W11: Non-Strabismic Binocular Vision Disorders
Non-Strabismic Binocular Vision (NSBV) Disorders
Definition: Accommodative or oculomotor alignment anomalies characterized by symptoms such as blur or asthenopia.
Key Features:
Fusion is consistently present.
No constant manifest strabismus.
Anomalies may occur in accommodation, ocular alignment, vergence capacity, or interactions between accommodation and vergence.
Clinical Measures:
Compare clinical findings with age-specific expected measures.
Findings that are outside the normal range support the diagnosis of NSBV disorder.
Classifying NSBV Disorders
Symptom Assessment:
Symptoms must correlate with the function of the eyes.
Severity of symptoms tends to increase later in the day when the patient is fatigued or has used their eyes for extended periods
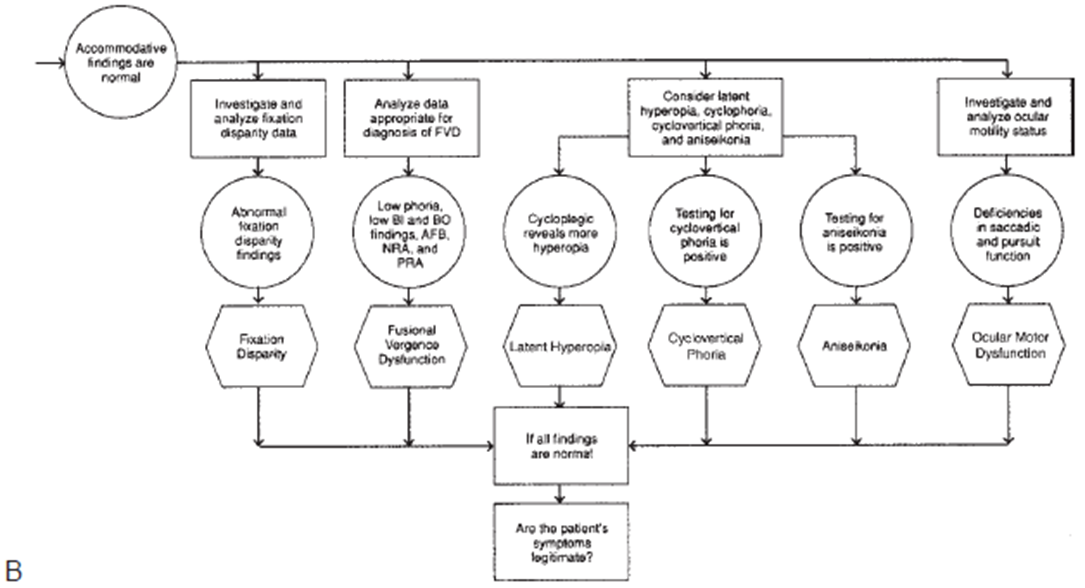
If no symptom escalation is noted, consider alternative etiologies (non-functional or malingering).
Non-functional causes to consider:
Convergence paralysis from ischemic infarction, demyelination, viral infections, Parkinson's disease.
Case History Questions:
Recent illnesses or medications taken? Changes in medication dosage?
Experiencing dizziness or balance issues?
Recent trauma?
Had any fainting spells or numbness/tingling sensations?
Clinical Testing:
To rule out non-functional aetiologies, perform evaluations such as:
External evaluation of eyes.
Pupil evaluation.
Colour vision test (monocularly)
Ophthalmoscopy.
Versions assessment.
Cover test (distance and near, including 9 positions of gaze).
Confrontation fields examination.
Evaluation of Vision and Health:
Confirm that vision, eye health, and refractive error are normal or corrected.
Progress to Classification:
Utilize multiple approaches: flow charts that differentiate between vergence and accommodative dysfunction.
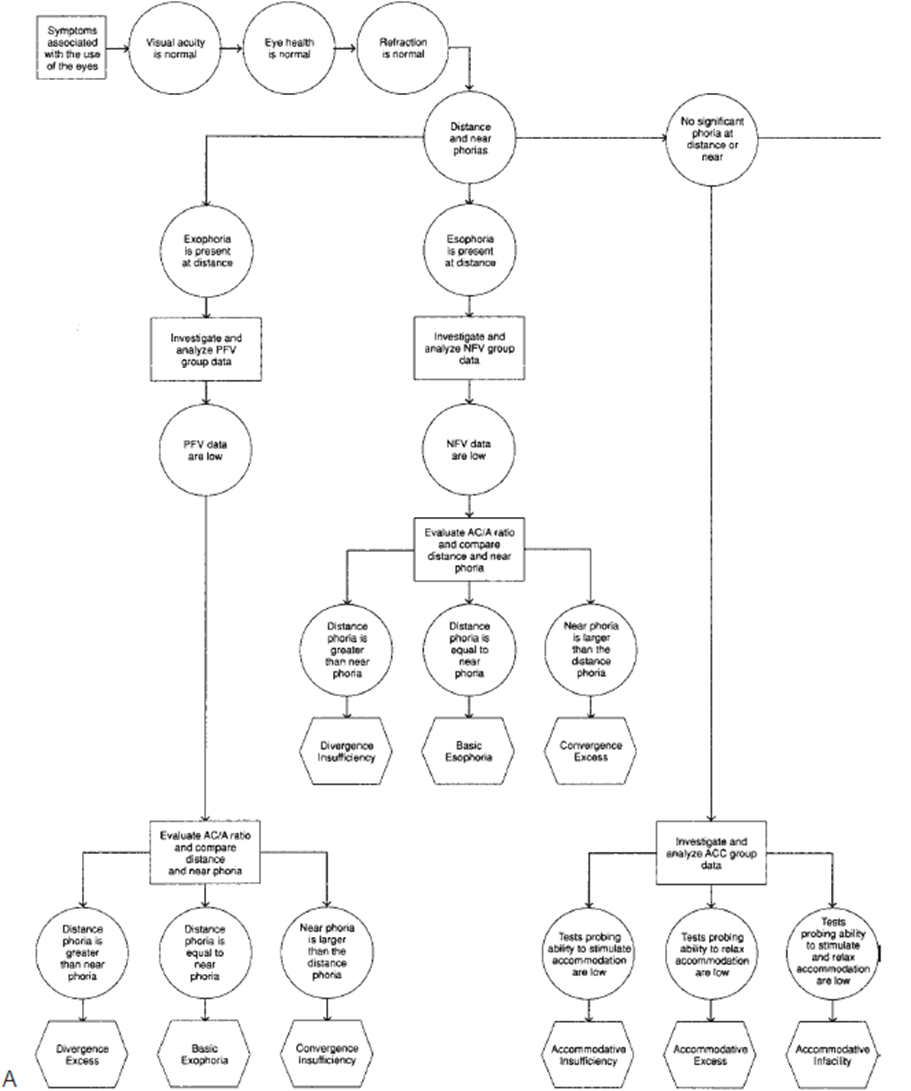
Esophoria: investigate PFV data = anything related to BO or anything related to NRA
Exophoria: investigate NFV data = anything related to BI or PRA / accommodation
Distance problem = divergence
Basic exophoria / esophoria: distance and near phoria within 10.
Near problem = convergence
excess conditions = high AC/A
responds well to added lenses (e.g., minus to exo will help change vergence posture).
over minus for divergence excess
over plus for convergence excess
insufficiency conditions = low AC/A
do not benefit from added plus or minus
need vision therapy or prisms.
convergence = vision therapy
divergence = prisms.
No significant phoria → look into accommodative findings.
MEM / Fused crossed cyl
Facility
Amps
PRA / NRA
when unable to clear minus lenses - reduced AA, PRA, facility → not able to accommodate = accommodative insufficiency.
when unable to clear positive lenses - reduced NRA, facility → can’t relax accommodation = accommodative excess.
Inconsistent - accommodative infacility.
Accommodation not influenced by AC/A
^^ don’t spend to much time ^^
Symptoms associated with NSBV Disorders
Vision acuity is typically normal.
Eye health is normal.
Refractive error is correctable.
Assess phoria:
Distance phoria: Greater than near phoria indicates possible issues.
No significant phoria at distance or near implies further investigation needed.
Investigation Procedures for NSBV Disorders
Group Data Analysis:
Evaluate Positive Fusional Vergence (PFV) and Negative Fusional Vergence (NFV) group data.
Analyze associated conditions and responses to clinical measures (e.g., AC/A ratio comparison).
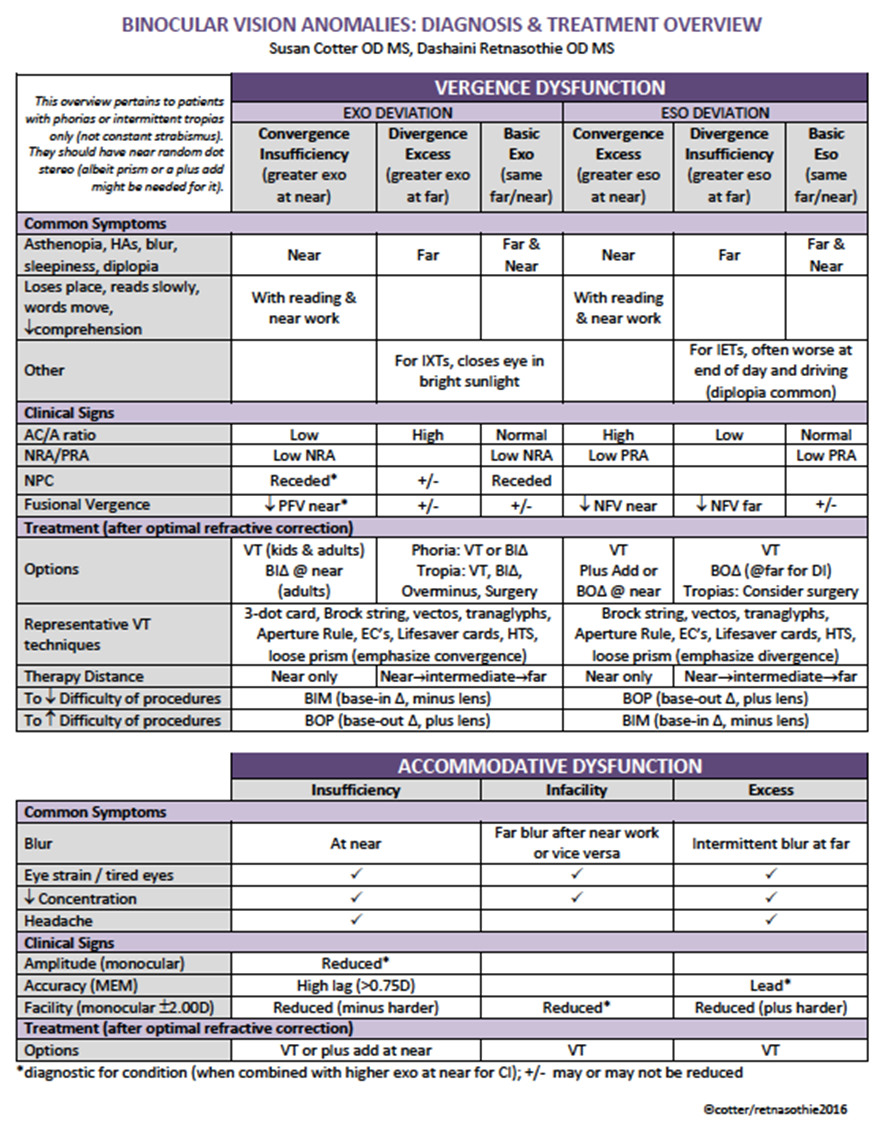
Exodeviation: Convergence Insufficiency
symptoms related to near work:
Asthenopia/headaches (HAs)
Intermittent blur/diplopia
Worse at end of day
Burning/tearing
Inability to sustain and concentrate
Words move on the page
Sleepiness when reading
Decreased reading comprehension over time
Slow reading
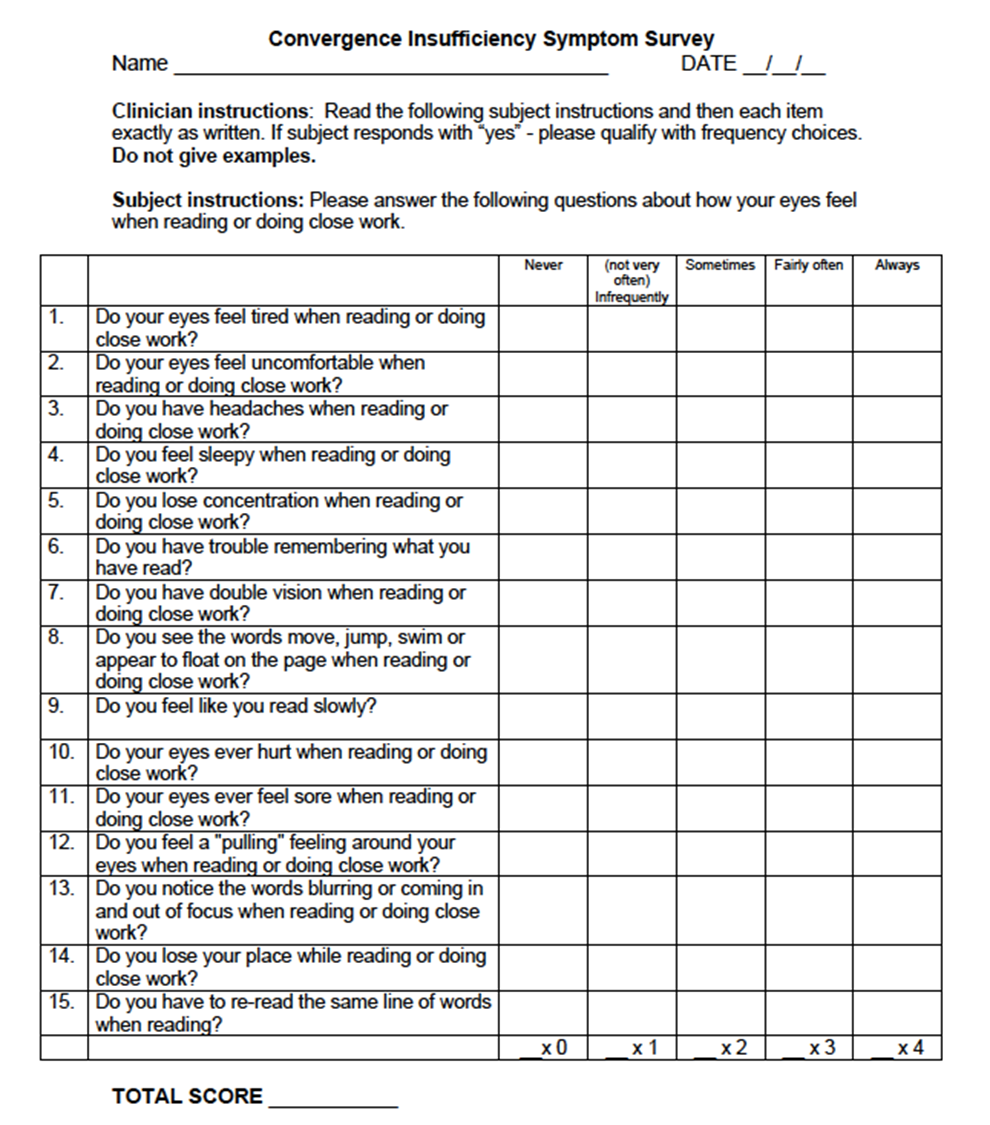
higher score = worse.
Signs:
Greater exophoria at N (than D)
May be orthophoria at D
May be intermittent exotropia at N
Reduced PFV
Reduced vergence facility with BO
Intermittent suppression (if significant, stereopsis may also be reduced)
Receded NPC
Low AC/A ratio
Fails binocular accommodative facility with + lenses
Low MEM/FCC
Low negative relative accommodation (NRA)
Exofixation disparity
Management:
primary approach = vision therapy for sensory motor function (Children and adults)
build BO fusion range (to twice of phoria)
build awareness of NPC
secondary option = prism (BI at N)
especially in adults who don’t want to do vision therapy.
use fixation disparity as a guide.
Exodeviations: basic exophoria
symptoms:
asthenopia (D and N)
Intermittent blur / diplopia (D and N)
worse at end of day
Signs:
Similar exophoria at D and N
Reduced PFV
Reduced vergence facility with BO
Low NRA
Fails binocular accommodative facility with + lenses
Low MEM/FCC
Exofixation disparity
Management:
Primary approach = vision therapy for sensory motor function
Build BO fusion range
Secondary option = added lenses
over minus if IXT
prism (BI if >20pd)
Exodeviation: divergence excess
symptoms:
intermittent eye turn (turning out)
occasional near point asthenopia
child closes one eye in bright light
Newcastle control score:
useful for determining when ophthal referral is needed.
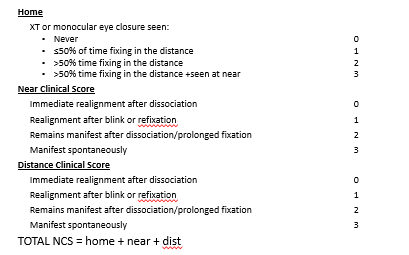
score 9 - full IXT.
problem - on review score may go up due to patients’ parents being more attentive in future.
alternate: IXT control scale
Signs:
Greater exophoria or IXT at D (compared with N)
High AC/A ratio
Suppression at D
Normal NPC
Fusional vergences may or may not be reduced
Normal stereopsis at N
Management:
Primary approach = vision therapy for sensory motor function
Create awareness of diplopia and then build BO fusion range
Secondary option = added lenses (over-minus if child <6 years)
Determine lowest ‘minus’ that will eliminate symptoms/normalise data
Promotes accommodative vergence to achieve alignment
two options:
-2.50D on top of cyclo refraction (not good for myopia management!!)
formula used to calculate the over minus. Considers accommodation and reserves.
Esodeviations: convergence excess
Symptoms: near work issues.
Asthenopia/HAs
Intermittent blur/diplopia
Worse at end of day
Burning/tearing
Inability to sustain and concentrate
Words move on the page
Sleepiness when reading
Decreased reading comprehension over time
Slow reading
May have symptoms of intermittent diplopia/blur/asthenopia at distance as well
Signs:
Significant esophoria at N
Reduced NFV
Reduced vergence facility with BI prism
Low PRA
Fails binocular accommodative facility with minus
High MEM/FCC
Esofixation disparity
Management:
Primary approach = added lenses (plus)
Lowest plus to eliminate symptoms/normalise data
Consider FCC/MEM or midpoint between NRA/PRA
Use AC/A as a guide
three ways
look at accommodative posture and aim to add plus to get to normal range (+0.50)
balance NRA and PRA
underaccommodating - PRA will be reduced compared to NRA
add shifts range
e.g., -1/+3 - balanced is -2/+2 → needs + 1 Add.
ESO and AC/A
aim for range to be half of their negative fusional vergence
use AC/A as a guide.
Secondary option = vision therapy
Aim to build negative fusional vergence (BI) range
quite difficult to teach divergence at distance.
Esodeviations: basic esophoria
Symptoms:
Asthenopia (D and N tasks)
Intermittent blur/diplopia (D and N)
Worse at end of day
Signs:
Esophoria of similar magnitude at D and N
Reduced NFV
Reduced vergence facility with BI
Low PRA
Fails binocular accommodative facility with minus
High MEM/FCC
Esofixation disparity
Management:
Primary approach = vision therapy and added lenses (plus)
Aim to normalise negative fusional vergence (BI) range (especially if no refractive error)
Added lens power may be moderately effect; lowest amount plus to eliminate symptoms/normalise optometric data
Consider NRA/PRA, MEM, AC/A
Secondary option = prism (BO)
May be considered if no plus refractive error correction indicated
Use fixation disparity measure to guide amount of BO prism to prescribe
Esodeviations: Divergence insufficiency
MUST EXLUDE OTHER PATHOLIGES - RED FLAG!
Symptoms:
Asthenopia (D tasks)
Intermittent blur/diplopia (D)
Worse at end of day
Generally long-standing (not acute symptoms)
Signs:
Esophoria greater at D (compared with N)
Reduced NFV
Reduced vergence facility with BI
Esofixation disparity
Management:
Primary approach = prism (BO)
Majority require relieving horizontal prism
Fixation disparity/associated phoria measure OR
Dissociated phoria and vergence range (1:1 rule – see later slides)
Secondary option = vision therapy
Aim to normalise negative fusional vergence (BI) range
May need to consider surgery if distance esotropia
Accommodative dysfunction: Accommodative insufficiency
Symptoms
Blurred near vision
Discomfort/strain associated with N tasks
Fatigue associated with N tasks
Difficulty with attention and concentration when reading
Signs
Low accommodative amplitude
Low PRA
Fails monocular and binocular accommodative facility with minus lenses
Esophoria at N
High MEM/FCC
Management
Primary approach = added lenses (plus)
Consider additional + at near based on MEM, PRA/NRA midpoint, FCC
Secondary option = vision therapy
Improve ability to stimulate accommodation and normalise amplitude of accommodation
Accommodative dysfunction: Accommodative excess
Symptoms:
asthenopia / HAs with near tasks
intermittent blurred distance vision
Signs:
Variable VA findings
Variable refraction (dry)
Low level of ATR astigmatism
Low MEM/FCC
Low NRA
Esophoria at N
Fails monocular and binocular accommodative facility with plus
Management:
Primary approach = vision therapy
Improve ability to relax accommodation
Accommodative dysfunction: Accommodative infacility
Symptoms
Difficulty focussing from D to N and N to D
Asthenopia with N tasks
Difficulty with attention and concentration when reading
Intermittent blur at N
Signs:
Fails binocular and monocular accommodative facility with plus and minus
Low PRA
Low NRA
Management
Primary approach = vision therapy
Improve ability to stimulate and relax accommodation
DONT OVERLY STUDY PARTS BELOW HERE!! (2 minutes)
Fusional vergence dysfunction
Symptoms
Asthenopia/HAs at N
Intermittent blur at N
Worse at end of day
Burning/tearing with N tasks
Inability to sustain and concentrate
Sleepiness when reading
Decreased reading comprehension over time
Slow reading
Signs: poor in both directions
Orthophoria or low eso/exophoria
Reduced NFV and PFV (D and N)
Reduced vergence facility (BI and BO)
Low PRA and NRA
Fails binocular accommodative facility with both plus and minus
Normal monocular accommodative facility
Management:
Primary approach = vision therapy
Establish normal PFV and NFV ranges and facility
Vertical Phoria
Symptoms
Blurred vision
Asthenopia/HAs
Diplopia
Car/motion sickness
Inability to attend and concentrate during sustained visual tasks
Sleepiness
Loses place when reading (returns to wrong line)
Signs:
Anomalous head position
Hyperphoria
Reduced PFV and NFV (horizontal)
Reduced vergence facility (BO and BI)
Vertical fusional vergence may be reduced or unusually large
Management:
Primary approach = vertical prism
Prescribe associated phoria (reduce fixation disparity to zero)
Secondary option = vision therapy
Extend vertical vergence ranges
not a good option / very hard
Ocular Motor Dysfunction
Symptoms:
Excessive head movement
Frequent loss of place
Omission of words
Skipping lines
Slow reading speed
Poor comprehension
Short attention span
Difficulty copying from board
Difficulty with tasks requiring columns of numbers (e.g. test sheets, maths)
Poor performance in sports
Signs:
Below 15th percentile on DEM test
Below 15th percentile on NSUCO tests
Management:
Primary approach = vision therapy
Improve large saccadic ability and small excursion/pursuit ability
Management options - NSBV
Added Lens Power:
Accommodative insufficiency - add plus
Convergence excess - add plus
Basic esophoria - add plus
Divergence excess or intermittent exotropia - add minus
Plus power:
AC/A is primary test to determine effectiveness of added lenses
If high AC/A, generally effective approach
E.g. 12 esophoria at N and AC/A ratio of 10:1; an addition of +1.00 expect 2 esophoria
Bifocal lens design is preferred (higher seg height in children)
Minus power:
Determine least amount of minus that allows fusion
1.00D – 2.50D
AC/A ratio is not critical factor
Single vision lens as fulltime wear
suited for really young children, and people without history of family myopia.
Prism Use:
Horizontal relieving prism
vertical relieving prism
Horizontal relieving prism:
Exophoria:
Sheard’s criterion: fusional reserve must be at least twice demand
Prism needed = 2/3(demand) – 1/3(reserve)
E.g. 10 exophoria at N, BO = 12/20/10
Prism required = 2/3(10) – 1/3(12) = 6.67 – 4 = 2.67Δ BI
one dioptre increments for left / right → prescribe 1pd right & 1 pd left.
Esophoria:
1:1 rule
BI recovery should be at least as great as amount of esophoria
BO required = (esophoria – BI recovery)/2
E.g. 12 esophoria at N, BI = 12/18/8
Prism required = (12 – 8)/2 = 2Δ BO
Percival’s criterion
Prism needed = 1/3 (greater lateral range blur limit) – 2/3 (lesser of lateral range blur limit)
E.g. BI = 26/30/20; BO = 6/14/8
Prism required = 1/3 (26) – 2/3 (6) = 4.66 BOΔ
Vertical relieving phoria:
Prescribe associated phoria measurement
I.e. amount of prism that reduces fixation disparity to zero
electronic charts with polarised lenses.
Conditions best managed with prism:
Divergence insufficiency - prism
Vertical heterophoria - prism
Vision therapy
Effective for:
Reducing symptoms
Increasing amplitude of accommodation
Increasing accommodative facility
Improving near point of convergence
Increasing fusional vergence amplitudes
Increasing fusional vergence facility
Eliminating suppression
Improving stereopsis
Improving accuracy of saccades and pursuits
Conditions best managed with vision therapy:
Convergence insufficiency
Divergence excess
Fusional vergence dysfunction
Basic exophoria
Accommodative excess
Accommodative infacility