Endocrinology Slides
Diabetes Mellitus
Terminology
Use correct medical terminology for:
Diabetes mellitus
Thyroid disorders
Adrenal disorders
Diabetes insipidus
Recommended Readings
Insulin and diabetes mellitus: ALL sections, Chapter 16 Endocrine System Disorders in Gould’s pathophysiology for the health professions (7th ed.).
Learning Outcomes
Describe the regulation of blood glucose by hormones in the body.
Describe the pathophysiology, etiology, clinical manifestations, monitoring tests and parameters, complications, and treatment of type 1 and type 2 diabetes mellitus.
Describe drugs in the following classes according to their generic and brand names, place in therapy, mechanism of action, pharmacokinetics, pharmacodynamics, precautions and contraindications, adverse effects, and auxiliary labels:
Insulin
Biguanides
Sodium-Glucose Cotransporter 2 Inhibitors (SGLT-2I)
Incretins
Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RA)
Dipeptidyl Peptidase-4 Inhibitors (DPP-4I)
Alpha-glucosidase Inhibitors
Insulin Secretagogues
Sulfonylureas
Meglitinides
Thiazolidinediones (TZDs)
Glucagon
Insulin and Diabetes Mellitus
The fundamental problem in diabetes mellitus is inadequate insulin (hormone) effects in receptor tissues caused by:
Deficit of insulin secretion AND/OR
Cellular insulin resistance
Diabetes results in abnormal carbohydrate, protein, and fat metabolism.
Deficit in protein and glycogen (storage of glucose) production.
Alterations in the transport of glucose and amino acids into cells.
Regulation of Blood Glucose
Blood glucose is normally maintained at:
Fasting
Postprandial (1 to 2 hours after the start of a meal),
Insulin and glucagon are peptide hormones secreted from endocrine cells in the islets of Langerhans in the pancreas.
Insulin is secreted from beta cells in response to high blood glucose levels.
Insulin lowers blood glucose, and glucose is transported into cells.
Glucagon is secreted from alpha cells in response to low blood glucose levels.
Glucagon raises blood glucose and converts stored glycogen into usable sugars.
Other Hormones Involved in Blood Glucose Control
Incretins act on the beta cells of the pancreas to stimulate insulin secretion.
Secreted by endocrine cells in the small intestine in response to glucose. yes to insulin
Amylin slows gastric emptying, suppresses glucagon secretion, and modulates appetite. decrease insulting
Secreted from beta cells along with insulin in response to elevated blood glucose levels.
Epinephrine and cortisol both antagonize the effects of insulin and increase blood glucose levels.
Epinephrine increases blood glucose levels and inhibits insulin secretion.
Cortisol (stress hormone) increases blood glucose levels to provide fuel and building blocks during adaptation and stress.
> better if more blood glucose so more fuel and use pgycogen storage
Types of Diabetes Mellitus
Type 1 Diabetes (DM1) either born with it or an autoimmune disease (usually much younger, found out before their birthday
Autoimmune destruction of beta cells
Absolute insulin deficiency
Type 2 Diabetes (DM2) (progressive disease, moniter the patients glucose levels to be
Insulin resistance and/or insulin deficiency
Usually, the beta cells are capable of secreting insulin, but secretion is impaired and eventually stops
Gestational Diabetes (GD)
Glucose intolerance with onset of pregnancy
People with GD have an increased risk of developing type 2 diabetes
Type 1 Diabetes
Etiology is an autoimmune destruction of beta cells in the pancreas
Absolute insulin deficit in the body
Insulin replacement required
Acute onset in children and adolescents
Not linked to obesity
Genetic factors may play a role
Type 1 Diabetes (DM1) 10% of people have this one
Metabolic changes:
Catabolism of fats and proteins
Excessive amounts of fatty acids and metabolites
Ketones in the blood (product of fat breakdown)
Ketonuria
Decrease in pH of body fluids (ketones are acidic)
Decreased serum bicarbonate
Ketones are excreted in urine (acidic byproduct in the body, which can cause diabetic keotonacidosis (has a fruity smell of the breathe) which is why some people do hte keto diet )
Decompensated metabolic acidosis
Medical emergency required
Type 2 Diabetes (DM2) (progressive disease)
90% of people with diabetes (lack of excercise, diabetes, genetics, eating habits)
Etiology is: dont make enough insulin , dont respond enough to insulin, and or too much glucose production in the liver)
Decreased production of insulin
Increased resistance by body cells to insulin
Increased production of glucose by the liver
Onset is slow and insidious, usually in those older than 50 years
Associated with obesity
Component of metabolic syndrome
Increasing incidence in teens and young adults
DM1 vs DM2 Characteristics & Symptoms *****
Feature | DM1 | DM2 |
|---|---|---|
Onset Age | Usually < 30 yrs; peak 12-14 yrs | Usually > 40 yrs; increasing prevalence among obese children |
Etiology | Autoimmune destruction of beta cells in the pancreas | Familial, lifestyle, environmental factors, obesity |
Clinical Presentation | Rapid onset; symptoms more severe and include weight loss and ketoacidosis | Symptoms are milder compared to Type I |
Body Weight | Thin | Obese |
Percentage of People w/ DM | 10% | 90% |
Pancreatic (β-cell) Function | Usually none | Insulin present in low, normal, or high amounts |
Treatment | Insulin + nutrition, physical activity, amylin mimetics (synthetic compounds that mimic the effects of the natural hormone amylin) | Oral antihyperglycemic agents + nutrition, physical activity, insulin, amylin mimetics |
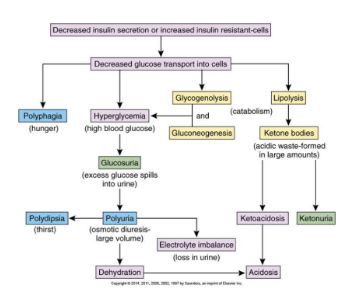
Pathophysiology of Insulin Deficit / (urine sweeter?, pee more, hungrier, DEHYDRATED )
Decreased transportation < 🚎 and use of glucose 🍦 in many cells causes: =
Hyperglycemia – blood glucose levels rise
Glucosuria – excess glucose in urine
Glucose in the filtrate exceeds the capacity of the renal tubules to resorb it
Polyuria – large urine volume
Osmotic pressure due to glucose load
Polydipsia – dehydration causes thirst
Polyphagia – lack of nutrients in cells stimulates appetite
Dehydration – fluid loss through urine
Accompanying losses of sodium and potassium
3 Ps!
Polyuria
Polydipsia
Polyphagia
Progressive Manifestations
If insulin deficits are severe or prolonged: 🫥
Lack of glucose in cells = the body uses fats and proteins for energy
Metabolite of fat catabolism = ketones (acetone + 2 organic acids)
Eventual decrease in body pH (ketones are acidic)
Ketonuria – ketones are present in urine
Buffers are eventually overwhelmed, and dehydration is occurring (from polyuria), leading to a decompensated metabolic acidosis
Diabetic ketoacidosis (DKA)
Treatable, but very dangerous and can be life-threatening
Diagnostic Tests
Fasting blood glucose level
8 hours since food
Diagnostic level + not producing enough insulin
Glucose tolerance test
Oral glucose tolerance test (OGTT) – 2 hours after 75 gram of oral glucose
Diagnostic level + if they dont come down to 11.1, most likely diabetic
Glycosylated hemoglobin test
Glycosylated hemoglobin (A1C) = HbA1C must used test
Average glucose control over 8-12 weeks
Diagnostic level
Targets for Glycemic Control
HbA1C (blood test, lab tests it and gives the result) | Fasting or Preprandial Glucose | 2-hour Postprandial Glucose | |
|---|---|---|---|
DM 1 and 2 | < or = 7% | ||
(if A1C targets not being met ) | |||
Normal Range | < or = 6% |
Treatment Principles
Lifestyle modification
Diet and exercise under the guidance of health professionals
Treatment goals are to maintain blood glucose levels in the normal range
DM1 patients require insulin
DM2 patients may require initiation of insulin, other antihyperglycemic pharmacotherapy, or lifestyle modifications alone
Self-Monitoring of Blood Glucose
Conducted by the patient at home using a blood glucose monitor
Frequency of testing is dependent on the patient
DM1
Recommended that testing occur times per day
2 hours after lunch
2 hours after dinner
Bedtime
Frequent testing guides lifestyle and food choices and pharmacological therapy
Illness/infection warrants more frequent testing (will change insulin requirements)
DM2
Frequency of testing not as clear for individuals managed with lifestyle and/or oral antihyperglycemics
If taking insulin frequency should be the same as that recommended for type 1 DM
Insulin Types
Basal Insulins (once daily)
Ultra-long-acting
Long-acting
Intermediate-acting
Bolus (Mealtime) Insulins (take at meat times to reduce spikes)
Fast-acting
Regular-acting
Premixed Insulin (long and short acting in them)
Basal-Bolus Secretion
Goal of insulin therapy is to mimic physiological levels of insulin:
Basal secretion - the pancreas constantly secretes small amounts of insulin throughout the day
Bolus secretion - the pancreas secretes a larger amount of insulin response to a meal
Insulin therapy in type 1 diabetes combines different types of insulin with different durations of action to mimic basal-bolus secretion
Insulin Products
All insulin preparations in Canada are prepared using recombinant DNA technology (use recombinant DNA to chemically copy the insulin in a human’s body)
MOA
Structurally identical to human insulin
Preparations are classified based on their duration of action, time of onset, and peak actions
Kinetics and Dynamics
Insulin analogues which are modified to change their pharmacokinetics
Most common route of administration is subcutaneous
Regular insulin can be given intravenously in hospital settings
Subcutaneous Administration
Site should be rotated within the same anatomical region
Absorption is:
Fastest from the abdomen
Intermediate in the arm
Slowest from the thigh Ex. 1 basal in the morning, 3 bolus during the day
Insulin Packaging
Commercially available as:
Vials
10 mL
Use needles and syringes to draw insulin out of vials
Cartridges (also called Penfills)
3 mL x 5 per box (15 ml in total)
Used with reusable insulin pens and disposable needle tips (pen tips)
Pre-filled disposable pens ( after usage once, okay for 28? days)
3 mL x 5 per box (15 mL in total)
Used with needle tips (pen tips) and then discarded when empty
Insulin is dosed in units
100 unit/mL standard concentration for most insulins
Concentrated solutions are available in hospital and are denoted “U200”, “U300”, or “U500”
Caution: potential for lethal errors
Wegovy and ozempic are insulin like drugs, weekly injectable, diff type of meds but same type of giving out
Insulin Considerations
ROLLING/SHAKING
Insulins that are CLEAR do NOT need shaking prior to use
Insulins that are CLOUDY DO need rolling to mix prior to use
SHAKE GENTLY MIXING INSULINS
Some insulins (like Lantus® and Levemir®) form a precipitate in subcutaneous tissue after injection and these can NEVER be mixed with other insulins
Injection sites should be well spaced from other insulins
STORAGE AND STABILITY
Most insulins are stored at 2oC to 8oC at the pharmacy and before first use
KEEP IN FRIDGE; DO NOT FREEZE,,, after first use can stay outside
Once brought to room temperature, insulins can usually be used for one month (refer to product monograph)
CALCULATE BEYOND USE DATE WHEN DISPENSED
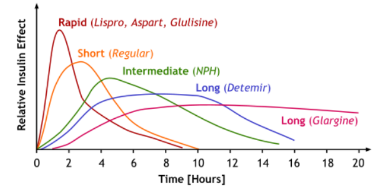
Relative Insulin Effects over Time
The relative effects of rapid, short, intermediate, and long-acting insulins over time are visually represented in a graph.
Basal Insulin Ultra-Long-Acting
Products
degludec (Tresiba®)
U100 and U200
glargine (Toujeo® U300),
Kinetics and Dynamics
SC dose once daily HS or BID (split a dose)
Duration of action is 36 to 42 hours
Precautions and Adverse Effects
Clear insulin = DO NOT SHAKE
Do not mix with other insulins
STORE IN THE FRIDGE; DO NOT FREEZE
CALCULATED BUD AT ROOM TEMPERATURE (usually a month)
Basal Insulin Long-Acting
Products
glargine (Lantus®); biosimilar glargine (Basalglar®)
detemir (Levemir®)
Kinetics and Dynamics
SC dose once daily HS or BID
Duration of action is hours
Precautions and Adverse Effects
Clear insulin = DO NOT SHAKE
Do not mix with other insulins
STORE IN THE FRIDGE; DO NOT FREEZE
CALCULATED BUD AT ROOM TEMPERATURE (usually a month)
Basal Insulin Intermediate-Acting
Products CLoudy INSULINE SHAKE GENTLY
insulin isophane (Humulin® N)
insulin isophane (Novolin® ge NPH)
Kinetics and Dynamics
SC dose once daily HS or BID
Precautions and Adverse Effects
Cloudy insulin = SHAKE GENTLY
STORE IN THE FRIDGE; DO NOT FREEZE
CALCULATED BUD AT ROOM TEMPERATURE (usually a month)
Bolus (Mealtime) Insulin Fast-Acting
Products CLEAR INSULIN = DO NOT SHAKE
insulin aspart (Fiasp®)
Ultra-fast acting! Onset of action is 4 minutes
insulin aspart (NovoRapid®); biosimilar aspart (Trurapi®)
insulin glulisine (Apidra®)
insulin lispro (Humalog®); biosimilar lispro (Admelog®)
Humalog U100 and U200
Kinetics and Dynamics
SC dose 0 to 15 minutes before (or within 20 min of) a meal
Insulin lispro, glulisine, and aspart can be used in insulin pumps (pump insulin into body and put into blood stream)
Precautions and Adverse Effects
Clear insulin = DO NOT SHAKE
STORE IN THE FRIDGE; DO NOT FREEZE
CALCULATED BUD AT ROOM TEMPERATURE (usually a month) 28 days based on monograph, (KNOW which insulins fit into each category)
Bolus (Mealtime) Insulin Regular-Acting
Products
insulin regular (Humulin® R) (Novolin® ge Toronto)
Kinetics and Dynamics
SC dose 30 to 45 minutes before a meal
Onset of action is 30 minutes
Precautions and Adverse Effects
CLEAR insulin = DO NOT SHAKE
STORE IN THE FRIDGE; DO NOT FREEZE
CALCULATED BUD AT ROOM TEMPERATURE (usually a month)
Premixed Insulins
Products CLOuDY = SHAke Gently
cinsulin lispro/lispro protamine (Humalog® Mix25, Mix50)
insulin aspart/aspart protamine (NovoMix® 30)
Kinetics and Dynamics
SC dose BID 0–15 min before or within 20 min of a meal
Precautions and Adverse Effects
Cloudy insulin
SHAKE GENTLY
STORE IN THE FRIDGE; DO NOT FREEZE
CALCULATED BUD AT ROOM TEMPERATURE (usually a month)
Insulin Pumps
Insulin pumps provide a continuous supply of insulin to mimic basal secretion and allow for bolus doses in association with meals
A reservoir within the pump contains fast-acting insulin
Insulin lispro, glulisine, or aspart
An infusion set is used to deliver insulin into subcutaneous tissue
Some pumps can be interfaced with blood glucose monitors
Precautions and Adverse Effects
Hypoglycemia (too much = drops blood sugar)
Lipohypertrophy at the site of injection
Rare hypersensitivity reactions
Drugs that affect glycemic control
Beta-blockers
Mask symptoms of hypoglycemia
Alcohol
Acutely, blood glucose will drop (when the liver is processing alcohol, it stops releasing glucose)
Over time, excessive alcohol consumption (> 3 drinks a day) can reduce the overall effectiveness of insulin = higher HbA1C
Drugs that increase blood glucose:
Sympathomimetics (mimics sympathetic nervous system?), strenuous exercise
Corticosteroids
Thiazide and loop diuretics
Niacin
Estrogens
know which wh insulins fall in what category, main things about storage, clody vs clear*
Antihyperglycemic Agents
Biguanides
Sodium-Glucose Cotransporter-2 Inhibitors (SGLT-2I)
Incretin Mimetics
Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RA)
Dipeptidyl Peptidase-4 Inhibitors (DPP-4I)
Alpha-glucosidase Inhibitors
Insulin Secretagogues
Sulfonylureas
Meglitinides
Thiazolidinediones (TZD)
Management of DM2
Initial management generally depends on the HbA1c
In patients with an HbA1c at or near their target
Nonpharmacologic therapy alone (e.g., diet and exercise) for 3 months
If targets are not met in 3 months:
Monotherapy with metformin (Brings down A1c, very common , but causes stomach irritation, and slowly introduce it with meals) is the drug of choice, or
Combination of oral agents and/or insulin
In patients with an HbA1c well above their target
Pharmacotherapy is started immediately (along with diet and exercise)
Combination therapy (metformin combined with another drug, possibly hs insulin)
The goal of pharmacotherapy is to reach their HbA1c target within 3 to 6 months
Dosage titration and/or addition of other agents
Nonpharmacological Management
Self-management education is vital for patients to be full participants their own care
Nutritional management with a registered dietitian to personalize goals and tailor a dietary plan
Blood glucose monitoring is essential to manage diabetes well
Exercise
Physical activity can improve cardiovascular function, enhance insulin sensitivity, and lower blood pressure and lipid levels
Encourage aerobic exercise totaling minutes per week with resistance training at least twice a week,,, Eye exams every year
Ongoing monitoring of other organ systems
Blood pressure measurements, foot examinations, bloodwork to monitor renal function and lipid profiles, ophthalmologist/optometrist for eye examinations
Biguanides
Products FIRST LINE TO USE
metformin (Glucophage®)
metformin SR (Glumetza®)
DO NOT CRUSH OR CHEW AND TAKE WITH FOOD
many combination products
Place in Therapy
First choice for patients with a new and uncomplicated DM2 diagnosis
MOA
Primarily, it decreases hepatic glucose production
It also lowers glucose absorption and enhances insulin-mediated glucose uptake (decreases glucose production in the liver)
Kinetics and Dynamics
Oral medications
Drug interactions:
Alcohol = Increased risk of lactic acidosis and potentiates hypoglycemic effects
Renal contrast dyes
Precautions and Adverse Effects
Minimal risk of hypoglycemia when used as monotherapy
Significant nausea, diarrhea, metallic taste
“Start low and go slow” to minimize GI side effects
TAKE WITH FOOD
Does not promote weight gain (weight neutral)
Lactic acidosis (rare)
Contraindicated in patients with hepatic impairment, severe renal impairment or previous lactic acidosis
Sodium-Glucose Cotransporter 2 Inhibitors (SGLT-2I)
Products
canagliflozin (Invokana®)
dapagliflozin (Forxiga®)
empagliflozin (Jardiance®)
Place in Therapy
Well tolerated option in DM2 with minimal risk of hypoglycemia
Proven cardiorenal benefits in high-risk populations
MOA
Prevent glucose reabsorption in the kidneys, leading to increased excretion of urinary glucose and a lowering of blood glucose
Kinetics and Dynamics
Oral medications
Many drug interactions: SGT-2Is are strong CYP enzyme inducers (lowers to increase?) peeing glucose out, leving the body = less fat = weight loat)
Precautions and Adverse Effects
Increased risk of genitourinary infections
Reduced intravascular volume = hypotension (especially with loop diuretics)
Hyperkalemia
Risk of diabetic ketoacidosis
Some weight loss is associated with SGLT-2Is
Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RA)
Products
Short acting (works on post-prandial glucose = given with meals)
exenatide subcut bid (Byetta®)
lixisenatide subcut daily (Adlyxine®)
Long-acting (without regards to meals)
dulaglutide subcut weekly (Trulicity®)
liraglutide subcut daily (Victoza®)
semaglutide subcut weekly (Ozempic®),, mtizaritide?,
Oral
semaglutide oral once daily (Rybelsus®)
Daily on an EMPTY STOMACH upon waking, with only MINIMAL WATER and NOTHING ELSE FOR 30 MINUTES (no other food, drink or medications)
Place in Therapy
Well tolerated option in DM2 with minimal risk of hypoglycemia
Proven cardiorenal benefits in high-risk populations
MOA
Mimic the actions/agonist of GLP-1 (an endogenous incretin hormone) that is secreted in response food ingestion
GLP-1 increases insulin secretion, suppresses glucagon secretion, slows gastric emptying, and increases satiety
Kinetics and Dynamics
Gradual dose increase over weeks to months
Precautions and Adverse Effects
Significant nausea, and possible vomiting and diarrhea
Rare acute pancreatitis
Caution in patients with arrhythmias and severe renal impairment
Causes weight loss (slows gastric emptying = feel full longer)
Dipeptidyl Peptidase-4 Inhibitors (DPP-4I)
Products
alogliptin (Nesina®)
linagliptin (Trajenta®)
saxagliptin (Onglyza®)
Saxagliptan (Onglyza®) must be avoided in patients with heart failure; ++ interactions
sitagliptin (Januvia®)
Place in Therapy
Well tolerated option in DM2, decrease HbA1C with minimal risk of hypoglycemia
CV safety but NO proven cardiorenal benefit
MOA
Increases the availability of GLP-1 (by preventing the enzyme that breaks it down)
GLP-1 increases insulin secretion, suppresses glucagon secretion, slows gastric emptying, and increases satiety
Kinetics and Dynamics
Drug interactions – only with saxagliptan (Onglyza®)
Taken orally once daily with or without food
Precautions and Adverse Effects
Nasopharyngitis
Hypersensitivity reactions
Rare pancreatitis and severe joint pain
Saxagliptin (Onglyza®) must be avoided in patients with heart failure
Alpha-Glucosidase Inhibitors
Products
acarbose (Glucobay®)
Place in Therapy
Well tolerated option in DM2; minimal risk of hypoglycemia so monitored, 3-4th line agent for dm2
CV safety but NO proven cardiorenal benefit
MOA
Inhibits the intestinal enzyme alpha-glucosidase which breaks down complex polysaccharides into simple sugars
Acarbose delays the absorption of carbohydrates which improves postprandial glucose control
Kinetics and Dynamics
Taken orally with the first bite of each meal (tid)
Start low and titrate slowly to minimize GI adverse effects!
Potentiate the effect of other antihyperglycemics
Precautions and Adverse Effects
Flatulence, diarrhea, abdominal pain, cramps, and nausea
Contraindicated in irritable bowel syndrome and inflammatory bowel disease ((USE glucose to treat hyperglycema)
Secretagogues: Sulfonylureas
Products
glicazide (Diamicron®, Diamicron MR®)
MR (long acting) = DO NOT CRUSH OR CHEW
glyburide (generics)
Place in Therapy
Agents have CV safety, but NO proven cardiorenal benefits
Risk of hypoglycemia
MOA
Enhance secretion of insulin by pancreatic beta cells
Stimulate both basal and mealtime insulin release
Must have functioning beta cells for these drugs to work! (no dm1, it would not work)
Kinetics and Dynamics
Given orally once or twice daily
Hypoglycemic effects are potentiated by salicylates, sulfonamides, MAOIs, and other oral antihyperglycemics
Precautions and Adverse Effects
TAKE WITH FOOD
Hypoglycemia
Weight gain
Avoid in / constraindicated in those with sulfa allergy and with decreased kidney function
Secretagogues: Meglitinides
Products
repaglinide (GlucoNorm®)
Place in Therapy
Agents have CV safety, but NO proven cardiorenal benefits
Risk of hypoglycemia
MOA
Enhance secretion of insulin by pancreatic beta cells
Stimulate both basal and mealtime insulin release
Must have functioning beta cells for these drugs to work!
Kinetics and Dynamics
Given orally 0 to 30 minutes before meals
More rapid onset and shorter duration of action compared to sulfonylureas
Useful in individuals who have irregular mealtimes
Affected by drugs that induce or inhibit CYP3A4 = many interactions
Precautions and Adverse Effects
Hypoglycemia (especially if not taken a meal)
TAKE WITH FOOD
Weight gain
Thiazolidinediones (TZD)
Products
pioglitazone (Actos®)
rosiglitazone (Avandia®)
Health Canada requires that physicians counsel patients and obtain their written consent for all new and renewed rosiglitazone prescriptions because of the increased risk of MI (heart attack)
Place in Therapy
Agents have a risk of heart failure and cause weight gain
MOA
Insulin ‘sensitizers’
Influence gene expression in the cell leading to enhanced insulin sensitivity, and lower levels of blood glucose and circulating insulin
Kinetics and Dynamics
Potentiates effects of other antihyperglycemic agents
Gemfibrozil inhibits metabolism and increases plasma levels
Insulin (associated with increased incidence of edema and worsening of heart failure)
Precautions and Adverse Effects
Weight gain
Edema
Worsening of heart failure
Macular degeneration
Rosiglitazone: significantly increases the risk of heart attack; requires consent in Canada
Pioglitazone: Increased risk of fractures; may increase risk of bladder cancer
QUICK REVIEW:
Basal = long acting, continual secretion throughout the day
bolus = immediate in response to food / calories
sc administration rotated around in the same site. thigh/glutes slowest, stomach/abdomen fastest
standard concentration for most insulins = 100U/mL
Premixed insulins which are cloudy need gentle shaking before administration like insulin isophane
3 bolus insulins that are fast acting, given aroind 15 minutes before meals, aspart / flasp/ novorapid, trurapi, apidra, humalog, admelong
Complications of Diabetes Mellitus
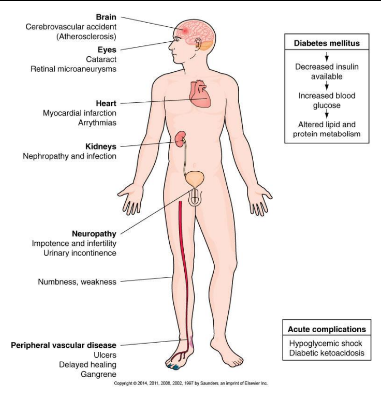
Describe the complications of diabetes mellitus, including hypoglycemia, diabetic ketoacidosis, microangiopathy, macroangiopathy, infections, and cataracts
Complications are directly related to duration and extent of abnormal blood glucose levels
Acute complications
Hypoglycemia and diabetic ketoacidosis (DKA) (low blood glucose)
Chronic complications
Macrovascular, microvascular, and infection (high blood glucose)
Hypoglycemia (Low blood glucose)
More common with insulin treatment
Can occur with some hypoglycemic drugs
Excess insulin in circulation = glucose deficit in blood
Can be life-threatening or cause brain damage if untreated (below 3?,,,
Causes
Strenuous exercise
Dosage error
Vomiting
Skipping meal after taking insulin
Pathophysiology of Hypoglycemia
Excess insulin in blood
Increased transport of glucose into cells
Hypoglycemia
Decreased CNS function = little to no glucose in the blood
Stimulates SNS
Clinical signs:
Weakness, confusion
Pallor
Diaphoresis
Tremors
Increased gluconeogenesis (making glucose out of other particles, like fat proteins and muscles)
Excess insulin transports glucose into cells (IF there is a glucose intake, return to normal state)
No glucose intake
Blood glucose levels decrease further
Neurons cannot function
Coma and death
Signs & Symptoms of Hypoglycemia
Disorientation and change in behavior
May appear impaired
Anxiety or decreased responsiveness
Decreased blood glucose level
Decreased BP, increased heart rate
Decreasing level of consciousness
Immediate administration of glucose is required to prevent brain damage
Treatment of Hypoglycemia
Check blood glucose immediately
No meter? Treat the symptoms anyway!
Eat or drink a fast-acting carbohydrate (15 grams of glucose)
125 mL (1/2 cup) of juice or regular soft drink
15 mL (1 tablespoon) of honey or jam/jelly
15 mL (3 teaspoons) or 3 packets of table sugar dissolved in water
6 Life Savers® (hard candies are not preferred due to choking risk)
Wait 10 to 15 minutes, then check the blood glucose again
If it is still low: treat again!
If the next meal is more than one hour away (or physical activity is anticipated) eat a snack with 15 grams of carbohydrate and a protein source
Like a half-sandwich or cheese and crackers
If unconscious, call 911
Give nothing by mouth
IV glucose is required
**DIABETIC KETOACIDOSIS = high blood glucose also causes a loss of consciousness, assessment should be done to check the cause
Glucagon
Products
glucagon (powder for reconstitution for subcut, im or iv injection)
Place in Therapy
Emergency treatment of severe hypoglycemia in unconscious patients treated with insulin
MOA
Hormone that causes an increase in blood glucose by converting liver glycogen to glucose
Kinetics and Dynamics
Patients typically respond within 10 minutes of subcut or im injection
Precautions and Adverse Effects
Severe adverse reactions are very rare
Nausea, vomiting, or hypokalemia may occasionally occur
Diabetic Ketoacidosis (DKA)
Occurs most commonly in DM1, can occur in DM2 if insulin dependent
The cause is insufficient insulin in blood which cause hyperglycemia (high sugar in the blood)
May result from error in dosage (underdosage), serious infection, change in diet, alcohol intake, exercise, or prolonged stress
The body mobilizes and uses lipids and proteins to meet cellular needs, which results in the production of ketoacids
Development of DKA
DKA Signs amd Symptoms
• Thirst
• Dry oral mucosa and skin
• Rapid pulse (but may be weak)
• Blood pressure is low (vascular volume decreases, vasodilation)
• Kussmaul respirations – fast, deep respirations
• Sweet, fruity-smelling breath – caused by acetone in the blood
• • Indicates depression of the central nervous system
Headache, lethargy and decreased responsiveness
• • Electrolyte imbalances cause abdominal cramping, nausea, and weakness
• Compensatory mechanisms to conserve fluid in the body begin Polyuria, then oliguria
Pathophysiology and Treatment of DKA
Ketones bind with bicarbonate ions in the blood
buffering system
• Decreased blood bicarbonate
As dehydration progresses the renal buffering
systems become overwhelmed, and acidosis
worsens
• Decreased blood pH
• Decompensated metabolic acidosis
• Coma is possible
Intravenous Treatment
• Extracellular fluid volume contraction
• Correct potassium deficit
• Insulin administration
• Correct serum osmolality
Vascular complications of DM microangiopathy
• Basement membrane of capillaries and small arteries become thick and hard
Leads to obstruction or rupture = tissue necrosis and loss of function
Eyes = retinopathy, Microaneurysms, neovascularization, and fibrosis in the retina
• Leads to blindness
Kidneys: nephropathy: Vascular degrenation in the kidney glomeruli, leads to chronic renal failure, some antihyperglycemics and antihypertensives have acardiorenal benefits (some of thesese are GLP -1RA, SGLT-21, ACEIs, ARBs)
Nerves: Neuropathy which is peripheral and autonomic: • Ischemia of neurons, as well as metabolic abnormalities that
cause myelin degeneration change nerve conduction
• Peripheral • Impaired sensation in extremities
• Burning, tingling, weakness, and muscle wasting
• Autonomic • Impaired gastric motility
• Erectile dysfunction
• Urinary incontinence
Vascular Complications of DM Macroangiopathy
Atheroscelerosis in large arteries, related to hyperlipidemia, hypertension, and DM related changes to the arterial intima, I.E. myocardial infarction, strokes, peripheral vascular disease like ischemia, necrosis, and gangrene can lead to lower limb amputation
Statistically: 60-80% of people with DM die of heart disease, the risk of stroke is 50% higher in persons with diabetes, and is the leading cause of non-traumatic leg amputations
Other complkcations of Diabetes Mellitus
Infections, are more frequent nd more severe, infections in lower body caused by vasucalr and neurologic impairment , candida fungal infections, rurinary tract infections, dental caries, gingivitis, and periodontitis
Cataracts: abnormal metabolism of glucose causes damage to the lens
Complications in Pregnancy: in both mother and fetus may occur, more chance of miscarriage, infants may have increased size and weight and may experience hypoglycemia in first hours postnatally
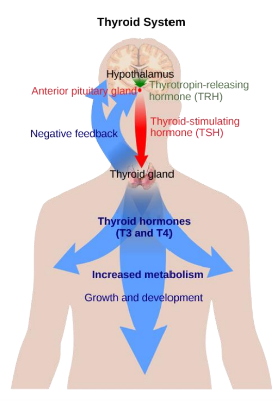
Thyroid Disorders
thyroid gland (in the throat) traps iodine and uses it to create two thyroid hormones, t# and t4 = thyroixine
release in response to TSH from pituitary, disroders may result from pituitary or thyroid gland dysfunction
start teratment when its high, so increase dose to decrease tsh more as its too high
Goiter
Goiter is an enlargement of the thyroid gland caused by hypo OR hyper thyroid conditions
Endemic goiter (Hypothyroid condition in regions with low iodine levels in soil and food, dietary deficiency leads to hyperplasia and hypertrophy in the thyroid gland
Goitrogens (foods and drugs that block synthesis of triiodothyroxine and thyroxine
Toxic goiter (hyoerthyroid condition caused by an overactive thyroid gland)
Hyperthyroid Graves disease
related to autoimmune factor most common in females over 30
hypermetabolism and increased stimulation of SNS (intolerance to heat, increasemetabolism, thin with increased appetite, flushed and warm skin, tachycardia, restless tremors and insomnia )
toxic gioter
expophthalamos (presence of protruding staring eyes, decreased blink and eye movement, result of increased tissue mass in the orbit, may result in visual impairment)
Treatment of hyperthyroidism
surgical removal of the thyroid gland and or administartion of radioactive iodine, induces hypo thyroidism
pharmacotherapy:
thioamides or iodine can be used to suppress thyroid function
beta blockers are used to suppress sympathetic overstimulation
corticosteroids are used tin treatment resistant cases
Thioamides
• • • Preferred agent
methimazole (Tapazole®)
• • Only used in the 1st trimester of pregnancy
propylthiouracil (PTU)
Products
• • Antithyroid drugs are used to make people euthyroid (either long-term or before surgery)
Place in Therapy
• • Decrease the production of T3 and T4; PTU also inhibits peripheral conversion of T4 to T3
MOA
• • Rash, allergic reaction, or agranulocytosis
• Rare hepatotoxicity or nephrotoxicityPrecautions and Adverse Effects
Hypothyroidism
Possible causes:
• Mild hypothyroidism is common
• • Iodine deficit
• Hashimoto thyroiditis (an autoimmune disorder)
• • Surgical removal or treatment of gland, 131I treatment, drugs such as
lithium, amiodarone, and sulfonylureas
Iatrogenic
• Pituitary dysfunction
• Congenital
Signs and Symptoms of hypothyroidism
• Intolerance to cold
• • Weight gain with decreased appetite
Decreased metabolism
• Skin is pale and cool
• Bradycardia, enlarged heart
• Lethargic, slow CNS functioning
• Goiter (if cause is endemic iodine deficiency)
• SEVERE CASES: myxedema coma
• Facial puffiness and thick tongue (due to edema)
• Hypotension, hypoglycemia, hypothermia
Treatment of hypothyroidism
• The treatment goal is to normalize TSH
• • Levothyroxine (L-T4)
• Liothyronine (T3)
• Desiccated thyroidPharmacotherapy with thyroid hormones
Levothyroixine
• • levothyroxine (Eltroxin®, Synthroid®) (controversy regarding the interchangeability of synthroid and eltroxin, patients should be maintained on one brand through dose adjustments)
Products
• • Levothyroxine is the treatment of choice for hypothyroidism
Place in Therapy
• • Hormone replacement therapy
MOA
• Dosage adjustments are made at 6-week intervals (6 weeks to steady
state)
• • • “Either ALWAYS take it on an empty stomach (preferred), OR ALWAYS take it with food”
Food and drink CAN significantly change absorption so EMPTY STOMACH; BUT the
monograph also suggests CONSISTENCY WITH REGARDS TO MEALS
Absorption may be reduced by antacids, calcium salts, cholestyramine
(separate administration by 6 hours), colestipol, and iron salts
Kinetics and Dynamics
Precautions and Adverse Effects
• • Symptoms of hyperthyroidism if overtreated!
• Other disease conditions may vary when thyroid is regulated (e.g.
anticoagulation with warfarin, glycemic control with diabetes)
Lopthyroine (T3)
Cytomel / triiodothyronine
Place in therapy: Short term management of patients with thyroid cancer in preparation of treatments
Moa: hormone replacement therapy
• • • Not ideal in monotherapy
Triiodothyronine (T3) is a very short-acting preparation
• Absorption may be reduced by antacids, calcium salts,
cholestyramine (separate administration by 6 h), and colestipol
Kinetics and Dynamics
• • Symptoms of hyperthyroidism if overtreated!
• Other disease conditions may vary when thyroid is regulated (e.g.
anticoagulation with warfarin, glycemic control with diabetes)Precautions and Adverse Effects
Desiccated thyroid
products desiccated thyroid (thyroid)
PLace in therapy: Rarely used because LEVOTHYROXINE has more reliable dosing
MOA: hormone replacement therapy ,,, is derived from porcine thyroid glands and may not be acceptable for patients who are vegan or those who do not consume pork/pig
kinetics and dynamics: dosage adjustments are made at 4-6 week intervals, Absorption may be reduced by antacids, calcium salts,
cholestyramine (separate administration by 6 h), and colestipol
Precautions and adverse effects: Symptoms of hyperthyroidism if overtreated!
• Other disease conditions may vary when thyroid is regulated (e.g.
anticoagulation with warfarin, glycemic control with diabetes)
Cushing Syndrome
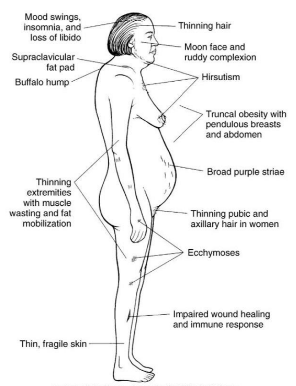
Collection of signs and symptoms due to prolonged
exposure to glucocorticoids (cortisol)
• • Adrenal adenoma
• Pituitary adenoma
• Ectopic carcinoma
• Iatrogenic conditions, such as large doses of glucocorticoids
over time for inflammatory and other conditionsMany causes, including:
Signs and symptoms of cushing syndrome
Change in person’s appearance: • Truncal obesity and weight gain
• Round face (moon face)
• Fat pad between scapulae
(buffalo hump)
• Fragile, thin skin with striae
Retention of sodium and water
Hypertension and edema
• Immune response suppression
• Delayed healing
• Cataracts and glaucoma
• • Emotional lability and euphoria
• Insomnia
Mood disturbances
• • Osteoporosis
Increased catabolism of bone and
protein
• • Hyperglycemia
Increased insulin resistance and
possible glucose intolerance
these are also the adverse effects of systemic corticosteroids
Addision Disease
Deficiency of adrenocorticoid secretions usually caused by an autoimmune reaction
Sign and symptoms: Fatigue, decreased blood glucose levels, inadequate stress response, weight loss, frequent infections, low serum sodium concentration, decreased blood volume, hypotension, high potassium levels
Treatment of Addison Disease
Pharmacotherpay
glucocorticoid replacement (hydrocortisone, alternative = predinisolone)
Mineralocorticoid Replacement (fludrocortisone)
Glucocorticoids
Products
hydrocortisone (Cortef)
prednisone (generics)
Place in therapy
treatment with glucocorticoids and mineralocorticoids is critically necessary for patients with addison disease
MOA
replacement of adrenal cortex hormones
Kinetics and Dynamics
Hydrocortisone is taken po bid to tid
Prednisone is taken po once or twice daily
Precautions and Adverse Effects (as with cushing syndrome)
Change in person’s appearance (truncal obesity and weight gain, round face (moon face), fat pad between scapulae (buffalo hump), fragile/thin skin
• Retention of sodium and water (hypertension and edema)
• Immune response suppression
• Delayed healing
• Cataracts and glaucoma
• Mood disturbances (emotional lability and euphoria, insomnia)
• Increased catabolism of bone and protein (osteoporosis)
• Increased insulin resistance and possible glucose intolerance (hyperglycemia)
Mineralocorticoids
Products
Fludrocortisone (florinef)
Place in therapy
treatment with glucocorticoids and mineralocorticoids is critically necessary for patients with addison disease
MOA
replacement of adrenal cortex hormones
Kinetics and Dynamics
fludrocortisone is taken po once daily
Precautions and Adverse Effects
Oral tabs are stored at 2-8 degrees celsius
KEEP IN THE DRIGE
adverse effects as with glucocorticoids, in addition to fluid and electrolyte disturbances
Diabetes Insipidus
Kidneys are unable to conserve water
Two Types
Central diabetes insipidus
Lack of antidiuretic hormone (ADH) from the pituitary
Nephrogenic Diabetes Insipidus
Failure of the kidneys to respond to ADH
Nephrogenic may be drug induced (Lithium or amphotericin B)
Signs and Symtoms (2)
excessive thirst
excessive urination
Treatment of diabetes insipidus
• • • Oral tablet, orally disintegrating tablet, and nasal spray
desmopressin (DDAVP®, generics)
Products
• • First-line treatment for central diabetes insipidus
Place in Therapy
• • Analogue of ADH; increases water resorption in the renal
tubules
MOA
• • • DISSOLVE TABLET UNDER THE TONGUE
Recommended dose is given tid sublingually
Kinetics and Dynamics
• • Headache, nausea, and abdominal pain
Precautions and Adverse Effects
• DDVAP® is
indicated for
nocturnal
enuresis
(bedwetting)
• MELTS are given 1
hour before
bedtime for up to
3 months