Scrotum and Testes Part 3
Learning Objectives
Identify and describe common pathologies on sonographic images of the scrotum and testes
Differentiate the aetiology, clinical presentations, and sonographic appearances of:
Hydrocele
Epididymal cyst
Varicocele
Epididymitis
Epididymo-orchitis
Cryptorchidism
Scrotal pearl
Microlithiasis
Germ cell tumours
Common Pathologies for Scrotum and Testes
Clinical Indicators
Extratesticular lumps or swelling:
Hydrocele
Epididymal cyst
Varicocele
Epididymitis, orchitis, or epididymo-orchitis
Cryptorchidism
Scrotal pearl
Microlithiasis
Intratesticular lumps or swelling
Scrotal swelling with pain (discussed in part 4 in lecture series)
Extratesticular Lumps or Swelling
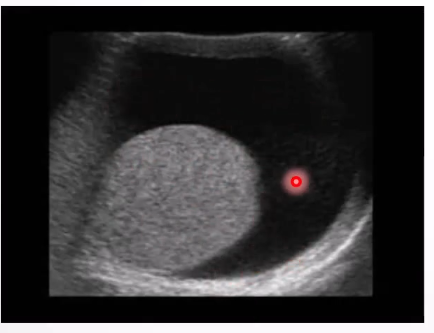
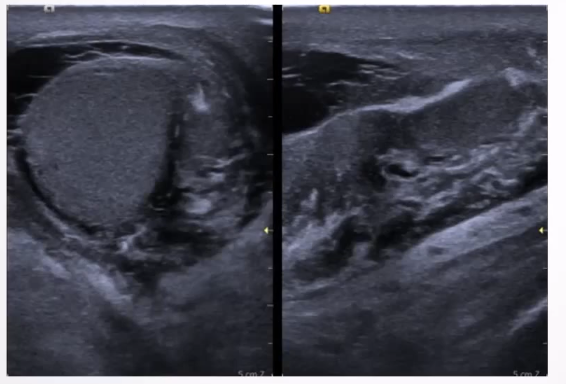
Hydrocele: A serous fluid collection between layers of the tunica vaginalis surrounding the testis or spermatic cord.
Types: Acquired or congenital
Causes of acquired hydroceles: Trauma, epididymitis, testicular torsion, neoplasm, and infarction.
Clinical Presentation: Usually a painless scrotal swelling; can become painful if infected (pyocele).
Ultrasound Appearance: Testicular
Simple avascular fluid collection around the testis, may extend to the inguinal canal
Low-level echoes possible due to protein aggregation or cholesterol crystals.
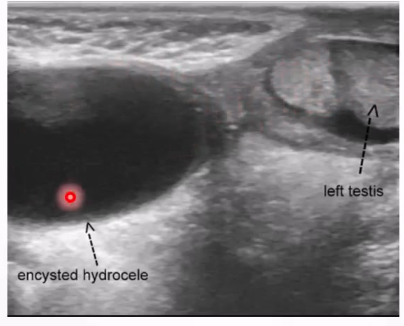
Ultrasound Appearance: spermatic cord
Anaechoic mass in the groin along the spermatic cord
Situated above and separate from the testis and epididymus
Avascular
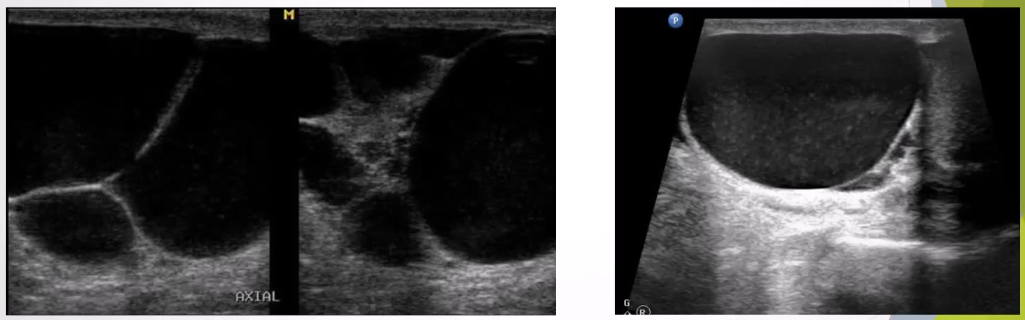
Epididymal Cyst:
Most common epididymal mass, usually contains lymphatic fluid, can be single or multiple.
Clinical Presentation: Often a palpable mass, asymptomatic in one-third of patients.
Ultrasound Appearance:
Well-defined anechoic lesion within the epididymis
Shows posterior acoustic enhancement.
Large cysts can displace the testis

Spermatocele: benign cystic lesions that contain spermatozoa, lymphocytes and debris
Cause: forms as a result of efferent duct obstruction and usually located at the head of epididymus
Cannot be differentiated from epididymal cysts apart from spermatoceles usually having septations
Can be associated with a prior vasectomy
Clinical presentation: usually a painless incidental finding; can present as a mass lesion if large enough
Ultrasound apperance: well defined epididymal cystic lesions with posterior enhancement; low-level echoes representing spermatozoa; septations; can still be anaechoic and singular; indistinguishable from an epidiymal cyst
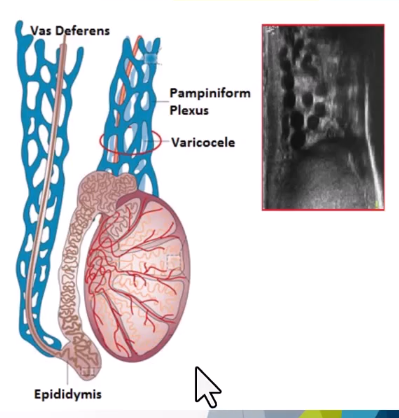
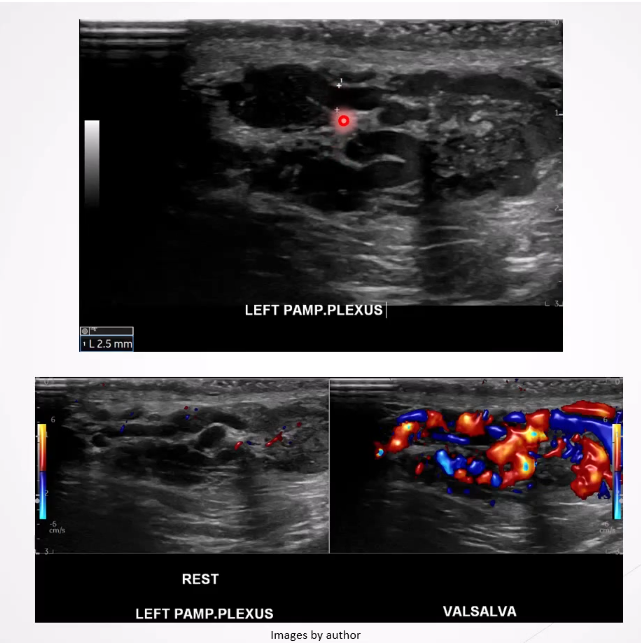
Varicocele: Dilatation of the pampiniform plexus of veins within the spermatic cord and the most common mass of the spermatic cord. Most common cause of male infertility
Causes: most are primary resulting from incompetent or congenitally absent valves in the testicular vein.
Secondary varicoleles less common and reuslt from increased pressure in testicular vein due to compression from renal enal mass, lymphadenopathy or renal vein compression in nutcracker syndrome
Left testicles more affected than the right due to the anatomical differences in venous drainage, leading to a higher incidence of varicocele on the left side.
Clinical Presentation: Can be asymptomatic; symptoms may include scrotal mass/swelling, pain, testicular atrophy, and infertility.
Ultrasound Appearance:
Dilated veins >2-3 mm in diameter
Scrotal mass with a "Bag of worms" appearance above or posterior to the testes
Veins increase in size with Valsalva maneuver.
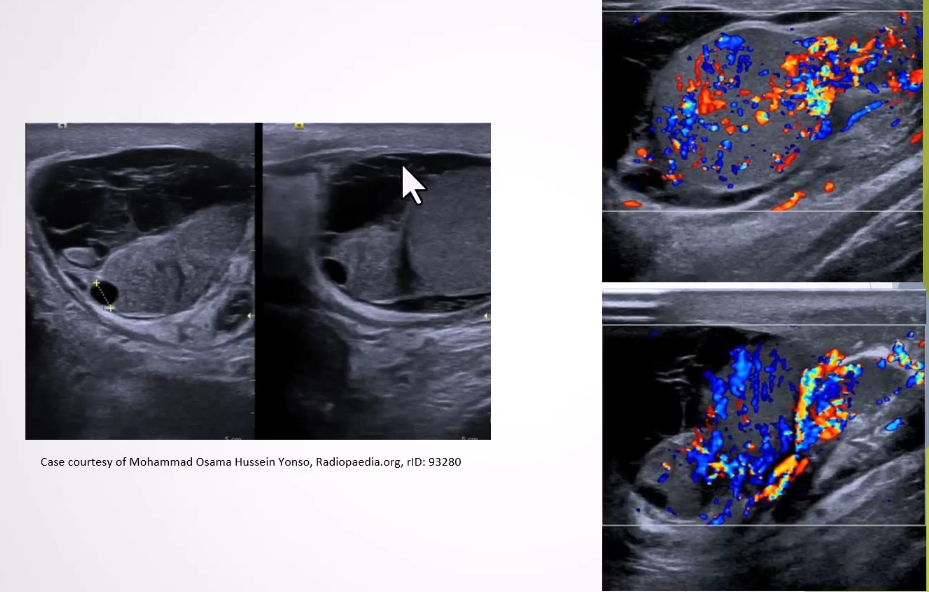
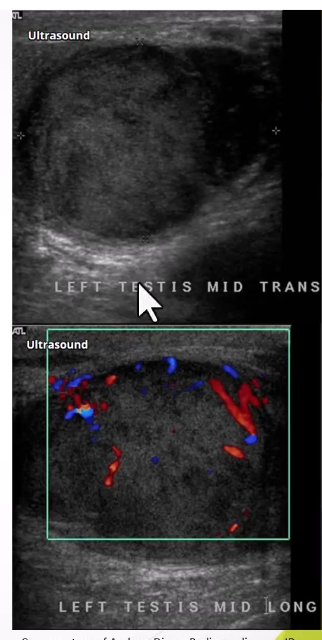
Epididymitis and Epididymo-orchitis:
Infection that originates in bladder/prostate and spreads via ductus deferens → lymphatics → spermatic cord —> epididymis → testis
Tail of epididmysis affected first - epididymitis
If nfection then moves to head of epididymis then testis - epidiyomo-orchitis
Clinical Presentation: Range from mild tenderness to acute scrotal pain; fever, warmth, and swelling in the scrotum can occur.
Ultrasound Appearance:
Thickened, hypoechoic epididymis with increased blood flow; reactive hydrocele may be present.
Epididymo-orchits - testes have increased blood flow which can be large and heterogenous
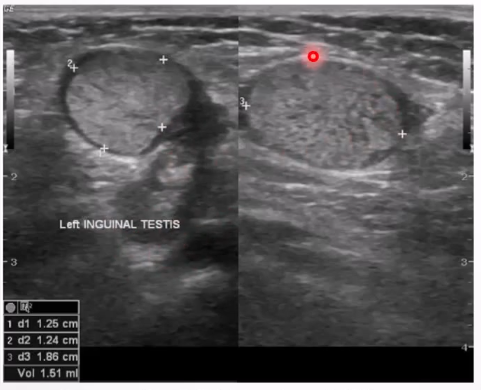
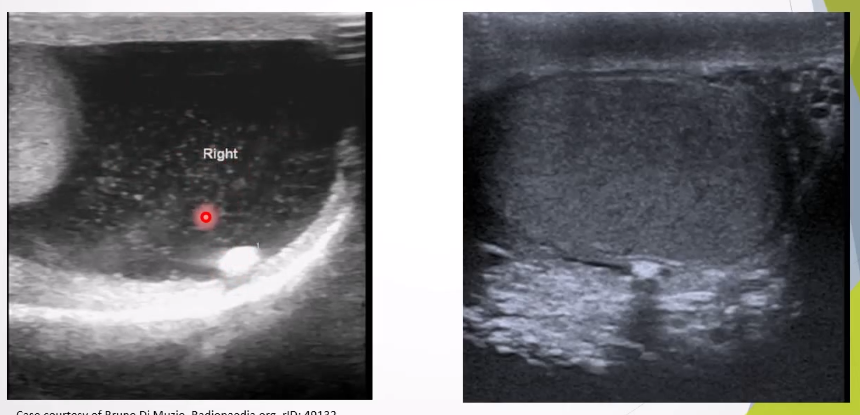
Cryptorchidism: Absence of testis in scrotal sac, due to undescended or ectopic testis.
Causes: Premature birth, IUGR, maternal lifestyle during pregnancy (smoking, alcohol).
Clinical presentation: one testis or both missing from scrotal sac
Ultrasound Appearance:
Lack of testis in scrotal sac; undescended testis appears homogenous and hypoechoic.
Scrotal Pearl: Benign macrocalcifications in scrotum, occur due to microtrauma.
Clinical Presentation: Usually asymptomatic; diagnosed incidentally.
Ultrasound Appearance:
Small mobile hyperechoic extratesticular focus within the tunica space; pearl may show posterior acoustic shadowing if large; can appear as free floating if there is a hydrocele
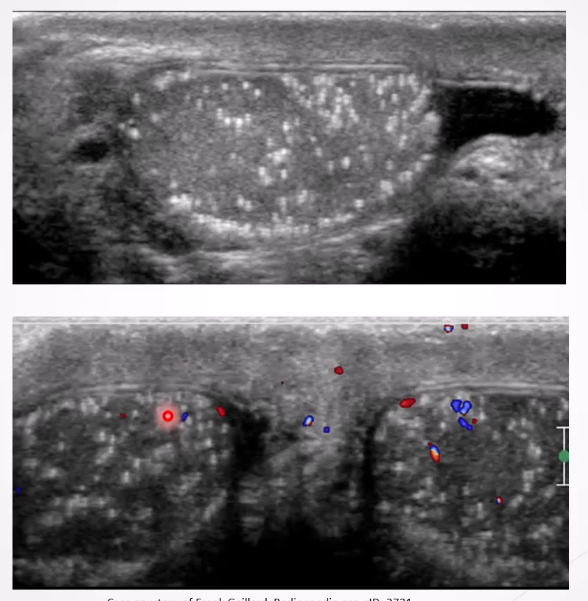
Microlithiasis: Tiny calcium deposits within testes associated with increased risk of testicular cancer.
Clinical Presentation: Usually asymptomatic.
Ultrasound Appearance:
Small non-shadowing hyperechoic foci ranging in diamter from 2-3mm , uniform in size or clustered but can be seen peripherally or segmentally
Intratesticular Lumps
Germ Cell Tumours:
Most common type of testicular cancer (includes seminoma and non-seminoma).
Seminomas: Most common in males aged 15-49 years; associated with undescended testes.
Risk Factors: undescended tests; family history of germ cell tumour, microlithiasis, infections such as HIV, mumps, orchitis
Clinical Presentation: Painless testicular mass; other symptoms may include discomfort or back pain.
Ultrasound Appearance: Homogeneous intratesticular mass, well-circumscribed with lobulated margins, internal vascularity
Non-seminomas: Occur mainly in younger patients, more aggressive, and metastasize frequently.
Clinical Presentation: Similar to seminomas with potential for metastasis.
Ultrasound Appearance: More heterogeneous with cystic areas or calcification.
