CHAPTER 3: PRENATAL DEVELOPMENT
the germinal stage
The germinal stage lasts from conception to implantation, approximately 2 weeks.
The zygote starts dividing within 36 hours of conception.
The blastocyst forms through cell differentiation.
It consists of two distinct layers in the inner part, known as the embryonic disk.
The outer part differentiates into four membranes called the trophoblast.
Prior to implantation, the dividing cells are nourished by the yolk of the original egg.
There is no gain in mass until implantation.
Miscarriage (spontaneous abortion) usually stems from abnormalities in development, with about one-third of all pregnancies resulting in miscarriage.
the embryonic stage
The embryonic stage begins with implantation (3rd week) and lasts through the 8th week.
During this stage, major organ systems differentiate.
Developmental trends include:
Cephalocaudal: Head takes precedence over lower parts of the body.
Proximodistal: Development proceeds from the central axis of the body outward.
The embryonic disk differentiates into three layers:
Ectoderm (outer layer): Develops into the nervous system, sensory organs, nails, hair, teeth, and the outer layer of skin.
Endoderm (inner layer): Forms the digestive and respiratory systems, liver, and pancreas.
Mesoderm (middle layer): Develops into the excretory, reproductive, and circulatory systems, muscles, skeleton, and inner layer of skin.
The neural tube develops into the brain and spinal cord.
Head and blood vessels begin to form during the 3rd week.
Arm and leg buds appear in the 4th week.
Eyes, ears, nose, and mouth begin to take shape.
Limbs elongate, and facial features become distinct by the 8th week.
Teeth buds have formed, and the kidneys and liver are functioning by the 8th week.
By the end of the first month, the neural tube is producing 400 million neurons per day.
Neurons migrate to parts of the brain where they will function as different brain structures.
Cerebral hemispheres form during the 5th week.
Cells in the nervous system begin to release neurotransmitters in the 2nd month.
sexual differentiation
Nondescript sex organs form between 5 to 6 weeks.
Internal and external genitals at this stage resemble female structures, including Müllerian (female) ducts and Wolffian (male) ducts.
Sex organs begin to differentiate based on the genetic code during the 7th week.
The presence of a Y chromosome causes testes to differentiate.
The absence of a Y chromosome causes ovaries to differentiate.
Distinct external genital structures are evident by 4 months.
Male hormonal influences:
Testes produce androgens.
Testosterone differentiates the male duct system (Wolffian).
DHT (dihydrotestosterone) triggers the development of male external genital organs.
Müllerian inhibiting substance (MIS) prevents Müllerian ducts from developing into the female duct system.
Female hormonal influences:
Small amounts of androgens are produced, playing a role in secondary sexual characteristics in adolescence and are important in the sex drive of females.
Wolffian ducts degenerate, and Müllerian ducts develop into Fallopian tubes, uterus, and the inner part of the vagina.
amniotic sac and placenta
The amniotic sac is surrounded by a clear membrane and contains amniotic fluid, protecting the embryo/fetus within the uterus.
The placenta is a mass of tissue that exchanges nutrients and wastes between the embryo/fetus and the mother.
The umbilical cord connects the fetus to the placenta.
The placenta acts as a filter between the bloodstream of the mother and the bloodstream of the embryo/fetus.
Oxygen and nutrients reach the child.
Carbon dioxide and waste pass to the mother.
Many germs and drugs may also reach the child.
The placenta secretes hormones that prepare breasts for nursing and stimulate contractions that prompt childbirth.
the fetal stage
The fetal stage extends from the third month through birth.
By the end of the first trimester:
Major organ systems are formed.
Fingers and toes are formed.
Eyes can be distinguished.
The sex of the fetus can be determined visually.
By the end of the second trimester:
The fetus opens and shuts eyes.
The fetus sucks its thumb.
The fetus alternates between sleep and wakefulness.
The fetus responds to light and sound.
Born at 22 to 25 weeks - about 50% survival rate related to quality of care.
By the end of the third trimester:
The heart and lungs are increasingly capable of sustaining independent life.
The fetus gains in weight and length.
During the 7th month, the fetus turns upside-down in the uterus.
Born at end of 7th month – nearly 90% survival rate.
First movements begin about the 4th or 5th month.
By 29-30 weeks, the fetus:
Moves vigorously and turns somersaults.
Begins slow squirming movements.
Begins sharp jabbing and kicking movements.
As the fetus grows, movements become restricted.
Prenatal activity predicts activity levels after birth.
environmental influences on prenatal development
Malnutrition in the mother (especially in the last trimester) is linked to:
Low-birth-weight
Prematurity
Stunted growth
Retardation of brain development
Cognitive deficiencies
Behavioral problems
Cardiovascular disease
Effects of fetal malnutrition can sometimes be overcome by supportive caregiving environment.
Maternal obesity is linked to a higher risk of stillbirth and increases the risk of neural tube defects.
Nutrients that are important during pregnancy include:
Protein
Vitamins A, B, C, D, and E
Iron; trace minerals zinc and cobalt; folic acid
Calcium
Calories
Most women who eat a well-rounded diet do not need supplements, but most doctors recommend them to be safe.
Mothers who are too slim risk preterm deliveries and low-birth-weight babies.
Amount of recommended weight gain depends on pre-pregnancy weight:
BMI below 18.5: gain 28 to 40 pounds
Normal weight: gain 25 to 35 pounds
BMI between 25 and 29.9: gain 15 to 25 pounds
BMI over 30: gain 11 to 20 pounds
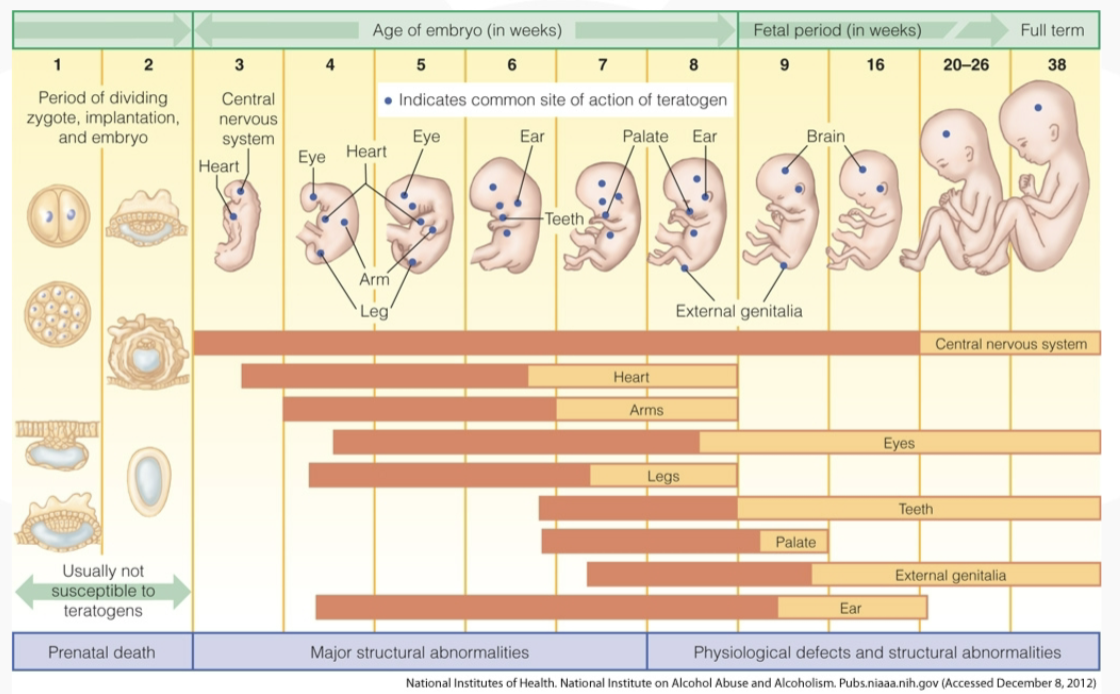
what are teratogens?
Teratogens are environmental agents that can harm the embryo or fetus, including:
Drugs ingested by the mother
Substances produced by the mother
Heavy metals such as lead and mercury
Excessive hormones
Radiation
Pathogens (bacteria and viruses)
Critical periods of vulnerability correspond to times when organs are developing.
Syphilis can cause miscarriage, stillbirth, or congenital syphilis.
It can be diagnosed by routine blood tests early in pregnancy.
The baby probably will not contract syphilis if the infected mother is treated before the 4th month of pregnancy.
If the infected mother is not treated, the baby has a 40-70% chance of being infected in utero or developing congenital syphilis.
HIV/AIDS (human immunodeficiency virus/acquired immunodeficiency syndrome) disables the body’s immune system and is lethal unless treated.
About 25% of babies born to HIV/AIDS-infected mothers become infected.
Many babies are infected during childbirth.
HIV is also found in breast milk.
Influenza (Flu) is a respiratory infection that may be related to fetal brain abnormalities, autism, and schizophrenia.
Rubella (German measles) is a viral infection that may cause birth defects.
Pre-Eclampsia (Toxemia) may cause premature or undersized babies and is a cause of pregnancy-related maternal death.
Rh Incompatibility involves the transfer of maternal antibodies that may cause brain damage or death.
effects of drugs taken by the mother
Accutane, prescribed for difficult cases of acne, is linked to numerous abnormalities during the first trimester.
Thalidomide can result in missing or stunted limbs.
Tetracycline, an antibiotic, may lead to yellowed teeth and bone abnormalities.
Progestin, a hormone, can masculinize the external sex organs of a female embryo.
DES, a hormone, can cause cervical and testicular cancer.
High doses of vitamins A and D are associated with central nervous system damage, small head size, and heart defects.
Maternal addiction to heroin and methadone is linked to low-birth-weight, prematurity, and toxemia; the baby may be born addicted.
Marijuana (Cannabis) use carries a risk of low-birth-weight and immature development of the nervous system, predisposing offspring to dependence on opiates, even in adulthood.
Cocaine use increases the risk of stillbirth, low-birth-weight, and birth defects; in utero exposure results in problems throughout childhood.
Alcohol passes through the placenta and poses risks for death of the fetus and neonate, malformations, and growth deficiencies.
Fetal Alcohol Spectrum Disorders include:
Fetal Alcohol Syndrome (FAS): Physical and psychological defects
Fetal Alcohol Effect (FAE)
Caffeine use has inconsistent findings, but some studies show an increased risk of miscarriage and low-birth-weight.
Cigarettes:
Nicotine and carbon monoxide pass through the placenta.
Nicotine stimulates the fetus.
Carbon monoxide is toxic and decreases oxygen to the fetus.
Smokers are more likely to deliver smaller babies and are more likely to have stillborn babies or babies die soon after birth.
Long-term effects include short attention spans, hyperactivity, lower cognitive scores, and poor grades.
Men who smoke are more likely to produce abnormal sperm.
effects of environmental hazards during pregnancy
Heavy metals (lead, mercury, cadmium, selenium, zinc) threaten the baby’s cognitive development.
PCBs are connected with smaller, less responsive babies; babies are more likely to develop cognitive deficits.
Radiation can cause defects in a number of organs (including eyes), the central nervous system, and skeleton, and increases the risk of intellectual disabilities.
maternal stress on the child
Maternal stress is linked to the secretion of stress hormones.
Adrenaline stimulates the mother’s heart and respiratory rates.
Corticosteroids decrease the growth of the placenta.
Extreme anxiety has been linked to low birth weight, prematurity, and miscarriage.