Robbins: Chapter 3 Inflammation and Repair
- %%What is Inflammation?%%
- inflammation is a protective response to damage or infection of vascularized tissue
- it triggers immune cells from the circulatory system to eliminate offending agents
- phagocytic leukocytes, antibodies, complement proteins
- %%What are the four cardinal signs of inflammation?%%
- redness
- swelling
- heat
- pain
- function ( later added)
- %%What are some causes for inflammation?%%
- infections
- tissue necrosis
- foreign bodies
- immune reaction (hypersensitivity)
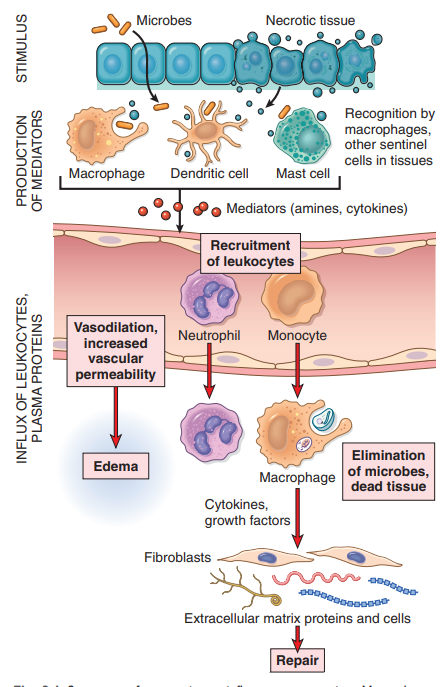
- %%Steps in inflammation?%%
- microbe enters body/ trauma
- Recognition the skin barrier is broken and macrophage, dendritic cells, and Mast cells
- cellular receptors for microbes → PAMPs(pathogen-associated molecular patterns)
- senores of cell damage → DAMPs( damage-associated molecular patterns)
- They recognize the microbe and trigger mediates amiens and cytokines) to recruit leukocytes
- cytokines → what to do!
- chemokines → where to go!
- Removal of stimulus Monocytes → macrophages and Granulocytes eliminate microbes.
- Repair of possible damaged tissue
- %%3 major components of acute inflammation?%%
- dilation of small vessels leading to an increase in blood flow
- increased permeability of the microvasculature, enabling plasma proteins and leukocytes from the circulation
- emigration of leukocytes from the microcirculation, their accumulation in the focus of injury, and their activation to eliminate the offending agent
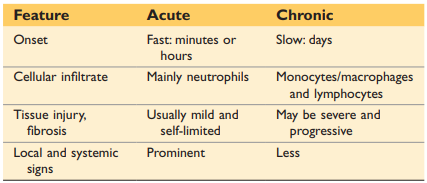
- %%Difference between acute and chronic inflammation?%%
- acute inflammation: is the initial rapid response (within minutes or hours) to eliminate offenders
- characteristic:
- vasodilation
- edema (increased vascular permeability)
- emigration of leucocytes( predominantly neutrophils)
- Chronic inflammation: is triggered when the initial response fails to clear the stimulus
- characteristics:
- longer duration
- more tissue destruction
- dominated by lymphocytes and macrophages
- more proliferation of blood vessels and fibrosis
- What is exudate and transudate? how is it related to acute inflammation?
- %%exudate%%: extravascular fluid that has high protein concentration and contains cellular debris → implies existence of inflammatory process
- in big amounts it is called pus
- %%transudate%%: fluid with low protein content with little to no cellular material → produced due to hydrostatic imbalance but not due to inflammation
- in big amounts called edema
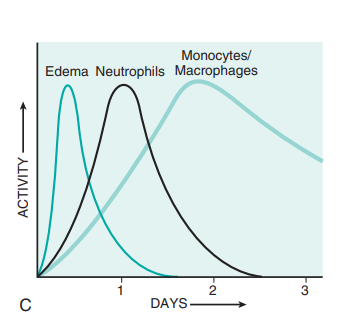
- %%what are changes in vascular flow in response to inflammation?%%
- increased blood flow → vasodilation → cause of heat and redness
- increased permeability: exudate of fluid into extravascular tissue
- loss of fluid → slower blood flow(stasis) + increased viscosity
- as stasis develops neutrophils accumulate along the vascular endothelium( more this in a later question)
- %%What is the multistep journey of leukocytes?%%
- (1) rolling → from center to endothelium walls with the help of selectins, which are the ligands found on leucocyte
- (2) integrin activation by chemokines
- (3) stable adhesion → integrins are the ligands found on leukocyte membrane that attach to the receptors on endothelial cells
- (4) migration through endothelium (diaphyses/transmigration)
- %%What are chemoattractants? And give some examples.%%
- Chemoatractes are produced by microbes and by host cells in response to n infections r tissue damage. They signal neutrophils and leukocytes towards which direction the inflammatory site is. First, neutrophils arrive to the site, but due to their short half-life, they are then replaced by Monocytes/Macrophages.
- examples:
- LTB4
- C5a
- IL-8
- %%What is key when terminating the inflammation and what are the associated steps?%%
- Phagocytosis and clearance of the offending agent
- (1) recognitions and attachment of the particle to be ingested by the leukocyte
- (2) engulfment, with subsequent formation of a phagocytic vacuole
- (3) killing or degradation of the ingested material with lysomome
- %%What is the function compliant system?%%
- it only destroys bacteria by drilling holes into the cell walls of the bacteria
- if this happens in normal healthy cell this causes major tissue damage
- %%What are the possible outcomes of acute inflammation ?%%
- complete resolution
- restoration of the site to normal tissue
- removal of cellular debris
- no edema
- healing by connective tissue replacement
- scarring or fibrosis
- Progression of the response to chronic inflammation
- How can you recognize inflamed tissue under a microscope?
- fluid-filled space → edema
- fibrinous exudate
- accumulation of granulocytes
- purulent inflammation → pus( dead granulocytes)
- ulcer → local tissue destruction
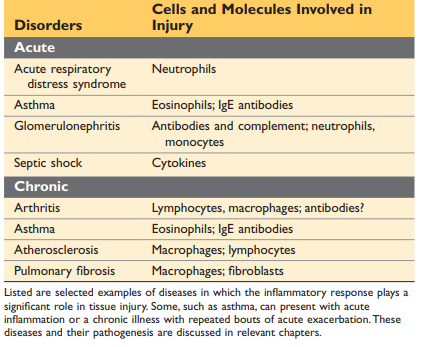
- Name different acute and chronic inflammatory diseases:
- What causes chronic inflammation?
- Immune-mediated inflammatory( hypersensitivity)
- autoimmune disease
- allergies
- Persistent or prolonged exposure to microbial infections by microorganisms that are difficult to eradicate
- Due to a delayed response immune reaction
- development if granulomatous inflammation
- walling of epithelial cells due to dead granulocytes
- What are two types of macrophage activation?
- what are systemic effects of inflation
- production of proteins: acute-pashe protein
- C-reactive protein (CRP) and serum amyloid A protein( SAA)
- Fever
- %%when does the repair of damage start?%%
- the work simoultainsly and can´t be seen as separate processes
- inflammatory vs anti
- autoimmune lymphocytes that recognize cells falsely
- autoinflammatory aggressive cells that just fire but it is not targeted
- each phase of the inflammatory response are associated with disease with the off switch of proteins is faulty
- What happens when microbo flora crosses the one cell layer that protects
- the first line of defense: innate immune → 99% of invasive microbes are depleted
- epithelium
- macrophages
- neutrophils
- adapt system is triggered by an innate system via chemokines( signaling molecules)
- b and t cells
- Tuberculosis is a bacterium that causes a chronic inflammatory response
- in crohns the histology looks similar because the body falsely reacts to microbes because the body confuses the two → genetic defects
- If you have impairment in innate response than their is a bigger/faster response of the auqired immune system to make up for the work
- lazy leukocyte syndrome
- leuity work slower ad, therefore, cause chronic inflammation because they fulfill they job to slow
- post-infectious autoimmune disease!!
- a microbe is recognized by t cell; however, after that the body confuses its own body causing chronic inflammation
- granuloma
- to prevent spreading through the body
- chronic granular disease
- Hermans putlock disease
- neutrophils love shortly
- regulatory t cell -→ controls immune response (dampens it)
- T-cell diseases → organ specific
- too many t cells or too little regulatory t cells
- repair and regeneration
- repair → with scaring
- regeneration → exact copy of what was damaged
- cholangiocytes: scar cells
- remodeling: differences in tissue in organs
- why repair and not regeneration
- repair is faster
- Kupfer cells are macrophages in liver
- what happens after liver failure?
- edema
- turn yellow
- very sensitive to toxins
- steps after cutting skin
- \
- clotting
- \
- epithelial cells
- \
- granulation tissue