Lesson 11
Lesson 11: Functional Residual Capacity (FRC)
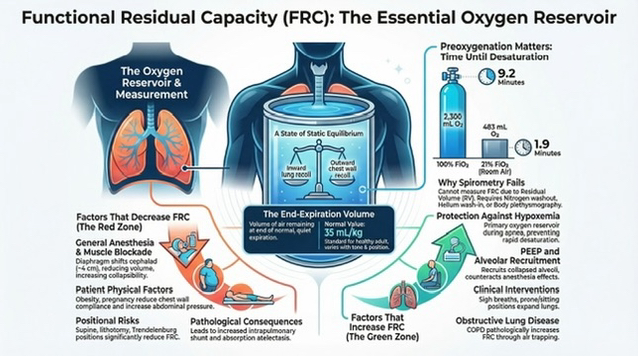
Volume of air in lungs at end-expiration.
Acts as oxygen reservoir to prevent hypoxemia during apnea.
At FRC, inward elastic recoil of lungs is balanced by outward elastic recoil of chest wall (static equilibrium).
Factors Affecting FRC
Decreasing FRC:
General Anesthesia (GA)
Obesity
Pregnancy
Supine Position
Fluid Overload
Increasing FRC:
Positive End-Expiratory Pressure (PEEP)
Advanced Age
Sigh Breaths
Prone or Sitting Positions
Measuring FRC
Indirect Measurement Methods:
Nitrogen washout
Helium wash-in
Body plethysmography
Cannot be measured via spirometry due to residual volume (RV) presence in FRC.
Normal FRC value: .
FRC Duration During Apnea
Estimated using:
Example for FRC = 2300 mL, VO2 = 250 mL/min:
Breathing 100% O2:
Breathing 21% O2: .
Clinical Implications of Altered FRC
Reduced FRC shortens apnea tolerance; critical during airway management.
Conditions that reduce outward lung expansion or lung compliance increase intrapulmonary shunt (West zone 3).
Alveolar recruitment maneuvers and PEEP help restore FRC and reduce shunting.
Common Conditions and Their Effects on FRC
General Anesthesia: Decreases FRC due to diaphragm shift and lung compliance.
Obesity & Pregnancy: Decrease FRC due to abdominal pressure influence.
Positioning: Supine, lithotomy, and trendelenburg position reduce FRC; upright position tends to increase it.
Neuromuscular Blockers & IV Fluids: May decrease FRC by impairing lung volume.
PEEP: Increases FRC, enhances lung recruitment, and prevents atelectasis.