Communitive Diseases and Immunizations
Role
RT TO VACCINES
proper hand hygiene
education benifits:
Improving the client’s health status
promoting autonomy and decision making
adoption of healthy lifestyle practices
Promoting client safety, especially regarding medications and the management of illnesses
Promoting client adherence to the prescribed treatment plan
Reducing client anxiety
Improving client outcomes
screen, assessment, population, vaccines,
education: vaccine-preventable diseases and their potential risks, emphasizing the benefits of timely immunization in safeguarding children's health.
Notifieable diseases Surveillance system:
Covid 19
Diphtheria
Giardiases
Heamophilus influenzea
Hep A/B/C
Meningitis
pertussis
poliomyelitis
rubella
tetanus
varicella
children have lost of hand-to mouth = higher risk of GI and resp infection
hand washing
correct isolation: standard and transmission-based percaution
standard = universal based that any thing may have contagious agent
preventive = PPE, hand hygene, safe inject
transition
droplet: agent <3ft or mucous membrane
do not remain infectous over long distances = no special ventilation
single room
face mask, and pt wear surgical mask if outside
pertussis, FLU, meningitis, adenovirous, Rhinovirus, group A strept
Contact: indirect and contact
single room
gown/gloves → removed receptacle immediately priors to child room
C. diff, VRE, MRSA
Airborne: micro that suspended in air → travel long distance
(-) pressure + N 95
TB, covid, rubeola
PPE
hand hygene
gown
mask
face shield
gloves
→
gloves
face shield
gown
face mask
hand hyegene
Chickenpox
VZV → remains in latent
by aerosolized virus or contact an open vesicle
upper resp tract (2-6 day) → blood stream → viremia in 10-12 → vesicle
IgG Y immunity
in sensory nerve → shingles
s/s: small, itchy blisters → scabs
fever, fatigue, sore throat, h/a, 5- 7 days
dx: s/s → sample from vesicles + blood sample for immune responds
tx: relief
acetaminophen = fever
pruritis = calamine lotion, lukewarm baking soda or oatmeal bath, antihistamine
cotton clothing, and avoid overheating w/ heavy blanket
trimming child fingernails
NO ASA due to Reye syndrome
hydration
antiviral if severe or low immune → abx if 2nd bacterial
keep child away from pregnant, newborn, compromised immune
AIRBORNE + cared for someone varicella
immunization, frequent hand wash (infected contact, avoid close contact)
Diphtheria
Corynebacterium diphtheriae = exotoxins → inflammation of throat + gray pseudomembrane in the throat and pharynx → thickens = occludes airway + toxins in lymph/ hematologic → myocarditis and neuritis
impacts => integumentary and resp
risk:
non-adherence = DTaP
more in tropical, crowded
s/s:
FLU s/s ( throat, fever, malaise, h/a, cervical lymphadenopathy) + gray pseudomembrane in the throat and pharynx
hx of endemic regions w/ 2-5d incubation
gray pseudomembrane in the throat and pharynx
lab/dx:
throat swab, PCR for type of bacteria,
tx:
abx (penicillin G)/ erythromycin, diphetheria antitoxin (DAT) → CHECK ALLERGY
hospitalization
soft diet, fluid, calm enviroment , emotional support/ distraction
DTaP
Mumps
paramyxoviridae → upper airway + regional lymph nodes → viremia = slalvary, gonad, (rare CNS) inflammation
highly contageous by droplet or infected saliva or fomites = mostly salivary glands + orchitis
s/s:
parotid salivary glands → fever, h/a, anorexia, myalgia, fatigue
→ orchitis, meningitis, encephalitis,
lab/dx: s/s → RT-PCR, buccal swab, IgM
tx:
MMR, bosters
restm adequate hydration, thermo pain relief, elevation (orchitis) OTC analgestic
soft diet, isolation, emotional support
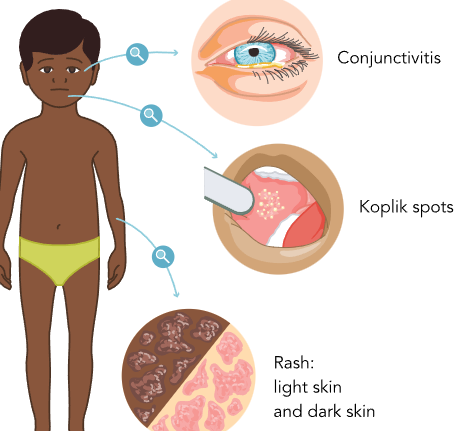
Measles (ruobela)
Morbillivirus: nasopharyngeal + conjuctival mucosa → regional lymph → spleen, liver, bone marrow → inflammation occurs in every cell attacked
direct contact or droplet (remian for 2 hrs)
fever, cough, rhinorrhea, conjutivitis → small, red spots w/ white center ( koplik) in mouth, hairline and downward rash
lab = s/s → serum or PCR (in outbreaks/ or atypical s/s)
most accurate = plaque reduction neutralization assay
tx: no viral tx
AIRBORN → nutrition, hydration, 2 day vit A sup
comfort = fever, resp
cool mist/ steamy for cough/ congestion
MMR + herd immunity
Poliomyelitis
mouth → GI = nasopharyngeal secretions and in stool
nervous system = paralysis (fecal-oral route but also contact/ sneeze)
from travelers and non vaccinated or weak immune
s/s = mild flue (2-5 days) → CNS = paralysis/ muscle weakness in legs (mild to complete loss) → resp failure
targets motor neurons in spine = loss of muscle control
lab/dx = assess s/s,
labs → throat swabs, stool, CSF = for virus and strain
MRI/ EMG for muscle function
early dx !!!!
tx:
mild = combact w/ immune
if paralusis or resp = PT, OT, orthopedic for skeletal deformities, resp support
nutrition/ hydration/ immunization
special devices (brace, wheelchair, orthopedic aid)
resp support, pain management, emotional support
immunization: inactive polio vaccine (IPV) or oral polio vaccine (OPV)
Covid
milder than adults
tissue damage + vs T cell, monocyte, neutrophil, cytokine
→ widespread response
direct contact/ resp (possible fecal-oral)
s/s: fever, cough, resp issue,
multisystem inflammatory syndrome in children (MIS-C) = inflammation of multiple organs
long term consequences after acute = fatigue, resp issue, neuro
dx: molecular, PCR/ rapid antigen/ nasopharyngeal sample collected, Y test
tx:
antiviral: remdesivir for hospitalized and required O2 or 3kgs or >28days
dor those >12y w/ 40kg mininum, mild-to moderate w/ risk of severe = ritonavir- nirtmatrelvir
O2, resp s/s, hydration/ nutrition
remote learning
good hand hygiene, air purify if possible, and wear a well-fitting mask for 5 days after testing positive, 6 feet
>6m old = immunization
Meningitis
Viral (aseptic)
entero, herpes, adenovirus → significant in <5yr _ immunocompromized
mouth/nose
found in fluids and stool → direct or indirect
being in close contant, crowded setting, weak immune
more in summer/fall
s/s:
infnat/ young:
Fever/ Hypothermia (in newborns)
Irritability (crying, difficult to console) →Poor eating or vomiting
Lethargy/ Sleepiness or difficult to awaken
Full or bulging anterior fontanel
older children:
Fever
N/V
Photophobia, Diplopia or blurred vision
H/A
Nuchal rigidity
Irritability
Lethargy
lab/dx:
lumbar puncture = CSF for cell count, protein, glucose + culute → PCR
tx:
emperic abx even viral since takes 48hrs for results
if not → acyclovir
DROPLET abx 24hrs
I/O for dehydration due to vomiting/ fever, oral fluid → IV for fluid
fever/ discomfort w/ antipyretics + cool compress
low stimuli
E/I = low Na ~ SIADH
neuro check (PERRLA, LOC) + ICP + seizure
good hygene, no close contanct w/ those w/ infection
bacterial
meningococcus, pneumococcus, GBS, Hib
from saliva, nasal discharge, feces, sharing drink, utensil, person items w/ infected
communal setting, unvaccinated, low immune
nasopharynx/ URI (sinusitis. otitis media) → bacteremia → BBB
s/s: ~ to viral but can → sepsis, hearing loss, hydrocephalus, death
Brudzinski: involuntary flexion of knees when passive neck flexion
kernig: pain while exteding knee and pt is supine while hips are flexed
→ diff to elicit in young/ even if (-), cna still be meningitis
meningoccoccal → petechial rash → if not tx = necrosis of underlying rash tissue
lab:
viral<bacterial (>1k) WBC
mild protein < elevated
glucose normal > less than 40
tx: → hospitalization + early dx!!!
emperic abx → dx → abx adjusted
reduce fever, discomfort (corticosteroids reduce inflammation,) check hearing loss
exposed use prophylaxis ~ 3feet
check worsen ICP
dark enviroment, HOB 30, body alignement neutral
meningococcla, pneumococcal, Hib vaccine
Hepatits
A/B liver failure , C = chronic infection
A= food/water , B/C= bloodborn/ body fluids
risk factors = unsafe sex, IV drug, inadequate sanitation, exposure to infected fluids
s/s: fatigue, fever, jaundice, anorexia, abd pain, nausea, dark urine
A= more GI (n/v, diahrrea)
B = phases
prodromal = non specific → malaise, decreased appetite, RUQ pain
icteric: RT hepatic → jaudice, hepatomegalu, pale stool, dark urine
→ recover or chronic
C = no s/s if not then malaise/ low appetite
lab:
chronic = liver bipsy
Hep A= blood test and Y status
B= based on acute/ chronic = surface antigen (HBAg), or Y
Hep C = anti HCV and liver biopsy
tx: low s/s + complications ( chronic = low viral load)
antiviral
immunomodulator
liver transplant
regular monitoring, lifetyle and Rx adherance
A= supportive → hospitalization to manage dehydration or liver failure
B= acute is supportive + lamivudine ( !!!) / chronic = antoetroviral
ADR: h/a, nausea, fatigue, infection
C = since no s/s = usually fine
if chronic - interferon alfa-2b (immunomodulator) IM/ subq
ADR = alopecia
hydration, nutrition, rest
immunization: Hep A/B,
hygiene (handwash/ sanitation) → Hep A
C= use sterile needle/ avoid contact w/ infected blood
Mononucleosis
Epstein-Barr virus (EBV) from saliva → B lymph of oropharyngeal → spreads to lymphatic synstek → nodes, liver, spleen inflammation (long incubation of 3-6week)
“kissing disease”
s/s:
fever, fatigue, lymphadenopathy, h/a, malaise
enlarged tonsils w/ exudate patches
splenomegaly or hepatosplenomegaly
~→ airway obstruction, splenic rutpture, Guillain- Barre syndrome
lab/dx: heerophile Y test (monospot) + WBC of high lymphocytes
tx:no antiviral so alleviate s/s
rest,hydration, pain relief for pharyngitis, fever
no active/ contact sports for 4-6 w due to possible slepic rupture + infor on s/s → HCP
gargling warm water w/ sal or throat lozenges, regurlar moniotring
educate hygiene, no sharing cups or utensils
Roseola Infantum (exanthem Subitum)
“sixth disease” herpe virus (HHV-6)
leukocyte cell in salivary gland → febrile seizure due to enter of BBB
saliva contact and rRESP DROPLET
more in<2yrss/
onset fever of (40C) =3-5days
irritable w/ periorbital edema, otalgia, anorexia, mild URI (corugh, rhinorrhea, cervical lymphoedenopathy)
rash: small, rose- pink, maculopapular rash → spread in neck, face, and extremeties but non- pruritic = wash hands to prevent transmission
lab: ~ fever and rash
tx:
well-hydrated, providing fecer-reducing, calm/ reassuring, limit contact w/ other children (until 24hr to prevent),
hydration, dress in loose, lightweight, clothing to not overheat, call 911
naturally acquired infection
Fifth Disease (Erythema Infectiosum)
human parvovirus B19 “ fifth disease” , DROPLET or contact blood
more in 2nd trimester and SC
s/s: FLU-like = fever, malaise, h/a, myalgia, GI
slapped-cheek rash by non-pruritic maculapapular rash , net-like pattern in trunk and limbs (5 days)
arthtopathy for 3 week
lab/dx: serology and B19 IgM Y
tx:
s/s, can resolve w/o tx
fever, sore, rash comfort, hydrated,
keep child at home for a week,
rash is not itchy and is not contageous
immunity after infection is long lasting + no vaccine
hand, foot, mouth disease (HFMD)
enterovirus, cozxackievirus → resp tract, oral secretion, or vesicle fluid
enter mouth → lymoh tissue in lower intestine + pharyn - regional lymph
→ skin, CNS, heart, liver
6 weeks post-infection in stool and oropharynx sheed in 4 week
transmission:
oral-fecal
direct/ indirect
close contact or w/ oral, nassal secretion, fluid vesicles
more in summer, and both adult and 5yr old
s/s:
low-grade fever, sore throat, malaise, exanthem of shallow ulcer sores (widespread rash) w/ red borders and white/ gray-yellow bases
maculopapular or vesicular rash (hands, feet, small, red spots, blister) in buttocks, perineum, arms, legs
lab: distinguish from VZV, and herpes from microscopy bipsy or vesicular scrap, stool sample
tx:smooth for mouth pain (cold foods/ liquid)
can become meningitis/ encephalitis
CONTACT, fever, hydration, nutrition (of soothing foods from mouth ulcer and irritation),
avoid hot beverages/ acidic fruit and juice
popsicles are best
rest, comfortable clothing
hygiene, cleanliness and communlal areas, no Rx or vaccines
impetigo
high contagious + honey colored crusted facial leasion
primary: area infection in area not impacted/ second = bacterium w/ estblish wound
bullous/ non bullous
(group A- beta-hemolytic strep/ Staph. aureus)bacteria → fibronectin recptors → bacterial colonization
s/s: in integumentary
nonbulluos (common) = honey-crusted in vesicular/ pustular form in face + lymphadenopathy
bullous by large bullae (blister) → small vesicel → large blister = clear/ yellow into purulent or dark in color but hiney crust does not form + ~ lymphadenopathy/ fever
lab: s/s + bacterial culture and bipsy
tx:
abx (tpical)= mupirocin
oral abx = cephalexin (for nobullous) due to # of satellite lesions and system s/s + bullous
decrease rheumatic fever, education on acute post-strep glomerulonepphritis
correct application of abx = clean crust tw/ soap/water then topical abx
wash clothing and bed linen to prevent re-infection
cover lesion and contact w/ other avoided
conjutivitis
bacterial
moraxella catarhalis, Strept. pneumoniae, Haemophilus influenzae w/ close contact or touch object w/ bacteria then touching eye
vertical transmission of Chlamydia from vaginal birth
close contact w/ contagious person, inadequate hand hygiene, pre0existing ocular condition (SJS), wear contact lenses adn if do not properly celan or sleep w/ them
s/s: engorgement of blood vessel in conjuctival lining from pink/red appearance of conjusctiva and formation of purulent drainage
scelreal red, purelent disharge (stick to eyelash), eye irritation
lab: eye exam, sample of disharge for bacterial culture
tx:
topical abx eye drop or ointment = ciprofloxacin ophthalmic
hygiene, cool/warm compress over closed eyelid (use celan each time)
OTC artificial tears dut not for those to reduce redness
clean water/ sterile, avoid eye rubbing, no sharing personal items
viral
adenovrius, but also herpes, enterovirus → dilation
~ w/ URI and hand-to eye contact or w/ contaminated surfaces
s/s:
red sclera, watery disharge, itching/ tearing
hx of resp and HSV if vesicles in face or eyelid
lab: s/s and ELISA
tx: no antiviral
artifical tears, cool compress
if herpes → eye drop = acyclovir/ ganciclovir
HSV can cause damage to cornea, uvea, retina → blindness
no eye touch/ rub, temporarily isolate child
allergic
from pollen, air pollution, pet dander = IgE → mast cell degranulation = inflammation
~ + rhinitis or asthmas
s/s: red, itchy, eyelid edma, burning/ eye discomfort + no disharge
lab = hx of allergy, s/s → allergy testing
tx: antihistamine or mast-cell stabilizing eye drop → if severe =oral
epinastine
cool compressm allergen avoidance (purifiers, windows closed during pollen peak, and avoid outdoos)
rinse eyes w/ cool, clean water, OTC tears
refrain from rubbing eye
can have allergy shots
forein body
like wood, snadm dust → red, tear, flush, gritty → when removed= no more s/s
lab: conduct eye assessment, potential irritant, anesthetic eye drops w/ pain, fluorescein dye stain to assess corneala abrasion
tx:
flush w/ water or sterile solution, artifical tears
flsuh for chemincal
remove object w/ soft dacial tissue → if not able to remove = ER
NSAID
wearing protective eyewear
Stomatitis
herpetic gingivostomatitis
mouth and gums by HSV → s/s herpetic lesion and ganglia infection = herpetic gingivostomatitis from HSV-1/2
direct contact w/ saliva/ lesions
s/s:
painful vesicular osres or ulcers on gums, tongue, inside cheeks → swollen/ bleeding gums, high fever, irritability, diff eating/ drinking
lab: s/s but use viral culture of ulcer tissue and confirm presence of HSV
tx: acyclovir or IV
hygiene, dehydration, pain releif,
aphthous stomatitis (Canker Sore)
canker sores = recurrent inflammattory condition for oral mucosa
T-cell lymph and cytokine tumor necrosis factor alpha
stress, nutritional deficiency, trauma, family hx, strep. snaguinis
s/s: painful, flat, round-shaped ulcers,\ white-gray/ yellow center/ red border
in inner lining lips, cheeks, tongue, floor mouth
small, ranging mll to 2-3 cm
not contagious but 10yr of age
lab: s/s, if ulcer → biopsy
tx: topical analgesic/
avoid spicy, acidic = discomfort/ quit cmolimg
corticosteroid ( triamcinolone acetonide)
antibacterial/ anesthetic mouthwashas, systemic costicosteriois
soft toothbrush, avoid abravive toothpaste
rising mouth/ warm saline solution, hydration, OTC pain med
stress reduction technique (avoid trigger), vit B/C/ zinc
Immunotherapy terms
Antibody: y protien w/ two heavy cahins and two light chains
neutralize, tag for destruction (opsonization), trigger complement system, enhance immune response, stimulate immune cells to target cells through antibody-dependent cellular cytotoxicity (ADCC)
IgG = most abbundant + long term
IgM= fist to be produce during infection
IgA = in body secretions (localized)
IgE= allergic/ parasites
IgD= precise → less understood on B cells
when B cells find presence of antigen (memory are for future attacks)
for vaccine, dx test (for past or present infeciton), Y-therapy for autoimmune, cancer, covid
Antigen: provoke immune response from parts od organism or non-infections (allergy)
lock and key w/ Y
stim T cell (recognize other intracellular pathogen)
foreing or autoantigen
dx: indenify infection or autoimmune,
vaccines w/ harmless antigen to stim Y
antitoxin: Y for toxin → neutralize and eliminate toxin from system
for toxin-related illness and posioning
→ botulism, tetanus, snake bites
passive immunity
attenuate: process of reducing virulence while maintianing its ability to induce immmune response → vaccine
methods:
passage from diff host/ culture → adapt = reduce ability to cause severe illness
expose to physcial or chem agents
good for long-lasting immune but not for weakned immune systems
for measles, mumps, rubella, chickenpox
cocooning: create protective barrier though immunization of close contacts and parents from immunecompromized, or newborns, or unable to receive vaccines
→ vs covid, FLU, pertussis
immunity:
natural: innate from body mecahnics (rapid/ nonspecific
→ barriers, immune cells (macrophages, neutrophil, NK), inflammation,
not long term
acquired:
active = from exposure naturally or artificially (temporary)
passive: when immune cells or Y are transferred
for long term
herd: large % of population is immune and harder for patho to spread and protect immunocompromised (95%) to prevent outbreaks
methods:
immunization campaign
can face vaccine hesitency, limited access, waning immunity
Immunobiologics
tx from biological source (cell, tissue, immune cell component)
vaccines
immunomodulators = modify immune
for over reactive immune (autoimmune) or underreactive
nonoclonal Y (mAbs) = lab Y to target for cancer, autoimmune, infectious
cell-based therapy: utilize immune cells to target cancer or pathogen
adoptive T-cell
immunization
eradication or near-elimination of small pox, polio, measles, mumps, rubella, diptheria
rotuine ummunization
helps w. personal immunity while helping herd immunity
mRNA vaccine for rapid threats like Covid
barrriers: hesitancy, limited access, misinformation
Y therapy: healthy donors for Kawasaki disease to severe combined immunodeficiency disorders (SCID)
IV IG, injection (hepatitis B IG)
toxoids: vaccine vs toxins
chemical or heat to weaken/ deactivate
diphtheria/ tetanus
vaccine types
combination: multiple into one
→ reduce # of injections, streamline immunization schedules, clinic visits, improve adherence, ensure coverage
measles, mumps, rubella, diphetheria, tetanus, pertussis, polio, hep B, Hib
but requires extensive testing
conjugate: enhance immune response vs bateria that have polysaccharide capsules since they inc virulence
attach polysaccharide antigen to carrier proten → then immune system recognize
Strep, pneumonie, Hib, Neisseria meningitidis
usually required booster
monovalnet= for specific pathogen, usually for diff strains each year ( FLU, covid)
polyvalent: multiple strains of pathogent or RT pathogen (FLU)
FLU
Common vaccines
consideration = check C/I/ precaution
ADR/ guidelines/ type (IM)
precaution inc risk of ADR
mild illness should not delay immunization
Hib:
for <5y
2 and 4 m or 6m → booster of 12-15m = 3-4 doeses
IM in vastus lateralis
ADR: erythema, edema in site, fever
not foor under 6 e
Hep:
A:
2 doses = 12-23m → 6 m between 6-11 months of travelling
early adm of single does does not exclude infants from receiving tarditional
B:
3 dose= 24hr → 1-2m → 6-18 m → in combination
specialized scedules if LBW and parent w/ HbsAg +
mild fever
Polio:
inactivated poliovirus vaccine (IPV):
2m → 4m → 6-18m → 4-6yr = 6m period
deloid if 1yr or older
oral polio vaccine (OPV)
not recommended since can get polio if immunocompromised and is live
some formulations may have stroptomycin, polymyxin B, neomycin fo check allergy
C/I = acute febrile illness
pneumococcal: vs Strep penumoniae
penumococcal conjugate vaccine (PCV)
3 doses= 2→ 4 → 6 months → 12-15m
may need boster
pneumococcal polysaccharide vaccine (PPSV) = after PCV for immunocompromised
IV
ADR: soreness in injection, fever, sleep alteration
monitor for 1st 15 mins
rotavirus: live-attenuated vaccine =oral drop
2→ 4m = 2 doses → 6m = if 3 doses
started before 15 w and not after 8 m
usually due to GI
C/I = intussusception, SCID
mild: irritability/ temporary mild diarrhea vomit → can cause intussusception’
varicella:
12-15m → 4-6 yr
varicella or MMR/ varicella
IM or sub q for 12m<
C/I = pregnancy, immunosuppression, allergy for gelatin, neomycin,
injection site sorem milkd rash, low-grade fever
febrile seizure, pneumonia
DTaP
DTap <7y / Tdap >7y
DTaP = 2,4,6m → booster = 15-18m → 4-6yr
Tdap = 11-12yr → booster q10yr
IM
C/I: severe allergic ; precaution = Guillain-Barre or severe pain or swell
MMR
12-15m → 4-6yr
stand alone or w/ varicella
is subq
C/I= preg, immunocompromise, seere allergy
ADR = fever, mild rash → febrile seizure
No relation to ASD
HPV: for 9-45yr
11-12yr → 6-12m apart (rec to 9-14yr)
or 3 dose = 15-45yr →1/2m apart → 6 m apart
ADR: injection site pain or swelling, temperature elevation, headache, nausea, or muscle or joint pain, syncope
Allergy to yeast
meningococcal:
ACWY → 11-12y → booster 16y
B= 16-8yr
ADR: erythema, swelling, and soreness at the injection site; fatigue; and headache
FLU: for 6m or older
→ 9yr < require annual
if <9y = 1month apart = 2 years apart
if under 9 = received 2 doses = anually
3-35m = 0.25mL/0.5mL → 3yr = 0.5mL
live-attenuated influenza vaccine (LAIV), nasal spray vaccine
C/I = egg, LAIV = gelatine, immunosupress, ASA, whezzing in past yr
low grade fever
COVID -19= 6m or older
6m-4yr for 2-3 doses
5-11yr → one-series
unvaccinated 12yr ager = receive updated
1 annual booster w/ 8weeks
ADR: site reaction, fever, myalgia, and irritability among young children, myocarditis, adolescent for syncope for 15min,
c/i: hx of allergic,
percautions: myocarditits, pericarditis,
parasites
from protozoa, to helminths, arthopods
from food, water, insect bites, infected individuals, exposure of contaminated soil
malaria , amoebasis, giardiasis, helminthic infection
prevention, accurate dx/ tx,
proper sanitation, access to clean water, vector control, reduce exposure,
tx: antiparasitic, supportive care, alleviate s/s
scabies
Sarcotes scabiei mite = survive 1-2m and latch eggs for 2-3w
direct contact of 10 mins
mites burrowing eggs = intense itching, inflammatory especially at night → wrist, genital, interdigital spaces
rash of tiny, linear burrow/ erythematous papule → impetigo or cellulitis
lab: examination, skin scraping,
tx: permethrin cream → relieve + eradicate
not for 2 month old, or any close mucosa,
~ SOB if allergy w/ ragweed
use gloves → remove cream 8-14hrs
shampoo → dry → apply → 10 mins
proper handwashing, avoiding skin-to-skin contact, laundering contaminated clothing and bedding in hot water, and implementing isolation measures in institutional settings help prevent the spread of scabies.
vaccuming furniture, trimming child fingernails, cool baths,
monitoring
lice
pruritis due to hypersensitivity → develop in 2-6 week
feed of human blood, spread through close contact, sharing personal combs, hats, bedding
small, red bums from scratch
→ visible nits
lab → s/s or wood lamp
tx: OTC, or RX shampoo, lotion, creams
→ permethrin, two step = apply → 1week then reapply
→ lindane, ivermectin can give neurotoxicity
fine-tooth comb, infested clothing, bedding, personal items in hot water to eliminate lice
trimming fingernails, all household members checked for lice
avoid close contact w/ infected individual, regular inspection
pinworm (enterobiasis)
egg → GI hatch 4-8w → anal opening
small, white, thread like parasitic worm from ingestion by hands, bedding, clothing, surface,
s/s: itching around anus, disturbed sleep, abd discomfort
lab → perianal area using transparent aghesive test or pinworm paddle = collect early morning
tx:
mebendazole → follow up 2 weeks later
not w. metronidazole, repeat dose in 2 week
wash hands after toilet, disinfect living spaces, trim fingernals, shower in morning to remove deposited eggs, laundering bedding, clothing and towel in hot water
giardiasis
GI: diarrhea, impaired absorption due to alterations of epithelial cells
poor sanitation or contaminated water sources → water/food due to fecal-oral
water sources, inadequate hgiene practices, contact w/ infected
as/s or
→ diaherrea, abd cramps, bloating, gas, fatigie, weight loss
may resolve on its own
lab: 3 seperate stool samples in Giardia cysts/ trophozoites over several days w/ DFA or EIAs
tx:
metroniadazole, proper hydration/nutrition, or IV fluid replacement
hand hyegene, proper sanitation, safe drinking water,
dairy sensitiity after infection
use water filters or boil water