Pathology of Restrictive Lung Disease
restrictive-diffuse-interstitial lung disease
reduced lung compliance-stiff lungs
low FEV1 & low FVC but FEV1/FVC normal ratio because no limitation to air moving in and out, just less air to move in n out
reduced gas transfer-diffusion abnormality
ventilation/perfusion imbalance when small airways affected by pathology
Main physiological problem is gas diffusion
dyspnoea shortness of breath on exertion → shortness of breath at rest (as disease progresses)
patient may have type 1 respiratory failure with hypoxaemia, with cor pulmonale and heart failure
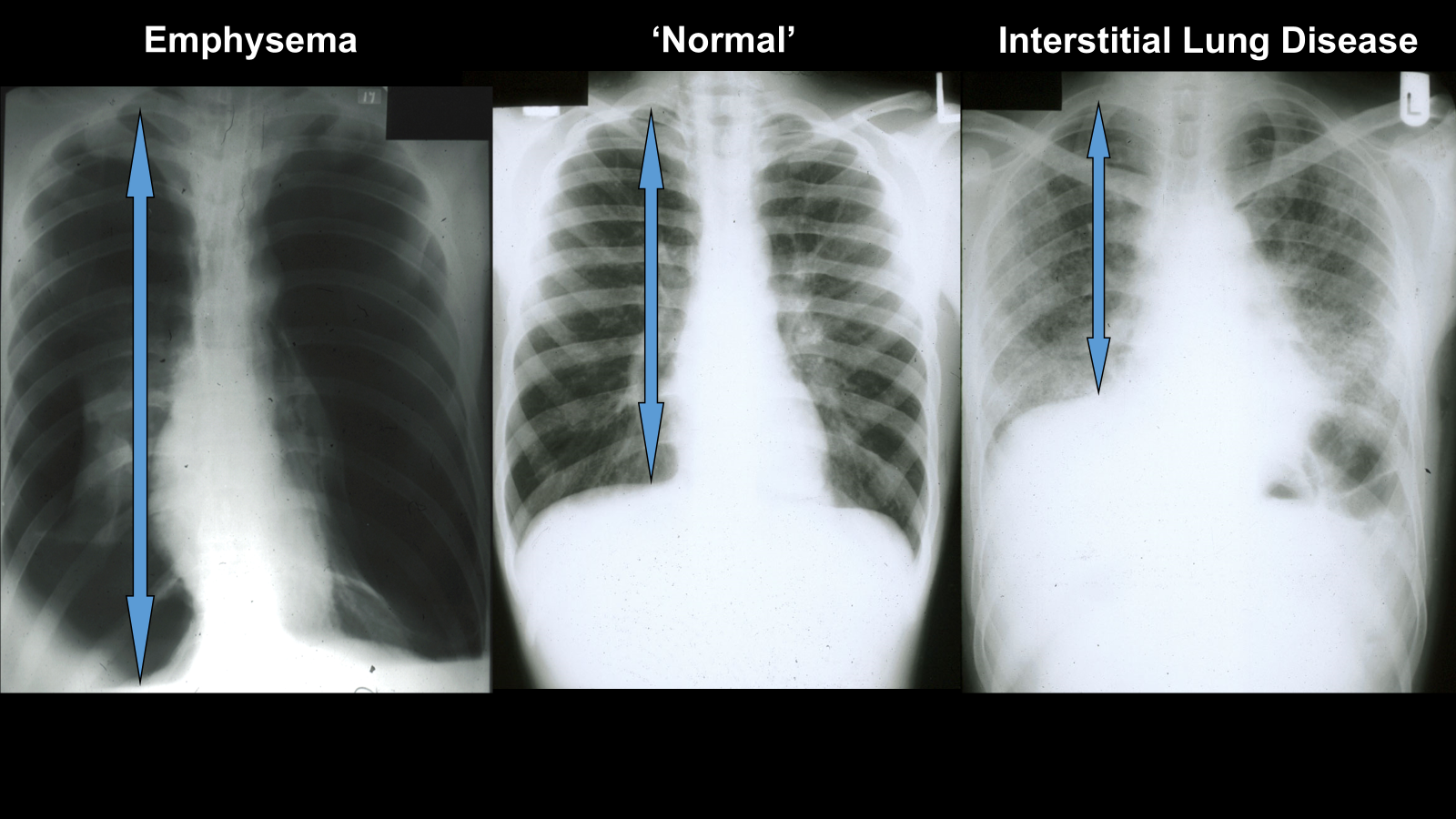
emphysema, increased lung volume as they have to maintain more air in lungs for small airways to breath in and out
interstitial reduced lung volume as less space for air?
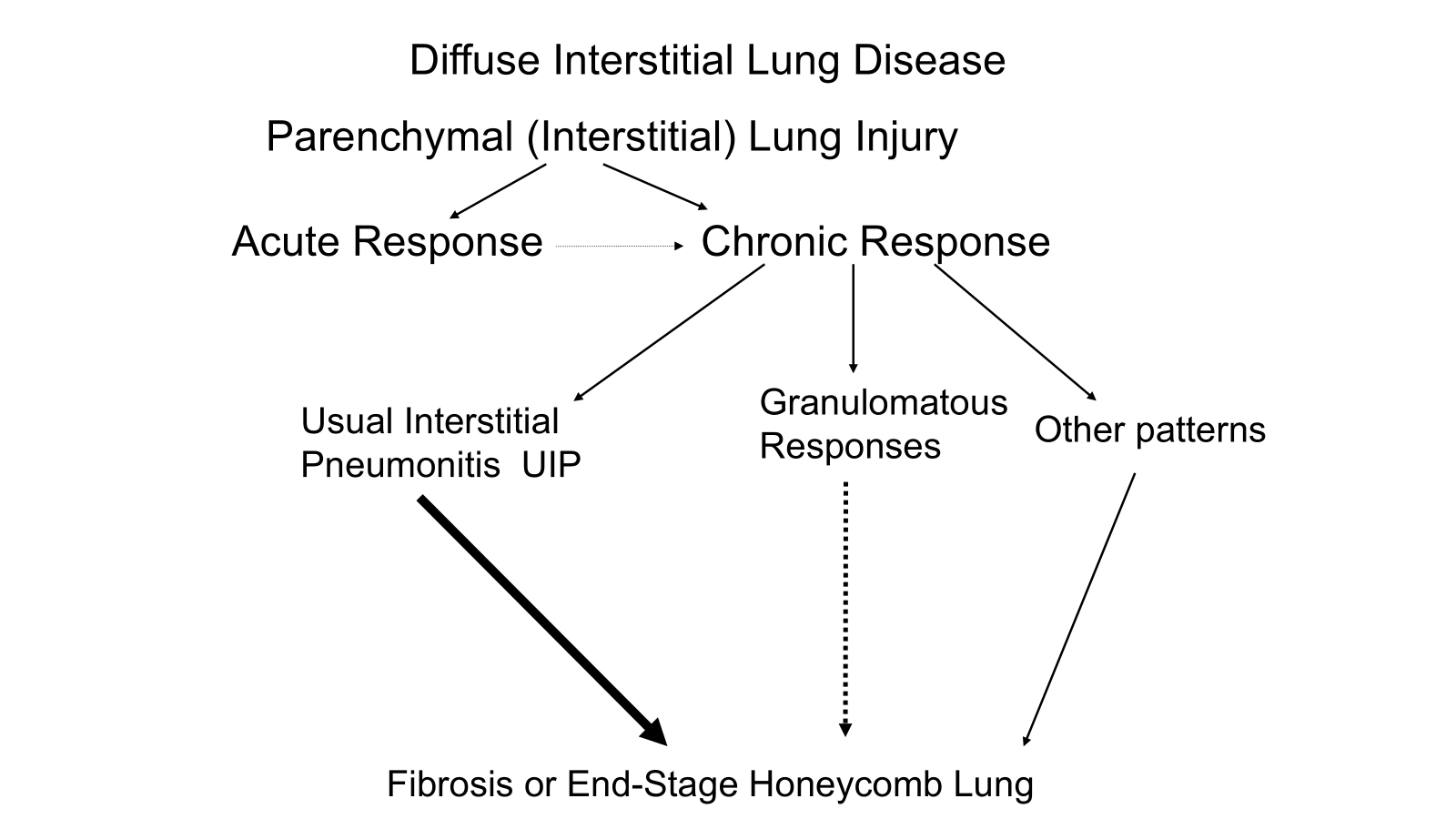
the end result is irreversible
UIP almost inevitable to end up with pulmonary fibrosis
granulomatous less likely to progress into end stage fibrosis
diffuse alveolar damage (DAD) also known as acute respiratory distress syndrome (ARDS)
is an acute inflammatory process
not only leaking of capillary walls but damage of epithelial cells, leaks into alveolar air space, fills lungs with fluid
protein becomes deposited around alveoli
after a few days becomes more chronic
ultimately fibrosis follows as an attempt to heal
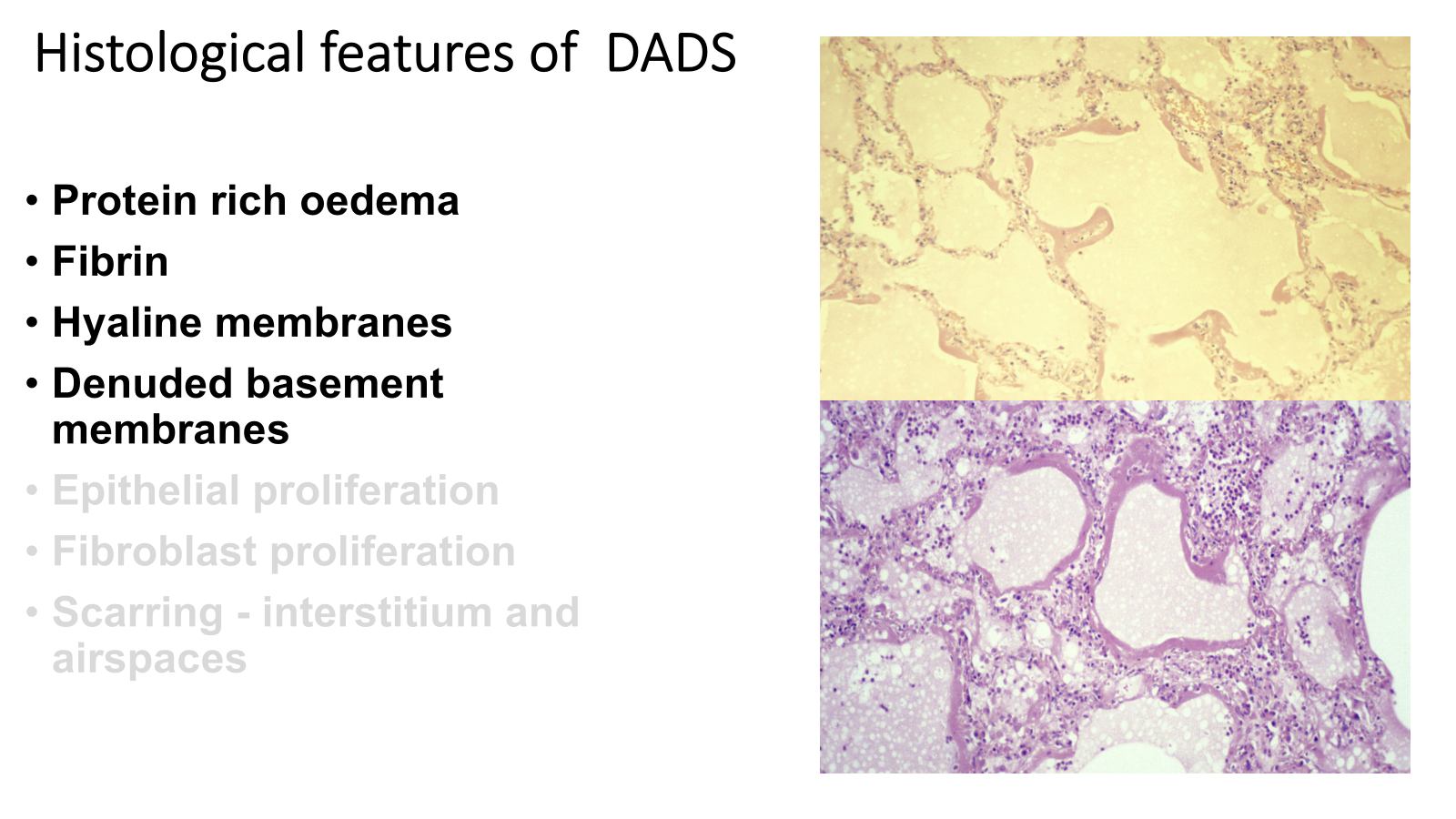
pink layer is hyaline membrane
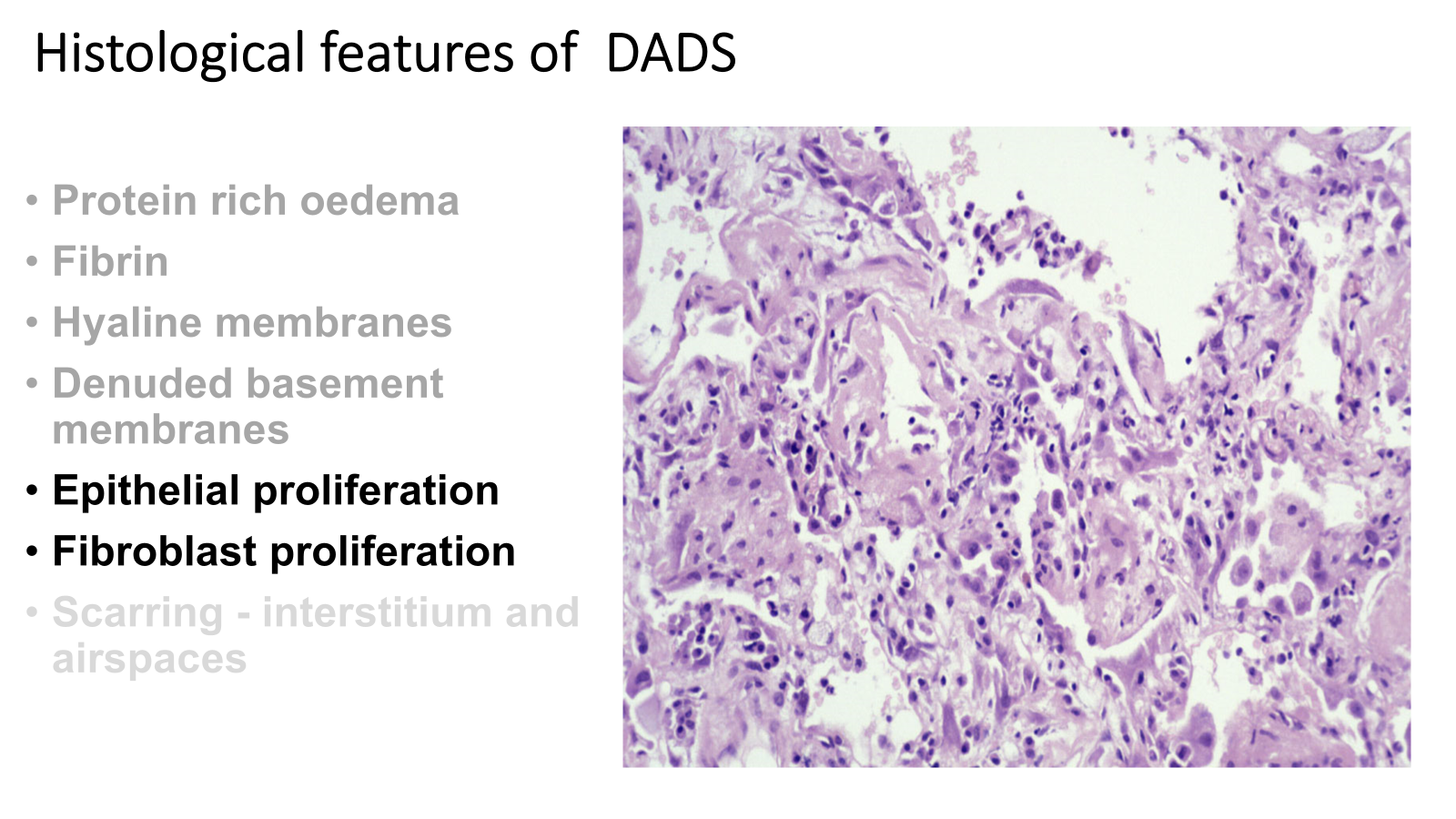
mechanism to repair and heal kick in but don’t work very well
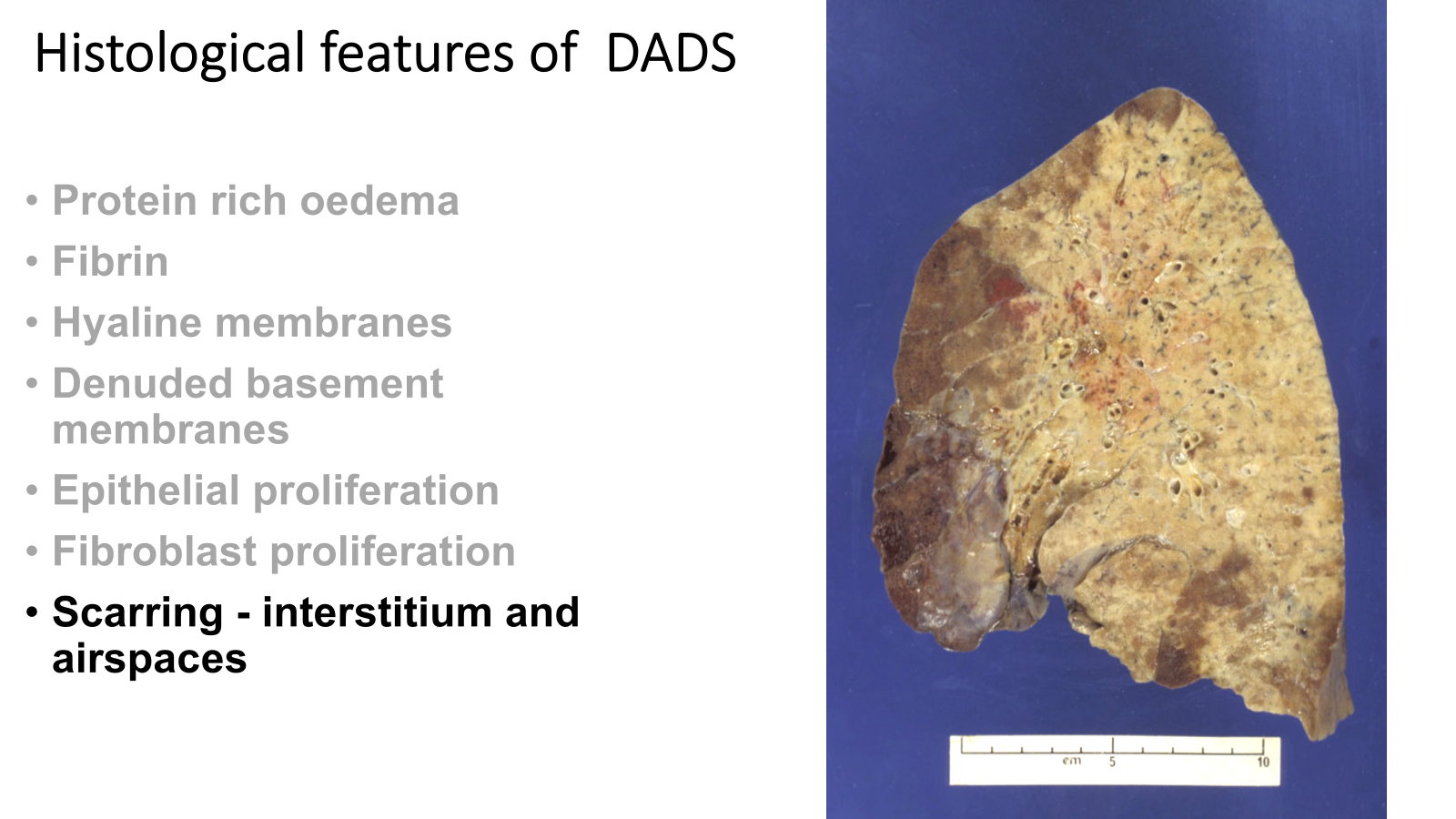
less than 50% make it out of Intensive care, most die
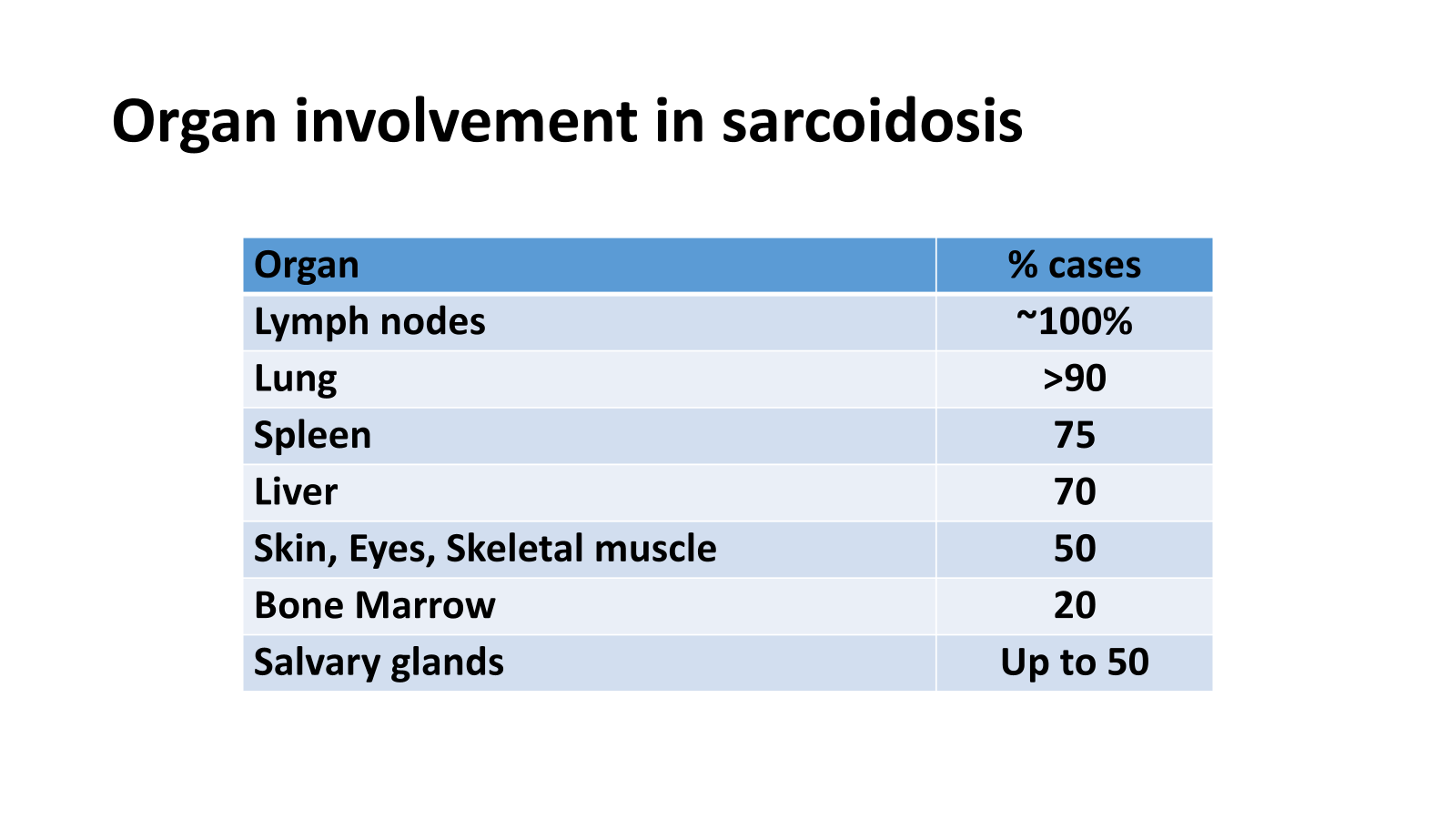
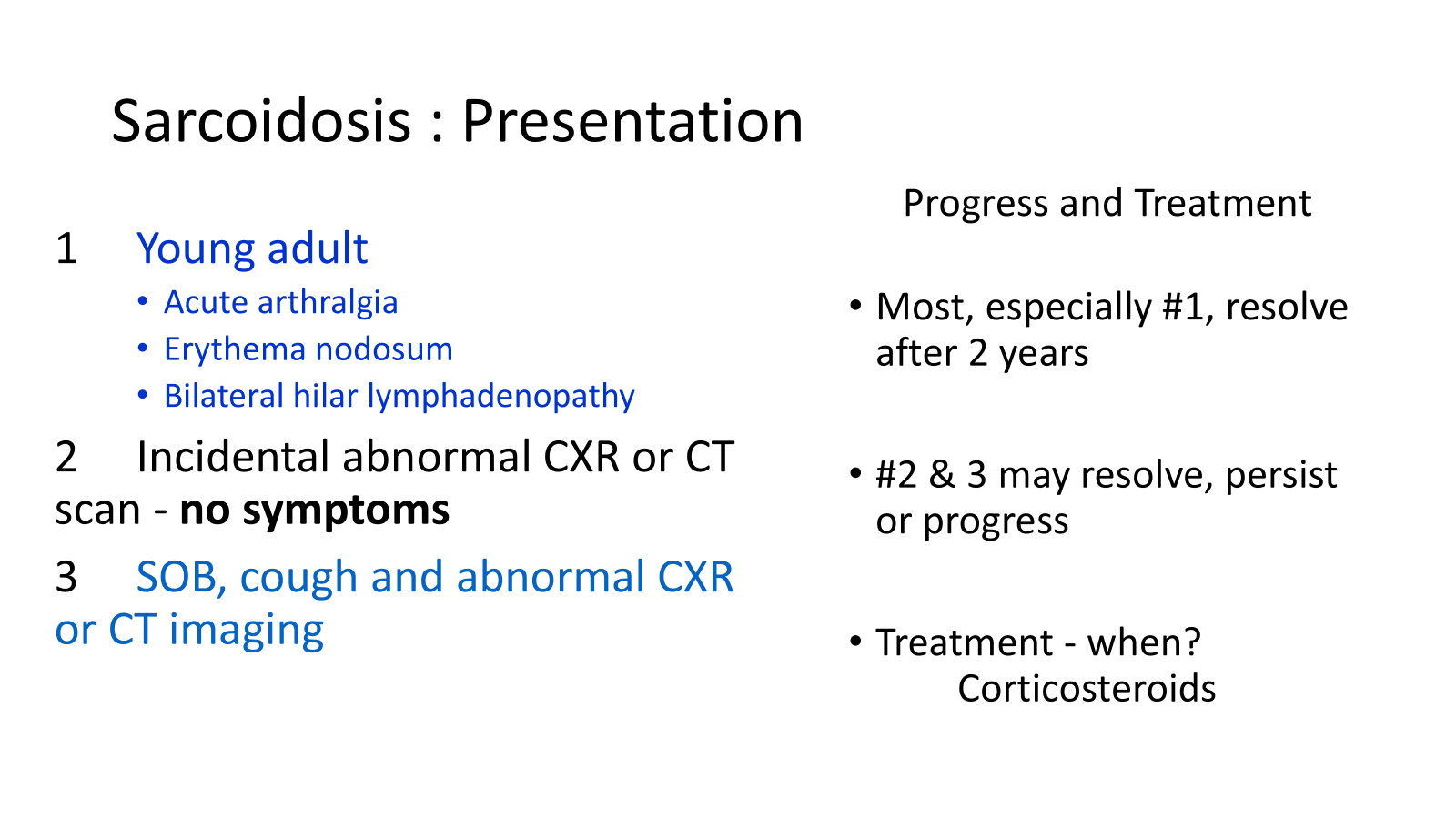
Sarcoidosis is a multisystem granulomatous disorder of unknown aetiology (unknown cause)
evidence of type 4 hypersensitivity reaction, but to what? They don’t know
histopathology: epithelioid and giant cell granuloma
necrosis/caseation very unusual
very few lymphocytes associated with these granulomas, little lymphoid infiltrate
variable associated fibrosis
commonly affects young adults, female > male
100% involvement of lymph odes in sarcoidosis, >90% etc
Hypersensitivity Pneumonitis : The antigens
inhaled (often organic) antigens
thermophilic actinomycetes
farmers lung, breathes in all the organisms from the wet hay
bird fanciers lung, develop hypersensitivity to feathers or bird poo
feathers from duvet
some patients with hypersensitivity pneumonitis might present like they have pneumonia but it is more chronic
type 3 & 4 hypersensitivity reactions
lots of granulomas and interstitial
dominates in upper zone of the lungs
hypersensitivity pneumonitis is a bit more likely to give you fibrosis
UIP, 5 year survival of 30%, inevitably a progressive disease
UIP is commonly idiopathic pulmonary fibrosis
also in connective tissue diseases, drugs, asbestos, viruses (can all get UIP)
histopathology of UIP is patchy interstitial chronic inflammation
progressive accumulative damaging lung inflammatory process, goes over for a long period of time
eventually die of respiratory failure
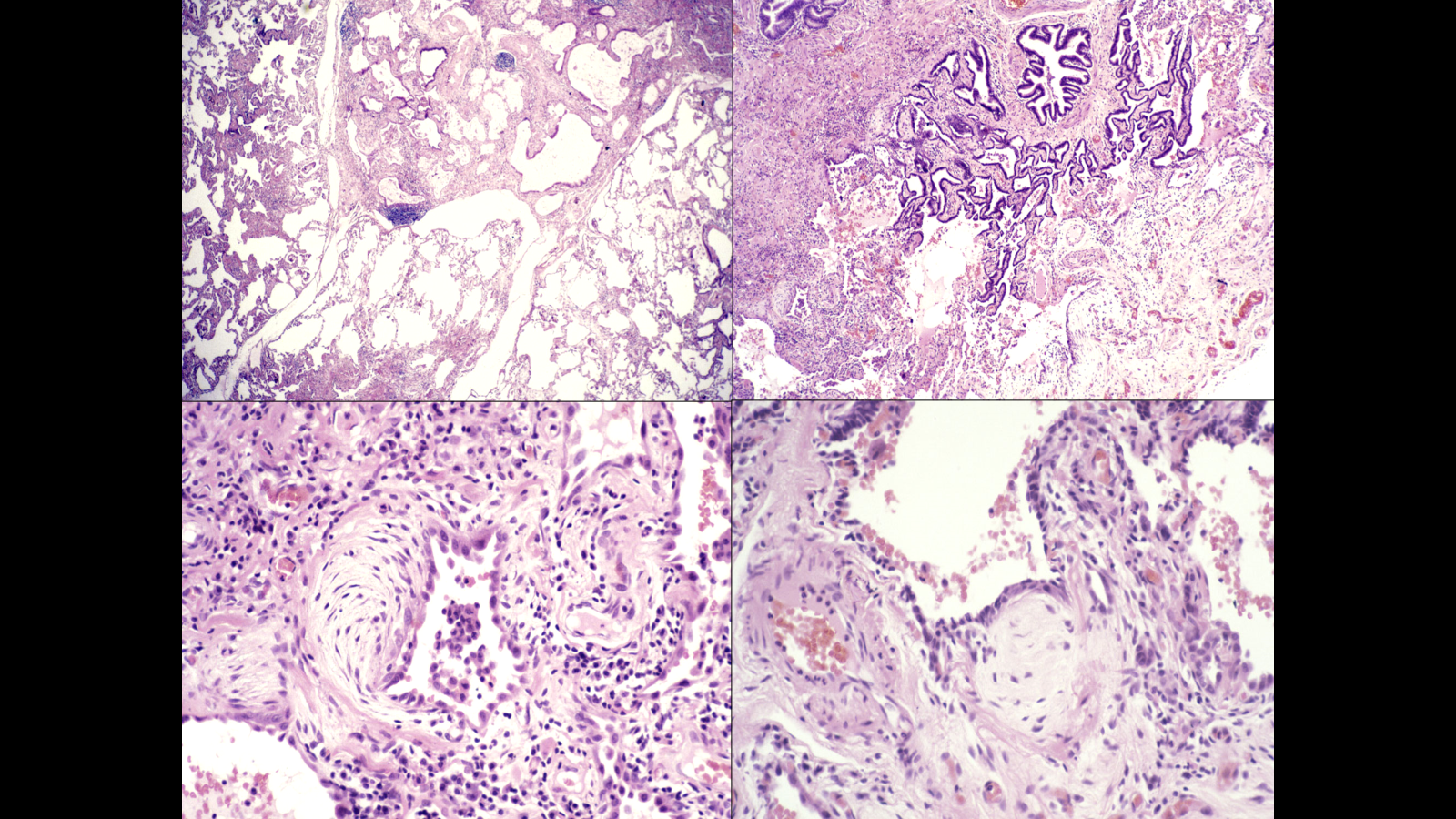
in lower images fibroblastic fossi-key pathological change indicating damage and fibrosis that will scar up and lead to damaged lung
Idiopathic Pulmonary Fibrosis
•Elderly >50 M>F
•Pathology is Usual Interstitial Pneumonitis
•Clinically show
•Dyspnoea, Cough,
•Basal Crackles, Cyanosis, Clubbing
•Progressive Disease : Most dead within 5 years
•CXR : Basal/Posterior, Diffuse infiltrates, Cysts, ‘ Ground Glass ’
•Restrictive PFT & Reduced Gas Transfer
•Poor Prognosis : Some fulminant, some steroid responsive
diffusion impairment means it takes LONGER for blood and alveolar air to equilibrate, particularly for oxygen
diseases impairing gas diffusion usually do NOT change CO2 levels
CO2 diffuses 20 times faster than O2 due to greater solubility
FIO2 = the Fraction of Inspired air which is Oxygen
•Equilibration normally takes 0.25 seconds
•Capillary transit time normally 0.75 seconds at rest
•In disease, equilibration may take close to 0.75 seconds
•PaO2 maintained at rest but……
•Serious falls in PaO2 may occur on exercise as capillary transit time falls
•Hypoxaemia may be corrected by increasing FIO2. This increases PAO2, thus increasing rate of diffusion. Rarely clinically the sole cause of hypoxaemia
if you increase time for equilibration to occur you get closer to 0.75 seconds opportunity, if you increase and it takes longer than 0.75, patient not hypoxic at rest but when they exercise, less time available, if fibrosis and increased time for equilibration you will get breathless at exercise
severe pulmonary fibrosis, even at rest with more time, might not be long enough for equilibration to take place so patient breathless at rest