GASTROINTESTINAL TRACT_2
GASTROINTESTINAL TRACT |
Beginning with the mouth and terminating with the anus “28 – 34 ft.” in length (840-1020 cm).
Radiologically important accessory organs of the digestive system are:
Salivary glands, Liver, Pancreas & GB
ACCESORY ORGANS
SALIVARY GLAND– secrete fluid for insalivation
LIVER – production of bile
PANCREAS – produces specialized digestive juices into the small intestine.
chyme – during gastric digestion
chyle – during intestinal digestion
milky fluid taken from the food during digestion
GALLBLADDER– storage for bile
ALIMENTARY CANAL
ORAL CAVITY
PHARYNX
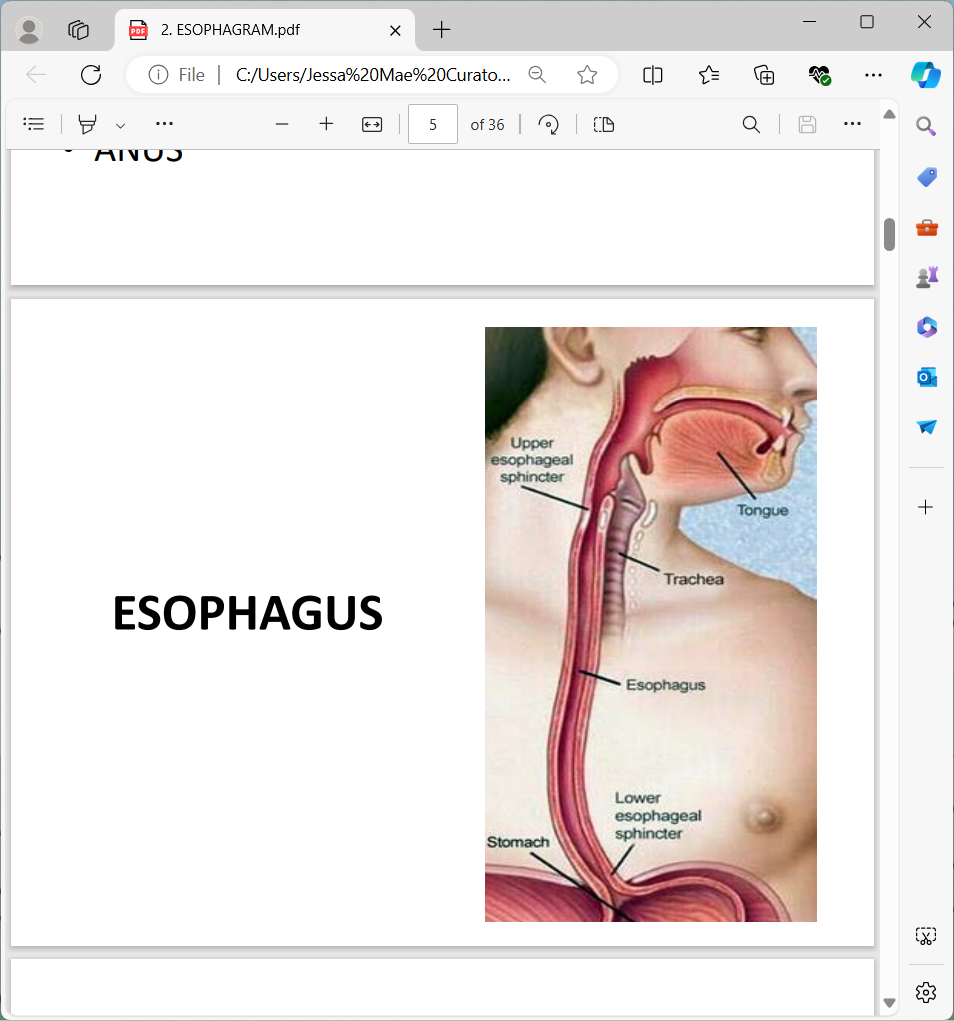
ESOPHAGUS
STOMACH
DUODENUM & SMALL INTESTINE
LARGE INTESTINE
ANUS
Esophagus
A muscular, collapsible tube located posterior of the larynx & trachea.
Serves as the connection between the pharynx and stomach and is approximately 22.5 – 27.5 cm in length. 2cm in diameter
25cm> Bontrager
Esophagram
Radiographic study of esophagus from pharynx down to the junction of the stomach with the used of positive and negative contrast media.
Contrast to be used
Single contrast
30 – 50 % weight / volume suspension
Double contrast (for w/ UGIS)
low-viscosity, high density barium
Note: whatever the weight/volume concentration of barium, the most important, it must flow sufficiently to coat the walls of esophagus.
4 normal esophageal constriction
AORTIC ARCH
LEFT MAIN BRONCHUS
HEART (LEFT VENTRICLE)
DIAPHRAGM
CLINICAL INDICATIONS
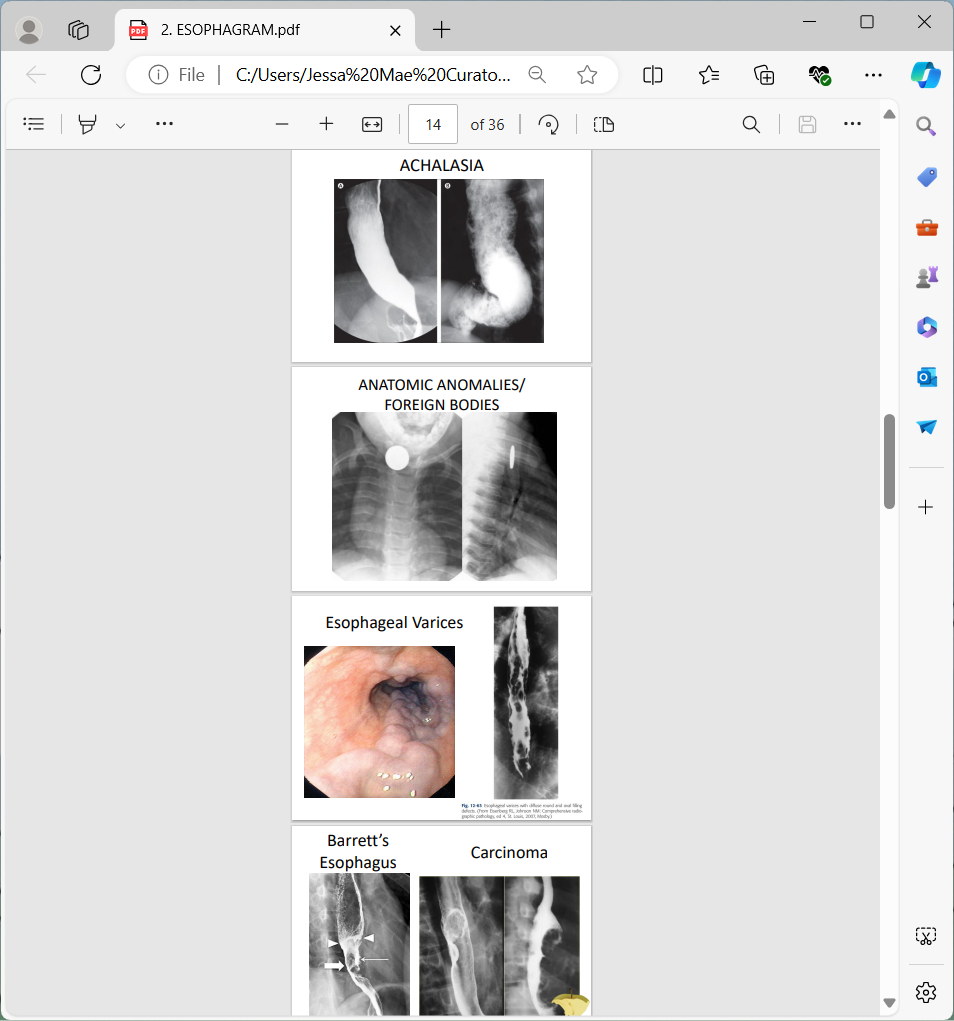
• ACHALASIA(CARDIOSPASM)
• ANATOMIC ANOMALIES
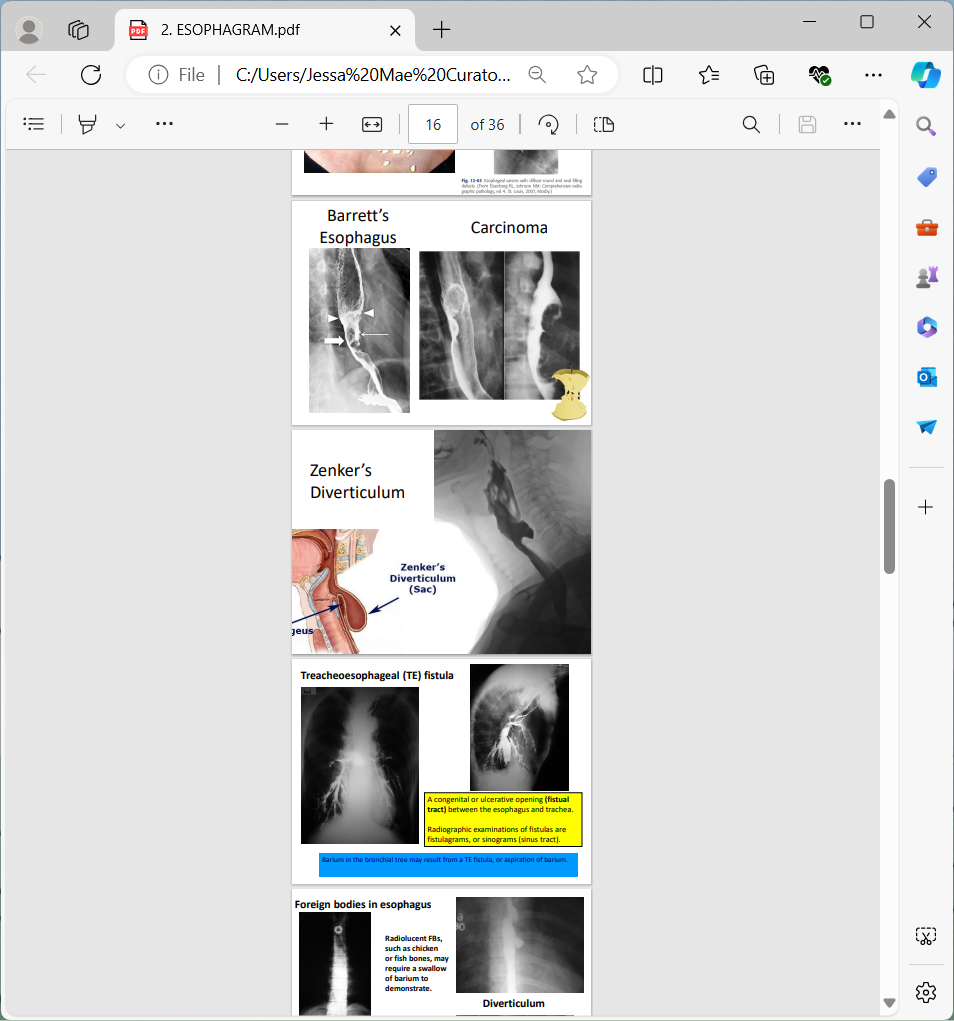
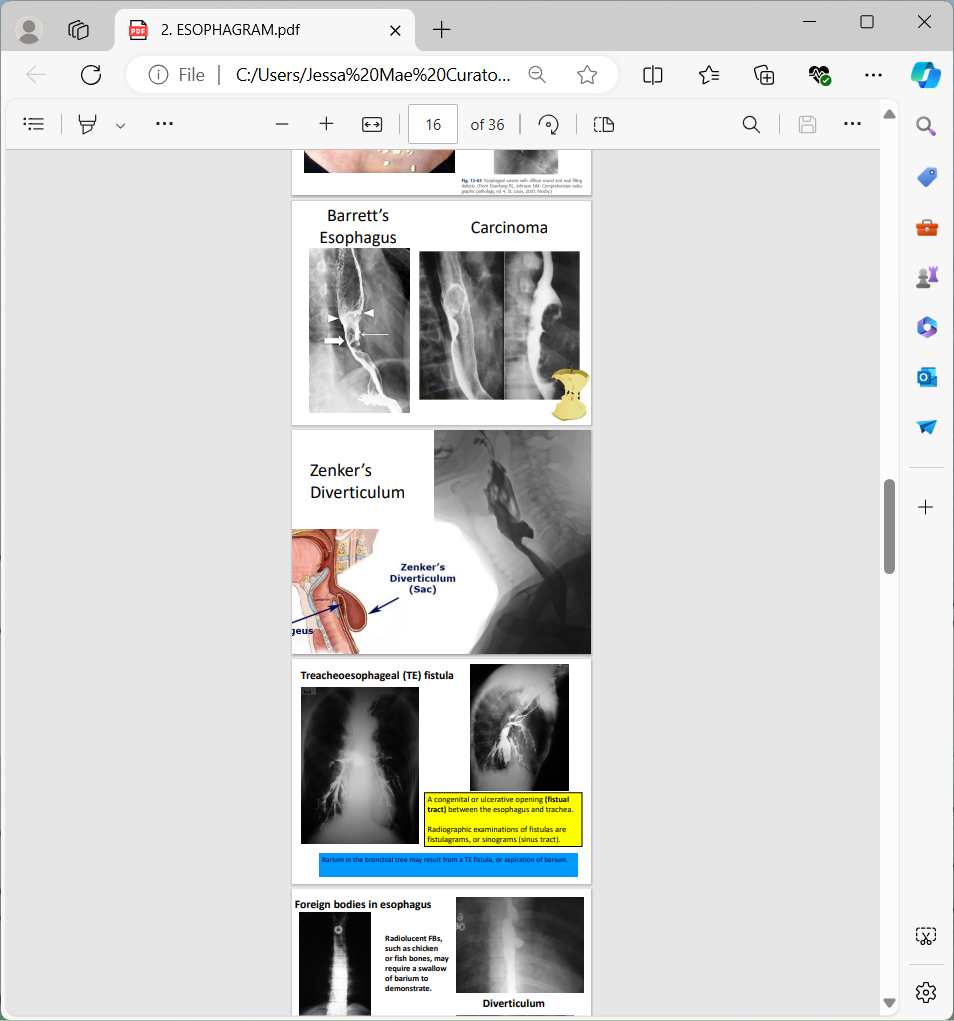
• BARRETT'S ESOPHAGUS
• CARCINOMA
• DYSPHAGIA
• ESOPHAGEAL VARICES
• FOREIGN BODIES
• GERD (Gastroesophageal Reflux disease)
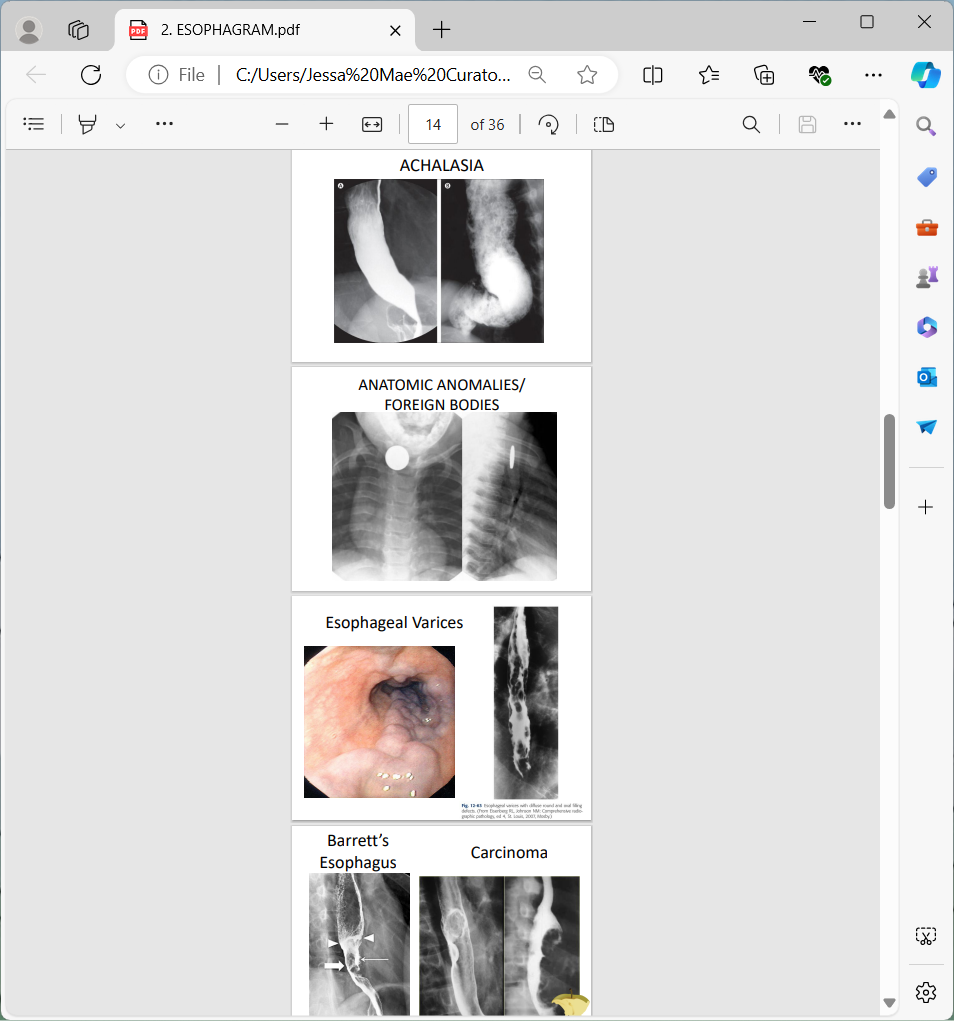
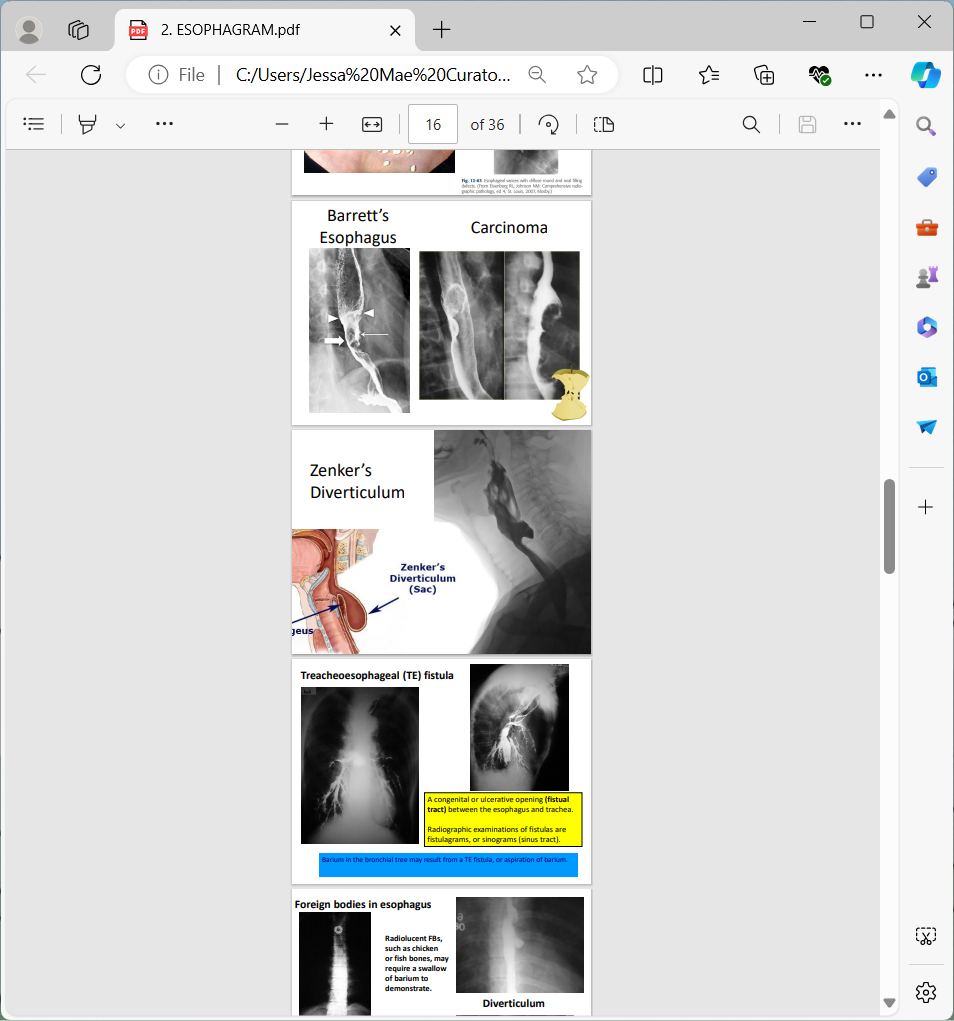
Treacheoesophageal (TE) fistula
A congenital or ulcerative opening (fistual tract) between the esophagus and trachea.
Radiographic examinations of fistulas are fistulagrams, or sinograms (sinus tract).
Barium in the bronchial tree may result from a TE fistula, or aspiration of barium.
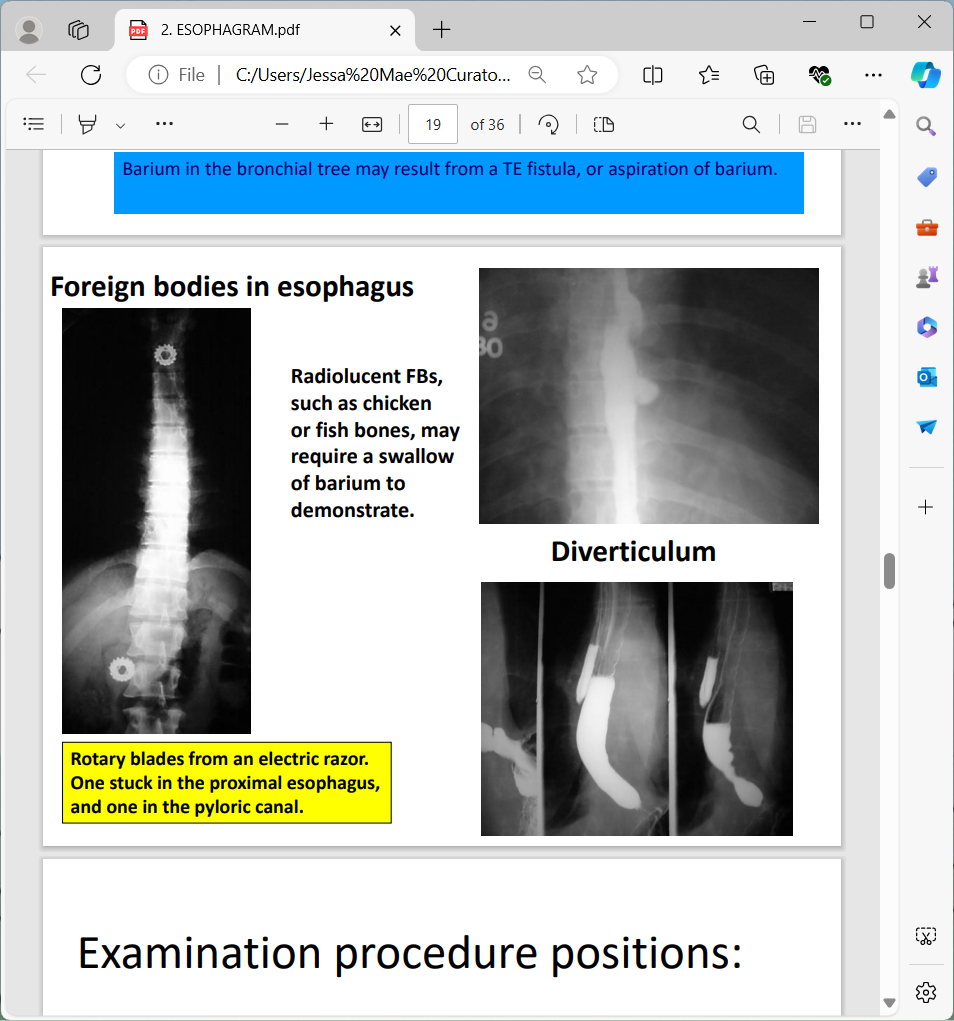
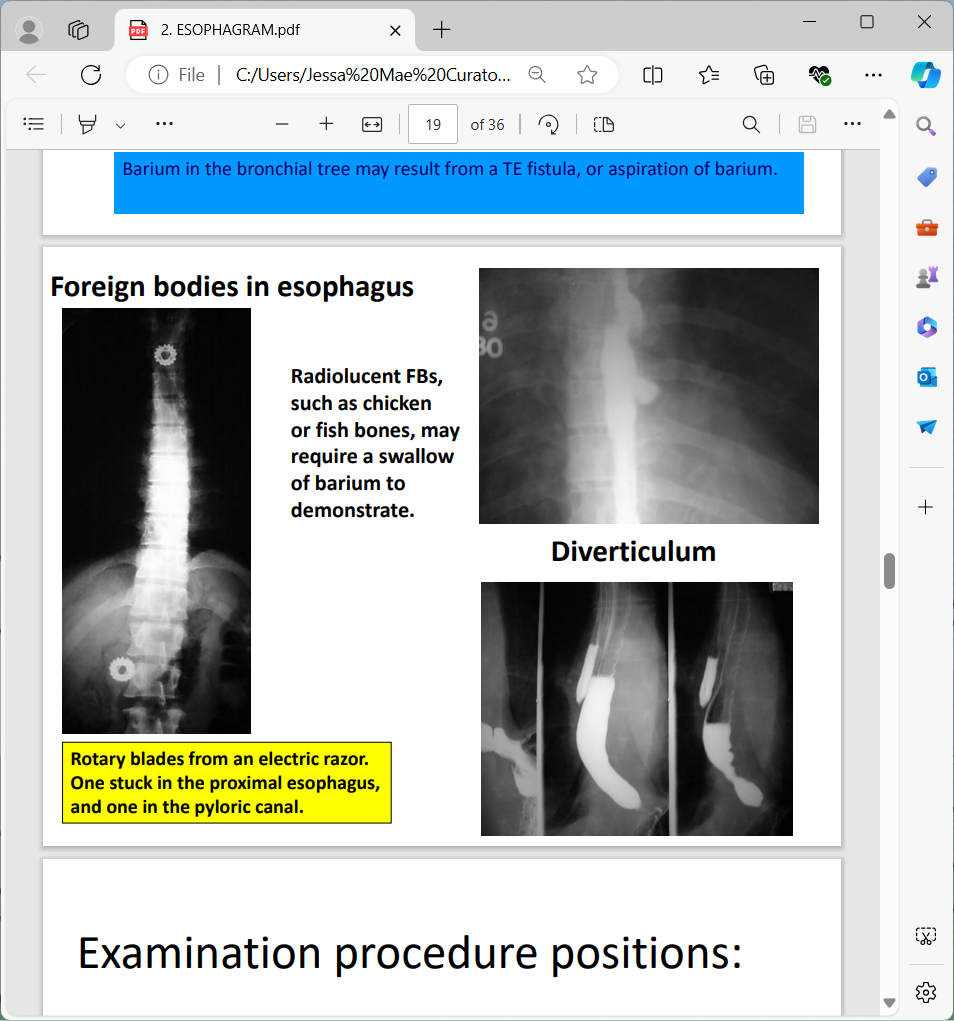
Foreign bodies in esophagus
Radiolucent FBs, such as chicken or fish bones, may require a swallow of barium to demonstrate.
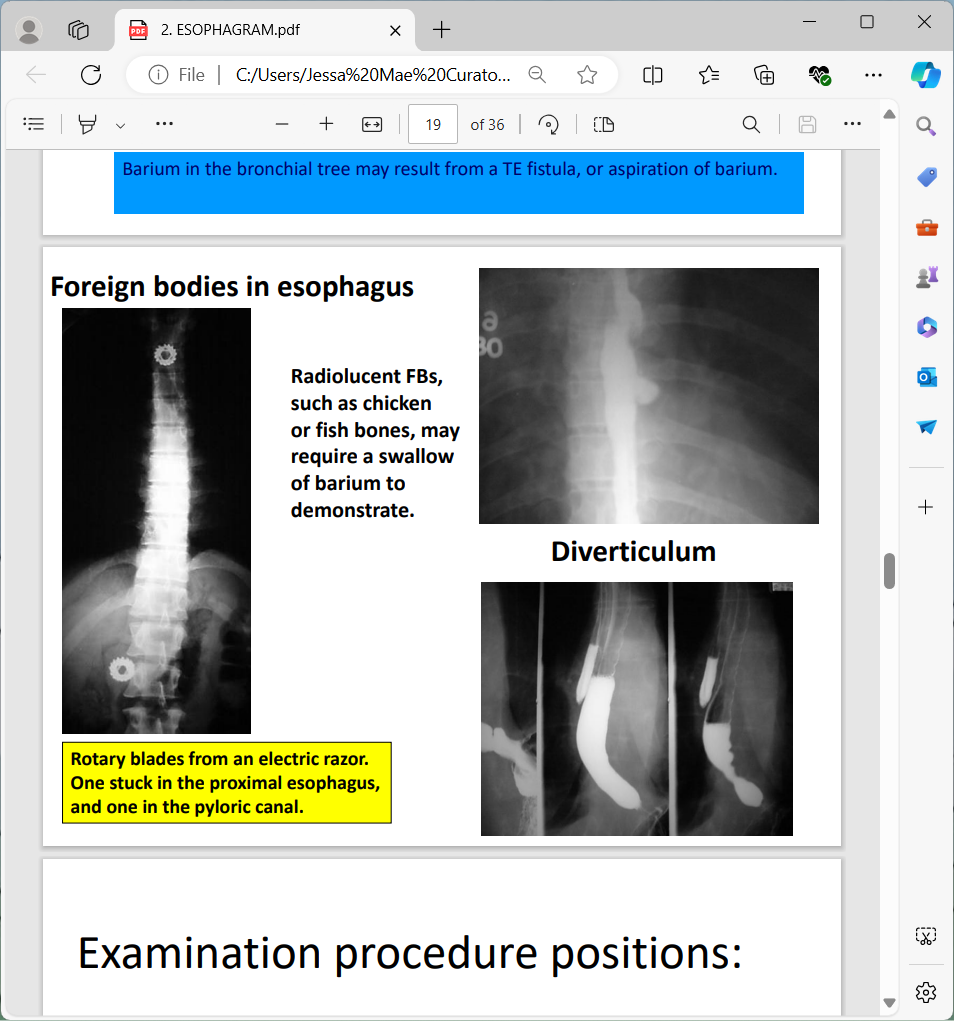
Rotary blades from an electric razor. One stuck in the proximal esophagus, and one in the pyloric canal.
DIVERTICULUM
Examination procedure positions:
upright position whenever possible.
AP/PA projection, Oblique and lateral positions
Examinations of the esophagus
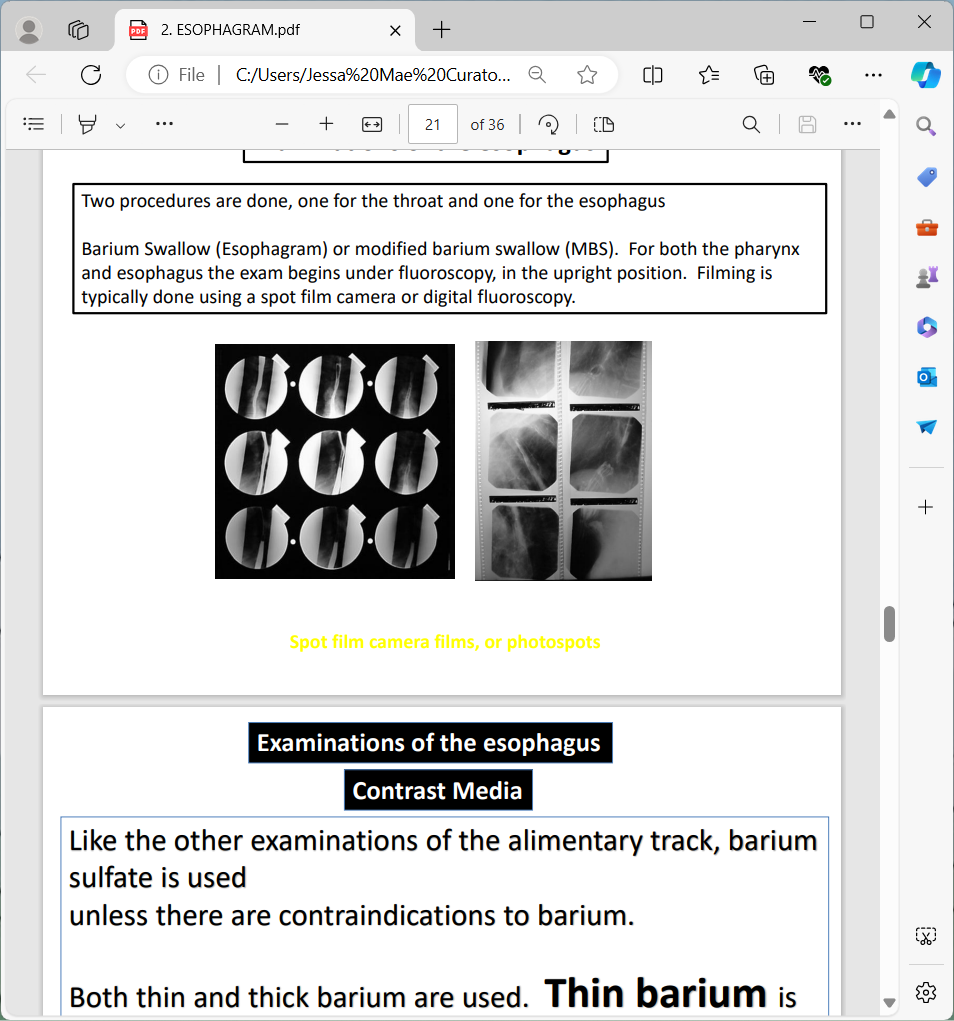
Two procedures are done, one for the throat and one for the esophagus
Barium Swallow (Esophagram) or modified barium swallow (MBS). For both the pharynx and esophagus the exam begins under fluoroscopy, in the upright position. Filming is typically done using a spot film camera or digital fluoroscopy
Examinations of the esophagus
Contrast Media
Like the other examinations of the alimentary track, barium sulfate is used unless there are contraindications to barium.
Both thin and thick barium are used.
Thin barium is useful to outline the esophagus quickly. When administered in the upright position is empties into the stomach in seconds.
Thick barium (barium paste) is mixed with one part water to 3-4 parts barium powder. Commercial products are often packaged in a tube.
Thick barium coats and adheres to the mucosa. It may be mixed with cotton balls, marshmallows, or other foods.
No patient preparation is need for an esophagram, unless it is to be followed by an UGI
Esophagrams begin under fluoroscopy, in the upright position. The patient holds a cup of barium, with a straw, in the right hand. The radiologist instructs the patient to patient to drink, and films in the AP, RPO, and LPO positions.
The patient is often put into an RAO before the table to lowered to horizontal. The examination continues in the recumbent position.
Overhead films are taken per the radiologist’s routine.
A large diameter straw is needed, and care must be taken that the end of the straw does not become vacuum sealed to the bottom of the cup.
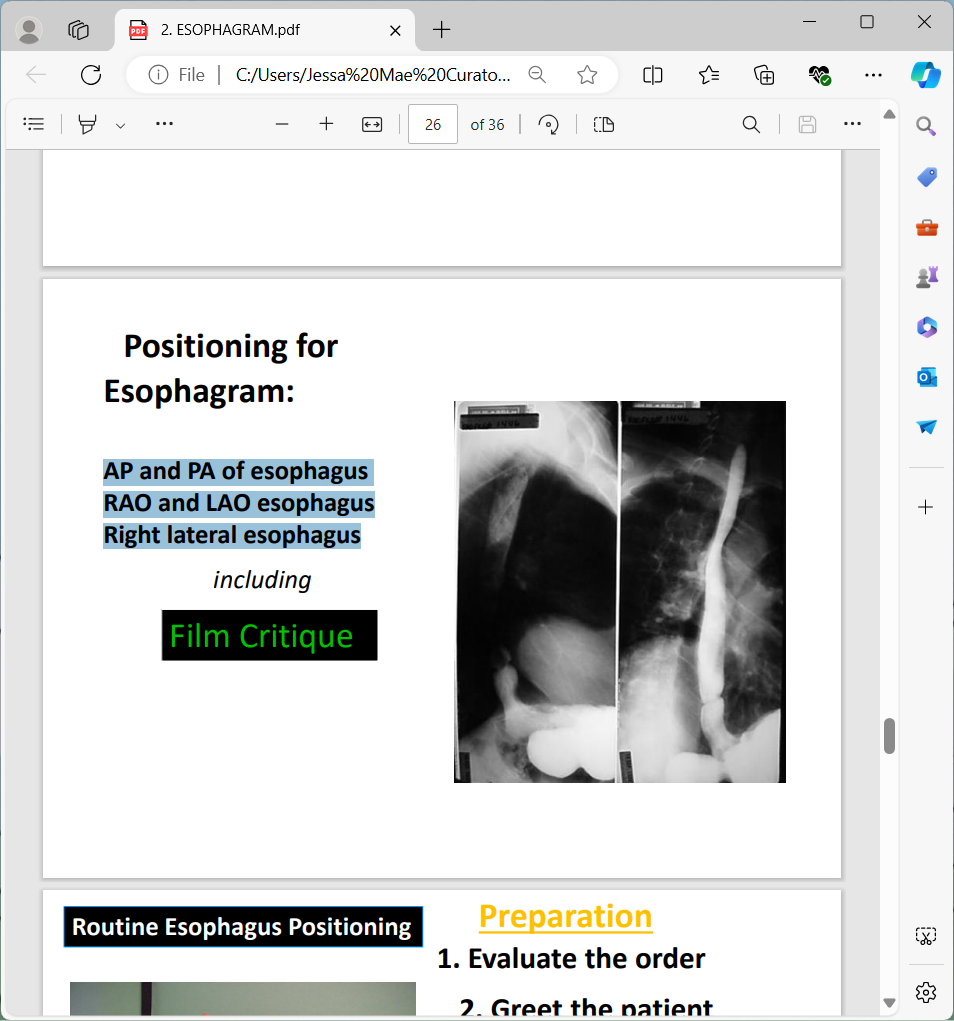
Positioning for Esophagram:
AP and PA of esophagus RAO and LAO esophagus Right lateral esophagus Film Critique
Routine Esophagus Positioning
Preparation
Evaluate the order
Greet the patient
Take History
What is pertinent Hx?
chest pain, heartburn, dysphagia (difficulty swallowing), odynophagia (pain on swallowing)
Remove jewelry, check attire, snaps, pins, NG tubes, etc.
Explain the exam in layman’s terms
Questions?
Set technique before positioning
Routine AP, PA Positioning
Steps
Pathology demonstrated: Strictures, foreign bodies, anatomic anomalies and neoplasm
14” x 17” lengthwise (7” x 17” are also used)
Shielding: place lead shield over pelvic region (gonadal)
Central Ray:
CR perpendicular to IR
CR MSP, 1inch inferior to sternal angle (T5-T6)
40 SID> Table
72SID> Upright
Part Position:
Align MSP to Midline of IR
Right arm up to hold cup
IR 2 inches above the houlder to place CR Center to IR
Use of thick barium, 1 part and 3 spoon fools
Structure shown:
Entire esophagus filled with barium
Critique criteria for frontal projections of the esophagus
Entire esophagus filled with barium, in an unrotated frontal projection.
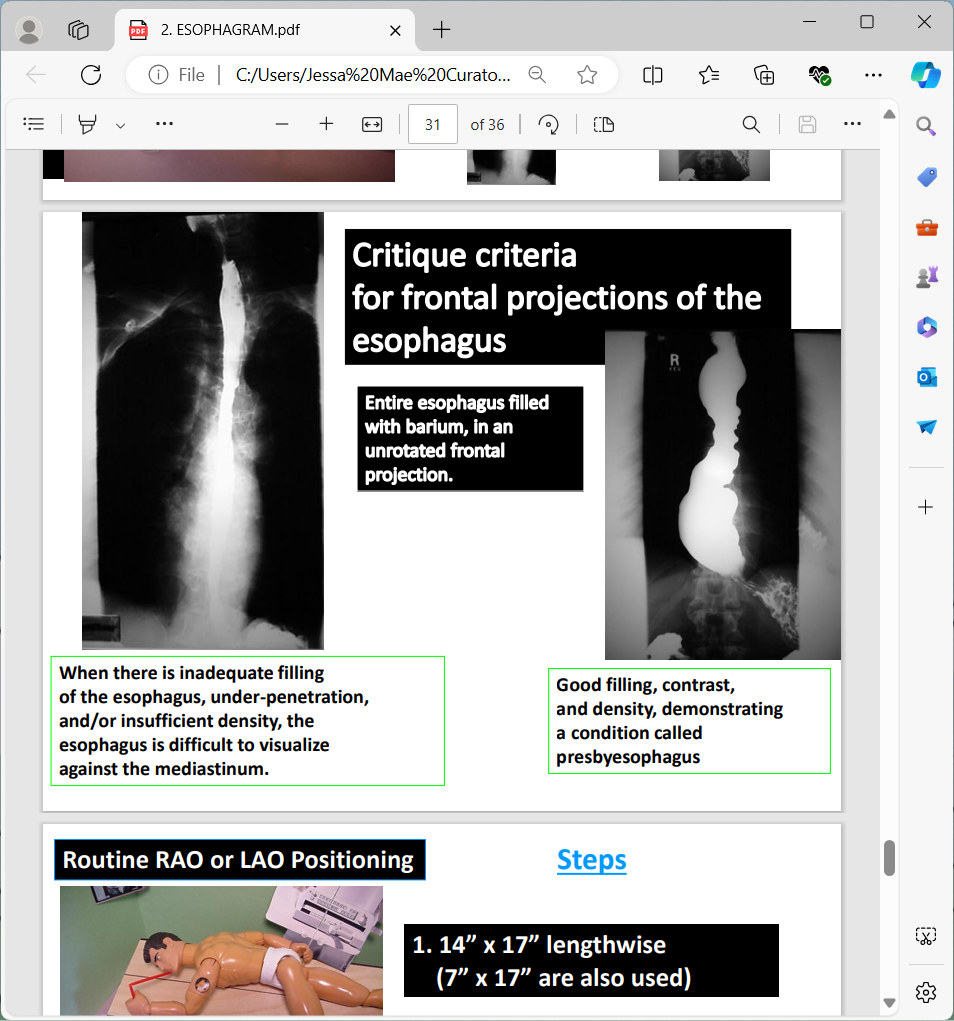
When there is inadequate filling of the esophagus, under -penetration, and/or insufficient density, the esophagus is difficult to visualize against the mediastinum.
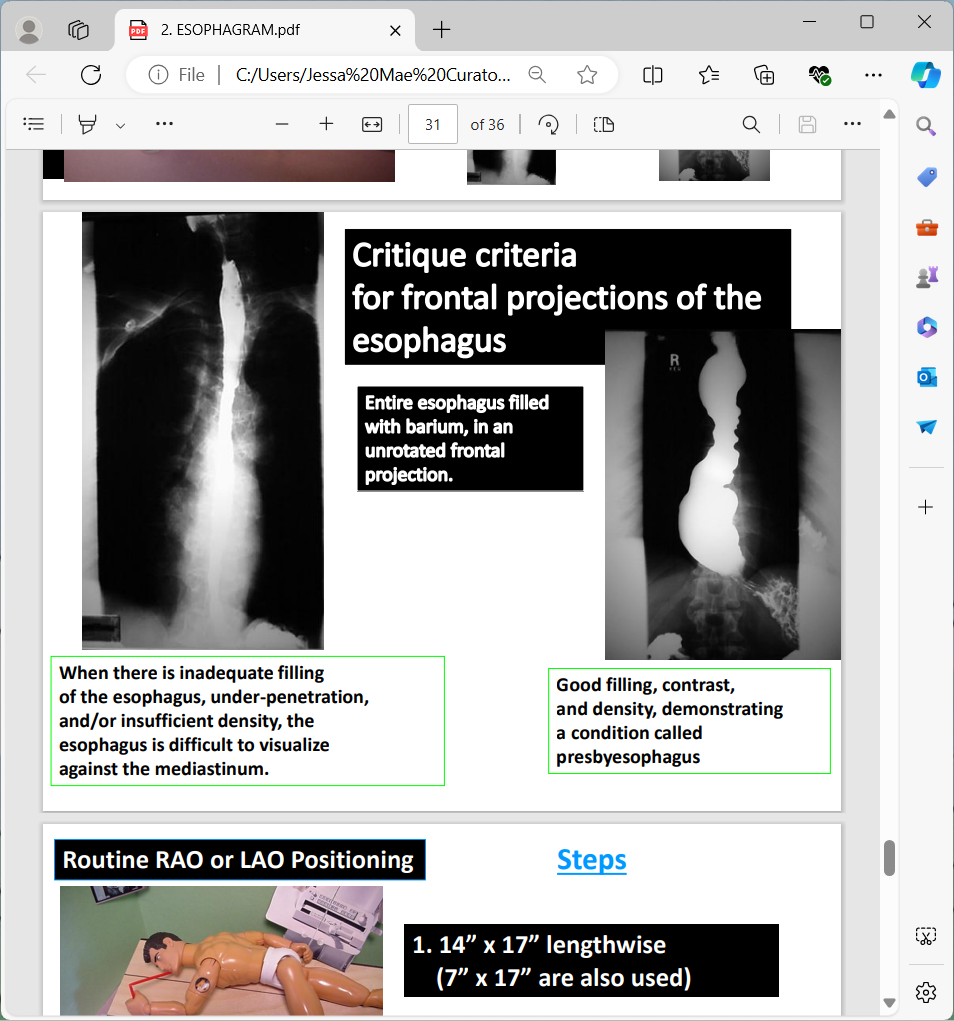
Good filling, contrast, and density, demonstrating a condition called presbyesophagus
Routine RAO or LAO Positioning
Steps
14” x 17” lengthwise (7” x 17” are also used)
50 -450 RAO position. (Spine must be as straight as possible, especially with tight collimation.)
CR to T5-6 (Top of film 2” above shoulders), several inches left of the spinous processes.
Critique criteria for RAO & LAO esophagus
Like the RAO stomach, which is the single best projection, the RAO is also best for the esophagus.
The heart provides a homogeneous background to contrast it against, and the distal esophagus, traversing the esophageal hiatus, is laid out in profile.
The RAO should demonstrate the entire barium filled esophagus.
The abdominal portion is more important than the pharyngeal portion, which may be evaluated by direct inspection.
Critique criteria for LAO esophagus
The LAO may provide valuable diagnostic information, but contrasts the esophagus against the hilar area of the right lung and foreshortens the abdominal esophagus at the gastroesophageal junction.
The RAO & LAO should both demonstrate the entire barium filled esophagus.
The abdominal portion is more important than the pharyngeal portion, which may be evaluated by direct inspection.
Routine Right lateral Positioning
Steps
14” x 17” lengthwise (7” x 17” are also used)
Right lateral. C-spine “coextensive” to T-spine.
CR to T5-T6 (Top of film 2”above shoulders) in the midcoronal plane.
The arms may be raised and superimposed (like a lateral chest position), or the left shoulder may be rotated posteriorly for a “swimmers lateral.”
Critique criteria for lateral esophagus
Entire barium filled esophagus projected posterior to heart, and anterior to the T -spine