Disorders of Childhood & Adolescence
Developmental Psychopathology
Focuses on origins and course of psych maladaptation in the context of normal development
Individual may “grow out” of certain problems, while others may severely impact future
Vulnerabilities
Dependence on others
Good or bad, abusive or exploitative
Lack of experience handling problems
Lack realistic views of world and self
Limited understanding of social expectations
Difficulty understanding why bad things happen
Resilience
better Ability to cope when negative things happen
better Ability to develop normally despite significant hardship
Childhood problems as risk factors
Externalizing problems
“undercontrolled”
Aggressive
ADHD
Conduct disorder
Oppositional defiance disorder
More boys
Internalizing problems
“overcontrolled”
Inner distress, shyness
More girls
Separation anxiety
Selective mutism
Disinhibited behavior is a trait of childhood
Children have poor impulse control, planning, delay of gratification, etc.
Think marshmallow/oreo test
If disinhibition persists into adolescence, it can result in increased risk taking, substance abuse, and suicide rates
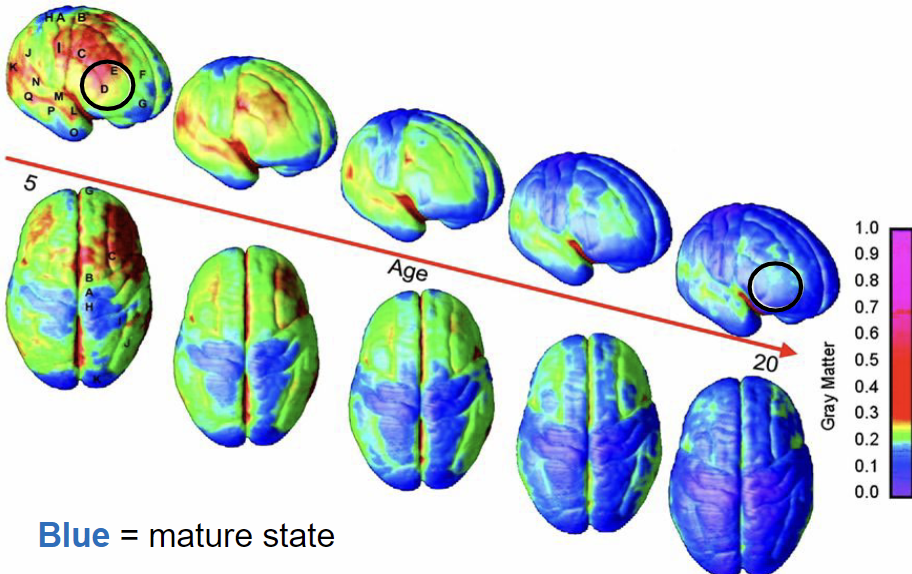
Brain Development
Subcortical regions develop more rapidly
Responsible for emotions, impulses
Prefrontal regions develop more slowly
responsible for planning, impulse control
Greatest disparity in development occurs around 17, could account for disinhibition during teenage/early 20s
Externalizing disorders
Attention Deficit Hyperactivity Disorder
Generally arises before 12
More common in boys (13%) than girls (4%)
Boys more likely to develop hyperactivity/impulsivity
Girls more likely to develop inattention
50% continue to have problems in adulthood
Prevalence has risen significantly in past 20 years
people with ADHD are eligible for disability services in 1992
Effective treatments are widely available
Stimulants
Effective for anyone trying to focus, regardless of ADHD diagnosis
Two aspects
Hyperactivity/impulsiveness
Fidgety
Leaving seat
Runs or climbs excessively when inappropriate
Excessive talking, difficulty staying quiet
Difficulty waiting turn
Interrupts questions, others, etc.
Inattention
Careless mistakes, poor attention to detail
Does not seem to listen
Difficulty following instructions (not oppositional)
Avoids/dislikes things that require sustained mental effort
Easily distracted by extraneous stimuli
Forgetful
Three subtypes
Hyperactivity/impulsivity subtype
Inattentive subtype
Combined subtype
Conduct disorder
Characterized by persistent antisocial behavior that violates
Rights of others
age appropriate social norms
Includes:
aggression towards people or animals
destruction of property
deceitfulness and theft
violation of rules
DSM Criteria:
Persistent violation of rights of others with 3 or more of the following:
Bullying
initiation of physical fights
use of weapons
cruel to people
cruel to animals
theft while confronting victim
rape
arson
deliberate destruction of other’s property
breaking and entering
conning others for personal gain
non-trivial theft
disregarding of parental rules
run away from home at least twice
truancy
Disorder of childhood; individuals over 18 can’t meet criteria
Other associated traits
Antisocial symptoms
peer/family rejection
academic skill deficit
low self esteem/depression
limited work and relationship opportunity
gravitation towards other deviant peers and behaviors
Prevalence
10% general population
More common in males
Gender differences
Males exhibit more violent traits, like fighting/theft/vandalism
Females exhibit more lying, truancy, running away, substance abuse, etc.
Childhood onset is associated with
Inadequate parenting
severe hyperactivity
violent/antisocial behavior
“life-course persistent”
Adolescent onset
emerge alongside puberty
common, temporary, near-normative
“adolescence limited”
Delinquency is normal?
Pushing boundaries and behavioral problems could be considered a normal part of teenage and young adulthood
Oppositional Defiant Disorder
Defiant or vindictive behavior
Resentment or anger towards authority
Similar to Conduct disorder, but less severe
Doesn’t include:
Physical aggression
property destruction
theft
Acting out is directed towards figures of authority more than peers
DSM criteria
Hostile, defiant behavior with at least 4 of the following
Loses temper
argues with adults
actively defies or refuses to comply with adult requests
deliberately annoys people
blames others for personal mistakes
touchy, easily annoyed
angry/resentful
spiteful or vindictive
Severity
Mild: sx occurs in 1 setting
moderate: sx occurs in 2 settings
severe: sx present in 3+ settings
Prevalence
10% in general population
Greater in males prior to puberty
roughly equal after puberty
appear before 8yo and usually persist through adolescence
Sxs usually seen in multiple settings
Associated features
Considered precursor to conduct disorder
Only 25% of ODD develop CD
Common comorbidities
ADHD
Depression
Substance use
effective treatments
Reward of appropriate behaviors
punishment of defiant behaviors
Internalizing disorders
Separation anxiety disorder
Most common type of childhood anxiety disorder
excessive anxiety about separation from attachment figures
child is terrified something terrible will happen to self or parents after separation
to a developmentally inappropriate degree
DSM Criteria
Inappropriate anxiety evidenced by 3 or more:
Recurrent, excessive distress upon separation from primary caregiver
(“attachment figure”)
Persistent fear of harm coming to attachment figures
Persistent worry about something bad happening that will prevent child from
seeing attachment figures
School refusal due to anxiety about separation
Persistent fear of being alone without attachment figures
Need to sleep near attachment figures
Repeated nightmares about separation
Physical Sxs upon separationDuration of at least 4 weeks
Onsets prior to 18
4% of children and adolescents develop SAD
Equally common across sexes
Adolescent onset is uncommon
Could be prompted by life stress
parent’s divorce, death of loved one
Associated features
social withdrawal
school refusal
difficulty concentrating, academic problems
Concerns about death and dying
Selective Mutism
Consistent failure to speak in specific social settings
normal speech in other situations
Disturbance interferes with educational, social, or occupational achievement
Duration of at least 1 month, not associated with start of school
Failure to speak is not due to lack of knowledge or comfort with the spoken language
Autism Spectrum Disorder
DSM criteria
Persistent deficits in social communication and interaction across multiple contexts, examples including
Abnormal social approach and failure of normal conversation
deficits in nonverbal communication, abnormal eye contact and body language
deficits in developing, maintaining, and understanding relationships. limited imaginative play or interest in peers
Restricted, repetitive behavior patterns
Interests, need for sameness, adherence to routine, repetitive motor movements or speech
Hyper or hyporeactivity to sensory input
Must be present in early development
cause clinically significant impairment
not better explained by intellectual disability
Intellectual disability is often present, but not always
verbal skills suffer most
Associated behaviors
hyperactivity
short attention span
impulsivity
aggression/tantrums
Prevalence
old diagnosis (autism disorder) was about 1 in 2000
rate of ASD is about 1 in 50
4-5 times higher rate in males than females
when females are affected, there tends to be greater intellectual disability
Etiology
Most established causes are genetic
Some common variants identified by genome-wide association study
Many severe cases attributable to de novo variants
neither parent has genetic risk factors, but child has severe ASD often with intellectual disability
occurs through genetic mutation in utero
There are certainly environmental factors that increase the risk of ASD, but not enough proof yet
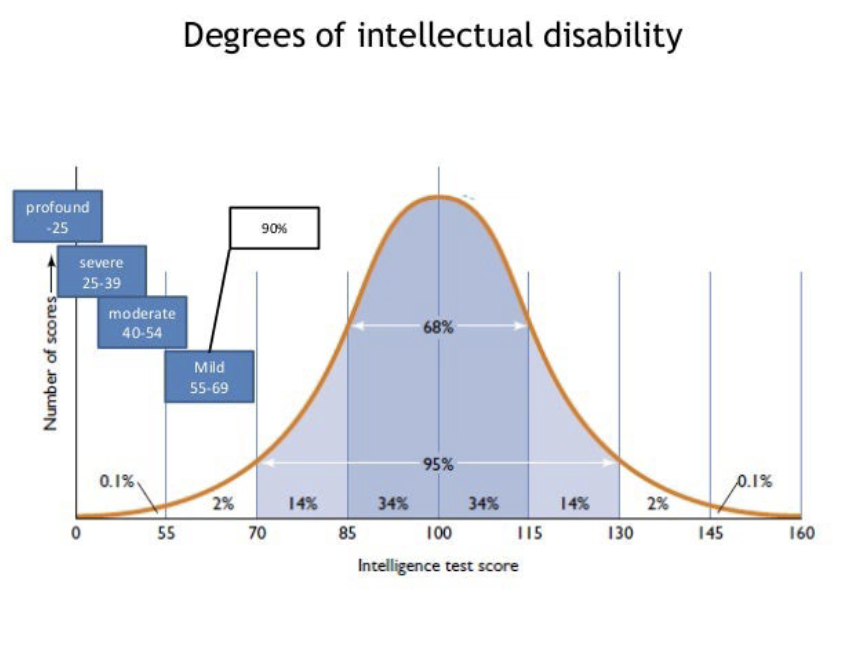
Intellectual Disability
Significant subaverage IQ of approx 70 or below
Inability to care for themselves
DSM Criteria
Deficits in at least 2 of the following areas
communication
self care
home living
social/interpersonal skills
use of resources
self direction
functional academic skills
work
leisure
health
safety
Onset prior to 18yo
Severity (IQ criteria)
Mild (55-70)
Moderate (40-55)
Severe (20-40)
Profound (<20)
Co-morbidity is difficult to determine
Presentation of other symptoms or diagnoses can be modified by ID
Etiology
Causes are varied
Mild ID is very multifactored with polygenic and pol-environmental causes
Severe ID tends to have some other genesis
Trauma
Toxins
Genetic/chromosomal conditions
PKU, Down’s, Fragile X, etc.