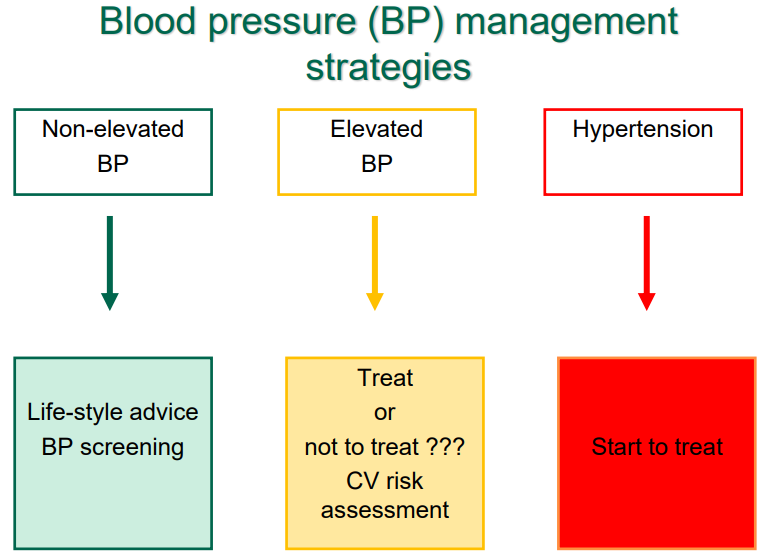
Hypertension
Non-elevated blood pressure < 120/70
Elevated blood pressure 120-139/70-89
Hypertension > 140/90
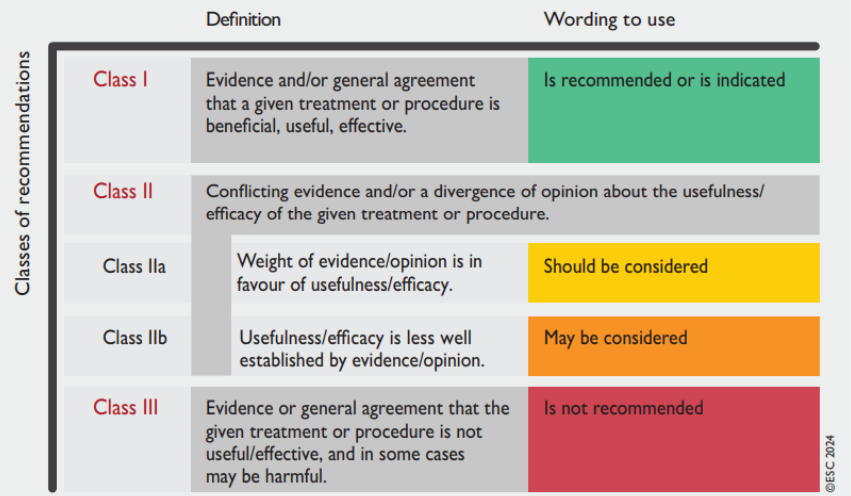
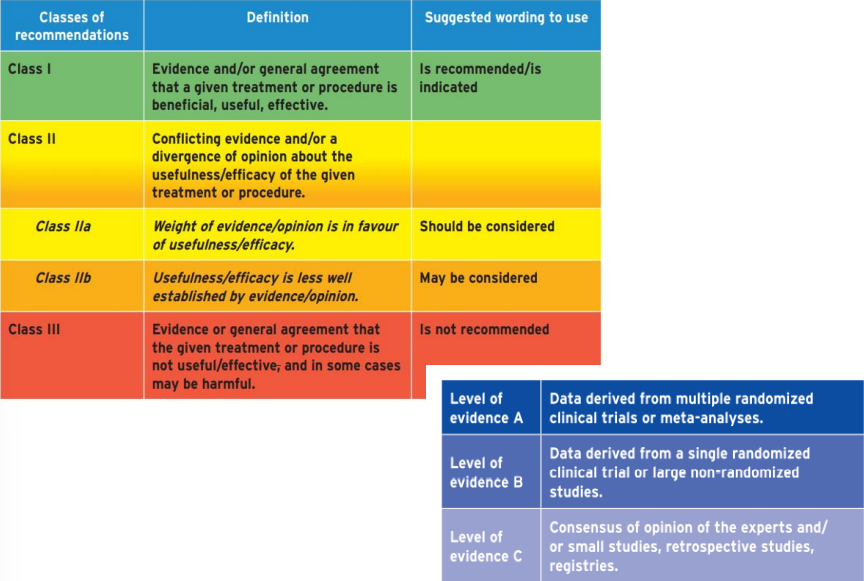
Classes of Recommendations
Factors influencing BP Regulation
Blood pressure is the product of CO and PVR (peripheral vascular resistance)
CO is the product of SV and HR. Factors affecting CO: sodium intake, renal function, mineralocorticoids
PVR depends on the sympathetic nervous system (SNS), humoral factor and local autoregulation. The SNS produces its effects via vasoconstrictor alpha effect or the vasodilator beta effect
The humoral actions are a result of mediators, such as vasoconstrictors (e.g. endothelin, angiotensin II, catecholamines) or vasodilators (e.g. nitric oxide, prostaglandins, kinins)
Arterial Hypertension Classification
The classifications are depending on:
Etiology
Primary
Secondary
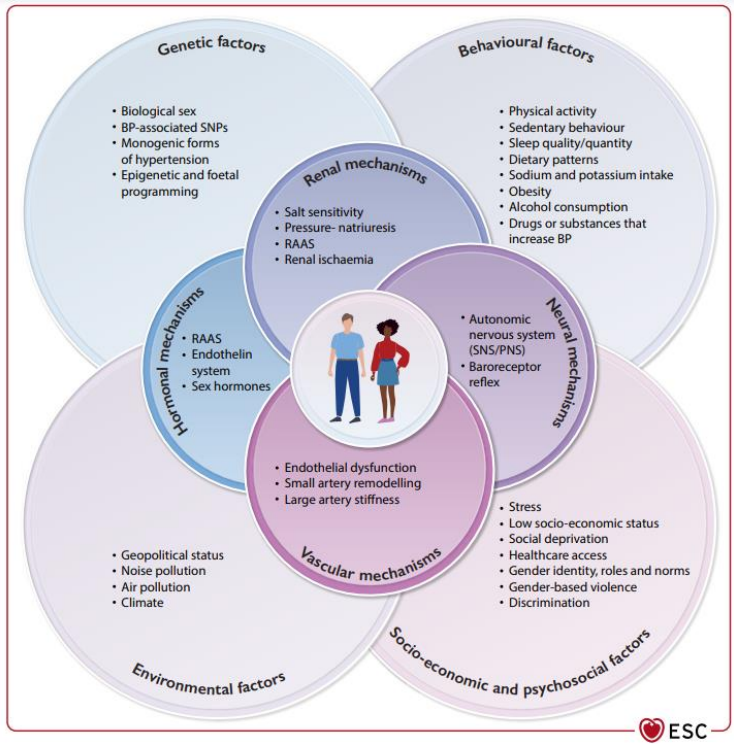
Pathogenesis of Primary Hypertension
The pathogenesis of primary hypertension is a complex interplay between
genetic predisposition,
lifestyle and environmental influences,
disturbances in vascular structure and neurohumoral control mechanisms.
Activation of the sympathetic system
Activation of renin-angiotensin-aldosterone system
A characteristic finding is an inappropriate increase in peripheral vascular resistance relative to the cardiac output
This is due to remodelling of small arteries (arterioles), - an increase in their media/lumen ratio
The functional integrity of large conduit arteries, i.e. the aorta, which becomes stiffer, also influences the development of hypertension— especially systolic hypertension
Cardiovascular Disease risk factors
Male sex
Age ( ≥ 55 years in men; ≥ 65 years in women)
Smoking
Dyslipidaemia (general population)
Fasting plasma glucose 5.6 – 6.9 mmol/l (102 – 125 mg/dl)
Abnormal glucose tolerance test
Diabetes
Obesity (BMI ≥ 30 kg/m²)
Abdominal obesity: waist circumference ≥ 102 cm in men; ≥ 88 cm in women (Caucasians)
Family history of premature CV disease ( < 55 yrs in men; < 65 yrs in women)
Factors influencing cardiovascular risk in patients with hypertension
Uric acid
Family or parental history of early-onset hypertension
Early-onset menopause
Sedentary lifestyle
Psychosocial and socioeconomic factors
Heart rate (resting values >80 beats/min)
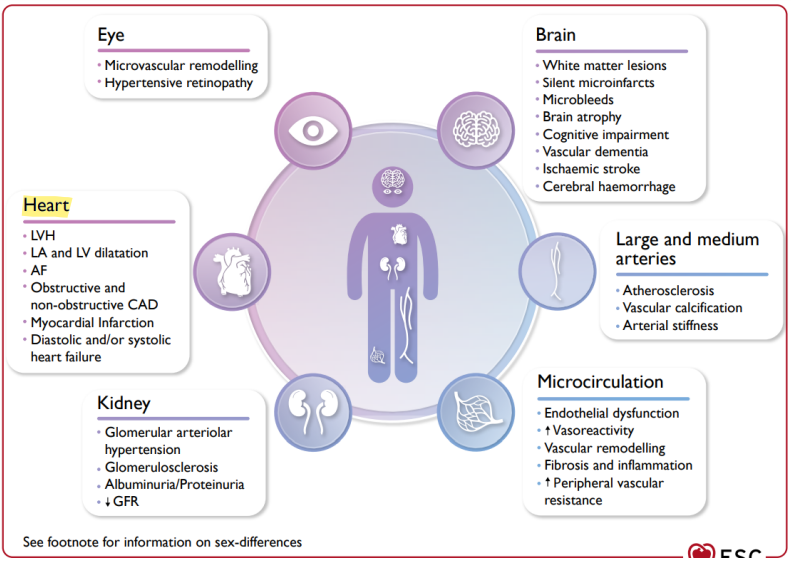
Clinical Consequences of AH
Longstanding hypertension causes organ damage and ultimately leads to cardiovascular, cerebrovascular, and clinical renal disease
Organs affected by elevated BP and hypertension:
Brain
Heart
Kidneys
Eyes
Vessels (macrocirculation and microcirculation in organs with low resistance, such as the brain or kidney
Consequences of these developments:
Cardiovascular diseases
Cerebrovascular diseases
Kidney failure
Blood pressure assessment methods
Office blood pressure measurement
quiet environment for 5 mins seated comfortably before measuring
3 BP measurements should be taken 1-2 minutes apart
arm should be supported
use phase 1 and V Korotkoff sounds to identify SBP and DBP
first visit: measure both arms (difference 5-10 mmHg, coarctation of aorta, pathologies in aorta/big arteries), lying and standing to avoid orthostatic AH - Difference should be 20mmHg
Home-based blood pressure measurement
average of all BP readings performed with a semiautomatic, validated BP monitor, for at least 3 days
in morning and evening, quiet room after 5 mins rest, seated, arm rested. Two measurements 1-2 mins apart
usually lower compared to office BP. diagnostic threshold for hypertension is ≥135/85mmHg
Ambulatory blood pressure measurement
ABPM provides the average of BP readings over a defined period, usually 24 h
The device is typically programmed to record BP at 15 - 30 min intervals, and average BP values are usually provided for daytime, night-time, and 24 h

Specific situations
White coat hypertension
The untreated condition in which BP is elevated in the office, but is normal when measured by ABPM, HBPM, or both
More common with increasing age, in women, and in non-smokers
Both ABPM and HBPM are recommended to confirm white-coat hypertension
Masked hypertension
Refers to untreated patients in whom the BP is normal in the office, but is elevated when measured by HBPM or ABPM
Greater in younger people, men, smokers, and those with higher levels of physical activity, alcohol consumption, anxiety, and job stress
Obesity, diabetes, CKD, family history of hypertension, and high–normal office BP are also associated with an increased prevalence of masked hypertension
Diagnosis
Hypertension diagnosis can`t be established based on one-time office blood pressure measurement.
Hypertension should be confirmed with repeated data: - preferably by ambulatory or home-based BP measurements
If BP > 180/110 mmHg – Hypertensive emergencies have to be excluded.
If it isn`t a Hypertensive emergency, repeated control should be obtained within a week. Treatment can be postponed until the next scheduled visit
Assessment of cardiovascular disease risk
The control/treatment of elevated BP and Hypertension treatment tactics depend on cardiovascular diseases (such as myocardial infarction, cerebral infarction and others) risk.
CV diseases risk depends on:
BP level
CV risk factors
Hypertension-mediated organ damage (HMOD)
Symptomatic cardiovascular and renal diseases
Elevated BP
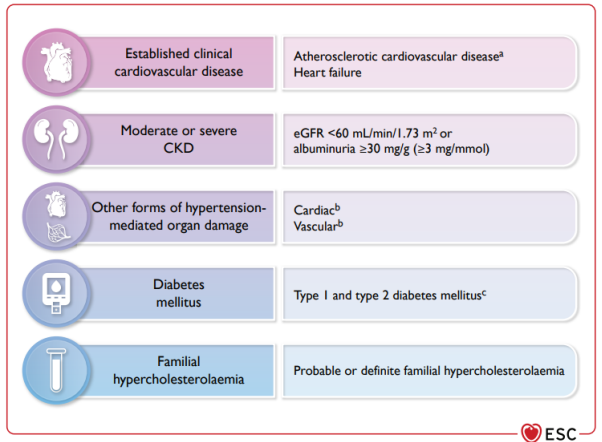
Step 1. Assessment of sufficiently high CV risk conditions
Hypertension mediated organ damage
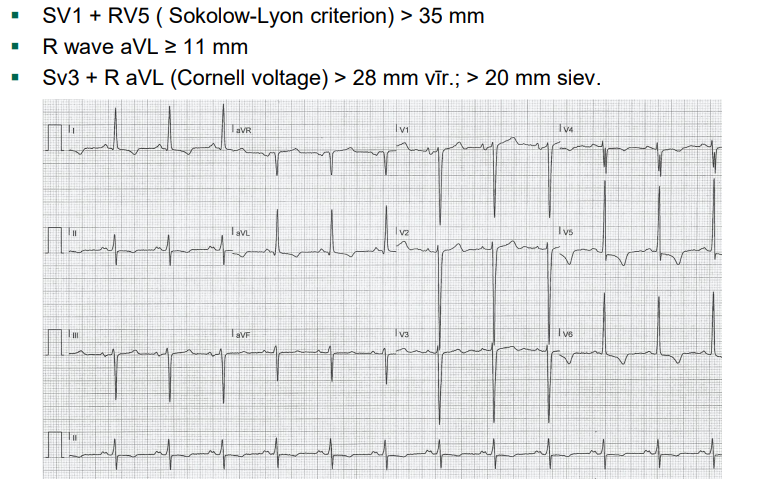
Heart
The most commonly used simple criteria and recognised cut-off points for definitions of electrocardiogram left ventricular hypertrophy, LA dilation (duration of P wave in lead II more than 120ms), arrythmias, blocks
Biomarkers: Hs-cTnT (high sensitive troponin) or TnI >99th percentile upper reference limit ▪ NT-proBNP > 125 pg/mL if aged <75 years, >450 pg/mL if aged ≥75 years.
Vessels
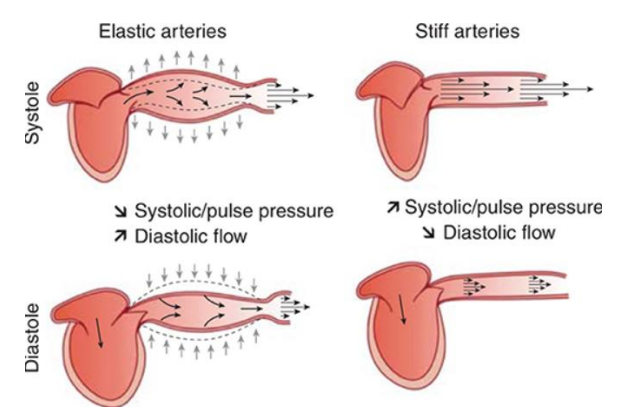
Pulse wave velocity
Carotid-femoral PWV > 10 m/s - shows how stiff arteries are
Brachial–ankle PWV > 14 m/s
ankle-brachial index - if less than 1 = normal
Carotid Ultrasound
Plaque (focal wall thickening > 1.5 mm). - see atherosclerosis!!
Computed Tomography (CT)
Calcium score > 100 Agatson units
Kidneys
eGFR < 60 ml/min/1,73 m² or
Urine Albumin-creatinine ratio > 30 mg/g
Step 2. Estimation of predicted 10-year CV risk
SCORE
Estimation of predicted 10-year CV risk
Criteria:
regional CV mortality (WHO data)
sex
age
blood pressure level
non-high cholesterol /non-HDL cholesterol
smoking
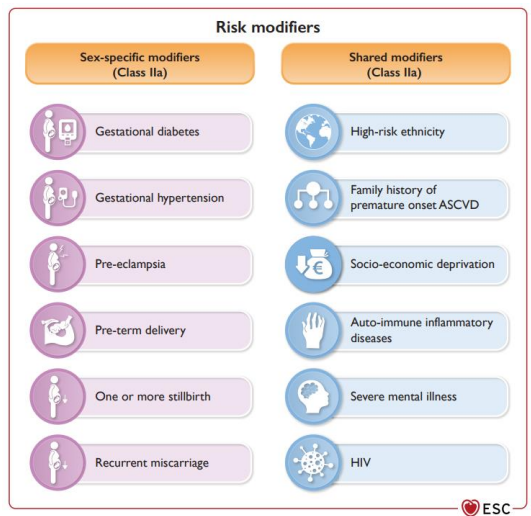
Step 3. Assessment of sex-specific and shared risk modifiers
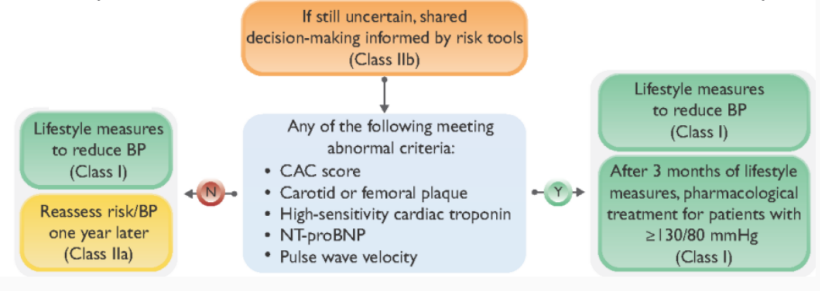
Step 4. Consider additional examinations for CV risk assessment
Secondary Hypertension
Renal
Pathologies of the parenchyma
chronic kidney diseases
acute glomerulonephritis
chronic pyelonephritis
polycystic kidney disease
diabetic nephropathy
hydronephrosis
Renovascular hypertension
stenosis of A.renalis( unilateral, bilateral)
Endocrine system pathologies
Acromegaly
Hypothyroidism
Hyperthyroidism
Pathologies of the adrenal gland:
cortex: Cushing syndrome, primary aldosteronism
medulla: pheochromocytoma
Drug induced:
corticosteroids
hormonal contraceptives
sympathomimetics
nonsteroidal anti-inflammatory drugs
erythropoietin
Coarctation of aorta, aortitis
Pregnancy hypertension
Neurological pathologies:
increased intracranial pressure (tumour, encephalitis); sleep apnoea etc.
Perioperative hypertension
Patient characteristics that should raise the suspicion of secondary hypertension
Younger patients (<40 years) with grade 2 hypertension or onset of any grade of hypertension in childhood
Acute worsening hypertension in patients with previously documented chronically stable normotension
Resistant hypertension
Severe (grade 3) hypertension or a hypertension emergency
Presence of extensive Hypertension mediated organ damage (HMOD)
Clinical or biochemical features suggestive of endocrine causes of hypertension or Chronic kidney disease
Clinical features suggestive of obstructive sleep apnoea
Symptoms suggestive of phaeochromocytoma or family history of phaeochromocytoma
Hypertensive emergencies
Hypertensive emergencies are situations where very high BP values are associated with acute hypertension-mediated organ damage, and therefore, require immediate BP reduction to limit extension or promote regression of target organ damage
Key target organs of acute hypertension-mediated damage are the heart, retina, brain, kidneys, and large arteries
The type of target organ damage is the principal determinant of the choice of treatment, target BP, and timeframe by which BP should be lowered
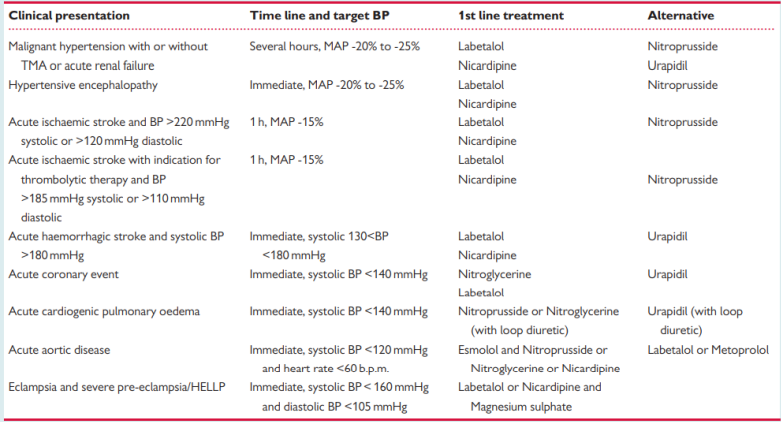
Clinical Presentations of Hypertensive emergencies
Malignant hypertension - a hypertensive emergency characterized by the presence of a severe BP elevation (usually >200/120 mmHg) and advanced retinopathy, defined as the bilateral presence of flame-shaped haemorrhages, cotton wool spots, or papilloedema
cerebral infarction
Hypertensive encephalopathy - When BP is markedly elevated and cerebral autoregulation cannot prevent a rise in intracranial pressure, cerebral oedema may develop, especially in the posterior areas of the brain where sympathetic innervation is less pronounced leading to less effective damping of BP oscillations.
Hypertensive retinopathy
intracranial haemorrhage
acute left ventricular failure
acute pulmonary oedema
aortic dissection
acute renal failure
eclampsia
Diagnostic studies in patients with suspected hypertensive emergency
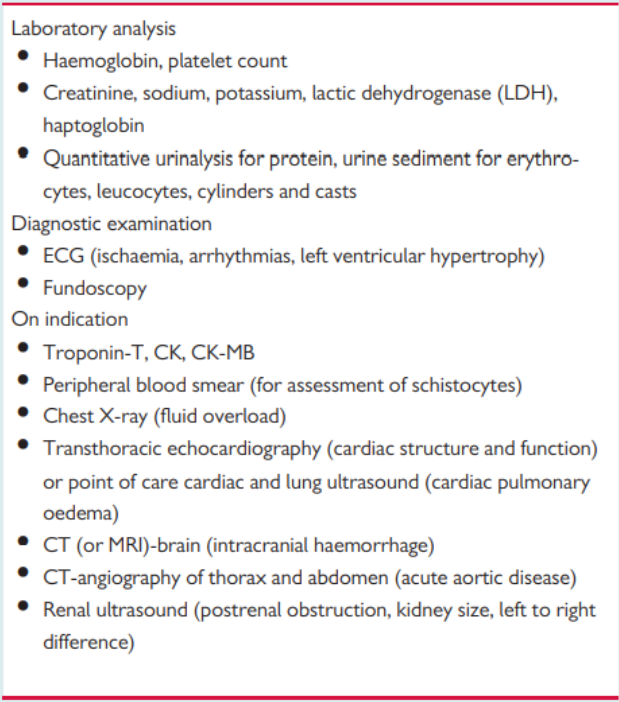
!!Blood tests
!!ECG - LVH LA dilation, arrythmias, blocks
!!Echocardiogram - signs of wall thickening, IV septum, diastolic function
Uncontrolled hypertension or Hypertensive urgencies
Is defined as large elevation in SBP and/or DBP associated without signs of the organ damages , just subjective or mild objective symptoms such as:
nasal bleeding
nausea, vomiting
headache, dizziness
chest pain
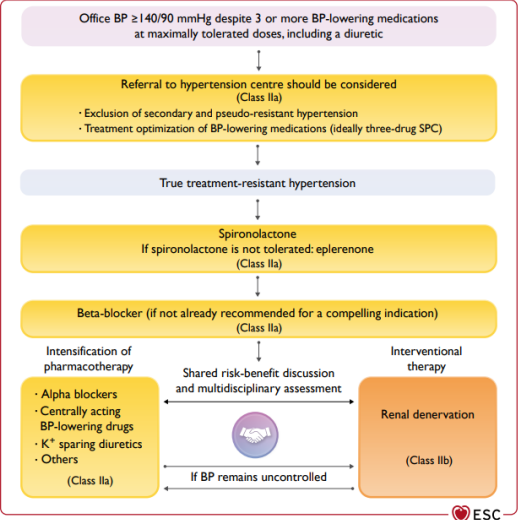
Resistant hypertension
Is defined as resistant to treatment when the recommended treatment strategy fails to lower office SBP and DBP values to < 140 mmHg and/ or < 90mmHg respectively, and the inadequate control of BP is confirmed by ABPM or HBPM in patients whose adherence to therapy has been confirmed.
The recommended treatment strategy should include appropriate lifestyle measures and treatment with optimal or best-tolerated doses of three or more drugs, which should include a diuretic, typically an ACE inhibitor or an ARB, and a CCB
Pseudo-resistant hypertension and secondary causes of hypertension should also have been excluded
The reasons of a true resistant hypertension:
Lifestyle factors such as obesity or large waist gains, excessive alcohol consumption and high sodium intake
Chronic intake of vasopressors, sodium retaining substances
Obstructive sleep apnoea
Undetected secondary forms of hypertension
Advanced and irreversible organ damages
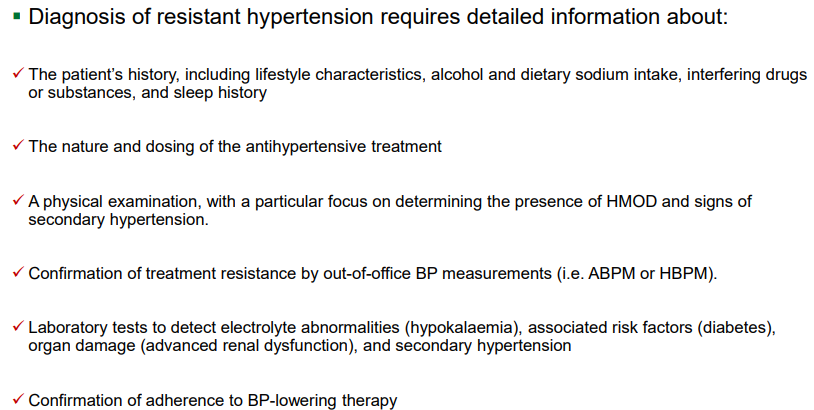
Diagnostic approach to resistant hypertension
Pseudo-resistant hypertension
The reasons of pseudo RH:
Poor adherence to prescribed medicines is a frequent cause of pseudo-resistant hypertension
White-coat phenomenon (in which office BP is elevated but BP is controlled at ABPM or HBPM) is not uncommon in these patients
Poor office BP measurement technique, including the use of cuffs that are too small relative to the arm circumference, can result in a spurious elevation of BP.
Marked brachial artery calcification, especially in older patients with heavily calcified arteries
Clinician inertia, resulting in inadequate doses or irrational combinations of BP-lowering drug therapies - doctors not giving enough dose of the medication
Classes recommendation and levels of evidence
Treatment of elevated blood pressure / hypertension
Two main treatment strategies:
Lifestyle interventions - can lower BP and in some cases CV risk, but most patients with hypertension will also require drug treatment
Pharmacological therapy
Data-based therapy
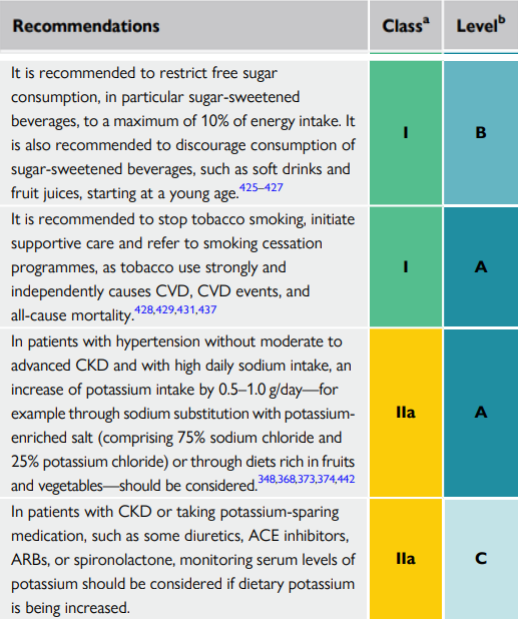
Non-pharmacological treatment of blood pressure and cardiovascular risk reduction
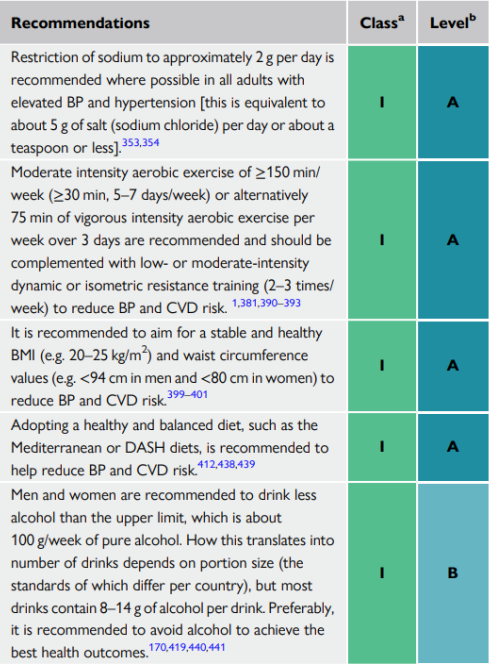
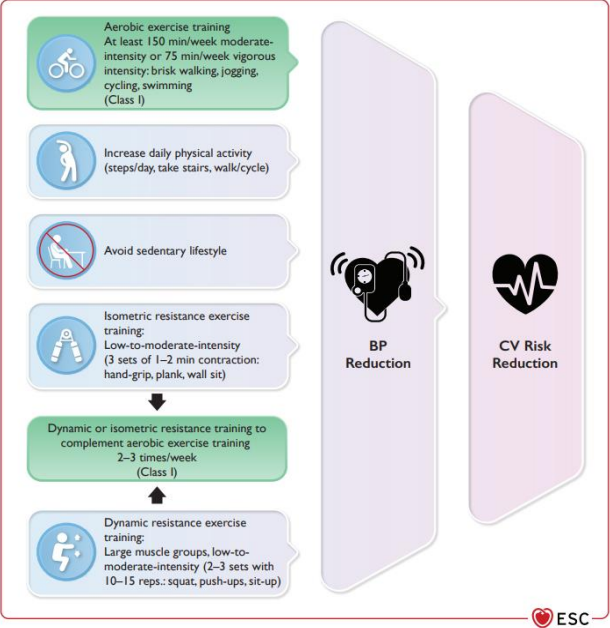
Physical Activity
Physical activity according to different types of exercise and reduction of blood pressure and overall cardiovascular disease risk.
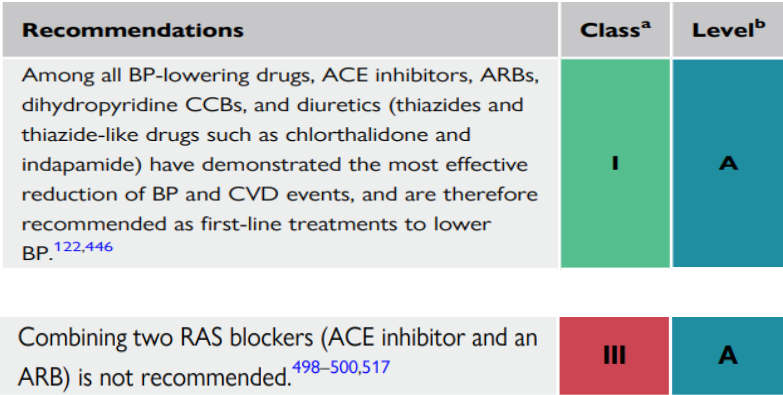
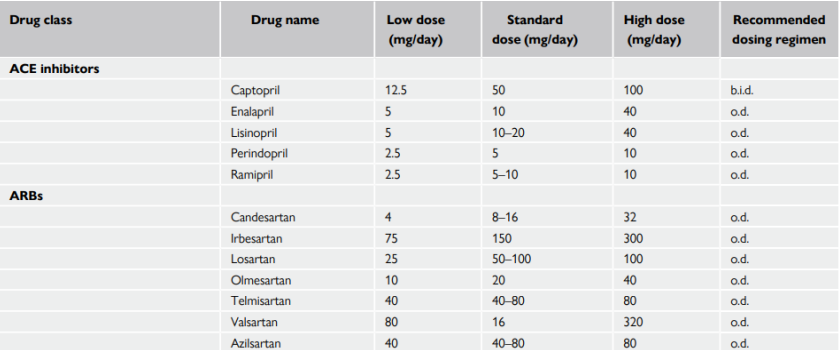
Pharmacological Therapy (Drugs)
Main groups (first line):
Diuretics (thiazides and thiazide- like)
Angiotensin-converting enzyme inhibitors (ACEI)
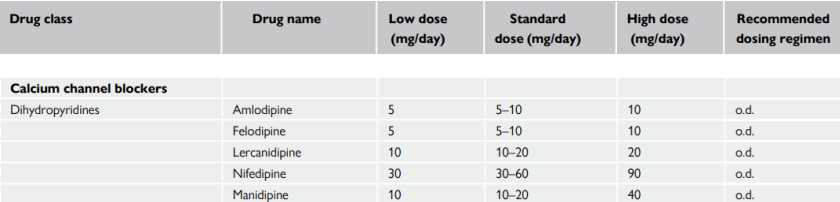
Calcium channel blockers - dihydropyridine (CCB-DHP)
Angiotensin receptor blockers (ARB)
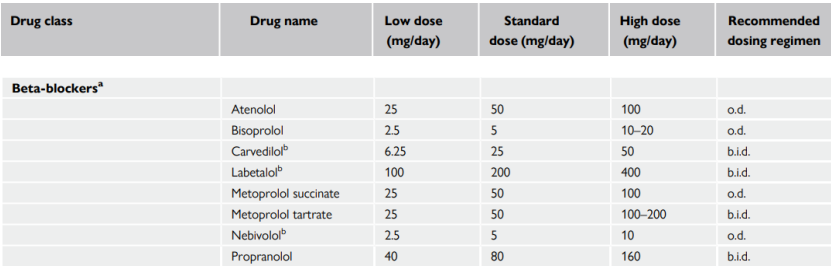
Beta-blockers (BB)
Others:
Mineralocorticoid receptor antagonists (MRAs)
Alpha -1- blockers
Central action drugs - methyldopa, clonidine, imidazoline receptor blockers
Loop diuretics
Alfa and beta receptor blockers
Direct vasodilatators (nitroglicerin, nitroprusid)
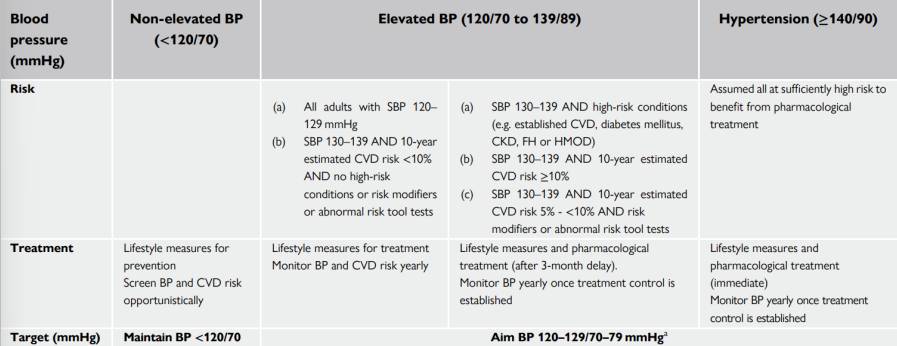
BP treatment targets
The first objective of treatment should be to lower BP to < 140/90 mmHg in all patients
Provided that the treatment is well tolerated, treated BP values should be targeted to 120-129/70 -79 mmHg
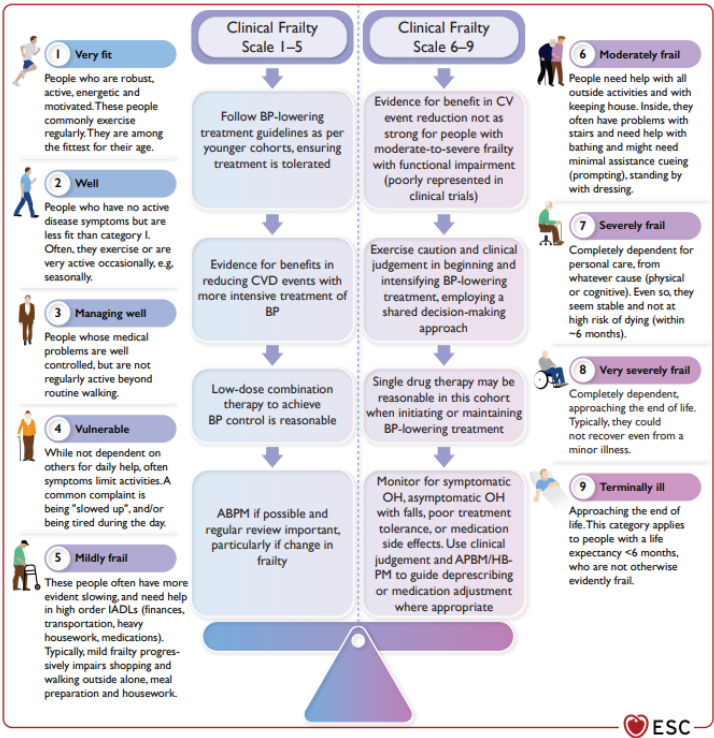
Personalised BP treatment targets can be instituted for people aged ≥85, those with moderate - -significant frailty at any age, and those with a limited predicted lifespan
In cases where BP-lowering treatment is poorly tolerated and achieving a systolic of 120–129 mmHg is not possible, it is recommended to target a systolic BP level that is ‘as low as reasonably achievable’
Angiotensin-converting enzyme inhibitors (ACEI) and Angiotensin receptor blockers (ARB)
Most widely used classes of antihypertensive drugs
Similar effectiveness as each other
ACE inhibitors and ARBs should not be combined for the treatment of hypertension - no added benefits, excess of renal adverse events
ACE inhibitors and ARBs reduce albuminuria, are effective at delaying the progression of diabetic and non-diabetic CKD, effective in preventing or regressing HMOD - such as LVH and small artery remodelling, reduce incident AF, indicated postmyocardial infarction and in patients with chronic HFrEF.
Calcium channel antagonists - dihydropyridine (CCB-DHP)
Widely used for the treatment of hypertension and have similar effectiveness as other major drug classes on BP
CCBs are a heterogeneous class of agents
CCBs have a greater effect on stroke reduction than expected for the BP reduction achieved, less effective at preventing HFrEF
More effective than beta-blockers in slowing the progression of carotid atherosclerosis, and in reducing LVH and proteinuria
Thiazide/thiazide-like diuretics (e.g. chlorthalidone and indapamide)
Diuretics appear to be more effective than other drug classes in preventing heart failure
Exhibit dysmetabolic effects that increase insulin resistance and the risk of new-onset diabetes
Both thiazides and thiazide-like agents are less effective antihypertensive agents in patients with a reduced GFR
In such circumstances, loop diuretics such as furosemide (or torasemide) should replace thiazides and thiazide-like diuretics to achieve an antihypertensive effect

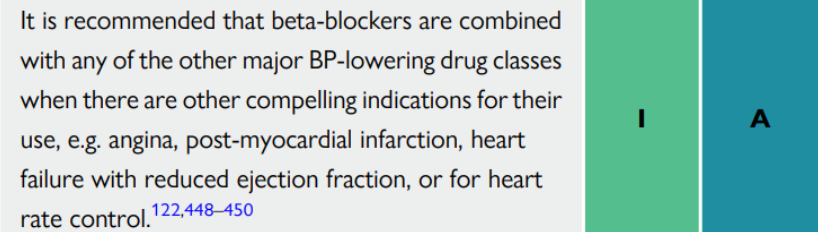
Beta-blockers
Beta-blockers significantly reduce the risk of stroke, heart failure, and major CV events in hypertensive patients.
Beta-blockers are usually equivalent in preventing major CV events, except for less effective prevention of stroke
Beta-blockers are useful for the treatment of hypertension in specific situations such as symptomatic angina, for heart rate control, post-myocardial infarction, HFrEF, and as an alternative to ACE inhibitors or ARBs in younger hypertensive women planning pregnancy or of child-bearing potential
Beta-blockers are less effective than RAS blockers and CCBs in preventing or regressing LVH, carotid IMT, aortic stiffness, and small artery remodelling.
Beta-blockers are also associated with increased risk of new-onset diabetes in predisposed subjects
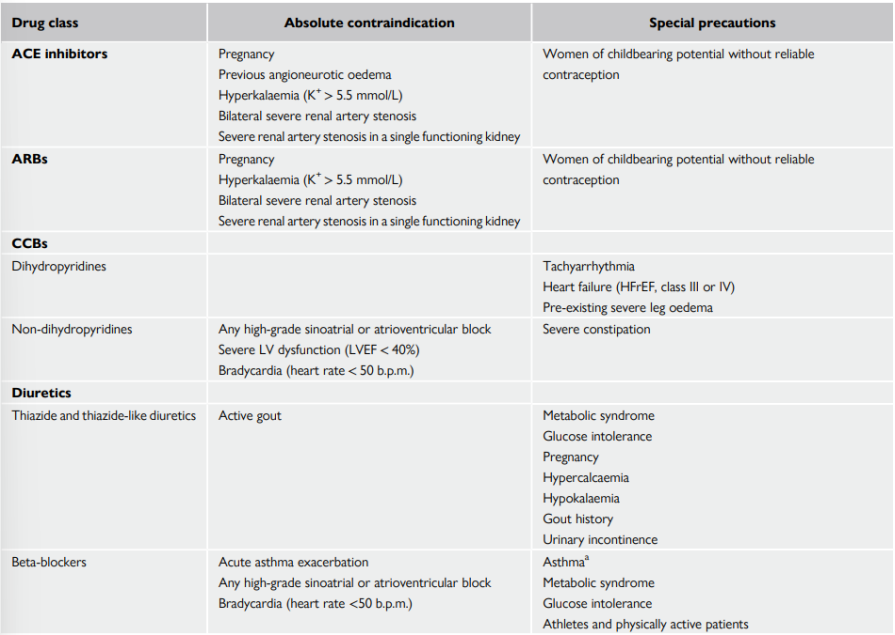
Drugs contraindications and special precautions
The Drug Treatment Algorithm for Hypertension
The initiation of treatment in most patients with an Single-pill Combination (SPC) comprising two drugs to improve the speed, efficiency, and predictability of BP control
Preferred two-drug combinations are a RAS blocker with a CCB or a diuretic. A beta-blocker in combination with a diuretic or any drug from the other major classes is an alternative when there is a specific indication for a beta-blocker, e.g. angina, post-myocardial infarction, heart failure, or heart rate control.
The Monotherapy can be used for patients aged ≥ 85, those with symptomatic orthostatic hypotension, moderate-to-severe frailty or elevated BP (120- 139/70-89 mmHg)
The use of a three-drug SPC comprising a RAS blocker, a CCB, and a diuretic if a two-drug SPC does not control BP
The addition of spironolactone for the treatment of resistant hypertension, unless contraindicated
The use of other classes of antihypertensive drugs in the rare circumstances in which BP is not controlled by the above treatments

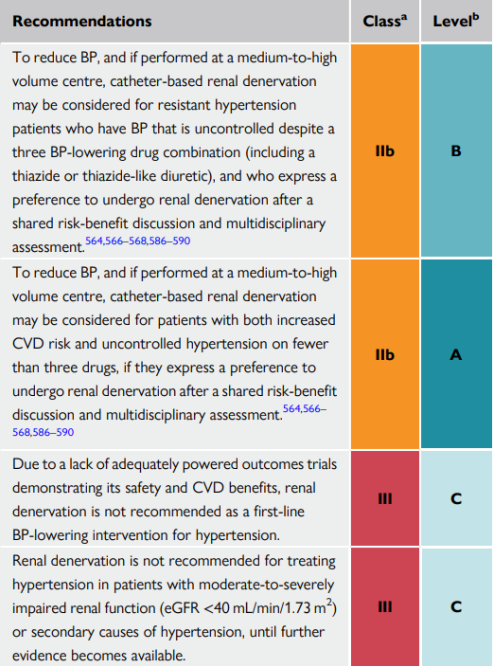
Device-based hypertension treatment
Use of device-based therapies is not recommended for the routine treatment or the first-line therapy of hypertension unless in the context of clinical studies and RCTs until further evidence regarding their safety and efficacy becomes available
Method:
Renal denervation
Bilateral destruction of the renal nerves travelling along the renal artery by radiofrequency ablation catheter
This causes reduction of sympathetic afferent and efferent activity to the kidney and blood pressure can be decrease

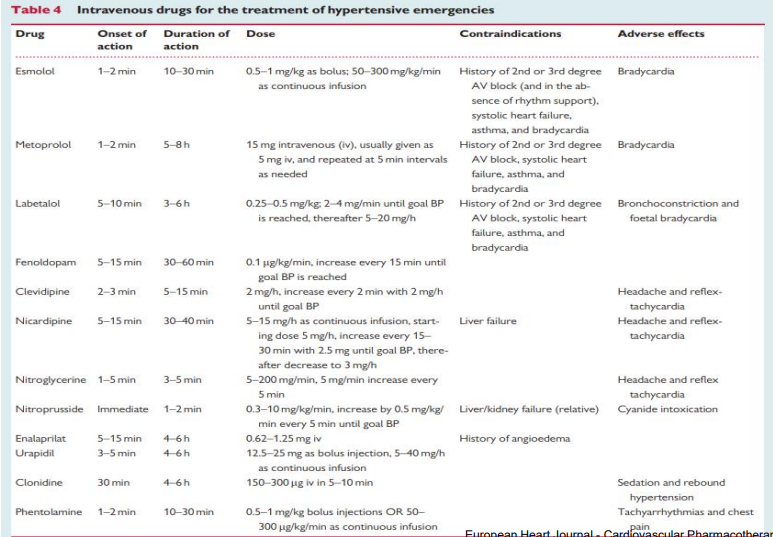
Hypertensive emergencies requiring immediate BP lowering
Intravenous (i/v) administration
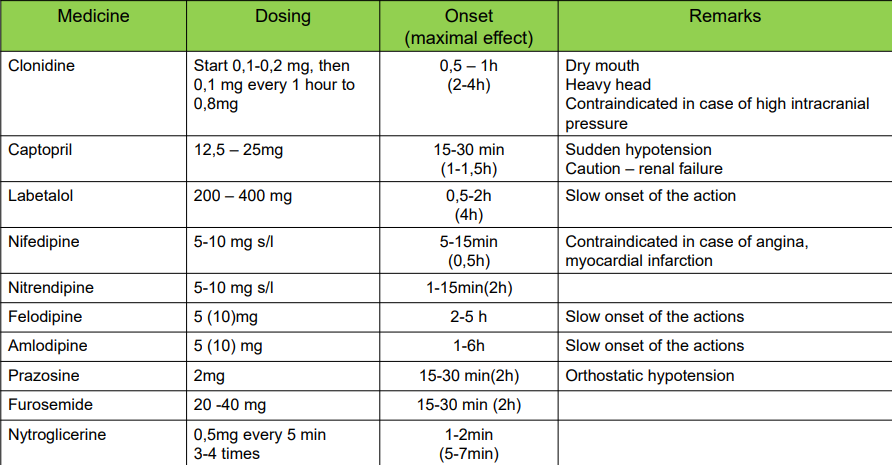
Hypertensive urgencies- treatment
Per oral administration (p/o)
Recommended pharmacological treatment of Resistant Hypertension
Reinforcement of lifestyle measures, especially sodium restriction
Addition of low-dose spironolactone to existing treatment
Or the addition of further diuretic therapy if intolerant to spironolactone, with either eplerenone, amiloride, a higher dose thiazide/thiazide-like diuretic, or a loop diuretic
Or the addition of bisoprolol or doxazosin
Management of resistant hypertension