HEALTH ASSESSMENT MIDTERM
Intro to HA
- Assessing = determine health problems and care needs of patient
- More precise = better outcomes
Precise vs Accurate
Accuracy
- measures how close results are to the true or known value.
Precision
- measures how close results are to one another
Purpose of the Assessment
- To collect data pertinent to the patient’s health status (Subjective/Objective)
- To identify deviations from normal
- To discover the patient’s strengths, limitations and coping resources
- To identify the actual problem
- To build rapport with a patient and his/her family.
Purpose of HEALTH ASSESSMENT
- To obtain baseline data about the client’s functional abilities.
- To supplement, confirm or refute data obtained in nursing history.
- To obtain data that will help establish nursing diagnoses and plan of care.
- To evaluate the physiological outcome of health care and the progress of the client’s health problem.
- To make clinical judgment about a client’s health status.
- To identify areas for health promotion and disease prevention.
Skills Required (CPPAE)
- Cognitive Skills
- Assessment is a “thinking” process
- Critical thinking
- Why? How? What? When?
- Critical decision-making
- Use knowledge and experience
- Problem Solving Skills
- With scientific methods
- Experience
- “Intuition” with experience
- Psychomotor skills
- Assessment is “doing”
- Skills involve physical movements and coordination, which are essential for performing tasks such as administering medication, performing physical assessments, and providing patient care
- Affective /Interpersonal Skills
- Assessment is “feeling” trust and mutual respect
- Ethical skills
- Assessment is “being responsible and accountable for your practice”
Four Types of Assessment (IFTE)
- Initial assessment
- Triage
- Aids in determining the nature of the problem and lays foundation for the subsequent stages of evaluation
- Done within specified time after admission to Hospital
- Examples:
- Obtain patients medical history
- Performing a physical exam
- Preparing a psychosocial assessment for a mental health patient.
- Focused assessment
- The problem is exposed and treated during the focused assessment step.
- Purpose;
- To determine the status of a specific problem identified in the earlier assessment & identify new or overlooked problems.
- Eg. Hrly fluid intake output assessment
- To determine the status of a specific problem identified in the earlier assessment & identify new or overlooked problems.
- Objectives;
- Diagnose
- Treat
- Examples:
- Vital signs
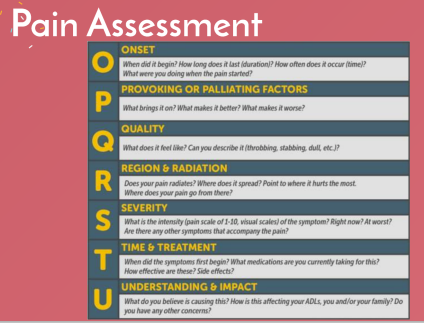
- Initial pain assessment.
- Examples:
- Time-Lapsed Assessment
- It may last one or two hours or several months, depending on the severity of the disease.
- The present status of the patient is compared to the previous baseline during and prior to therapy.
- It may includes:
- Blood tests
- X-ray
- Other diagnostic medical tests.
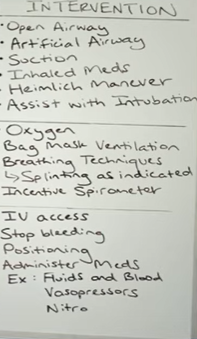
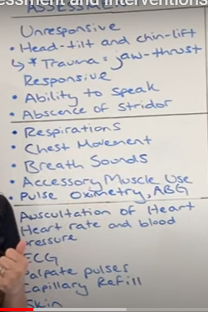
- Emergency Assessment (BLS)
- Identifying the patient’s core reasons of concern and monitoring the patient’s airway, breathing and circulation (ABCs)
- May become an initial or focused assessment once the ABCs have been stabilized
- (start with checking circulation if there is bleeding)
Methods of Assessment (OIE)
- Observation
- Systematic collection of data from persons who are getting care in order to inform clinical decision-making
- Entails taking a person-centered approach to actively connect with patients, their families and nurses
- Aims to build rapport while also assisting with assessment.
- 4 senses: vision, hearing, smell and touch
- Interview
- Also known as the history, serves as the starting point for all other aspects of the nursing process.
- Structured in a way that the nurse gains understanding of the patient adaptive process.
- A planned communication or a conversation with a puepose with two approaches;
- Directive
- Focused on leading clients to a solution
- Non directive
- Encourage clients to talk and open up
- Directive
- Factors
- Physical setting
- Nurse's behavior
- Type of questions asked
- How questions are asked
- Personality and behavior of patients
- How patient is feeling at the time of interview
- Nature of information being discussed or problem being confronted
- Health History
- It is the collection of subjective data that includes information on both the patient's past and present health status.
- It allows positive aspects of health problems, health teaching needs, and health concerns to be identified.
- Personal Profile
- Chief complaint or present illness
- Past Health History
- Current medication
- Personal habits and patterns of living
- Psychosocial history- Mental status Children and Adolescent
.
- Examination
- Four procedures; IPPA
- Inspection
- Palpation
- Percussion
- Auscultation
- Abdominal examination; IAPP
- Inspection
- Auscultation
- Percussion
- Palpation
- Signs
- Effect of a health problem that can be observe by someone else
- Any changes that can be physically observe
- Signs refer to the objective data (overt) and are based on what the nurses sees.
- Four procedures; IPPA
- OBJECTIVE DATA
- Observable and measurable data
- Collection of data through observation, physical examination, laboratory and diagnostic testing.
- By gathering of information using senses of seeing hearing, smelling and touching.
- Symptoms
- Subjective evidence of disease
- Only the patient can verbalize his/her feelings
- Refer to subjective data (covert) and based on what paients say.
- Symptoms
- SUBJECTIVE DATA
- The best source for finding out how someone is feeling from the person itself.
- Personal verbalization of the patient
- Includes information that the patient provides.
Acute vs Chronic
ACUTE
- Minutes - 3 months up to 6 moths
- Acute pain associated with a soft-tissue injury or brief illness. Usually goes away after the damage or illness recovers.
- If an injury does not heal properly or if the pain signals fail, acute pain can turn into chronic pain
CHRONIC
- CHRONIC illness lasts for months, usually more than 3
- Might be continuous or intermittent
- Persistent pain is pain that carries on for longer than 12 weeks despite medication or treatment.
Physical Assessment Techniques
INSPECTION
- Examine each body system for normal and abnormal conditions using vision, smell and hearing
- As the nurse analyzes each body system, look for color, size, position, movement, texture, symmetry, scents, and sounds.
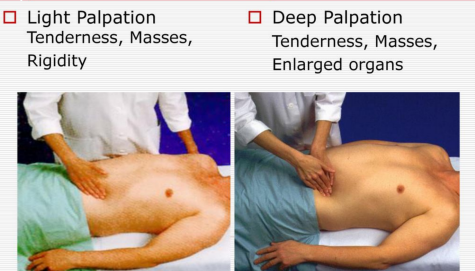
PALPATION
- Utilize different portions of your hands to touch the patient with varying degrees of pressure
- Keep your fingernails short and your hands warm
- Wear gloves- when palpating mucosal membranes or bodily fluids
- LIGHT PALPATION
- To feel for surface abnormalities
- Depress the skin ½ to ¾ (about 1-2 cm) with your finger pads, lightest touch possible.
- Assess for texture, tenderness, temperature, moisture, elasticity, pulsations, and masses.
- DEEP PALPATION
- To feel internal organs and masses for size shape, tendernes, symmetry and mobility
- Depress the skin 1 ½ to 2 inches (about 4 to 5 cm) with firm, deep pressure
- Use one hand on top of the other to exert firmer pressure, if needed.
PERCUSSION
- Tap your fingers or hands against sections of the patient's body fast and sharply
- To discover organ borders, idenify organ shape and position, and if an organ is solid, fluid-filled or gas-filled
- DIRECT PERCUSSION
- Reveal tenderness
- One or two fingers
- Tap directly
- Ask the patient to tell you which are are painful, and watch his face for signs of discomfort.
- INDIRECT PERCUSSION
- To elicit sounds that gives clues what makeup is in the underlaying issue.
- Press the distal part of the middle finger of your non-dominant hand firmly on the body part.
- Keep the rest of your hands off the body surface.
- Flex the wrist with your non-dominant hand
- Listen to the sound produced.

AUSCULTATION
- Listening for lung, heart, and bowel sounds using stethoscope
- Area is expose
Assessment process
- Collecting Data
- Primary source
- Patient - alert, oriented patient is most reliable source
- Secondary source
- Family members, significant others, medical records and diagnostic procedure.
- Subjective data
- Symptoms (covert) verbal ststement by the patient
- Ex. nausea, pain, fatigue, itching
- Objective data
- Signs (Overt)
- Can be seen, felt, heard, smell- information by observation or examination.
- Ex. discoloration skin, warm to touch, swollen part of the body.
- Ex. discoloration skin, warm to touch, swollen part of the body.
- Primary source
Factors
- Genuineness: open, sincere
- Respect: no judgment
- Empathy: acknowledge
Organizing data
- Written or computerized format to organize assessment data
- Cluster data into groups of info Format may modify acc. To Px physical status
Validating data
- Double checking or verifying to check if accurate and factual
- Ensures that assessment information is complete Objective and subjective data agree
Documenting Data
- Accurate documentation is essential
- Record in factual (no interpretation) -
- Appropriate documentation = excellent care by accurate reflecting nursing evaluation
OVERVIEW OF NURSING PROCESS
- Systematic, organized method of planning, and providing quality and individualized nursing care.
- Synonymous with problem-solving approach
GOSH Approach
- G- GOAL ORIENTED
- O- ORGANIZED
- S- SYSTEMATIC
- H- HUMANISTIC CARE
Effective Nurse
- Being able to assess and check that the patient is actually suffering from a fever.
Efficient Nurse
- Being able to help the patient improve from one status to another through nursing interventions.
Purposes
- To identify a client’s health status
- The actual/present and potential/possible problems or needs.
- Establish a Plan of care to meet identified needs.
- Provide nursing interventions to meet those needs.
- Provide an individualized, holistic, effective and efficient nursing care
Characteristic of the Nursing Process
- Dynamic and cyclic
- Patient-centered
- Goal directed
- Flexible
- Problem-oriented
- Cognitive
- Action-oriented
- Interpersonal
- Holistic
- Systematic
The Nursing Process
- ASSESSMENT
- Collecting subjective and objective data
- Most critical phase
- Is still ongoing and continuous throughout all phases of the nursing process
- More than gathering information
- It is analyzing and synthesizing that data, making judgements abut the effectiveness of nursing interventions and evaluations client care.
- Systematic collection of data
- Most important step
- Sets the tone and the rest of the process from it.
- Diagnosis
- Analysis of data to identify the problem
- Involves identifying and prioritizing actual or potential health problems or responses
- Actual nursing diagnosis, occurring health problems for the patient
- Potential nursing diagnoses, high risk health problem
- Possible is that it needs further data to support it.
Types of nursing diagnosis
- Problem-focused
- A clinical judgement concerning an undesirable human response to a health condition
- Ex.
- Acute pain related to trauma of surgical incision as evidenced by facial grimace and guarding behavior.
- Risk
- A clinical judgment concerning the susceptibility of an individual for developing an undesirable human response to health conditions/ life processes.
- Ex.
- Risk for infection related to surgical incision
- Health promotion
- A clinical judgment concerning motivation and desire to increase well-being and to actualize health potential.
- Syndrome
- A clinical judgment concerning a specific cluster of nursing diagnoses that occur together and is therefore best addressed through similar interventions
- PLANNING
- Determining outcome criteria and developing a plan
- Involves setting goals and outcome
- Goals
- Broad statement that describes a desired change in a patient’s condition, perceptions or behavior.
- Types of goals
- Long term goals
- Objective behaviors
- Response or behavior expected a patient to achieved over Longer period
- Short term goals
- Objective behavior
- Achieve in short time
- Long term goals
- Goals
- INTERVENTION
- Always write rationale (explain why nursing interventions were made)
- APPROACH
- Direct care
- Direct interventions
- Example: medication administration, vital signs, checking etc.
- Direct care
- Indirect care
- Performed a way form a patient but behalf of the patient or group of patient
- Example:
- Safety and infection control, delegating nursing care
- Tyoes
- Independent
- initiate s without supervision
- Dependent
- Order from health care provider.
- Collaborative
- Interdependent interventions
- Independent
- EVALUATION
- Outcome criteria have been and revising the plan as apology
Guidelines for Documentation
- Clear, accurate and accessible documentation is essential element of safe, quality, evidence-based nursing practice
- critical for nurses
Uses of nursing documentation
- Communication with the Health care Team
- Nurses aim to share information about patients and organizational functions that is:
- Accurate
- Timely
- Contemporaneous
- Concise
- Thorough
- Organized
- Confidential
- Nurses aim to share information about patients and organizational functions that is:
Electronic Health Record (EHR)
- Provides an integrated, real-time method of informing the health care team about the px status
- Timely documentation of information should be made and maintained in a patient’s EHR
- To ensure informed decisions and high quality care in the continuity of patient care.
Types of Information
- Assessment
- Clinical problems
- Communication with other health care professionals regarding the patient
- Communication with and education of the patient, family and the patient’s designated support person and other third parties.
- Medication records (MAR)
- Order acknowledgement, implementation and management
- Patient clinical parameters
- Patient responses and outcomes, including changes in the patient’s status
- Plans of care that reflect the social and cultural framework of the patient.
Communication with Other Professionals
- Credentialing
- To monitor performance of health care practitioners and the health care facility’s compliance with standards governing the profession and provision of health care
- Legal
- Documentation that is incomplete, inaccurate, untimely, illegible or inaccessible, or that is false and misleading
- Interfere with legal fact finding
- Jeopardizing the legal rights, claims and defenses of both patients and health care providers
- Putting health care organizations and providers at risks of liability
- Documentation that is incomplete, inaccurate, untimely, illegible or inaccessible, or that is false and misleading
- Regulation and legislation
- Audits of reports and clinical documentation provide the following:
- Method to evaluate and improve the quality of patient care
- Maintain current standards of care
- Provide evaluative evidence when standards require modification in order to achieve the goals, legislative mandates or address quality initiatives.
- Audits of reports and clinical documentation provide the following:
- Reimbursement
- Documentation is utilized to
- Determine the severity of illness
- The intensity of services
- The quality of care provided
- Documentation is utilized to
- Research
- Data from documentation with the patients characteristics and care outcomes
- Evaluation and analysis are essential for attaining the goals of evidence-based practice in nursing and quality health care
- Quality process and Performance Improvement
- Documentation is the primary source of evidence used to continously measure performance outcomes against predetermined standards
- Used to analyze variance from established guideline, measure, improve processes, and performance related to patient care
Nursing Documentation Principle
- Principle 1: Documentation characteristics
- Accessible
- accurate , relevant and consistent
- Auditable
- Clear, concise, and complete
- Thoughtful
- Timely, contemporaneous and sequential
- Reflective of the nursing process
- Retrievable on a permanent basis in a nursing-specific manner
- Principle 2: Education and Training
- Functional and skillful use of the global documentation system
- Competence in the use of the computer and its supporting hardware
- Proficiency in the use of the software system
- Principle 3: Policies and Procedures
- The nurse must be familiar with all organizational policies and procedures
- Policies and procedures on maintaining efficiency in the use of the “downtime” system for documentation when the available electronic system does not function.
- Principle 4: Protection Systems
- Security of Data
- Protection of patient identification
- Confidentiality of patient information
- Confidentiality of clinical professional information
- Principle 5: Documentation Entries
- Accurate, valid, and complete
- Authenticated: the information is truthful, the author is identified, and nothing has been added or inserted
- Dated and time-stamped by the persons who created the entry
- Legible/readable
- Made using standardized terminology, including acronyms and symbols.
- Principle 6: Standardized terminologies
- Terminologies should include the terms that are used to describe the planning, delivery and evaluation of the nursing care of the patient or client in diverse settings.
Guidelines:
- Use of the following modalities according to physician preference, if known. Wait no longer than 5 minus between attempts
- Messenger application (if known)
- Physicians call service
- During weekdays, the physician's office directly
- On weekends and after hours during the week, the physician’s mobile phone
- Mobile phone
- Prior to calling the physician, follow these steps:
- Have I seen and assessed the patient myself before calling?
- Has the situation been discussed with a resource nurse or preceptor?
- Review the chart for the appropriate physician to call.
- Know the admitting diagnosis and date of admission.
- Have I read the most recent MD progress notes and notes from the nurse who worked the shift ahead of me.
- Have the available the following when speaking with the physician:
- Patient’s chart
- List of current medications, allergies, IV fluids, and labs
- Most recent vital signs
- Reporting lab results: provide the date and time
- Test was done and results of previous tests for comparison
- Code status
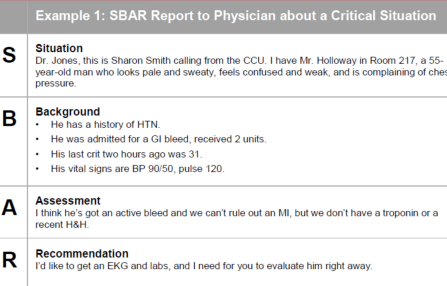
SBAR
- Situation
- What is the situation you are calling about
- Identity self . unit, patient’s full name, room number
- Briefly state the problem, what is it, when it happened or started, and how severe.
- What is the situation you are calling about
- Background
- Pertinent Background information related to the situation could include the following:
- The admitting diagnosis and date of admission
- List of current medications, allergies, IV fluids and labs.
- Most recent vital signs
- Lab results: provide the date and time test was done and results of previous tests for comparisons
- Other clinical information
- Code status
- Pertinent Background information related to the situation could include the following:
- Assessment
- What’s the nurse’s assessment of the situation
- Recommendation
- What is the nurse’s recommendation or what does he/she want?
- Examples;
- Notification that patient has been admitted
- Patient needs to be see now
- Order change
FDAR (focus, data, action, response)
- Guidelines:
- Focus charting must be evident at least once every shift
- Focus charting must be patient-oriented not nursing task-oriented
- Indicate the date and time of entry in the first column.
- Separate the topics words for the body of notes:
- Focus note written on the second column
- Data,action and response on the third column
- Sign name for every time entry
- Ex. Juan Dela Cruz SN
- Document patient’s status on admission
- Blue and black ink for AM and PM shift.
- Red ink for NIGHT shift
Do’s :
- Time and date all entries
- Use flow sheet/checklists. Keep information on flowsheet current
- Chart as you make observations
- Sign and initial every entry
- Described patient’s behavior and use direct patient quotes when appropriate
- Do record exactly what happens to patient and care given
- Factual and complete
- Draw single line thru an error. Mark this entry as “error and sign your name”
- Used only approved observation
- Document patient's current status and response to medical care and treatments
- Write legibly
- Ink
- Use accepted chart forms
Don’t s :
- Begin charting until you check the name and identifying number on the patient’s chart
- Chart procedures or care in advance
- Don't clutter notes with Repetitive or frequently changing data already charted on the flowsheet
- Make or sign an entry for someone else
- Change and entry because someone tells you
- Don't label a patient or show bias
- Don't try to cover up mistakes or incidents by inaccuracy or omission
- Dont whiteout or erase error
- Dont squueze in a missed entry or “leave space for someone else who forgot to chart
- Dont write in the margins
- Dont use meaningless words andphrases, such as good day or no complains
Focus
- It is the subject/purpose for the note
- Nursing diagnosis
- Event (admission, transfem discharge, teaching Etc).
- Patient event or concern (code blue, vomiting, coughing etc.
Data
- Contains a narrative of the subjective
- WHAT DOES THE PATIENT SAID, NON-MEASURABLE
- Objective data
- Assessment findings, vitalssigns ang other measurable values
- Supporting evidence for your focus
- You wnat to writer what you did this is what the patient is saying what i m seeing
Action - What you did with patient findings - Use of verbs
Response - px response to interventio
General survey
- Study of a Whole person
- Covering the general health state and any obvious physical characteristics
- Objective parameters
Getting ready
- Wash your hands and observe standard precaution as necessary
- Gather
- Knock
- Identify
- Explain
- Provide privacy
- See to safety
Getting ready
- Confirm comfort
- Leave the call
- See to safety
- Open curtain
- wash your hands
- Report and record
Four areas
- Physical appearance
- Body structure
- Mobility
- Behavior
Physical appearance
Normal
- Age; Appear his/her stated age
- Sex: sexual development appropriate for their age
- Level of consciousness: alert, oriented to person, place, time and situation.
- Responds appropriately
- Skin color: color tone is even, pigmentation variations, skin intact- no obvious lesions
- Tattoos and piercing and stage healing
- Facial features: facial features are symmetric with movement
- Ovverall appearance:
- No signs of acute distress are present
Abnormal
- Age; Appear older than stated age
- Sex; delayed puberty
- Level of consciousness:
- Aunt= active
- Clara- confusion
- Loves- lethargy
- Oranges = Obtunded
- snacks= Stupor
- Cookies = Coma
- Skin color:
- Pallor
- Cyanosis
- Jaundice
- Erythema
- Any lesions
- Facila features:
- immobile , mask like, asymmetric, dropping
- Overall apperance:
- Cardiac respiratory signs:
- Diaphoresis, clutching chest, shortness of breath, and wheezing.
- pain , indicated by facial grimace, and holding body part.
- Cardiac respiratory signs:
