Week 9: Penis Anatomy and Ultrasound
Anatomy of the Penis
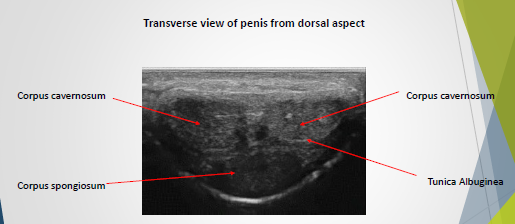
The penis comprises three cylindrical structures:
Two corpus cavernosa, located on the dorsal surface.
One corpus spongiosum, located on the ventral surface.
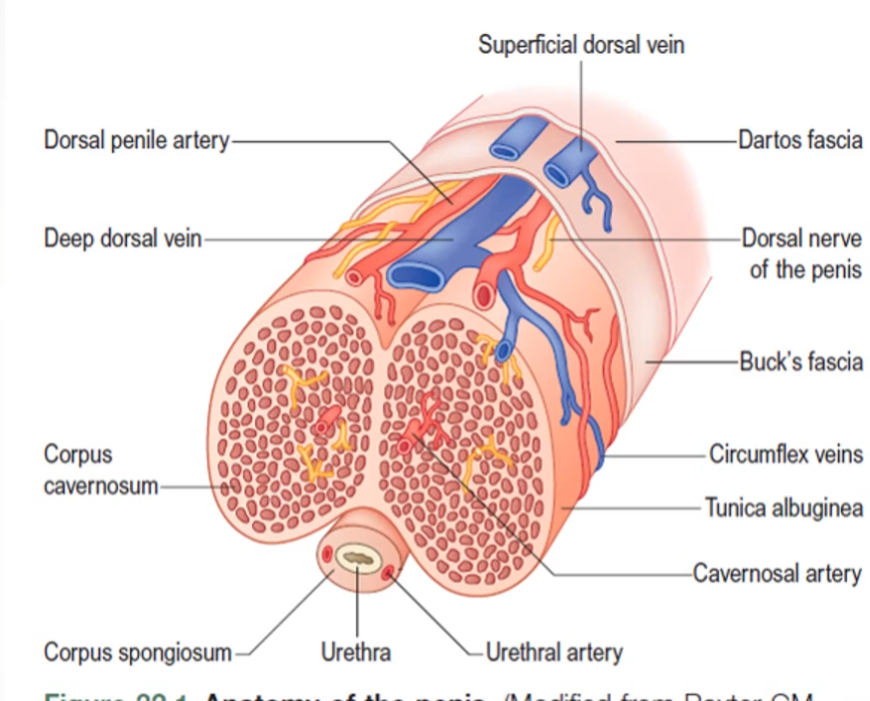
Corpus Cavernosa:
Paired dorsal structures with low reflectivity on ultrasound.
Main erectile structures containing distensible sinusoidal tissue.
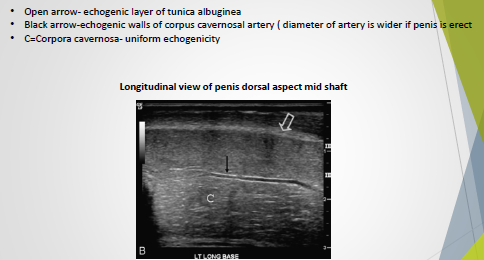
Surrounded by a thin, highly reflective tunica albuginea.
Corpus Spongiosum:
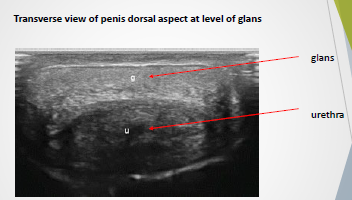
Ventral structure with high reflectivity.
Expands distally to form the glans penis.
The urethra passes through its center.
Both Corpus Cavernosa and Corpus Spongiosum:
Composed of sinusoidal spaces lined by smooth muscle and endothelium.
These spaces fill with blood during an erection.
The corpus spongiosum fills with blood but contributes minimally to the erectile state.
Tunica Albuginea:
A thick fascial sheath encasing both the corpus cavernosum and corpus spongiosum.
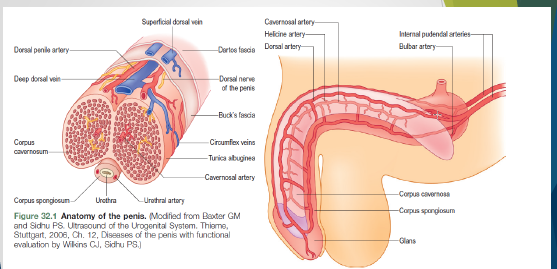
Blood Supply of the Penis
Primarily from the right and left internal pudendal arteries, originating from the right and left iliac arteries.
Each internal pudendal artery divides into:
Dorsal penile artery.
Bulbar artery.
Cavernosal arteries.
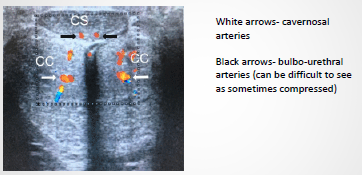
Cavernosal Arteries:
Primary source of blood flow for erectile function.
Dorsal Arteries:
Paired arteries supplying blood primarily to the skin and glans of the penis.
Venous Drainage of the Penis
Occurs via superficial and deep dorsal veins.
Superficial emissary veins perforate the tunica albuginea.
Drain into the deep dorsal vein via the cavernosal, spongiosal, and circumflex veins (visible on ultrasound).
The skin and glans are drained through the superficial dorsal veins.
Embryology
At the end of the first month of pregnancy:
The posterior intestine and the developing urogenital system migrate to the embryo's surface in the cloacal membrane region ventrally.
The cloacal membrane divides into:
A posterior (anal) half.
An anterior (urogenital) half.
Around the urogenital membrane, three bulges form:
Cephalic bulge: urogenital tubercle.
Two genital bulges: located on either side of the urogenital membrane.
At this stage, male and female embryos appear similar.
Male external genitalia development:
Triggered by testosterone release in response to luteinizing hormone from the pituitary gland.
The distance between the anus and genital structures increases.
The penis elongates.
The penile urethra forms from the penile groove.
The foreskin develops.
Foreskin development:
Starts in the 13th week of pregnancy via circular invagination of the ectoderm.
By the 20th week, the ectoderm covers the entire glans.
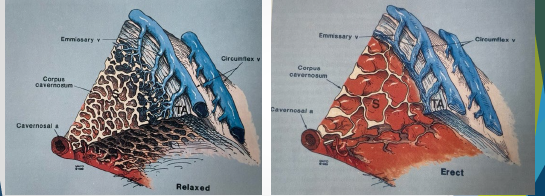
Physiology
Penile Erection:
Results from smooth muscle relaxation in the walls of the sinusoids, helicine, and cavernosal arteries of each corpus cavernosum.
As sinusoidal muscle tone decreases and sinusoids distend with blood, the small emissary veins are compressed between sinusoids and the peripheral tunica albuginea.
Veno-occlusive Mechanism:
Activated to maintain sinusoidal distension.
Limits venous outflow from sinusoidal spaces.
Results in arterial inflow and limited venous outflow.
Sinusoidal spaces distend, creating rigidity in cavernosal tissue, leading to penile erection.
Scanning Technique
Patient Preparation:
Maintain patient privacy (use a "do not disturb" sign).
Patient undresses from the waist down, with the gown open at the back.
Patient lies supine, with the penis positioned on the anterior abdominal wall.
Use the gown or a towel to hold the penis in place at the distal end.
Preserve patient dignity and comfort by covering areas not being scanned (e.g., the scrotal area).
Use warm gel if possible.
Transducer:
High-frequency (7.5-18MHz) linear transducer for high-resolution images.
Clean the transducer with appropriate disinfectant wipes after each scan.
Leave the patient in the room to dress in privacy.
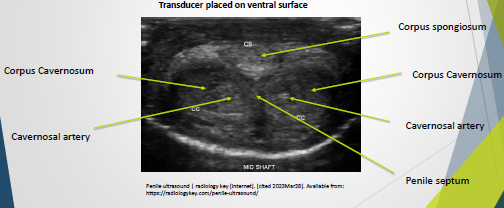
Imaging (Transverse)
Technique:
Place the transducer on the ventral surface at the level of the glans.
Move down to the base of the penis to complete a survey in the transverse position.
Take images at various intervals from the base, mid-shaft, and distal regions of the penis.
Corpus spongiosum is easily compressed.
Use extra gel to alleviate compression.
Colour Doppler evaluation:
Performed in the transverse position to visualize the cavernosal arteries.
Imaging (Longitudinal)
Technique:
Obtain longitudinal evaluations of each corporal body through the ventral surface.
Cavernosal arteries appear as tubular structures with echogenic walls in the center of the corpora cavernosa.
Image the corpus spongiosum and urethra from the ventral aspect.
Avoid unnecessary compression of the penis by using extra gel or a stand-off acoustic pad.
Imaging – Colour Doppler
Used to demonstrate the cavernosal arteries in longitudinal views.
Duplex Doppler exam of cavernosal arteries:
A non-invasive test to assess impotence.
Color Doppler in an erect state is needed when assessing erectile dysfunction.
When Imaging the Penis, Look For:
Plaque placement
Calcifications
Septal defects
Corporal fibrosis