Trauma
CHAPTER 27
The Kinetics of Trauma
The mechanism of injury (MOI) is how a person is injured.
Kinetic energy is the energy contained in a moving body
Mass × velocity2
2
Kinetic energy
Velocity is the more significant factory in determining the amount of kinetic energy.
Estimate the speed of the objects involved.
Motor vehicle collisions
Penetrating trauma
Acceleration and deceleration
A body at rest will remain at rest, and a body in motion will remain in motion, unless acted upon by an outside force.
A faster change of speed (acceleration or deceleration) results in more force exerted.
Three types of impacts in a vehicle collision
Energy is absorbed in each impact.
There can be multiple impacts of each type.
Vehicle collision
Body collision
Organ collision
Mechanisms of Injury
MOI provides a suspicion of injury; not an accurate indicator of injury.
You must assess the patient for indictors of injury.
Common MOIs include:
Vehicle collisions
Have a high suspicion of injury when there is:
Evidence of high speed collision
Death of another vehicle occupant
Altered mental status
Intrusion larger than 12 inches at occupant site; larger than 18 inches at any site
Ejection
Rear impact
Initially, the head and neck are whipped back.
A properly adjusted headrest and seat belts reduce injury.
Subsequent injury can follow an up-and-over or down-and-under pathway.
Rotational or rollover crash
Injury patterns are less predictable.
In rollovers there are multiple impacts and changes in direction.
Multisystem trauma is common.
Ejection is common with rollover; crushing injuries to ejected occupants are common.
Vehicle-pedestrian
Extent of injury depends on:
Vehicle speed
What part of the body is hit
How far the pedestrian was thrown
The surface the pedestrian landed on
The body part that first struck the ground
Motorcycle collisions
Helmet use is a significant factor in reducing morbidity and mortality.
Impacts may be head-on or angular, and may involve ejection.
Laying the bike down can result in severe abrasions and burns.
Falls
The most common mechanism of injury
Severity of trauma depends on several factors.
Distance
Surface
Body part impacted first
A severe fall is:
>20 feet in an adult
>10 feet or two to three times the height in a child
Penetrating injuries (gunshots, stabbings)
Gunshot wounds
90% of fatal wounds involve the head, thorax, and abdomen.
Explosions
The Golden Period and Platinum Ten Minutes
The best chances of survival from trauma occurs when intervention takes place as quickly as possible.
The goal is for EMS providers to limit scene time to 10 minutes with severely injured patients.
The Trauma System
Level I – Regional Trauma Center
Level II – Area Trauma Center
Level III – Community Trauma Center
Level IV – Trauma Facility
CHAPTER 28
Bleeding can be a life-threatening emergency.
Severe bleeding is controlled in the primary assessment.
Most soft tissue injuries are cared for after the primary assessment.
Recognizing shock is an important element of emergency care.
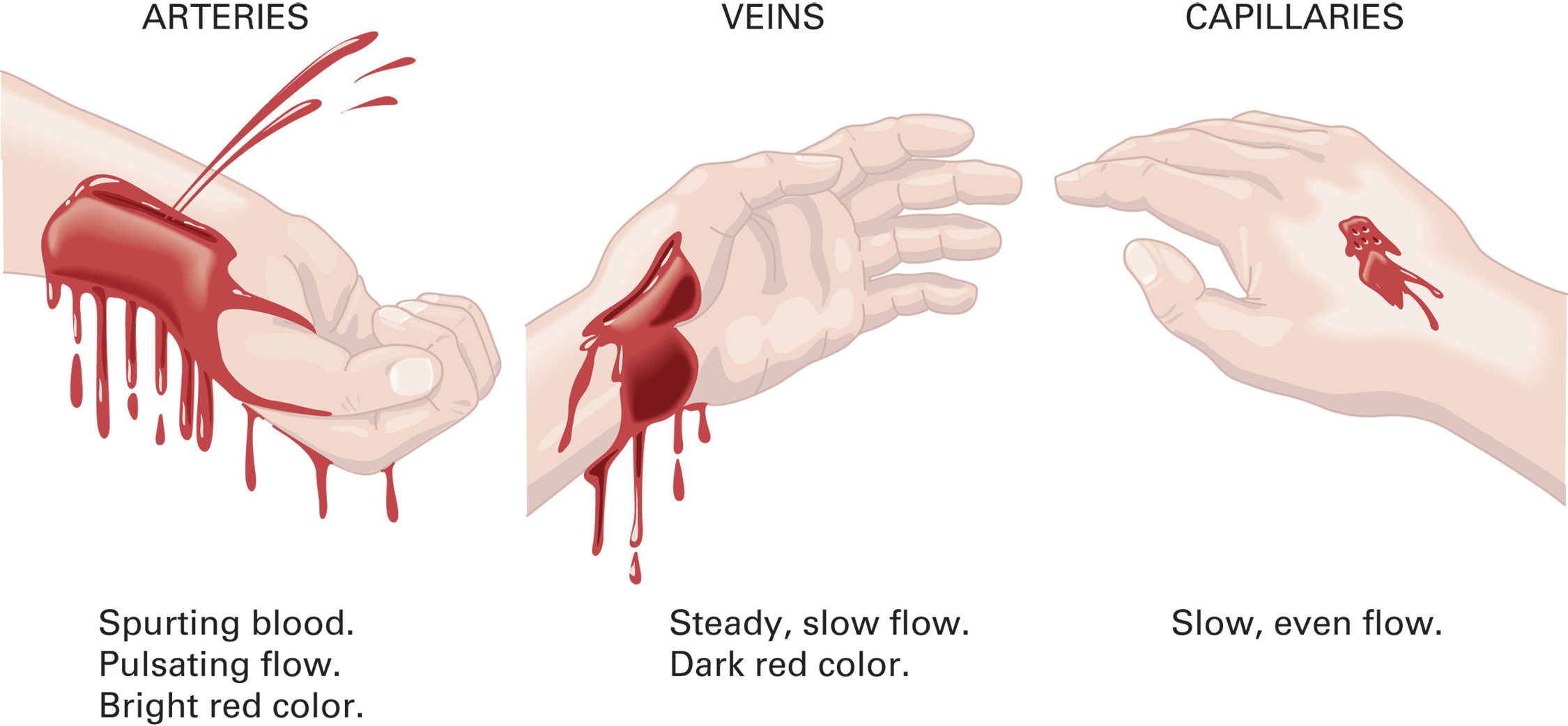
External Bleeding
The severity of blood loss depends upon the following:
Amount of blood loss
Rate of blood loss
Other injuries or existing conditions
Patient’s existing medical problems
Patient’s age.
The best way to estimate blood loss is by assessing the patient’s signs and symptoms.
Methods of Controlling External Bleeding
Steps to Control Bleeding
Apply direct pressure.
Direct Pressure
This is the first method to use to control bleeding.
A pressure dressing can be used.
Do not apply pressure to or remove impaled objects.
Apply a pressure dressing.
Apply a tourniquet.
Tourniquets
Tourniquets are used when direct pressure does not control bleeding.
There are several types of commercial tourniquets.
Tourniquets can be improvised if a commercial tourniquet is not available.
If a tourniquet can’t be used, consider using a hemostatic agent.
If multiple patients are hemorrhaging (i.e. M C I), proceed immediately to Step 3.
Splints
Splinting is an important way to reduce bleeding from an injured extremity.
A traction splint can be helpful for a fractured femur.
Do not delay splinting at the scene with an unstable patient.
Hemostatic Agents
These agents can be used when direct pressure is ineffective.
Hemostatic agents promote blood clotting.
Their use is generally reserved for long transport times.
There are some associated complications.
Junctional Bleeding Control
Junctional areas are where the extremities (and head) meet the torso.
Traditional tourniquets cannot be used.
There are devices used by military for these types of injures, but they are not yet approved for civilian use in E M S.
Assessment-Based Approach-External Bleeding
Scene Size-Up
Scene safety
Standard precautions
M O I /N O I
Number of patients
Additional resources
Primary Assessment
Assess the airway and breathing.
Maintain S p O2 of 94% or above.
Assess the pulses and skin.
Control bleeding, but do not let dramatic injuries distract you from the primary assessment.
Perform a rapid secondary assessment if:
There is significant bleeding.
The patient has an altered mental status.
There are multiple injuries.
There is a significant mechanism of injury.
Obtain baseline vital signs.
Assess for signs of hypoperfusion.
Emergency Medical Care
Maintain airway and ventilations.
Keep pulse oximeter >94%
Control bleeding with direct pressure.
If direct pressure is ineffective, apply a tourniquet.
Provide care for shock.
Immobilize injured extremities.
Reassess.
Bleeding from the Nose, Ears, or Mouth
This may indicate the following:
Skull injury or facial trauma
Digital trauma to the nose
Sinusitis
Hypertension
Clotting disorders
Esophageal disease.
Do not attempt to control bleeding from the ears or nose if the patient has experienced a head injury.
Epistaxis is controlled by direct pressure.
Internal Bleeding
Internal bleeding may result from trauma or medical problems.
Internal bleeding may not be obvious and can rapidly result in death.
Severity
Common sources of internal bleeding are injured organs and fractured extremities.
A hematoma is a contained collection of blood that can contain a significant amount of blood.
Use signs and symptoms to estimate the severity of blood loss.
Assessment-Based Approach-Internal Bleeding
Scene Size-Up and Primary Assessment
Perform a scene size-up; look for a mechanism of injury.
Form a general impression.
Immediately control major external bleeding.
Pay close attention to the patient’s mental status.
Assess airway, breathing, and oxygenation.
Assess the pulses, skin, and capillary refill.
Pay attention to changes in the respirations, pulse, and skin that can indicate blood loss.
Secondary Assessment
Perform a rapid secondary assessment if the mechanism of injury and assessment suggest internal bleeding.
Signs and Symptoms
Contusions
Abrasions
Deformity
Impact marks
Swelling
Signs and symptoms of internal bleeding include:
Pain, tenderness, swelling, discoloration
Bleeding from a bodily orifice
Vomiting, bright red or coffee-ground material
Hypotension or a narrowing pulse pressure
Nausea, vomiting.
Additional signs and symptoms of internal bleeding or hemorrhagic shock include:
Anxiety, restlessness, combativeness, altered mental status
Weakness, faintness, dizziness
Tachycardia, tachypnea.
Emergency Medical Care
Maintain airway and ventilations.
Keep pulse oximeter >94%
Control bleeding with direct pressure.
If direct pressure is ineffective, apply a tourniquet.
Provide care for shock.
Factors That May Increase Bleeding
Movement
Low body temperature
Medications
Intravenous fluids
Removal of dressings and bandages
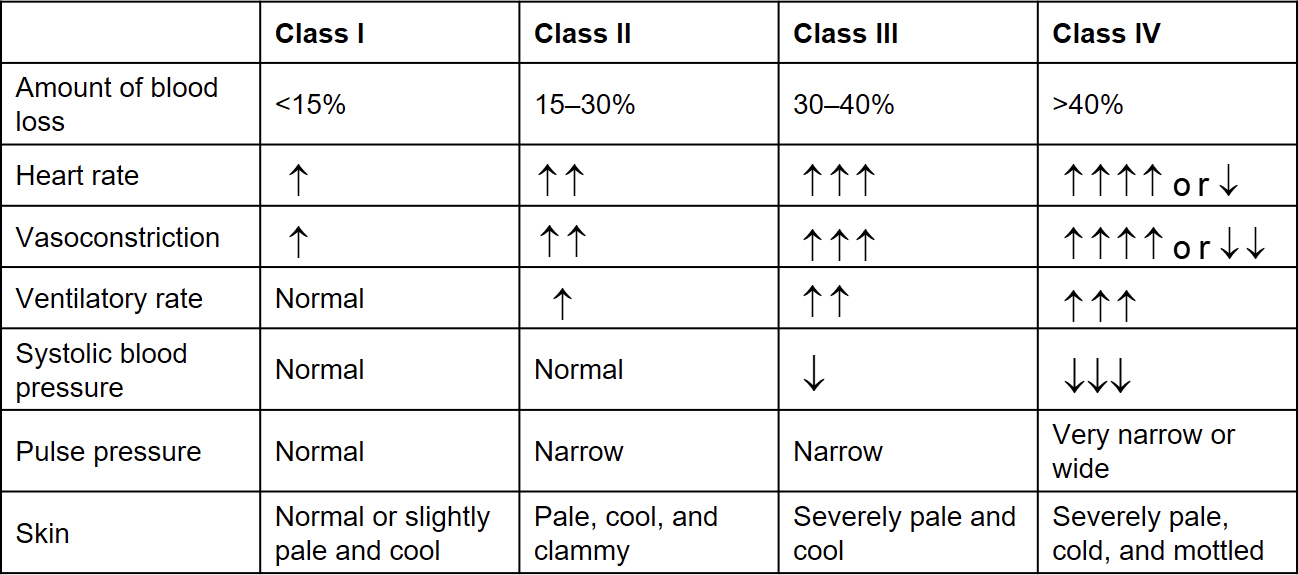
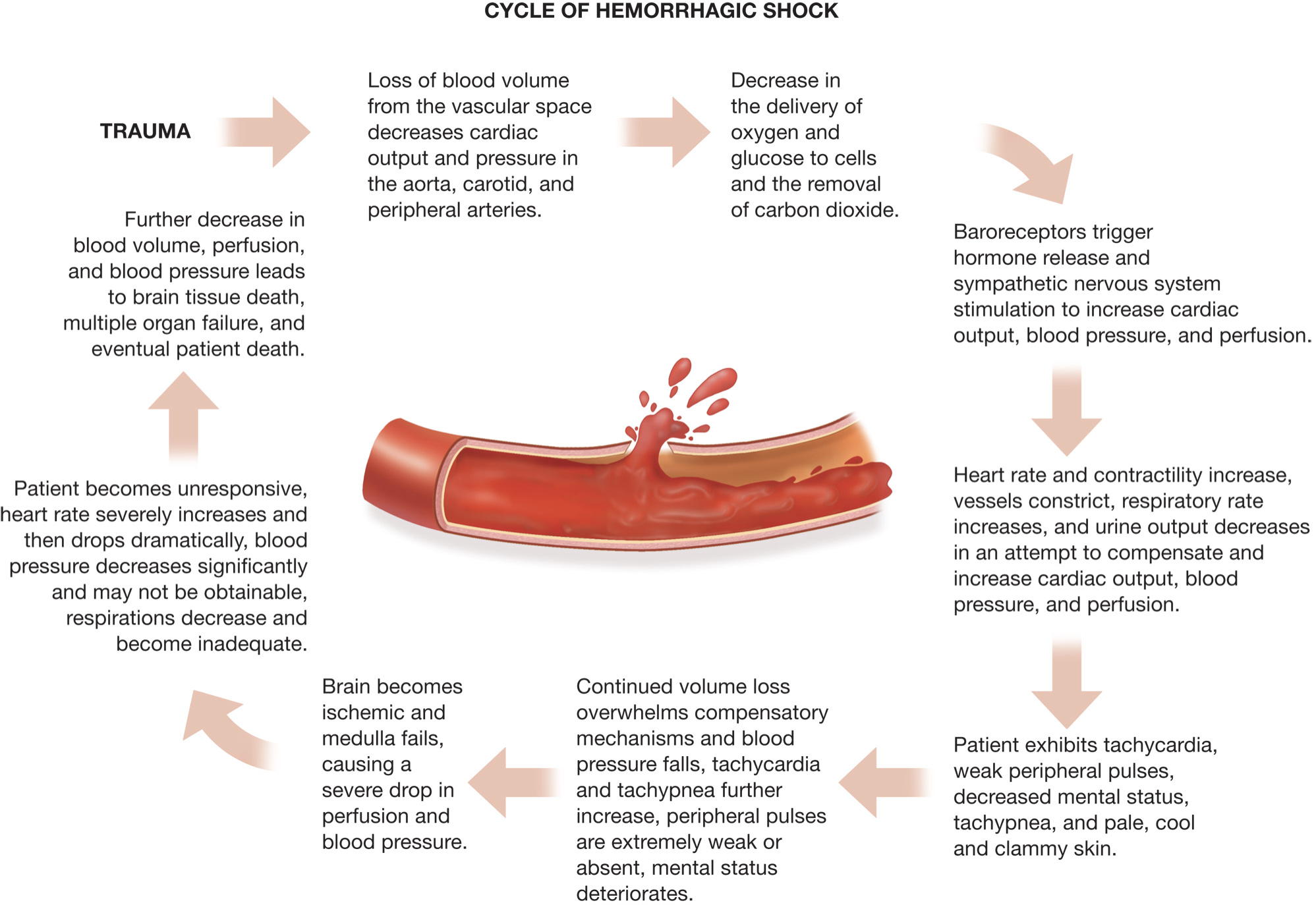
Hemorrhagic Shock
Shock results from inadequate tissue perfusion.
Significant hemorrhaging leads to inadequate perfusion.
Cells are deprived of oxygen and nutrients and begin to fail and die.
Immediate recognition and treatment are critical.
Assessment-Based Approach- Hemorrhagic Shock
Scene Size-Up
Primary Assessment
Secondary Assessment
Secondary Assessment
Signs and Symptoms
Mental status changes
Decreased peripheral perfusion
Vital sign changes and narrowed pulse pressure
Dilated pupils, nausea/vomiting, thirst
Physical Exam
Vital Signs
Reassessment
Emergency Medical Care
Maintain an open airway, administer oxygen, and assist ventilations as needed.
Control external bleeding.
Splint injuries as appropriate.
Place patient supine and treat for shock.
Transport the patient rapidly to an appropriate facility.
Emergency Care Protocol
Bleeding and Hemorrhagic Shock
Control any major life-threatening bleeding.
Establish spine motion restriction if spinal injury is suspected.
Establish and maintain an open airway; insert a nasopharyngeal or oropharyngeal airway if the patient is unresponsive and has no gag or cough reflex.
Suction secretions as necessary.
I f breathing is inadequate, provide positive pressure ventilation with supplemental oxygen at a minimum rate of 10–12 ventilations/minute for an adult and 12–20 ventilations/minute for an infant or child.
If breathing is adequate, administer a high concentration of oxygen by nonrebreather mask at 15 literperminute if signs or symptoms of poor perfusion are present to maintain t h e S p O2 greater than 95%.
Control bleeding with direct pressure (use fingertip pressure).
Apply a tourniquet if bleeding is not controlled with direct pressure. Note the time the tourniquet was applied and document the time. If it is not possible to apply a tourniquet to the body, apply a hemostatic agent with a dressing and continue to apply direct pressure.
Apply sterile dressings and bandages.
Maintain body temperature.
Consider application of the P A S G.
Place the patient supine.
If spinal injury is suspected, provide spine motion restriction.
Transport.
Perform reassessment every 5 minutes.
Soft Tissue Trauma
Soft tissue injuries may be closed or open.
The appearance of soft tissue injuries can be dramatic, but don’t be distracted from the priorities of care.
Dressings and bandages are used to help control bleeding and prevent further wound contamination.
The Skin
Protects the body from the environment and organisms
Helps regulate body temperature
Senses heat, cold, touch, pressure, pain
Assists in elimination of water, salts
Skin Layers
Epidermis
Dermis
Subcutaneous layer
Closed Soft Tissue Injury
In closed injuries, there is no break in the skin.
Three types of closed injury are:
Contusions
A bruise
Injury to blood vessels in the dermis
Swelling, discoloration (ecchymosis)
Hematomas
Involves larger blood vessels and tissue areas than a contusion
Forms as a pocket of blood beneath the skin and can separate tissues
Presents as a lump with discoloration
Crush injuries.
Results from significant blunt trauma or crushing force
May be open or closed
Serious damage to underlying tissues
Internal bleeding
Assessment-Based Approach-Closed Soft Tissue Injuries
Scene Size-Up and Primary Assessment
Perform a scene size-up; look for mechanism of injury.
Provide spine motion restriction precautions, if indicated.
Primary Assessment
Secondary Assessment
Emergency Medical Care
Ensure an open airway, adequate breathing, and maintain oxygenation.
Treat for shock, if indicated.
Splint suspected fractures.
Reassess and transport the patient.
Open Soft Tissue Injury
In open injuries, the continuity of the skin is broken.
Open injuries are at risk for external bleeding and contamination.
An open injury may be a sign of a deeper underlying injury.
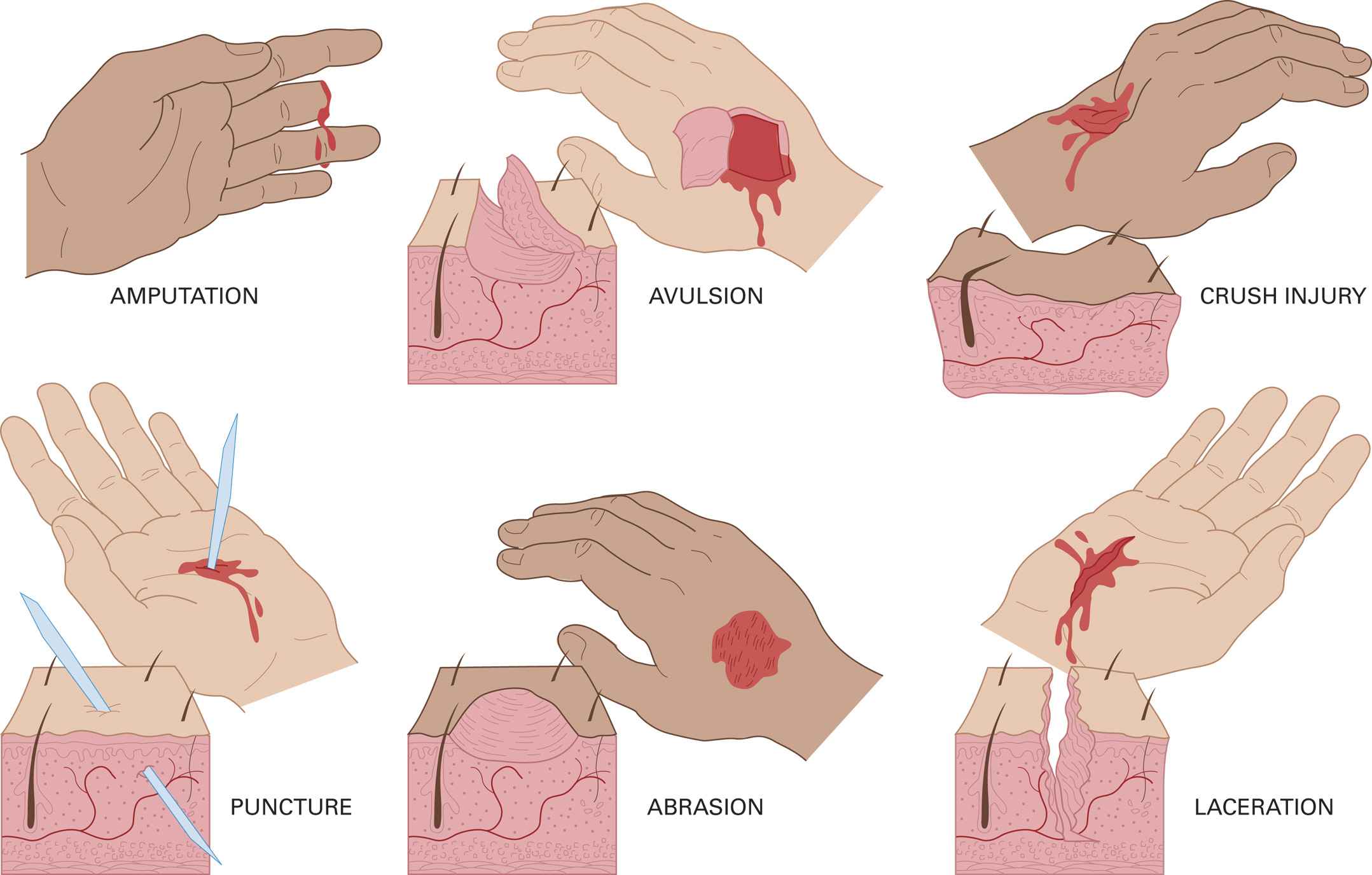
Six types of open injuries are:
Abrasions
Abrasion injuries are caused by scraping or rubbing away the epidermis.
The injuries are superficial, but painful.
Bleeding is easily controlled.
If large areas of the body are involved, infection is a concern.
Lacerations
A break in the skin
Depth may vary
May be linear or stellate
Possibility of significant bleeding
Avulsions
A flap of skin is torn loose or pulled off completely.
Bleeding can be severe.
Healing can be prolonged and scarring may be extensive.
Amputations
Disruptions in the continuity of an extremity or other body part
Result from ripping or tearing forces
Minimal or massive bleeding.
May be partial or complete
Penetrations/punctures
The injuries result from sharp, pointed objects being pushed or driven into soft tissues
The entry wound may be small, but the underlying damage can be severe.
A gunshot is a type of penetration injury.
A knife injury is also a penetration injury, and may be hidden.
Crush injuries.
The affected part may be painful, swollen, and deformed; bleeding can be minimal or absent.
There may be internal injuries and bleeding.
Shock can develop rapidly when the crushing object is lifted from the patient.
Other Soft Tissue Injuries
Bites
Dog bites can be complicated by infection, cellulitis, septicemia, and concerns of rabies and tetanus.
Human bites can result in infection and hepatitis.
Clamping Injuries
A body part is caught or strangled in machinery.
These injuries often include a finger or hand.
It becomes more difficult with time to extricate the body part(s) from machinery because of swelling.
Assessment-Based Approach-Open Soft Tissue Injuries
Scene Size-Up and Primary Assessment
Secondary Assessment
Signs and Symptoms
Secondary Assessment Signs and Symptoms
For an unstable patient or significant mechanism of injury, perform a rapid secondary assessment.
For a stable patient without significant mechanism of injury, perform a modified secondary assessment.
Emergency Medical Care
Ensure an open airway and adequate breathing and oxygenation.
Expose the wound and control bleeding.
Prevent further contamination.
Dress the wound; keep patient calm.
Treat the patient for shock and transport.
Special Considerations
Penetrating chest wounds
Requires an occlusive dressing
Penetrating or open abdominal injuries
Do not repack protruding organs.
These injuries require moist and sterile dressings and occlusive dressings.
Impaled objects
Do not remove the object unless it is in the cheek or neck and obstructing airflow through the airway.
Stabilize the object in place.
Amputations
Some amputated parts can be reattached, if cared for properly
Caring for Amputated Parts
Remove gross contamination.
Wrap the part in dry, sterile gauze.
Wrap or bag the part in plastic.
Keep the amputated part cool.
Never complete a partial amputation..
Transport the amputated part(s) and patient together, if possible.
Large neck injuries
Open neck wounds
Bleeding may be severe.
Air can be sucked into damaged veins, causing an air embolism.
Dressing and Bandages
Dressings
Cover the wound to help control bleeding and prevent further contamination.
Dressings should be sterile.
Various types of dressings are available.
Bandages
Used to secure dressings
Should be clean and free of debris
Various types available
General Principles of Dressing and Bandaging
Sterile materials are preferred.
Do not apply a bandage until bleeding is controlled.
Dressings should cover the entire wound.
Remove all jewelry from the injured part.
Do not bandage too loosely.
If bleeding is not controlled with direct pressure, apply a tourniquet.
Bandage snugly but not too tightly.
CHAPTER 29
Dirty review of skin anatomy
Layers of the skin
Epidermis
Dermis
Subcutaneous layer
The skin is the largest organ of the body
Functions of the skin
Physical barrier from the external environment
Insulates and protects the body
Provides sensory perception
Eliminates of some of the body’s wastes
Aids in production of Vitamin D
Pathophysiology of Burns
Most burn patients die in the prehospital setting from an occluded airway, toxic inhalation, or other trauma.
Maintain a patent airway, adequate ventilation and oxygenation, and control life-threatening bleeding.
Circulatory System
Burn injuries can cause extreme fluid loss.
Burns increase capillary permeability, which decreases intravascular fluid.
Edema can further compromise tissue perfusion.
The fluid shift results in hypovolemia.
Respiratory System
Burns and inhalation of superheated air can cause obstruction of the airway.
Toxin-Induced Lung Injury
Smoke and toxic gas can cause respiratory compromise and poisoning.
Cyanide
Carbon Monoxide
Sulfur Dioxide
Hydrogen Chloride
Renal System (Kidneys)
Decreased blood flow to kidneys reduces urine output.
The kidneys must handle an increased amount of waste products from cell destruction.
Kidney failure may occur.
Nervous and Musculoskeletal Systems
Nerve endings can be destroyed.
Loss of function of extremities can result.
Gastrointestinal System
Decreased G I perfusion can cause nausea and vomiting.
Longer-term considerations include ulcers and ensuring adequate nutritional support.
Classification of Burns
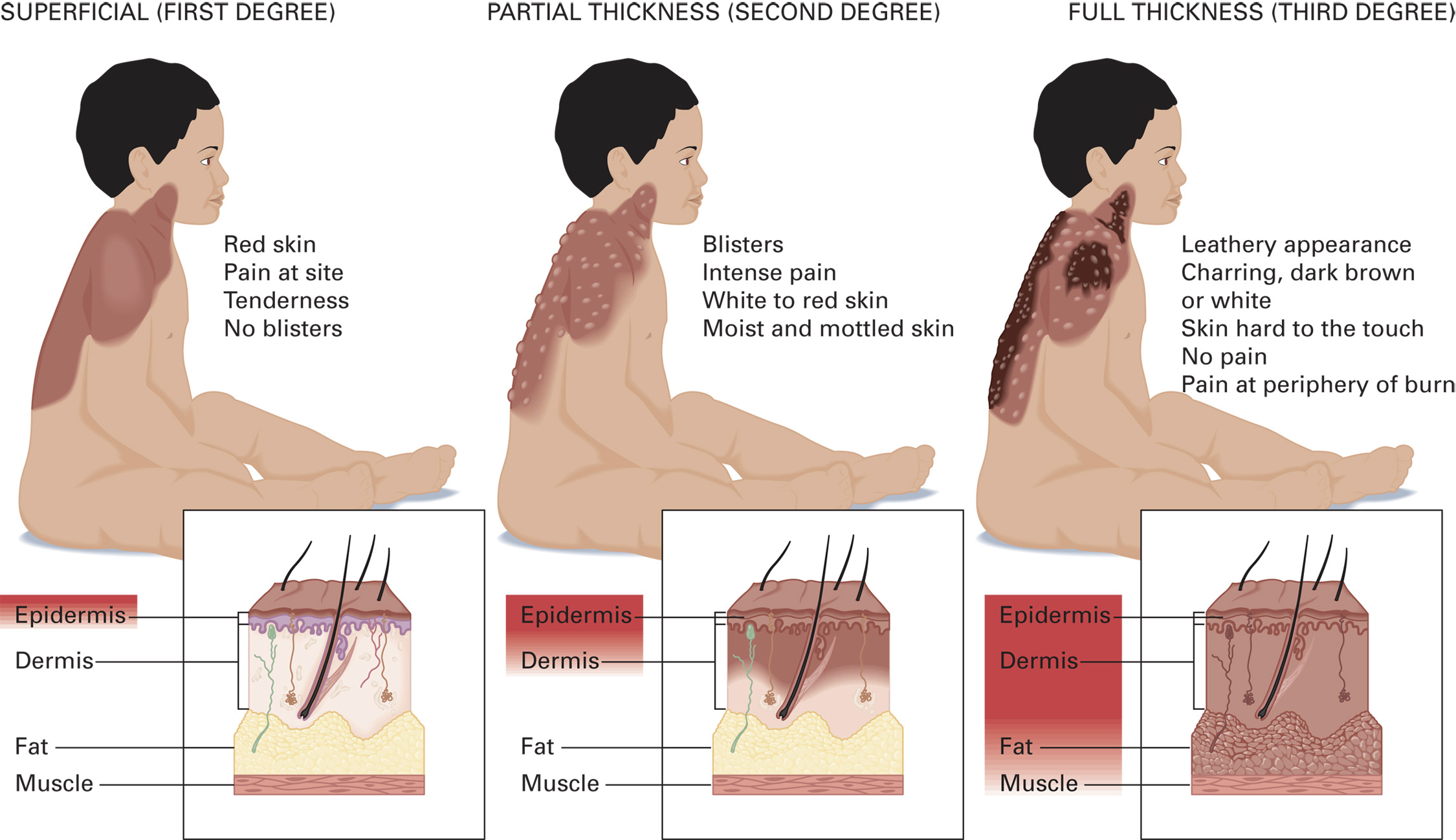
Classifying Burns by Depth
Superficial – 1st Degree
Involves only the epidermis
Partial-Thickness – 2nd Degree
Deep Partial-Thickness Burns
Full-Thickness – 3rd Degree
Eschar– Tough, leathery, dead soft tissue
Electrical injuries may result in 4th Degree Burns
Superficial Burns
Involves only the epidermis
Classifying Burns by Severity
Burns are classified by severity for treatment and transport decisions.
Factors in determining burn severity:
Depth of burn
Location of the burn
Patient’s age
Preexisting medical conditions
Percentage of body surface area involved
Burn Injury Location
Face
Risk of inhalation injury
Hands & feet
Loss of joint function
Circumferential Burns
Encircle a body area
Age and Preexisting Medical Conditions
Children under age two and adults over 50 have less tolerance for burn injury.
Children have the potential for greater fluid loss.
Fluid and heat loss are greater in infants and children than in adults.
Consider the possibility of child abuse.
Classifying Burns by Burn Size (Body Surface Area)
Rule of Nines- standardized way to quickly determine the body surface area (B S A) percentage, of a burn.
Do not include superficial burn area
Percentages differ for children and adults.
Rule of ones or rule of palms
Patient’s palm equals 1 percent surface area.
Types of Burns:
Thermal burns
Inhalation burns
Chemical burns
Electrical burns
Radiation burns
Causes of Burns
Flame burn
Contact burn
Scald
Steam burn
Gas burn
Electrical burn
Flash burn
Assessment-Based Approach: Burns
Scene Size-Up
First - determine if the scene is safe.
Primary Assessment
Remove the patient from the source of burning.
Within ten minutes of the burn, cool the burn with water or saline.
Remove jewelry and smoldering clothing.
Assess the airway, breathing, oxygenation, and circulation.
Look for indications of airway burns and difficulty breathing.
If toxic inhalation is suspected, administer oxygen by nonrebreather mask.
Secondary Assessment
Reassess the M O I and chief complaint
Check for other injuries
Continue to remove clothing
Determine accurate B S A
Obtain vital signs
Obtain a history
Signs and Symptoms
In addition to estimating B S A and noting location of the burns, determine depth.
Look for signs indicating inhalation injury.
Emergency Medical Care
Remove the patient from the source of the burn and stop the burning process.
Do not enter an unsafe environment.
Do not remove adherent materials from the burn.
Brush away dry powders before flushing with water.
Remove smoldering clothing.
Emergency Medical Care
Maintain an airway, adequate breathing, and oxygenation
Positive pressure ventilation for inadequate breathing.
Administer oxygen by nonrebreather for toxic inhalation.
Maintain an S p O2 of 94% or above.
Classify the severity of the burn
Take into account B S A, source of the burn, location of the burn, patient age, and preexisting medical conditions.
Transport patients with critical burns immediately.
Cover the burned area with a dry, sterile dressing, burn sheet, or approved commercial dressing.
Moist dressings can lead to hypothermia.
Some systems allow a moist dressing for <10% B S A.
Follow protocol.
Keep the patient warm, treat other injuries.
Transport to the appropriate facility.
Special considerations for dressing burns:
Burns of hands and toes.
Separate all digits with dry, sterile dressing material.
Burns of eyes.
Don’t attempt to open burned eyelids.
Apply a dry sterile dressing to both eyes.
Flush chemical burns medial to lateral.
Reassessment
Every five minutes for unstable patients.
Every 15 minutes for stable patients.
Continually evaluate the airway.
Chemical Burns
The longer a chemical is in contact with the skin, the greater the potential for injury.
Protect yourself first.
Brush away dry chemicals before flushing with water.
For most chemicals, flush with copious amounts of water.
Special Considerations in Treating Chemical Burns
When dealing with chemical substances, there are some special considerations.
Dry lime
Hydrofluoric acid
Carbolic acid (phenol)
Sulfuric acid
Electrical burns
All tissues between the entrance and exit of the current can be injured.
Damage is caused by heat; the body’s electrical impulses can be disrupted.
Scene safety is crucial in electrical burn injuries.
Never attempt to remove a patient from an electrical source.
Critical Burns
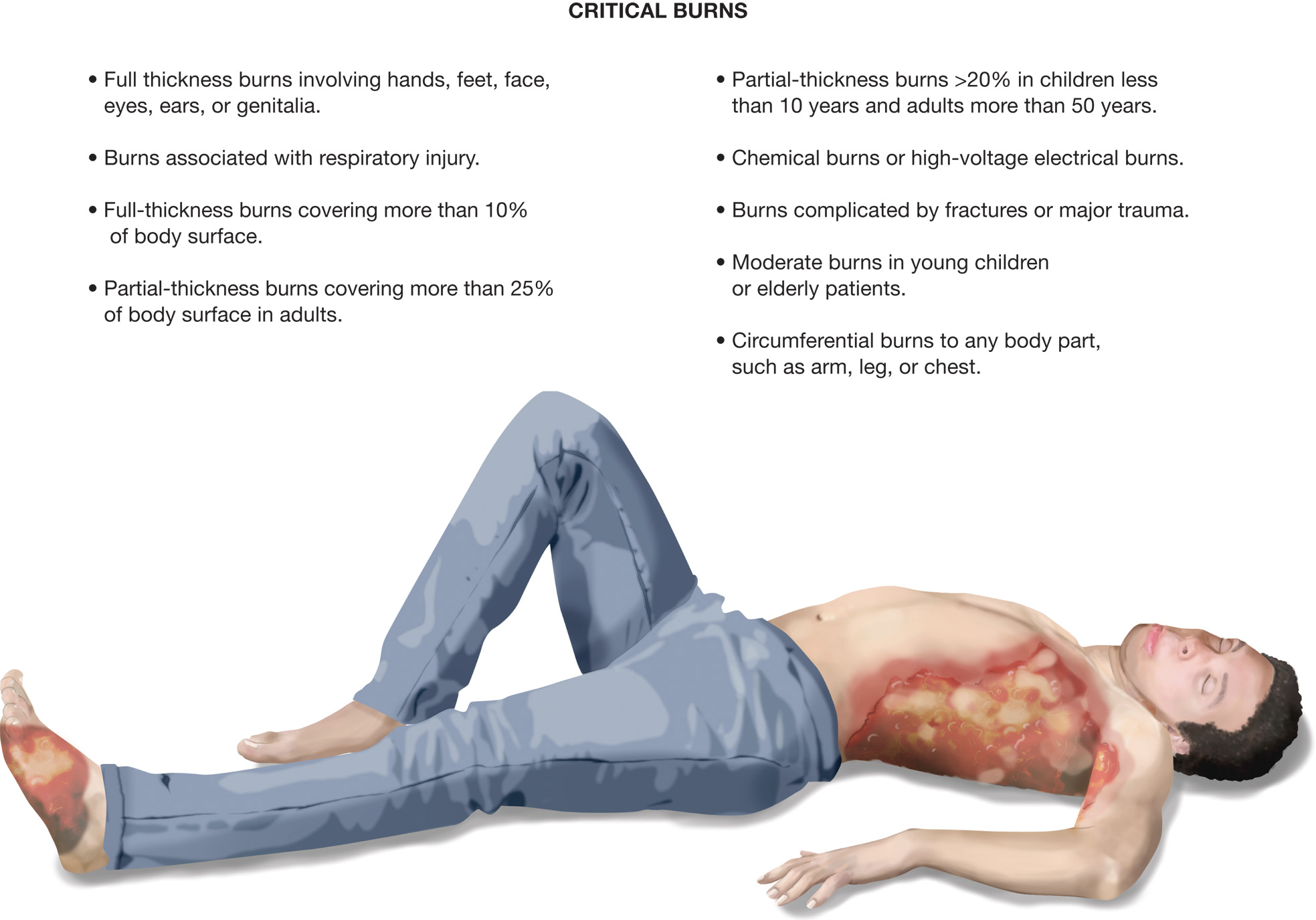
Assessment Summary: Burn Emergency
Scene Size-Up
Pay particular attention to your own safety. Look for:
Burning structures or material
Chemicals
Electrical sources
Confined spaces
Burned clothing
Obvious burns to patient’s body
Evidence of explosion
Other blunt or penetrating trauma
Primary Assessment
General Impression
Stridor or crowing from upper airway
Obvious burns to body and clothing
Burns to neck and face
Singed hair, nasal hair, eyebrows, and other facial hair
Carbonaceous (black) sputum
Mental Status
Alert to unresponsive
Airway
Stridor (indicates upper airway burn)
Edema to oral mucosa and tongue
Burns around neck and face
Black inside mouth
Breathing
Normal to increased if airway or respiratory tract is not involved
Increased or decreased, labored, and shallow if airway or respiratory tract burns
Circulation
Increased; may be decreased if severely hypoxic
Skin normal in unburned areas; may be cool, clammy, and pale
Status: Priority patient if large body surface area burns, airway or respiratory tract is involved, critical burns are apparent, or burns involve hands, feet, face, genitalia, or major joint locations
Secondary Assessment
Physical Exam
Head, neck, and face:
Burns
Singed hair, eyebrows, facial and nasal hair
Dark black (carbonaceous) sputum
Swelling of tongue and oral mucosa
Hoarseness
Coughing (may cough up black sputum)
Cyanosis
Stridor
Burns to the oral mucosa
Chest:
Burns
Wheezing
Circumferential burns around thorax may impede ventilation
Blunt or penetrating trauma if explosion or fall involved
Abdomen:
Burns
Blunt or penetrating trauma if explosion or fall involved
Extremities:
Burns (the appearance of the burn is largely determined by the burning mechanism, for example, thermal versus chemical)
Circumferential burns may reduce distal circulation
Swelling, pain, and discoloration if explosion or fall involved
Vital Signs
B P: normal, may decrease with severe burns after a few hours (if B P decreased at the scene, look for evidence of other trauma)
H R: normal or increased
R R: normal; increased and labored if respiratory tract burn involved
Skin: normal in unburned areas (if pale, cool, clammy immediately after burn may indicate shock from other trauma)
Pupils: normal
S p O2: may be less than 94% if inhalation injury or toxic inhalation has occurred
History
Signs and symptoms of superficial burns:
Skin that is pink or red, and dry
Slight swelling
Pain
Signs and symptoms of partial-thickness burns:
Skin that is white to cherry red
Moist and mottled
Blisters
Intense pain
Signs and symptoms of full-thickness burns:
Skin that is dry, hard, tough, and leathery
White and waxy, dark brown, or charred
No pain in burned area
Usually pain around the site of full-thickness burn
Signs and symptoms of inhalation injury:
Facial burns
Singed nasal and facial hair and eyebrows
Black sputum
Respiratory distress with labored breathing
Coughing, hoarseness, cyanosis, stridor
Emergency Care Protocol
Remove the patient from the source of burn and stop the burning process.
Provide spine motion restriction if spinal injury is sus-pected.
Establish and maintain an open airway; insert a nasopharyngeal or oropharyngeal airway if the patient is unresponsive and has no gag or cough reflex.
Suction secretions as necessary.
If breathing is inadequate, provide positive pressure ventilation with supplemental oxygen at a minimum rate of 10–12 ventilations/minute for an adult and 12–20 ventilations/minute for an infant or child
If breathing is adequate, administer oxygen by nonrebreather mask at 15 lpm if inhalation of a toxic gas or upper airway burn is suspected. If the burn is isolated to an area of the body and does not involve the face or a possible inhalation injury or toxic exposure, base your oxygen administration on the SpO2 reading and signs of hypoxia. Administer oxygen to maintain the SpO2 at 94% or greater.
Estimate body surface area burn (percent BSA) using the rule of nines.
Determine depth of burn: superficial, partial thickness, or full thickness.
Apply sterile dressings and bandages or a burn sheet.
10.If the burn is less than 10 percent BSA, dress wet per protocol. Dress all other burns dry.
Maintain body temperature.
12.Manage other associated injuries as appropriate.
13.If spinal injury is suspected, immobilize the patient to a backboard.
Manage specific burns as follows:
Dry chemical burn:
Remove affected clothing, brush off dry chemical, then irrigate with large amounts of water.
Liquid chemical burn:
Remove affected clothing; irrigate with large amounts of water if the chemical is one that does not react to water.
Burns to the hands and feet:
Remove all rings and jewelry; dress between digits.
Chemical burns to the eyes:
Flush with large amounts of water and continue to flush en route.
Thermal burns to the eyes: Do not attempt to open eyelids; apply dry, sterile dressing to both eyes.
Electrical burns: Carefully monitor pulse and respiration; inspect for entrance and exit wounds; assess for muscle tenderness; apply A E D if patient is in cardiac arrest.
15.Transport.
16.Perform a reassessment every 5 minutes if unstable and every 15 minutes if stable.
Chapter 30
Injuries to muscles, bones, and joints are common.
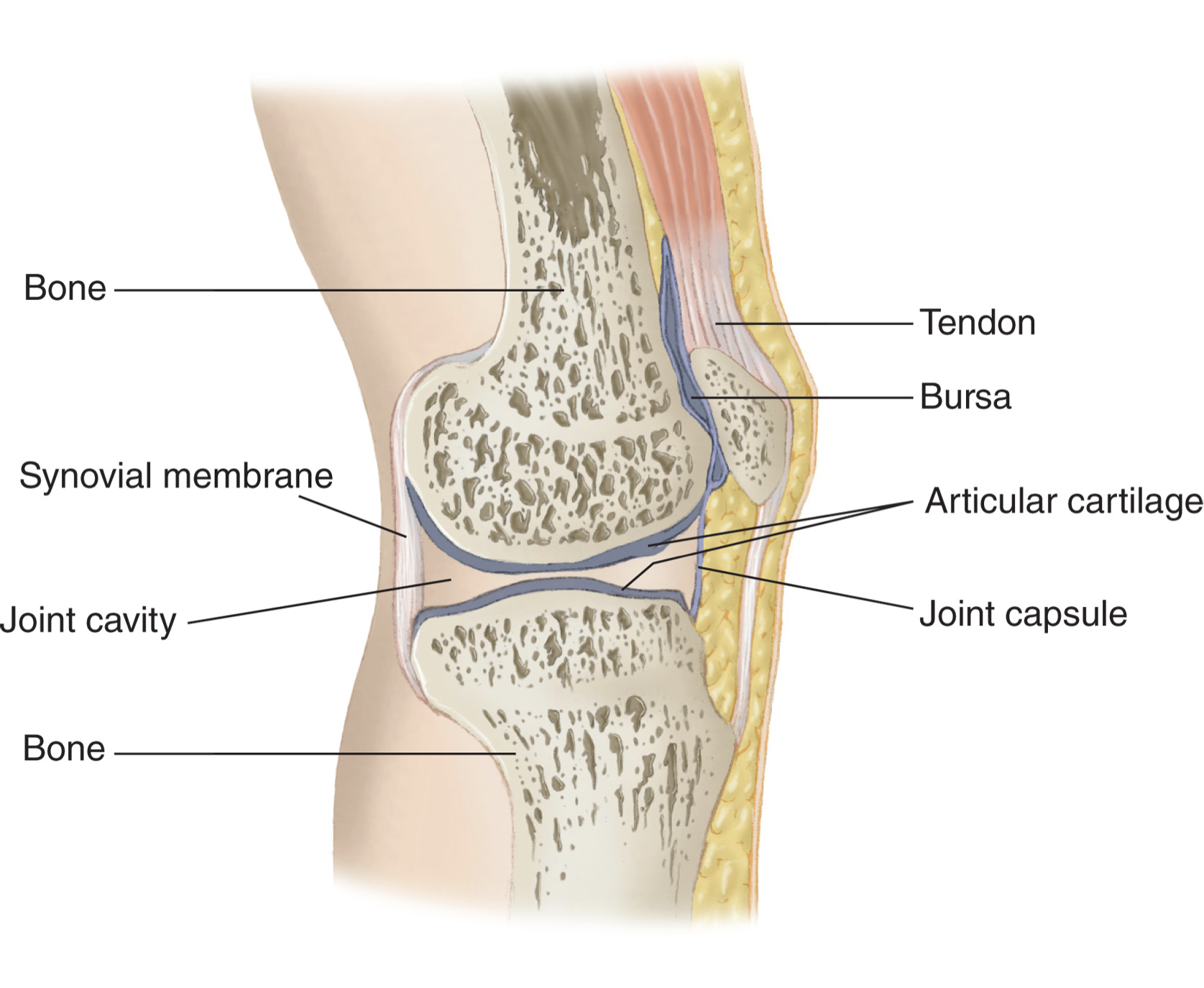
Musculoskeletal System Review
Functions of the musculoskeletal system are to:
Give the body shape
Protect the internal organs
Provide for movement
Store salts and other materials
Produce red blood cells
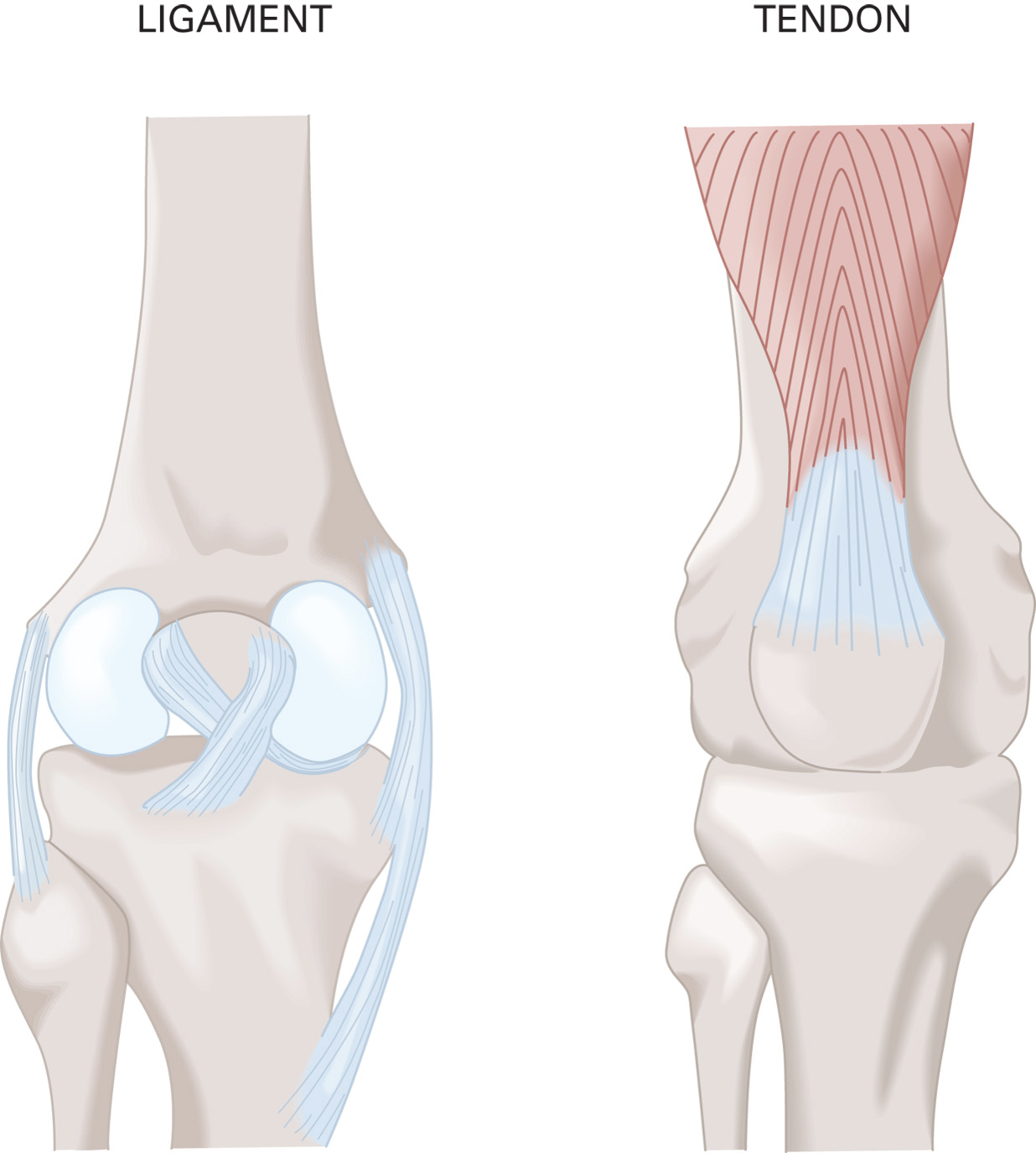
Ligaments connect bone to bone. Tendons attach muscle to bone.
The skeletal system
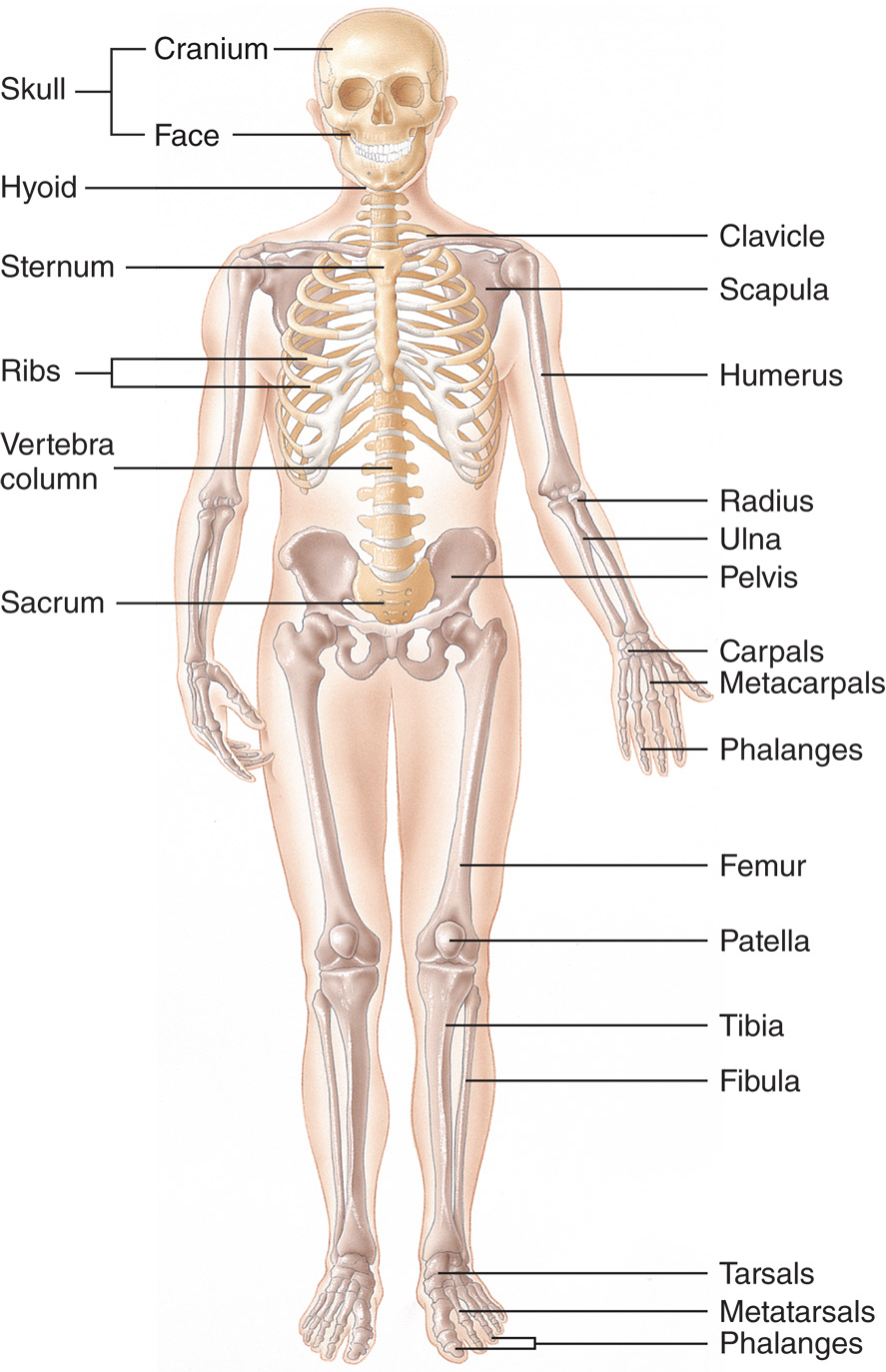
Axial skeleton
Appendicular skeleton
Injuries to Bones and Joints
Types of injuries
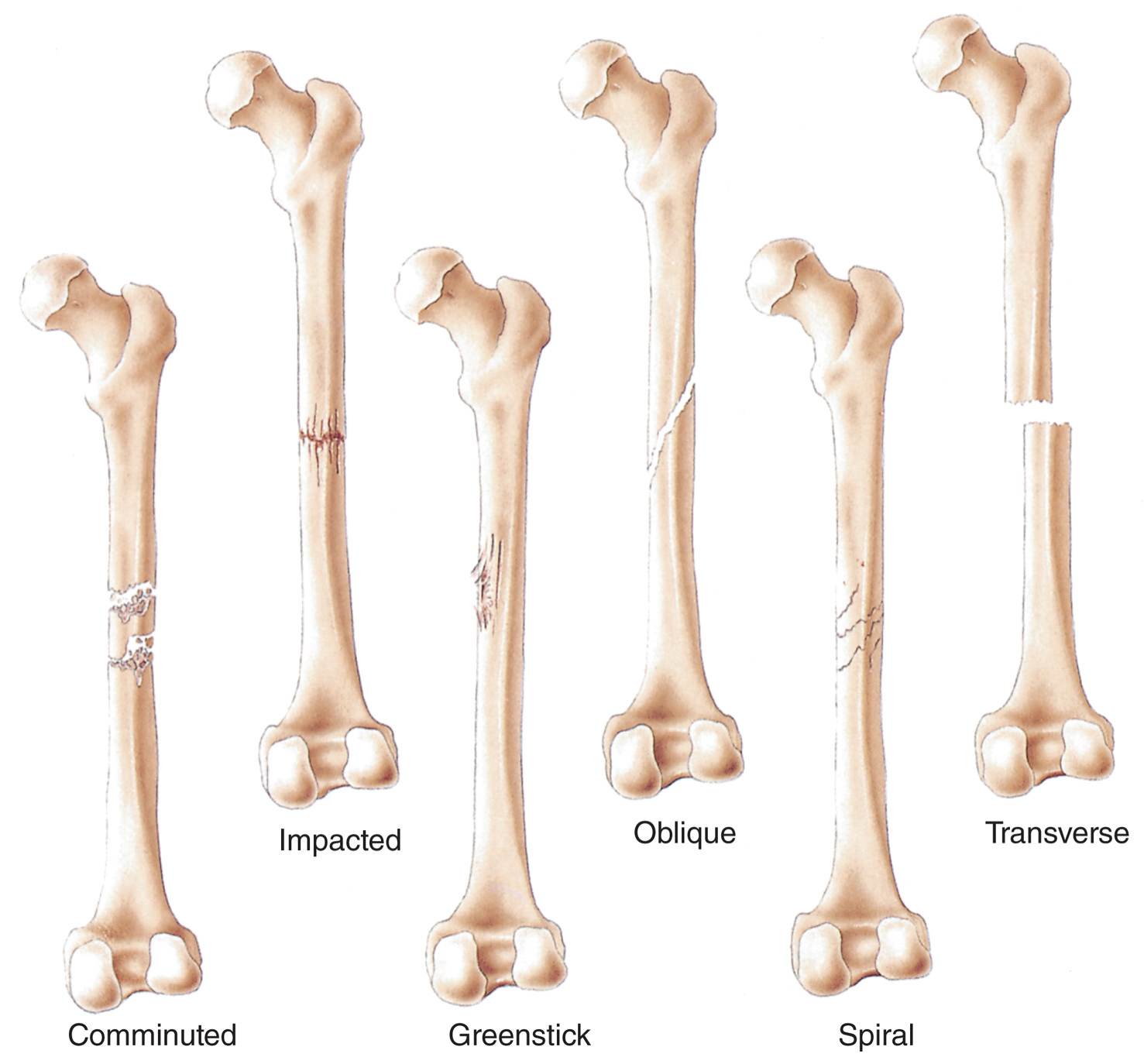
A fracture is a break in the continuity of a bone.
A fracture may be open or closed.
Fracture signs and symptoms
Pain
Tenderness
Deformity
Discoloration
ParesthesiaAnesthesia
Paresis
Paralysis/inability to move the extremity
Decreased pulse/perfusion
A pathologic fracture involves a diseased bone; less force is required to fracture the bone.
Osteoporosis is a bone disease that affects geriatric patients
A strain occurs when overexertion or overstretching causes muscle fibers to tear.
A sprain is an injury to a joint capsule, with damage to the connective tissue, usually the ligaments.
Dislocation
Displacement of bone from its normal position in a joint
Can cause damage to blood vessels and nerves
Critical fractures
The femur and pelvis
Potential for significant bleeding; can be life-threatening
Assessment-based approach
Life-threats or a pulseless or cyanotic extremity require transport immediately after the secondary assessment.
For life-threatening conditions, use a long backboard to immobilize the patient; do not splint individual injuries prior to transport.
Assess for the six "Ps"
Pain
Pallor
Paralysis
Paresthesia
Pressure
Pulses
Basics of Splinting
Splints are used to:
Prevent movement of bone fragments or ends, or dislocated joints to reduce further injury
Reduce pain and chances of complications
Complications include:
Damage to muscles, nerves, or blood vessels
Conversion of a closed fracture to an open one
Restriction of blood flow
Excessive bleeding
Increased pain
Paralysis of extremities (from spinal injury)
Hazards of improper splinting
Compression of nerves, tissues, blood vessels
Delayed transport
Reduced distal circulation
Aggravation of the injury
Excessive movement
Skin damage from improper padding
Traction splinting
Femur fractures can be accompanied by bleeding, pain, and muscle spasm.
Using traction to align the femur can reduce complications.
Treat for a fracture if the thigh is painful, swollen, or deformed.
Do not use a traction splint if:
The injury is within 1 to 2 inches of the knee or ankle
The knee has been injured
The hip has been injured
The pelvis has been injured
There is partial amputation or avulsion
Compartment syndrome
Pressure develops within the injured area.
The pressure exceeds the capillary pressure needed to perfuse the tissues.
The tissue becomes hypoxic, which results in further damage and swelling.
Compartment syndrome signs and symptoms
Severe pain or burning sensation
Decreased strength in extremity
Paralysis of the extremity
Pain with movement
Extremity feels hard to palpation
Distal pulses, motor, and sensory function may be normal
Always assess pulse, motor, and sensory function before and after splinting.
Chapter 35
Abdominal trauma has the potential to cause severe bleeding and hemorrhagic shock.
It is important to recognize mechanisms of injury and signs and symptoms of abdominal trauma.
Anatomy of the Abdominal Cavity
Hollow abdominal organs are not as vascular, but if their contents are leaked into the abdominal cavity, peritonitis results.
Peritonitis can be life-threatening, but signs and symptoms may be delayed by hours.
Solid organs are vascular and can bleed profusely when injured.
Bleeding may not produce severe abdominal pain.
Be alert to signs of shock.
Hollow organs
Stomach.
Gallbladder
Urinary bladder
Ureters
Internal urethra
Fallopian tubes
Small intestine
Large intestine
vs
Solid organs
Liver
Spleen
Pancreas
Kidneys
Abdominal Injuries
Multiple organs may be injured by both blunt and penetrating mechanisms.
Penetrating trauma is more obvious; blunt trauma is easier to miss.
Assessment-Based Approach: Abdominal Injuries
Primary assessment
in the general impression, note the patient's position.
Patients with abdominal injuries may have the legs drawn up.
Secondary assessment
Inspect the abdomen.
Look for contusions, lacerations, abrasions, punctures.
Look for distention.
Look for discoloration around the umbilicus and flanks.
Look for evidence of an improperly placed lap belt.
Look for and provide treatment for evisceration.
Palpate the abdomen.
Start at the point farthest away from the point of pain.
Note any masses or tenderness.
Note any rigidity.
Signs and symptoms of abdominal injury
Tenderness on palpation to areas other than the site of injury
Rigid abdominal muscles
Lying with legs drawn up to the chest
Distended abdomen
Discoloration around the umbilicus or to the flank
Rapid, shallow breathing
Signs of hemorrhagic shock
Nausea and vomiting
Abdominal cramping possibly present
Pain that radiates to either shoulder from irritation of the diaphragm
Weakness
Abdominal evisceration
Do not touch or attempt to replace the organs.
Genital Trauma
Can be painful and embarrassing for the patient.
Injuries to the male genitalia
Control bleeding with direct pressure.
Apply cold compresses if the scrotum is injured.
If the penis is avulsed or amputated, wrap the part in a sterile, saline-moistened dressing and keep it cool.
Assess for and manage shock.
Injuries to the female genitalia
Control external bleeding with direct pressure.
Do not pack or place dressings in the vagina.
Assess for and manage shock.