Wounds
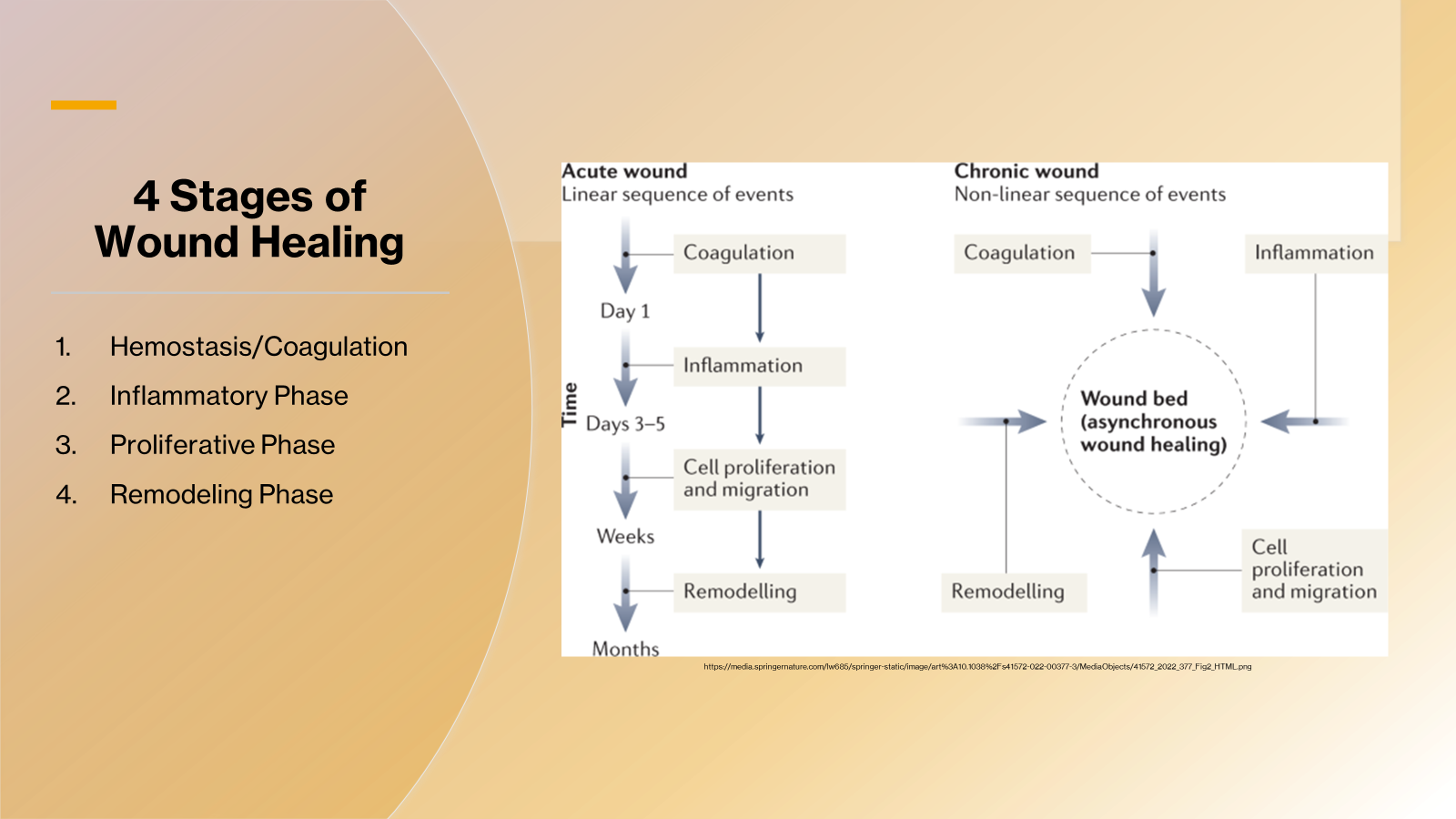
•4 Stages of Wound Healing
1.Hemostasis/Coagulation
2.Inflammatory Phase
3.Proliferative Phase
4.Remodeling Phase
•Stage 1 of Healing:
Hemostasis
•
•First response mechanism for injury. Lasts about 2 days.
•Vasoconstriction in area to inhibit blood flow and blood loss.
•Platelets are released coagulating with fibrin (fibrous protein) at the wound site. Platelets stick together to seal breaks in blood vessel walls.
•
•Stage 2 of Healing:
Inflammatory Phase
•
•Injury onset to day six
•Characteristics:
•Vascular changes
•Exudate from cells and blood vessels
•Clot formation
•Phagocytosis
•Early fibroblast activity
•
•Stage 3 of Healing:
Proliferative Phase
Granulation and Epithelialization
•
•Day 3 up to 6 weeks post onset
•Characteristics: granulation tissue formation
•Growth of capillary beds
•Collagen production
•Wound contraction
•Epithelialization
•
•Stage 4 of Healing:
Remodeling Phase
•
•Day 14 up to 10 weeks post onset
•Characteristics
•Maturation of collagen
•Contracture of scar tissue
•Remodeling of collagen
•Collagen aligns to stress
•
•Wound Assessment
1.Location
2.Size
3.Classification:
Depth of tissue involved:
•Superficial: epidermis
•Partial thickness: epidermis and dermis
•Full Thickness: epidermis, dermis and subcutaneous
Stage: Pressure ulcers
•Stage I-Skin is intact with non-blanchable erythema
•Stage II-Involves dermis and/or epidermis; ulcer is superficial and presents as an abrasion, blister, or shallow crater
•Stage III- Ulcer penetrates through epidermis and dermis to subcutaneous tissues
•Stage IV-Ulcer penetrates through subcutaneous tissue to muscle, tendon, and/or bone
•
4. Description of wound bed:
•Epithelial tissue: thin, shiny, translucent sheet of cells
•Granulation tissue:
•Tissue composed of blood vessels and collagen matrix.
•Healthy: beefy red, granular, shiny, moist
•Pal or dusky if infected or poorly vascularized
•Slough:
•A soft tissue composed of fibrin, protein, and wound drainage (exudate)
•Tan, yellow, white
•Stringy and mucous-like consistency
•Subcutaneous tissue:
•Healthy is pale yellow
•Necrotic is dark mustard yellow
•Muscle:
•Healthy is beefy red
•Necrotic is dull red
•Eschar:
•Hard dried necrotic tissue
•Brown or black
•
•
•Wound Assessment
5.Exudate: (drainage)
•Small amounts are normal
•None or scant leaves the tissue dry
•Moderate to copious amounts seen in chronic wounds, infected wounds and after aggressive debridement
•Color/consistency
•Serous: clear, pale yellow, or pink color and thin consistency are normal
•Serosanguinous: red color and thin consistency indicates some damaged blood vessels
•Yellow, tan, grey, or green color, and thick consistency indicate infection
•Red color and thick indicates trauma or infection
•
6.Condition of surrounding tissues:
•Color
•Degree of hydration
•Presence of hair
•Edema
•Temperature
•Texture and thickness
•Thin tissue will break down easily
•Thicken, callous like tissue around perimeter of wound blocks oxygen and nutrients to outer wound bed
7. Clinical signs of infection:
•Pain
•Redness
•Inflammation
•Edema
•Purulent drainage
•Presence of odor after cleansing
•Poor tissue quality
•Lack of decreased wound size for 2-4 weeks
•Elevated body temperature
•Malaise
•
•Stage I Pressure Ulcer
•Stage II Pressure Ulcer
•Stage III Pressure Ulcer
•Stage IV Pressure Ulcer
•Epithelium at Margins of Wound
•Healthy granulation tissue
•Granulating Wound
•Wound with 40% yellow slough
•Wound Bed Covered With Slough
•Wound bed covered with yellow slough
•Eschar
•Debridement of eschar
•Tunneling
•Biochemical Markers of PEM Defining Severity
•Key Elements in Effective Wound Care
·Ensure adequate nutrition
·Stabilize medical status
·Relieve pressure
·Remove devitalized tissue (debridement)
·Maintain a clean wound
·Maintain a moist wound environment
•
•Selective Debridement Techniques
Sharps:
•Use of scalpel, scissors or other sharp instruments to remove devitalized tissue
•Must be completed by PT
•Precautions/contraindications:
•Wounds d/t arterial insufficiency
•Low platelet count
•Anti-coagulant medications
•Gangrene
Enzymatic:
•Topical agents used to dissolve necrotic tissue
•US=Santyl (collagenase)
•Inactivated in presence of silver or iodine products
Autolytic:
•Necrotic tissue is digested by enzymes that are normal present in the wound
•Requires use of a dressing to hold drainage in the wound
•Contraindications: Arterial ulcer; Infection; Gangrene
Low Frequency Ultrasonic (20-100 KHz):
•Low frequency creates more powerful cavitation and acoustic streaming
•Benefits: Selective removal of necrotic tissue with preservation of granulation tissue
•Facilitates cleansing of tunneling and undermining
•Minimal blood loss
Biological:
•Maggot: Larva of greenbottle fly
•Digest bacteria and necrotic tissue
•Release enzymes that stimulate fibroblasts
•Contraindications:
•Dry wound
•Allergies to eggs, soybeans and fly larvae
•
•Non-Selective Debridement Techniques
Mechanical:
§Soft abrasion:
§use of gauze or cotton-tipped applicator to wipe in or around wound bed
§Wet-to-dry dressings:
·Gauze soaked in saline is applied to wound, then allowed to dry
·Dried gauze adheres to wound bed
·Dried gauze is removed, along with any adhered tissue (healthy or not)
·Often causes bleeding and pain; try to use another approach if possible
§Hydrotherapy:
§Cleanse wound of foreign matter
·Soften eschar
·Use for wounds with >50% necrotic tissue
§Pulsed lavage with suction
·Pressurized irrigation with suction at same time
·Reduces bacteria and epithelialization
·Flexible tip cleans into tracts, tunnels and undermined areas
·4-15 pounds per square inch (psi) cleanses tissue without forcing bacteria into tissue and without damaging viable tissue
Chemical:
§Use of powerful chemicals to remove bacteria, foreign matter, and necrotic tissue
§Goal is to soften and break down necrotic tissue separating it from healthy tissue
§Skin cleansers and anti-septic agents (Betadine, Hydrogen Peroxide)
·Should not be used on wounds with >50% granulation tissue as they have chemicals that are cytotoxic
·Should not be used with maceration or tunneling as chemicals become trapped in tissues
§Silver nitrate is used with hyper granulation tissue
•
•Benefits of Maintaining A Moist Wound Environment
•Wound Dressings
•Gauze Dressings
•
•Different Types of Gauze
•Cotton Gauze: Traditional gauze made from woven cotton fibers.
•Gauze Sponges: Small, square pieces of gauze, often used for cleaning wounds or absorbing exudate.
•Gauze Pads: Larger, flat pieces of gauze used to cover wounds.
•Impregnated Gauze: Gauze that has been treated with substances like antiseptics or medications to aid in wound healing.
•Mesh Gauze: Gauze with a mesh-like structure, often used for packing wounds.
•Non-Stick Dressings: Gauze designed to not adhere to the wound, minimizing trauma during dressing changes1.
•Gauze Rolls: Long strips of gauze used for wrapping around wounds or securing other dressings1.
•
•Wound Dressings
•Semi-permeable Film Dressings:
• Transparent polymer membrane coated with an adhesive acrylic layer
•Wound Dressings
•Semi-permeable Foam Dressings :
• Highly absorbent polyurethane
•Wound Dressings
•Hydrocolloids:
•Absorbent colloidal materials (pectin; gelatin) combined with elastomers and adhesives, backed with a layer of polyurethane film or foam
•Wound Dressings
•Hydrogels:
• Available either in gel form or in sheet form with polymer film backing
•Wound Dressings
•Calcium Alginates:
• Natural fiber dressings made from algae and kelp
Options To Enhance Wound Healing
·Vacuum Assisted Closure:
·Whirlpool
·Electrical Stimulation
·Ultrasound
·Diathermy
·Ultraviolet Light
•
•