance use disorder
- Depressants: alcohol-related disorders
- Psychological physiological effects of alcohol
- Central nervous system depressant
- Influences several neurotransmitter systems
- Dopamine
- Glutamate
- Specific target is GABA
- Relaxation
- Reduced anxiety
- Drowsiness
- Slowed respiration
- Psychological physiological effects of alcohol
- Chronic use
- Effects of chronic use
- Intoxication
- Withdrawal including delirium tremens → hallucinations, cardiovascular issues, can be fatal without medical treatment
- Nausea, vomiting
- Fetal alcohol syndrome
- Problems in fetus from alcohol use during pregnancy
- Intellectual disability
- Distinctive facial abnormalities
- Long term heavy alcohol use may lead to
- Dementia
- Brain atrophy
- Wernicke-korsakoff syndrome
- Neurological disorder
- Linked to vitamin B1 deficiency
- 1st stage: confusion, abnormal eye movements
- 2nd stage: memory problems, irreversible brain damage
- Dementia
- Effects of chronic use
- Progression of alcohol related disorders
- Those who start drinking at age 11 or earlier are at higher risk for chronic or severe alcohol use disorders
- Dependence usually develops over time, but course may be variable
- 20% are able to stop drinking on their own (spontaneous remission)
- Course is variable
- Women: 3 or more drinks in a day or more than 7 per week
- Men: 4 or more drinks in a day or more than 14 per week
- Alcohol and violence
- Drinking does not cause violence, but may increase the likelihood of impulsive behavior
- Alcohol is facilitator
- Sedative, hypnotic, or anxiolytic-related disorders
- Sedatives - calming
- Hypnotic - sleep inducing
- Anxiolytic - reducing anxiety tension
- Generally only prescribed for a few weeks (hard to taper off of medication)
- Have generally tranquilizing effects
- Combining depressants can have dangerous synergistic effects
- Also Act on GABA receptors
- Slow down brain activity
- Those who seek help more likely to be female, white, 35+
- Stimulants: an overview
- Most widely consumed drugs in the US due to both caffeine (coffee, energy drinks, soft drinks) and nicotine (tobacco)
- Stimulants increase alertness and energy
- Examples: amphetamines, cocaine, nicotine, caffeine
- Stimulant Use Disorder
- Effects of amphetamines
- Elation, vigor, reduced fatigue followed by extreme fatigue and depression
- Stimulate CNS by enhancing release and blocking reuptake of norepinephrine and dopamine
- Effects of Cocaine
- Short-lived sensations of elation, vigor, reduced fatigue
- Effects result from blocking the reuptake of dopamine
- Effects of amphetamines
- Tobacco-related disorders
- Effects of nicotine
- Stimulates nicotinic acetylcholine receptors in CNS, resulting in sensations of relaxation, wellness, pleasure
- Reinforcing effects
- Smoking has complex relationship to negative affect
- Appears to help improve mood in short-term
- Depression occurs more in those with nicotine dependence
- Effects of nicotine
- Caffeine-related disorders
- Caffeine Used by over 85% of Americans
- Found in tea, coffee, cola drinks, and cocoa products
- Small doses elevate mood and reduce fatigue
- Regular use can result in tolerance & dependence
- Caffeine blocks the reuptake of the neurotransmitter adenosine (promotes sleep and relaxation)
- More than 4 cups of coffee a day is too much caffeine (more than 400mg of caffeine)
- Opiates
- Opioids
- Opiate – natural chemical in the opium poppy with narcotic effects
- Opioids – natural and synthetic substances with narcotic effects
- Often referred to as analgesics
- Effects:
- Activate body’s enkephalins and endorphins
- Low doses induce euphoria, drowsiness, and slowed breathing
- Withdrawal symptoms can be lasting and severe
- Muscle aches, nausea, anxiety, intense cravings
- Brain makes similarly-acting substances called enkephalins, beta-endorphins, and dynorphins
- Opioids
- Cannabis-related disorders (hallucinogen-related disorder)
- Reactions include altered perceptions and mood swings
- Frequent, long-term users may experience impairments of memory, concentration, relationships with others, and employment
- Evidence regarding tolerance is contradictory
- Can be used in the treatment of some diseases
- Active ingredients are the tetrahydrocannabinols (THC)
- Hallucinogen-related disorders
- Hallucinations are altered sensory perceptions (e.g., seeing or hearing things that are not present)
- Hallucinogens can also produce delusions, paranoia
- Ex: feel irrationally threatened, feeling followed
- Examples of hallucinogens: LSD, psilocybin, mescaline, PCP
- Tolerance builds quickly, but resets after brief periods of abstinence
- Worsen psychosis
- Other drugs of abuse
- Inhalants
- Highest use during early adolescence (accessible, cheap, legal)
- Found in volatile solvents
- Breathed into the lungs directly
- Rapid absorption
- Examples: spray paint, hair spray, paint thinner, gasoline, nitrous oxide
- Effects similar to alcohol intoxication
- Produce tolerance and prolonged withdrawal symptoms
- Multiple negative physiological effects
- Gateway drug
- Can cause permanent damage to brain, liver, kidney, lungs, bone marrow, nerves
- Withdrawal not well researched
- Steroids
- Derived or synthesized from testosterone
- Used medicinally or to increase body mass
- No associated high
- Rather, dependence involves wanting to maintain the effects of the substance (i.e., increased muscle mass)
- May cause long-term mood disturbances
- Biological treatment of substance-related disorders
- Agonist substitution
- Safer drug with a similar chemical composition as the abused drug
- Antagonist drugs
- Drugs that block or counteract the positive effects of substances
- Aversive treatment
- Drugs that make use of substances extremely unpleasant
- EX: nausea, vomiting
- Efficacy of biological treatment
- Generally ineffective when used alone
- Used to help with withdrawal symptoms
- Agonist substitution
- Psychosocial treatment of substance-related disorders
- Community support programs
- Alcoholics Anonymous (AA) and related groups (e.g., NA) may be helpful; research is mixed
- Balancing treatment goals
- Controlled drinking vs. complete abstinence
- Abstinence works better for heavier drinking
- Controlled drinking vs. complete abstinence
- Component treatment
- Incorporate several elements such as psychotherapy and contingency management
- Ex: providing voucher for negative drug test, prizes
- Relapse prevention
- Incorporate several elements such as psychotherapy and contingency management
- Inpatient vs. outpatient care
- Little difference in effectiveness
- Community support programs
- Prevention of substance misuse
- Preventative efforts
- Recent shift away from education approaches to more wide-ranging, comprehensive approaches
- Programs like DARE may reduce illicit substance use but do not affect use of alcohol or tobacco
- Preventative efforts
- Inhalants
- Gambling Disorder
- Recurrent gambling leading to clinically significant distress or impairment
- Associated with four or more symptoms within a year:
- Difficulty stopping/reducing gambling
- Restlessness/irritability when trying to cut back
- Need to gamble with increasing amounts of money
- Frequent preoccupation
- Genetic research shows strong similarities in the biological origins of gambling disorders and substance use disorders
- Impulse-control disorders
- Intermittent explosive disorder
- Rare condition characterized by frequent aggressive outbursts leading to injury and/or destruction of property
- Often comorbid with mood and substance use disorders
- Can have legal consequences
- Kleptomania
- Failure to resist urge to steal unnecessary items
- Disorder may be more common in women than in men and typically starts in adolescence
- Comorbid with mood disorders and substance use disorders
- Pyromania
- Involves having an irresistible urge to set fires
- Rare even among convicted arsonists
- Treatment usually focuses on identifying urges and practicing incompatible behaviors
- CBT
- Intermittent explosive disorder
Eating Disorders
ED Demographics: Age
- Significantly earlier age of onset (<13) over the past few decades → COVID-19 pandemic
- Higher prevalence in boys in childhood
- Mostly seen for AN, ARFID
- 35-50% of childhood ED cases -> stunted growth, medical instability
- About half of patients fall off standard growth curve
- Can be irreversible
- Earlier the onset → greater the chronicity
Onset in childhood is predictive of persistence into adolescence and adulthood
- Particularly for girls
- Particularly when binge or purge is present
Most adult women with EDs developed them earlier in life
- For women >40 with EDs, average historical duration is ~26 years
- Rare to develop EDs after age 30
ED Demographics: Gender
- Boys make up a larger share of childhood EDs compared to adolescent or adult
- Roughly half of childhood EDs are in boys
- Roughly one third of adolescent EDs are in boys
- EDs in boys tends to decline towards adolescence, whereas EDs in girls increase
- EDs in boys/men often go unrecognized
- Stereotypes, expectations
- More concern with muscle mass, going to the gym
- Prevalence of EDs among Transgender and gender diverse individuals is 2-18%
- Difficulties with body image; minority
- Trauma
- PTSD
ED Demographics: Culture, Race
- EDs are increasing among those from a range of cultural backgrounds
- China: similar prevalence rates of AN (1.05%), BN (2.98%), and BED (3.53%) as seen in the West
- Rises in EDs in Eastern Europe, Middle East
- Improved epidemiological research with increased industrialization
- Increased disseminating knowledge on ED’s
- USA: prevalence of AN and BED is similar across Latinos, Asians, African Americans, and non-Latino Whites
- USA: BN is more prevalent among Latinos and African Americans than non-Latino Whites
- Rates of childhood EDs are higher for multiracial and Black children compared to White
ED Demographics: SES
- In the USA, childhood EDs are higher in families with greater economic insecurity
- Among adolescents and adults, there appears to be no association between ED prevalence and SES
- There is a positive association between treatment and SES
Anorexia Nervosa (AN)
- Very chronic
- Lifetime prevalence of 4% (females) and 0.3% (males)
- Rate of remission increases with treatment duration
- 25% at 2.5yrs, 68% at 8yrs, 84% at 16yrs
- Associated medical features
- Starving body borrows energy from internal organs, leading to organ damage
- Cardiac arrest, joint deterioration, broken bones, infertility
- Most deadly mental disorder due to physical consequences and suicide risk
- Criteria:
- A. Restriction of energy intake relative to requirements, leading to a significant low body weight in the context of the age, sex, developmental trajectory, and physical health (less than minimally normal/expected).
- B. Intense fear of gaining weight or becoming fat or persistent behavior that interferes with weight gain.
- C. Disturbed by one’s body weight or shape, self-worth influenced by body weight or shape, or persistent lack of recognition of seriousness of low bodyweight.
- Specifiers:
- Restricting type: During the last 3 months, has not regularly engaged in binge-eating or purging
- Binge-eating/purging type: During the last 3 months, has regularly engaged in binge-eating or purging
- Severe weight loss
- 3 months before diagnosis
- Remission:
- Partial remission: After full criteria met, low body weight has not been met for sustained period, BUT at least one of the following two criteria still met:
- 1. Intense fear of gaining weight/becoming obese or behavior that interferes with weight gain OR
- 2. Disturbed by weight and shape.
- NG tubes
- Full remission: After full criteria met, none of the criteria met for sustained period of time.
- Partial remission: After full criteria met, low body weight has not been met for sustained period, BUT at least one of the following two criteria still met:
Bulimia Nervosa (BN)
- Lifetime prevalence of 2.59% (females) and 1.21% (males)
- Rate of remission increases with treatment duration
- 27% at 1yr, 70% at 10yrs
- Onset typically in adolescence
- Associated medical features
- Most people with bulimia nervosa are within 10% of normal body weight
- Compensatory behaviors can result in severe medical problems, including cardiac arrest, complete loss of colon function
- Loss of electrolytes
Criteria:
A. Recurrent episodes of binge eating, as characterized by both:
a. Eating, within any 2-hour period, an amount of food that is definitively larger than what most individuals would eat in a similar period of time under similar circumstances. (could be around 8,000-10,000 calories)
- Objective vs. subjective binges
b. A feeling that one cannot stop eating or control what or how much one is eating.
B. Recurrent inappropriate compensatory behaviors in order to prevent weight gain such as vomiting; misuse of laxatives, diuretics, or other medications; fasting or excessive exercise.
C. The binge eating and inappropriate compensatory behaviors occur, on average, at least once a week for 3 months.
D. Self-evaluation is unjustifiably influenced by body shape and weight.
E. The disturbance does not occur exclusively during episodes of anorexia nervosa.
Binge Eating Disorder (BED)
- Lifetime prevalence of 1.85% (females) and 0.74% (males)
- Better response to treatment than other eating disorders
- Rate of remission increases quickly through treatment
- 25% at 1yr, 82% at 4yr
- Approximately 20% of individuals in weight-control programs have BED
- Approximately half of candidates for bariatric surgery have BED
- GLP 1 + Ozempic starting to be used for treatment
Criteria:
A. Recurrent episodes of binge eating characterized by both of the following:
a. Eating, within any 2-hour period, an amount of food that is definitively larger than what most individuals would eat in a similar period of time under similar circumstances.
b. A sense of lack of control over eating during the episode
B. The binge-eating episodes are associated with three (or more) of the following:
a. Eating much more rapidly than normal
b. Eating until feeling uncomfortably full
c. Eating large amounts of food when not feeling physically hungry
d. Eating alone because of feeling embarrassed by how much one is eating
e. Feeling disgusted with oneself, depressed, or very guilty after overeating
C. Marked distress regarding binge eating is present.
D. The binge eating occurs, on average, at least once a week for 3 months.
E. The binge eating is not associated with the regular use of inappropriate compensatory behaviors and does not occur exclusively during the course of anorexia nervosa or bulimia nervosa
Remission:
- In partial remission: After full criteria for binge-eating disorder were previously met, binge eating occurs at an average frequency of less than one episode per week for a sustained period of time.
- In full remission: After full criteria for binge- eating disorder were previously met, none of the criteria have been met for a sustained period of time.
- Current severity:
- Mild: 1–3 binge-eating episodes per week
- Moderate: 4–7 binge-eating episodes per week
- Severe: 8–13 binge-eating episodes per week
- Extreme: 14 or more binge-eating episodes per week
Avoidant / Restrictive Food Intake Disorder (ARFID)
- Lifetime prevalence of 2.5% (females), 1.4% (males), 2.9% (TGD)
- Extreme “picky eating”
- Textures
- Temperatures
- Colors
- Smells
- Sizes
- Combinations
- Onset in childhood
- Significant nutritional deficiencies
- Failure to meet expected weights / heights
Criteria:
A. An eating or feeding disturbance (e.g., apparent lack of interest in eating or food) as manifested by persistent failure to meet appropriate nutritional and/or energy needs associated with one (or more) of the following:
a. Significant weight loss (or failure to achieve expected weight gain or faltering growth in children)
b. Significant nutritional deficiency.
c. Dependence on enteral feeding or oral nutritional supplements.
d. Marked interference with psychosocial functioning.
B. The disturbance is not better explained by lack of available food or by an associated culturally sanctioned practice.
C. The eating disturbance does not occur exclusively during the course of anorexia nervosa or bulimia nervosa.
D. The eating disturbance is not attributable to a concurrent medical condition or not better explained by another mental disorder.
- Remission:
- In remission: After full criteria for avoidant / restrictive food intake disorder were previously met, the criteria have not been met for a sustained period of time.
Etiology of Eating Disorders
Genetic influences
- High heritability (AN 50-70%; BN 50-60%; BED 40-60%)
- Dysregulated dopamine receptor gene (reward processing, food intake behaviors)
- Dysregulated melanocortin 4 receptor gene (BED; appetite, energy balance)
Neurobiological mechanisms
- Altered hypothalamic function (high in AN, low in BN/BED) regulating hunger and satiety
- Altered prefrontal cortex function (high in AN, low in BN/BED) regulating impulse control
- Dysregulated serotonin production (mood, appetite, impulse control)
- Dysregulated dopamine production (food / restriction reward)
Environmental and Psychological
- Societal pressure, OCD, poor body image, trauma
Metabolic genetic component
- Metabolic predispositions may enhance ability to sustain AN
- Enhanced insulin sensitivity stabilizes glucose metabolism at low body fat and energy levels
- Body feels better at lower energy and body weight levels
- Low leptin response, low fat storage may make it harder to regain and maintain weight
- Low BMI, independent of ED behaviors
Comorbidities
Psychological
- Anxiety
- PTSD - 3X higher in BN (66%) than AN/BED ( 20%)
- Depression
- OCD - highest in AN
- Autism - Highest in ARFID
- Suicidality - 4X higher in AN-BP (25%) than AN-R (8%)
Medical
- Functional gastroint - highest in BN
- Cardiovascular - highest in AN
- Osteoporosis - highest in AN
- Type II diabetes - 8X higher in BED (33%) than BN (4%)
Treatment
- CBT
- For individuals with AN, BN, BED
- Disrupting behavioral patterns and challenging negative thoughts that perpetuate symptoms reduces ED severity
- Common components:
- Establish regular pattern of eating, systematic exposure to forbidden or binge foods, and skills to resist urges to compensate (e.g., restrict, purge)
- Modify dysfunctional beliefs about body shape, weight concerns, diet behavior
- Maintenance planning and relapse prevention
- *CBT is better suited for AN relapse prevention following HLOC weight gain; it is not well suited for weight restoration itself
- EX: therapist takes bite of cupcake, go to ice cream store to look at ice cream
- Family-based therapy
- Active and structured family involvement in the treatment of adolescents suffering from EDs significantly increases the likelihood of positive treatment outcomes
- For adolescents with AN, BN who are medically stable
- Consists of three phrases:
- Parents take charge of the process of nutritional rehabilitation and weight restoration with the help of the therapist
- Control over eating is returned to the adolescent in an age appropriate fashion
- Issues of psychosocial development in the absence of an eating disorder are addressed
- FBT also aims to correct misperceptions and misattributions of blame for the patient’s illness. Neither the parents nor the adolescent is responsible for the ED.
- Interpersonal psychotherapy
- Symptoms are related to interpersonal issues, and addressing interpersonal problems can alleviate the symptoms of the ED
- For individuals with BN, BED
- Explore, identify, and change maladaptive interpersonal patterns; as more adaptive interpersonal patterns are developed, ED symptoms will decrease
- Consists of three phases:
- Raising awareness of how interpersonal factors are associated with ED symptoms
- Addressing and resolving the client’s interpersonal conflict and problems
- Discussing impending termination, reviewing progress made in therapy, and exploring ways the client can address interpersonal difficulties in the future
Challenges in treatment
Resistance to treatment
- Denial of the disorder, lack of insight, ambivalence towards change
- More prevalent in AN
Chronicity of disorders
- 20-30% of patients with AN develop enduring form of disorder (>10yrs)
- High relapse rates (26%), particularly in AN and BN
- Hospitalization occurs in 26% of patients
Ethical dilemmas
- Respect of patient autonomy vs duty to protect
- Treatment against one’s will
Palliative Care for SE-AN
- Prioritize quality of live and relief of suffering over ED treatment
- Decreases acute care use and costs
- Suggested eligibility criteria:
- Lack of sustained treatment response
- Physical and psychological decline
- Terminal course
- “Terminal” AN defined as:
- Diagnosis of AN
- Age 30+
- Prior persistent engagement in high-quality, multidisciplinary ED care
- Consistent, clear expression by patient that they understand further treatment is futile, choose to stop trying to prolong life, and accept that death is natural outcome
Schizophrenia
- Schizophrenia*: a broad spectrum of cognitive and emotional dysfunctions including delusions and hallucinations, disorganized speech and behavior, and inappropriate emotions
- Emil Kraepelin – used the term dementia praecox* to describe schizophrenic syndrome
- Early subtypes of schizophrenia – Catatonia (rigid physical movement), hebephrenia (disorganized speech, no logical connections between words), and paranoia
- Eugen Bleuler – introduced the term “schizophrenia”
- Identified the different variants that were all included within a spectrum
- Positive symptoms*:
- Delusions
- Hallucinations
- Negative symptoms*:
- Avolition—inability to initiate and persist in activities
- Alogia—absence of speech
- Anhedonia—presumed lack of pleasure
- Asociality—lack of interest in social interactions
- Affective flattening—do not show emotions when emotions would normally be expected
- Disorganized symptoms*:
- Erratic speech & emotions
- Inappropriate affect and disorganized behavior
- Meeting DSM-5 Criteria
- Core symptoms (at least 2 or more required for a significant portion of 1 month; continuous disturbance/impairment for at least 6 months):
- 1. Delusions
- 2. Hallucinations
- 3. Disorganized speech
- 4. Grossly disorganized or catatonic behavior
- 5. Negative symptoms
- EX: Lauren Kennedy West living with Schizophrenia symptoms
- Auditory, tactile, olfactory hallucinations
- Hear voices telling her to do things when off medication → commands around self-harm, negative actions
- Still experience symptoms even on medications
- Very coherent and clear
- EX: Lauren Kennedy West living with Schizophrenia symptoms
- Schizophreniform disorder
- Psychotic symptoms lasting between 1 to 6 months (>6 months would be diagnosed as schizophrenia)
- Associated with relatively good functioning
- Most patients resume normal lives
- Lifetime prevalence: approximately 0.2%
- Might diagnose schizophreniform before diagnosing with schizophrenia
- First psychotic episode usually occurs in early adulthood
- Schizoaffective disorder
- Symptoms of schizophrenia + additional experience of a major mood episode (depressive or manic) - symptoms can be mood congruent or incongruent
- Psychotic symptoms must also occur outside the mood disturbance
- Prognosis is similar for people with schizophrenia
- Delusional disorder
- Characterized by delusions that are contrary to reality
- Lack other positive and negative symptoms
- Types of delusions include
- Erotomanic - “this person’s in love with me”
- Grandiose - pregnant with Obama’s baby
- Jealous - “everyone wants to be me”
- Persecutory - aliens are coming down to Earth
- Somatic - bugs under skin
- Not much overlap in symptoms
- Better prognosis than schizophrenia
- Characterized by delusions that are contrary to reality
Catatonia
- Unusual motor responses, particularly immobility or agitation, and odd mannerisms
- Tends to be severe and quite rare
- May be present in psychotic disorders or diagnosed alone, and may include:
- Stupor, mutism, maintaining the same pose for hours
- Opposition or lack of response to instructions
- Repetitive, meaningless motor behaviors
- Mimicking others’ speech or movement
Psychotic disorders due to other causes
- Psychosis may occur as the result of substance use, some medications, and some medical conditions
- Knowing these causes is important for treatment
- Address underlying cause
- Include:
- Substance/medication-induced psychotic disorder*
- Psychotic disorder associated with another medical condition*
- Brief psychotic disorder
- Characterized by positive symptoms of schizophrenia (e.g., hallucinations or delusions) or disorganized symptoms
- Lasts less than one month
- Briefest duration of all psychotic disorders
- Typically precipitated by trauma or stress
- Does not typically re-emerge
Schizophrenia by the numbers
- About 0.2% to 1.5% (or about 1% population)
- Often develops in early adulthood
- Can emerge at any time; childhood cases are extremely rare but not unheard of
Schizophrenia: Gender and culture
- Schizophrenia affects men and women about equally
- Females tend to have a better long-term prognosis
- Onset slightly earlier for men
Cultural factors
- Psychotic behaviors not always pathologized
- Yet schizophrenia is found at similar rates in all cultures
Causes of Schizophrenia: Genetic Research
- Family studies
- Inherit a tendency for schizophrenia, not specific forms of schizophrenia
- Risk increases with genetic relatedness
- Twin studies
- Monozygotic twins have greater concordance than dizygotic twins
- Adoption studies
- Adoptee risk for developing schizophrenia is high if a biological parent has schizophrenia
- But risk is lower than for children raised by their biological parent with schizophrenia
- Adoptee risk for developing schizophrenia is high if a biological parent has schizophrenia
Case study: The Galvin family
- 12 children (10 boys, 2 girls)
- 6 boys had schizophrenia
- Environmental and familial stressors
- Trauma, secrecy, stigma
- Non-diagnosed daughters
- experienced emotional distress, fear, neglect
- Scientists studying the family contributed to discoveries regarding
- COMT and DISC1 genres (implicated in schizophrenia risk)
- Role of neurodevelopmental factors in schizophrenia onset
Search for genetic and behavioral markers
- Genetic markers: Linkage and association studies
- Endophenotypes
- Schizophrenia is likely to involve multiple genes
- Behavioral marker (endophenotype): Smooth-pursuit eye movement
- Schizophrenia patients show reduced ability to track a moving object with their eyes
- Relatives of schizophrenic patients also have deficits in this area
Causes of schizophrenia: Neurobiological influences
- The dopamine hypothesis: schizophrenia is partially caused by overactive dopamine
- Evidence
- Drugs that increase dopamine (agonists) result in schizophrenic-like behavior
- Drugs that decrease dopamine (antagonists) reduce schizophrenic-like behavior
- Problem: overly simplistic
- Many neurotransmitters are likely involved
Causes of schizophrenia: other neurobiological influences
- Structural and functional abnormalities in the brain
- Enlarged ventricles and reduced tissue volume
- Hypofrontality – less active frontal lobes (a major dopamine pathway)
- Viral infections during early prenatal development
- Findings are inconsistent
- Marijuana use also increases risk among at-risk individuals
Causes of schizophrenia: psychological and social influences
- The role of stress •
- May activate underlying vulnerability and increase risk of relapse •
- Family interactions
- Unsupported theories: Schizophrenogenic mother, double bind communication (impair communication)
- High expressed emotion* (EE) – associated with relapse
- Key take aways on psychological factors:
- May function as the diathesis in a diathesis-stress model
- Exert only a minimal effect in producing schizophrenia
Medical treatment of schizophrenia
- Prior to 1950s, medical treatments were generally ineffective and sometimes barbaric
- Development of antipsychotic medications (e.g., Thorazine - strong sedative type drug, has side effects, patients not very responsive)
- Often the first line treatment for schizophrenia
- Began in the 1950s
- Most reduce or eliminate positive symptoms
- Primarily affect dopamine system, but also affect serotonergic and glutamate system
- Acute and permanent side effects may occur with both first-generation and second generation antipsychotics
- Loss of individuation
- Massive weight gain
- Parkinson’s-like side effects
- Tardive dyskinesia
- Compliance with medication is often a problem
- Aversion to side effects
- Financial cost
- Poor relationship with doctors
Psychosocial treatment
- Historical precursors: Psychodynamic therapy was not effective
- Psychosocial approaches
- Behavioral methods like the token economy* that reward adaptive behavior
- Community care programs
- Social and living skills training
- Virtual reality-based interventions
- Behavioral family therapy resembles classroom education
- Vocational rehabilitation
- Illness management and recovery
- Engages patient as an active participant in care
- Continuous goal setting and tracking
- Modules include social skills training, stress management, substance use
- Cultural considerations
- Take into account cultural factors that influence individuals’ understanding of their own illness (e.g., supernatural beliefs)
- Involve family and community if possible
- Always adjunctive, never primary
CBT for psychosis?
- Reduces positive symptoms: Helps challenge and reframe delusions and hallucinations, reducing their intensity and emotional distress.
- Improves coping: Teaches coping strategies for managing symptoms, improving self efficacy
- Prevents relapse: Reduces relapse risk by addressing cognitive biases and improving treatment adherence.
- Early intervention is key: Particularly effective in early psychosis, may prevent worsening
- Moderately effective overall, benefits for relapse prevention and social integration
- Limitations
- Used with medication, not as a stand-alone treatment
- Requires trained therapists and can be limited by the severity of symptoms
Personality Disorders
- Enduring, inflexible predispositions
- Maladaptive, causing distress and/or impairment
- High comorbidity with other disorders
- Generally poor prognosis
- Patients may not feel that treatment is necessary
- “Kind” (categorical) vs. ”degree” (dimensional)
- Personality disorders have traditionally been assigned as all-or-nothing categories (like the disorders I will introduce to you today)
- DSM-5 retained categorical diagnoses but also introduced additional dimensional model of personality disorders
- Dimensional model: Individuals are rated on the degree to which they exhibit various personality traits
- Having categories useful in treatment and insurance
- Alternative model for personality disorders (AMPD) Dimensional model introduced in DSM-5, has the following key features:
- 1. Impairment in personality functioning (Criterion A)
- Self-functioning (identity, self-direction) or interpersonal functioning (empathy, intimacy)
- 2. Pathological personality traits (Criterion B)
- Negative affectivity (vs. emotional stability) – e.g., anxiety, hostility
- Detachment (vs. extraversion) – e.g., withdrawal, anhedonia
- Antagonism (vs. agreeableness) – e.g., manipulativeness, deceitfulness
- Disinhibition (vs. conscientiousness) – e.g., impulsivity, irresponsibility
- Psychoticism (vs. lucidity) – e.g., unusual beliefs, eccentricity
- Five factor model of personality (“Big Five”)
- Openness to experience
- Conscientiousness
- Extraversion
- Agreeableness
- Neuroticism
- Cross-cultural research establishes the relatively universal nature of the five dimensions
- Personality disorders stats and facts
- Affect about 10% of the general population
- Origin of PDs thought to begin in childhood
- Tend to run a chronic course if untreated
- May transition into a different PD
- Personality disorders and gender Gender distribution and gender bias in diagnosis:
- Men more often show traits like aggression and detachment; women more often show submission and insecurity
- Antisocial – more often male
- Histrionic – equal numbers of male and female
- Personality disorder clusters
- Cluster A: Odd or eccentric
- Paranoid, schizoid, and schizotypal PD
- Cluster B: Dramatic or erratic
- Antisocial, borderline, histrionic, and narcissistic PD
- Cluster C: Anxious or fearful
- Avoidant, dependent, and obsessive-compulsive PD
Cluster A: Paranoid PD
- Clinical features:
- Pervasive and unjustified mistrust and suspicion
- Few meaningful relationships, sensitive to criticism
- Causes: may involve early learning that people and the world are dangerous or deceptive
- Cultural factors: more often found in people with experiences that lead to mistrust of others
- Treatment focuses on development of trust; cognitive therapy to counter negativistic thinking
- Ex: “Aviator” movie - main character locks himself in room and does not leave
Cluster A: Schizoid PD
- Clinical features:
- Pervasive pattern of detachment from social relationships
- Very limited range of emotions in interpersonal situations
- Etiology is unclear but may have significant overlap with autism spectrum disorder
- Treatments focus on the value of interpersonal relationships and on building empathy and social skills
- “Solo character”
- Avoid emotional interactions with others
Cluster A: Schizotypal PD
- Clinical features:
- Behavior and beliefs odd and unusual
- Socially isolated and highly suspicious
- Magical thinking, ideas of reference, and illusions
- Many meet criteria for major depression
- Some conceptualize this as resembling a milder form of schizophrenia
- Ex: Willy Wonka (peculiar speech patterns, magical thinking)
- Ex: Dr. Stanton had patient that believed that skateboarding was the best way to get to school (took an hour and a half)
- Odd beliefs around the best type of shoes regardless of weather
- Some type of shoes benefit quality of hair
Schizotypal PD causes and treatment
- Causes:
- Mild expression of “schizophrenia genes”?
- May be more likely to develop after childhood maltreatment or trauma, especially in men
- More generalized brain deficits may be present
- Treatment options:
- Address comorbid depression
- Main focus is combination of medication, cognitive behavior therapy, and social skills training
Cluster B: Antisocial PD
- Clinical features:
- Failure to comply with social norms
- Violation of the rights of others
- Irresponsible, impulsive, and deceitful
- Lack of a conscience, empathy, and remorse
- “Sociopathy,” “psychopathy*” typically refer to very similar traits
- Sociopathy - impulsive and emotionally reactive
- Psychopathy - cold, remorseless, calculated
- May be very charming, interpersonally manipulative
- Lack of modeling of empathy in childhood
Cluster B: Antisocial PD
- Often show early histories of behavioral problems, including conduct disorder
- “Callous-unemotional” type of conduct disorder more likely to evolve into antisocial PD
- Families with inconsistent parental discipline and support
- Families often have histories of criminal and violent behavior
Development of Antisocial PD
- Genetic influences: more likely to develop antisocial behavior if parents have a history of antisocial behavior or criminality
- Developmental influences: high-conflict childhood increases likelihood of APD in at-risk children
- Impaired fear conditioning: Children who develop APD may not adequately learn to fear aversive consequences of negative actions (e.g., punishment for setting fires)
- Arousal theory: People with APD are chronically under-aroused and seek stimulation from the types of activities that would be too fearful or aversive for most
Treatment of Antisocial PD
- Few seek treatment on their own
- Antisocial behavior is predictive of poor prognosis
- Emphasis is placed on prevention and rehabilitation
- Often incarceration is the only viable alternative
- May need to focus on practical (or selfish) consequences (e.g., if you assault someone you’ll go to prison)
Cluster B: Borderline PD
- Clinical features:
- Unstable moods and relationships
- Impulsivity, fear of abandonment, very poor self-image
- Self-harm and suicidal gestures
- Comorbidity rates are high with other mental disorders, particularly mood disorders, substance use disorders, and eating disorders
- Can be “manipulative” - skills deficit due to individual not being able to communicate otherwise of their pain
- A lot more treatment potential
- Ex: patient with BPD from video in class describes herself as a turtle without a shell in the past
- Suicidal in the past
- Patient had “psychotic break” after father’s death
- Handwriting sloppy
- Cutting wrists at work
- Telling boss that she wrote in her journal that she felt like she would kill her baby if she had one
- Unstable moods and relationships
How might clinical features of borderline PD contribute to stigma?
Examples:
1. Stigmatization in mental health care
2. Negative media portrayals
3. Social and interpersonal stigma
Borderline PD Causes
- Causes
- Strong genetic component
- High emotional reactivity may be inherited
- May have impaired functioning of limbic system
- Early trauma/abuse increase risk
- Could be abandonment from parents/guardians
- Person could be put on a pedestal - experiencing abandonment from person on pedestal devastating
- Could be abandonment from parents/guardians
- “Triple vulnerability” model
- Generalized biological vulnerability
- Generalized psychological vulnerability
- Specific psychological vulnerability
- Could be early trauma, early abuse, early abandonment
Borderline PD treatment
- Treatment options
- Antidepressant medications provide some short-term relief
- Dialectical behavior therapy* (DBT), developed by Marsha Linehan, is most promising treatment
- Focus on dual reality of acceptance of difficulties and need for change
- Four key skills:
- 1. Mindfulness
- 2. Distress tolerance
- 3. Emotion regulation
- 4. Interpersonal effectiveness
- Marsha Linehan (video in class):
- Patients sensitive to invalidation or statement that they were the problem in CBT → switch to DBT
- Technology of acceptance
- Problem-solving validation
CBT vs. DBT
- CBT:
- Primarily focuses on cognitive restructuring, where the goal is to identify and change distorted or unhelpful thinking patterns that lead to emotional distress.
- It also focuses on modifying maladaptive behaviors through reinforcement and behavior modification techniques.
- DBT:
- DBT, while it also focuses on changing harmful behaviors, puts a stronger emphasis on emotional regulation, mindfulness, and acceptance.
- The goal is to help individuals balance emotional acceptance with behavioral change. DBT teaches patients to accept themselves and their emotions while also working to change dysfunctional patterns.
Cluster B: Histrionic PD
- Clinical features
- Overly dramatic and sensational
- May be sexually provocative
- Often impulsive and need to be the center of attention
- Thinking and emotions are perceived as shallow
- More commonly diagnosed in females
Histrionic PD causes and treatment
- Causes
- Etiology unknown due to lack of research
- Often co-occurs with antisocial PD, suggesting it may be a sextyped variant
- Treatment options
- Focus on attention seeking and long-term negative consequences
- Targets may also include problematic interpersonal behaviors
- Little evidence that treatment is effective
Cluster B: Narcissistic PD
- Clinical features
- Exaggerated and unreasonable sense of self-importance
- Preoccupation with receiving attention
- Lack sensitivity and compassion for other people
- Highly sensitive to criticism; envious and arrogant
Narcissistic PD causes and treatment
- Causes are largely unknown
- Failure to learn empathy as a child
- Sociological view – product of the “me” generation
- Treatment options
- Focus on grandiosity, lack of empathy, unrealistic thinking
- Emphasize realistic goals and coping skills for dealing with criticism
- Little evidence that treatment is effective
Cluster C: Avoidant PD
- Clinical features:
- Extreme sensitivity to the opinions of others
- Highly avoidant of most interpersonal relationships
- Interpersonally anxious and fearful of rejection
- Low self-esteem
Avoidant PD causes and treatment
- Causes
- May be linked to schizophrenia; occurs more often in relatives of people with schizophrenia
- Experiences of early rejection
- Childhood experiences of neglect, isolation, rejection, and conflict with others
- Treatment
- Similar to treatment for social phobia
- Focus on social skills, entering anxiety-provoking situations
- Good relationship with therapist is important
Cluster C: Dependent PD
- Clinical features:
- Reliance on others to make major and minor life decisions
- Unreasonable fear of abandonment
- Clingy and submissive in interpersonal relationships
Dependent PD causes and treatment
- Causes
- Not well understood but may be linked to failure to learn independence
- Treatment options
- Therapy typically progresses gradually due to lack of independence
Cluster C: Obsessive-Compulsive PD
- Clinical features:
- Excessive and rigid fixation on doing things the right way
- Highly perfectionistic, orderly, and emotionally shallow
- Unwilling to delegate tasks because others will do them wrong
- Difficulty with spontaneity
- Often have interpersonal problems
- Obsessions and compulsions are rare
- Causes and treatments
- Causes are not well known
- Moderate genetic contribution
- Treatment
- Treatment targets include cognitive reappraisal techniques to reframe compulsive thoughts
- Target rumination, procrastination, and feelings of inadequacy
- Causes are not well known
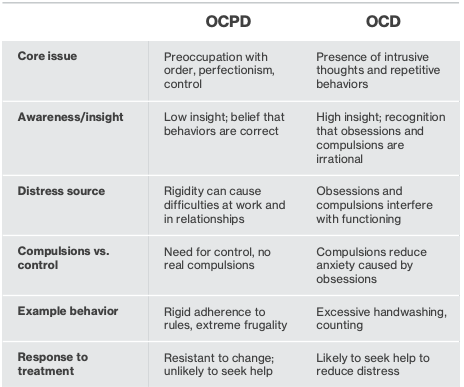
OCPD vs. OCD