Apex Respiratory
Airway Anatomy
Laryngeal muscles
Intrinsic (innervated by Recurrent Laryngeal muscle)
Control tension and position of the vocal cords and contribute to phonation
CricroThyroid: Cords Tense= elongate innervated by External branch of SLN
ThyroaRytenoid: They Relax= shorten
ADDucts and closes glottis
Posterior CricoArytenoid: Please come apart= aBduct Take away
Solely responsible for opening the vocal cords
Lateral CricoArytenoid: Let’s Close Airway= aDDuct LCAD
ADDucts and closes glottis
Extrinsic
Support the larynx inside the neck and assist with swallowing
all extrinsic end in -hyoid except digastric
Airway innervation
Sensory innervation (4) of the upper airway:
1.Trigeminal CN5: face and head
V1 (ophthalmic) = Nares anterior 1/3 of septum
V2 (maxillary)= Turbinates & nasal septum
V3 ( mandibular)= Anterior 2/3 of tongue (somatic)
2.Glossopharyngeal CN9: oropharynx to anterior side of epiglottis
Posterior 1/3 of tongue
Soft palate
oropharynx
Vallecula
Anterior side of epiglottis
3.Vagus nerve CN10: gives rise to SLN and RLN
Superior laryngeal:
Internal branch= posterior side of the epiglottis-> to level of the vocal cords
External branch= 0 sensory function (motor innervation to cricrothyroid muscle)
Recurrent laryngeal:
Below vocal cords-> trachea (innervates posterior cricoarytenoid muscle, tensing stops when paralyzed)
Risk factors for RLN injury:
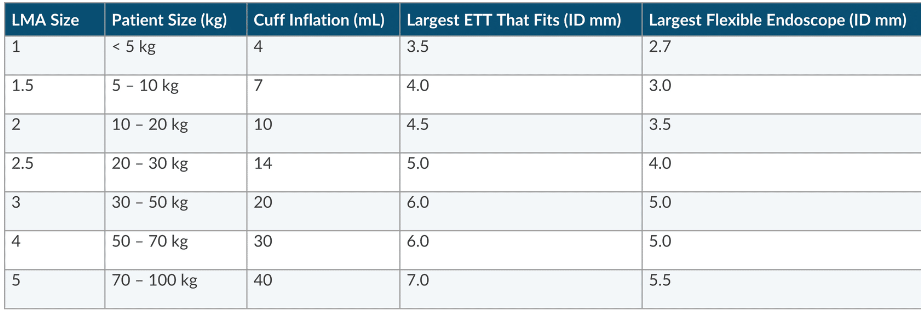
overinflation of ETT or LMA cuff
tumor
excessive neck stretching and surgery (thyroidectomy)
Left side RLN injury
PDA ligation
L atrial enlargement (mitral stenosis, aortic arch aneurysm, thoracic tumor)
Effect of recurrent laryngeal nerve injury:
Bilateral:
Acute: Respiratory distress (unopposed action of cricothyroid muscle) Stridor, dyspnea aphonia PRESENTS similar to laryngospasm
Chronic: No respiratory distress
Unilateral:
Hoarseness
No respiratory distress
Effect of superior laryngeal nerve injury:
Bilateral: Hoarseness/ No respiratory distress
Unilateral: No respiratory distress
Anesthetizing airway Block 3 nerves (Glossopharyngeal, SLN, RLN)
Base of tongue
oropharynx
hypopharynx
larynx
Benzocaine is commonly used; risk for methemoglobinemia and treatment is methylene blue
Cocaine can provide topical; avoid in PChE deficiency on MAOI drugs and SNS tone (CAD)
Land marks for 3 Airway blocks:
Glossopharyngeal nerve block: Palatoglossal arch at the anterior tonsillar pillar; carries 5% risk of seizure (intracarotid injection); needle is too deep if aspirate air, aspirate blood redirect needle medial
Super laryngeal nerve block: Greater cornu of hyoid, needle is too deep if aspirate air
RLN Transtracheal nerve block: Cricothyroid membrane (caudal direction) have patient breathe
Laryngeal Anatomy
Adult Larynx C3-C6-shaped like cylinder and narrowest part is glottic opening
Pediatric is shaped like a funnel < 5yrs
narrowest fixed region= cricoid ring
narrowest dynamic region= vocal cords
Components:
Bone: Hyoid
Ligaments: thyrohyoid, cricothyroid
Unpaired cartilages: epiglottis, thyroid. cricoid
Paired cartilages: corniculate, arytenoid, cuneiform
Needle is placed through cricothyroid membrane during cricothyroidotomy to emergently secure airway and for transtracheal block to anesthetize RLN
Cartilages:
Unpaired: Epiglottis, Thyroid, Cricoid
Paired: Corniculate, Arytenoid (ball joint can be impaired by rheumatoid arthritis and SLE), Cuneiform
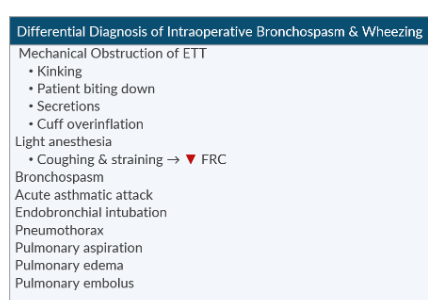
Laryngospasm:
Signs:
Inspiratory stridor
Suprasternal and supraclavicular retraction during inspiration
“Rocking horse” appearance of the chest wall (paradoxical movement)
Increased diaphragmatic excursion
lower rib flaring
Absent or altered EtCO2 waveform
Risk factors:
second had smoke
reactive airway disease
GERD
Causes:
Light anesthesia
airway secretions
surgery in airway
active or recent respiratory tract infection (<2 weeks)
Age < 1 yr
Treatment:
100% Fio2
Remove noxious stimulation
Deepen anesthesia
CPAP 15-20 cm H20
Open the airway (head extension, chin lift)
Succinylcholine:
Submental administration is fasted onset
Neonate/infant= 2mg/kg
Adult or child: 1mg/kg
Dose of 0.1mg/kg preserves ventilation
Infants and small children should receive atropine 0.02mg/kg with succinylcholine
If no IV access, submental administration will produce the fastest onset
If no IV access and patient can receive Succinylcholine, then Rocuronium is the only other NMB that can be given IM
Upper Airway Anatomy
Extends from mouth and nares to cricoid cartilage
Resistance is 2x higher in nasal passage than mouth
Reduce trauma during airway instrumentation in nares: direct device between inferior turbinate and floor of nasal cavity and orient bevel towards the turbinates.
Lower Airway Anatomy
Begins at the trachea and ends at alveoli
Trachea begins at inferior border of cricoid cartilage and ends at carina T4-T5
Lower airway begins as single tube (trachea) and bifurcates along 23 generations
Tube goes where nose goes
L Bronchus is 5cm and takes off 45 degrees from long axis of trachea
R Bronchus is 2.5 cm in length and projects 25 degrees
Children up to 3- B Bronchi take off 55 degrees from long axis of trachea
Type 1 pneumocytes provide surface for gas exchange and Type 2 produce surfactant and Type 1
Respiratory Physiology
Diaphragm and external intercostals contract during tidal breathing (inspiration)
Exhalation is passive
Accessory muscles for inspiration include sternocleidomastoid and scalene muscles
Accessory muscles for active expiration include rectus abdominus, transverse abdominis internal oblique and external oblique.
Vital capacity of 15ml/kg is required for effective cough
3 Zones of airway exchange:
Conducting zone= 0 gas exchange, anatomic dead space, begins in nares and mouth and ends in terminal bronchioles
Transitional zone=air conduit and gas exchange, respiratory bronchioles
Respiratory zone= gas exchange, begins at alveolar ducts and extends to alveolar sacs
Transpulmonary pressure is the difference between alveolar pressure (inside airway) and pleural pressure (outside airway)
TPP= Positive (airway stays open)
TPP= Negative (airway collapses)
Contraction of inspiratory muscles reduces thoracic pressure and increases thoracic volume= ex of Boyles law
Increase PaCo2 to EtCO2 gradient = Increase dead space:
PPV, HypoTN, Atropine
Dead spaces:
Anatomic Vd-Air confined to the conducting airway, Nose/mouth-> terminal bronchioles
Alveolar Vd-Alveoli that are ventilated but not perfused, Reduced pulmonary blood flow (decreased CO)
Physiologic Vd: Anatomic Vd: + Alveolar Vd
Apparatus Vd: Vd added by equipment Facemask. HME. Limb of circle system if incompetent valve present
Spontaneously ventilating patient Vd/Vt=0.33 (2mL/kg or 150mL in 70 kg patient)
Mechanically ventilated patient Vd/Vt=0.50
Factors that increase ratio of Vd to Vt= Facemask, atropine, neck extension
Factors that decrease ratio = ETT LMA and neck flexion
Physiological dead spec can be calculated with Bohr equation. Compares partial pressure of CO2 in the blood vs partial pressure of CO2 in exhaled gas
Most common cause of increased Vd/Vt under GA is HypoTN. Acute EtCO2 decrease first rule out HypoTN
Increases in Vd:
Facemask
HME
PPV
Anticholinergics
Old age
Extension
Decreased CO
COPD
PE (thrombus, air, amniotic fluid)
Sitting position
Decreases in Vd:
Endotracheal tube
LMA
Tracheostomy
In a circle system dead space begins at the y-piece. Anything proximal to the y-pieces does not influence dad space nor does increasing length of circuit. Except when there is incompetent valve in circle system.
Alveolar compliance curve:
Alveolar ventilation is a function of alveolar size and its position on the alveolar compliance curve.
The best ventilated alveoli are the most compliant (which is the steep slope of the curve)
The poorest ventilated alveoli are the least compliant (flat portion of the curve).
Ventilation is greatest at the lung base due to higher alveolar compliance.
Perfusion is greatest at the lung base due to gravity
Ventilation/Perfusion Mismatch
V/Q ratio
The V/Q ratio is the ratio of ventilation to perfusion (Ve/CO):
Normal Ve= 4L
Normal CO= 5L
Normal V/Q ratio= 0.8
Dead space and shunt are absolutes:
Dead space: V/Q=infinity (10/0=infinity)
Shunt: V/Q=0 (0/10=0)
V/Q mismatch occurs when the ratio is disturbed
If the number is larger than 0.8, then this moves towards dead space
If the number is smaller than 0.8 than this moves towards shunt
Atelectasis is most common cause of hypoxemia in the PACU. Leads to R-L shunt, V/Q mismatch, and hypoxemia
Patients with V/Q mismatch have more trouble with oxygenation than CO2 elimination. CO2 retention suggest severe V/Q mismatch
To combat dead space in Zone 1= bronchioles constrict to minimize ventilation of poorly perfusion alveoli
To combat shunt Zone 3- hypoxic pulmonary vasoconstriction reduces pulmonary blood flow to poorly ventilated alveoli
Law of Laplace- As the radius of a sphere or cylinder becomes larger, the wall tension increases as well. (Tension Pressure Radius)
Surfactant keeps alveolar pressure constant and prevents small alveoli from collapsing and emptying in to larger alveoli
Type 2 pneumocytes produce surfactant 22-26 wks with peak production 35-36 wks. Fetal lung maturity can be hastened by corticosteroids (betamethasone)
Zone 1:
PA> Pa>Pv
Dead space
Ventilation without perfusion
Zone 2:
Pa>PA> Pv
Waterfall
Normal physiology
Zone 3:
Pa> Pv>PA
Shunt
Perfusion without ventilation
Zone 4:
Pa>Pist>Pv>PA
Pressure in the interstitial space impairs ventilation and perfusion
Alveolar gas equation:
Hypoventilation can cause hypercarbia and hypoxemia. Supplemental oxygen reverses hypoxemia but does not reverse hypercarbia. Hypercarbia can go undetected.
Alveolar Oxygen= FiO2 x (Pb-PH2O)- (PaCO2/RQ)
Pb= Barometric/Atmospheric pressure (760 normal)
PH2O= 47mmHg
RQ= Respiratory quotient=0.8
RQ= (CO2 elimination/O2 consumption)= (200mL/250mL)
Hypoxemia & A-a Gradient
A-a gradient is the difference between alveolar oxygen (PAO2) and arterial oxygen (PaO2)
Calculating the A-a gradient diagnose the cause of hypoxemia by indicating the amount of venous admixture. Utilizes alveolar gas equation and obtain an ABG (PaO2).
Hypoxemia with normal A-a gradient <15mmHg:
low Fio2
hypoventilation
Hypoxemia with increased A-a gradient:
diffusion limitation
V/Q mismatch
shunt (NOT improved with supplemental oxygen)
Factors that increase A-a gradient:
Aging (closing capacity increases relative to FRC)
Vasodilators (decreased hypoxic pulmonary vasoconstriction)
R-L Shunt (atelectasis, pneumonia, bronchial intubation, intracardiac defect)
Diffusion limitation (alveolocapillary thickening hinders O2 diffusion)
Shunt increases 1% for every 20mmHg of Aa gradient
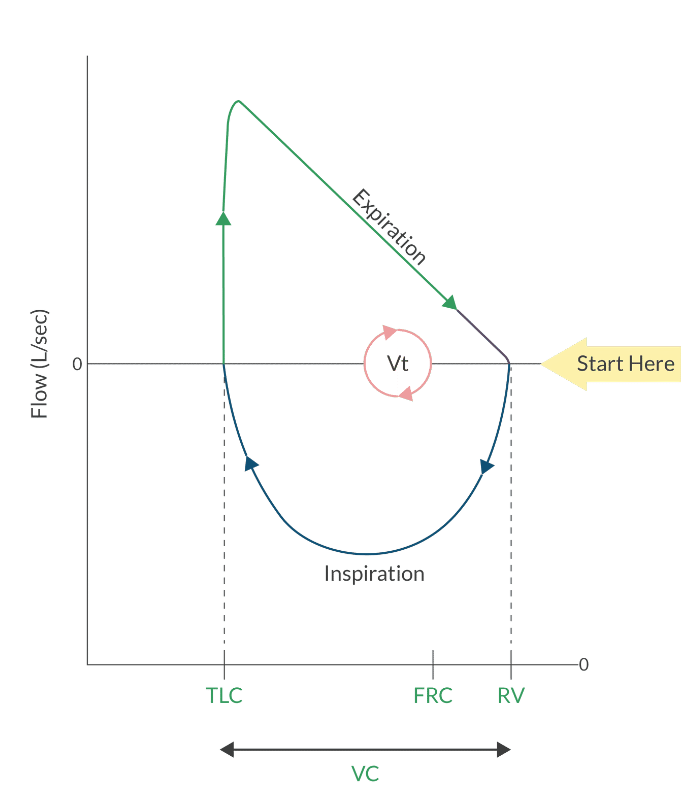
Lung Volumes & Capacities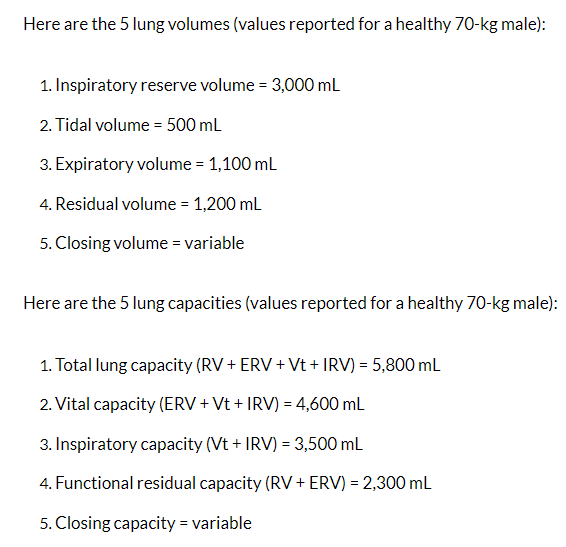 Spirometry cannot measure residual volume therefore it cannot measure total lung capacity, functional residual capacity or closing volume.
Spirometry cannot measure residual volume therefore it cannot measure total lung capacity, functional residual capacity or closing volume.
Oxygen Content
VO2=3.5mL/kg
VO2 ~ 250mL/min 
Oxyhemoglobin Dissociation Curve
Oxyhemoglobin dissociation curve tells the tendency of hemoglobin to bind oxygen
Right shift curve =hemoglobin has a lower affinity for oxygen (right=release) During normal physiology this occurs at the tissue level.
Left shift curve= hemoglobin has higher affinity for oxygen (left=love) During normal physiology this occurs int he lungs
P50 is the PaO2 where hemoglobin is 50% saturated with oxygen
Decreased P50= Left shift
Hgb has a stronger hold on oxygen
Examples: Hgb F, hypocarbia, methemoglobin and carboxyhemoglobin, alkalosis, decreased temperature, decreased 2,3 DPG
Increased P50= Right shift
Hgb is more willing to release oxygen
Examples: acidosis, hyperthermia, and increased 2, 3 DPG and temperature
A PaO2>100mmHg will increase O2 dissolved in blood but will not cause more to bind to hemoglobin.
The Bohr effect says that an increased partial pressure of CO2 and a decreased pH cause hemoglobin to release O2
2,3 DPG is produced during RBC glycolysis.
Maintains the curve in a slightly R shifted position
Hypoxia increases 2,3 DPG production= facilitates O2 offloading
Important compensation mechanism for chronic anemia
Banked blood the concentration of 2,3 DPG falls which causes curve to left shift and reduce O2 available to tissue.
HgbF doesn’t respond to 2,3 DPG= L shift P50-19mmHg
CO2 Transport
CO2 is primary by product of aerobic metabolism
CO2 is transported in 3 ways:
As bicarbonate 70%
Bound to Hgb 23%
Dissolved in plasma 7%
Carbonic acid is enzyme that facilitates formation of carbonic H2CO3 from H2O and CO2
To maintain electroneutrality, for every HCO3 that leaves the erythrocyte one Cl ion is transported in. This is known as the chloride or Hamburger shift.
An acidic environment of metabolically active tissue enhances O2 offloading from hemoglobin (Bohr effect) and increases CO2 loading in tot the blood (Haldane effect)
CO2 is 20x more soluble in blood than O2
Solubility is function of Henry’s Law
The Haldane effects describes CO2 carriage (oxygen causes erythrocyte to release CO2). Opposite of Bohr effect. Deoxygenated blood can carry more CO2
CO2 Dissociation curve
Oxygenated Hemoglobin shifts CO2 dissociation curve to the Right
Deoxygenated Hemoglobin shifts CO2 dissociation curve to the Left
Hypercapnia
Causes: sepsis, MH, Thyroid, storm, burns and shivering
Decreased CO2 elimination: airway obstruction, ARDS, COPD, opioid overdose
Causes of Rebreathing: exhausted soda lime, a faulty unidirectional valve in circle system and inadequate FGF in a Mapleson circuit.
Consequences of hypercarbia: hypoxemia, acidosis, cardiac depression, SNS stimulation and increased ICP.
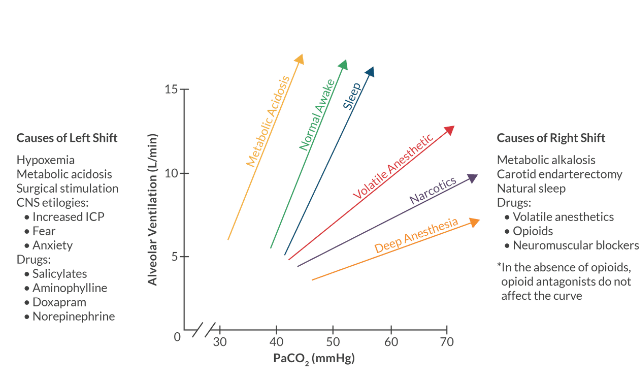
CO2 Ventilatory Response Curve
Describes the relationship between PaCO2 and min ventilation
The central chemoreceptor in the medulla is the primary monitor of PaCO2
The peripheral chemoreceptor in the carotid bodied and transverse aortic arch play a secondary role in monitoring PaCO2
Conditions that shift CO2 curve down and to the right:
Volatile anesthetics
Opioids
NMBs
Metabolic alkalosis
Carotid enterectomy
Right shift= apneic threshold has increased
Conditions that shift CO2 curve to the left:
hypoxemia
metabolic acidosis
surgical stimulation
intracranial hypertension
Drugs: Salicylates, Aminophylline, Doxapram, norepinephrine
Left shift= apneic threshold has decreased
 Neural Control of Ventilation
Neural Control of Ventilation
Reticular activating system in Medulla and Pons regulates speed and depth of breath (regulating PO2 and CO2)
Receives afferent input from the central and peripheral chemoreceptors as well as the stretch receptors in the lungs
Integrates signals with intrinsic resp pattern an sends response to diaphragm intercostals and accessory muscles.
Cerebral cortex modify these responses
Medullary respiratory center:
Dorsal: Active during inspiration
Ventral: Active during expiration
Pontine respiratory center:
Pneumotaxic center upper pons: Inhibits the DRG
Apneustic center lower pons: Stimulates the DRG
Resp rate and Pattern determined by:
Medulla:
Neural control in resp center
Chemical control in central chemoreceptors
Carotid Bodies and aortic arch:
Chemical control in peripheral chemoreceptors
Lungs:
Baroreceptors
Central chemoreceptors
Responds indirectly to PaCO2
BBB separates blood from CSF
CO2 free diffuse across BBB (H and HCO3 do NOT)
CO2 dissolves into H and HCO3 after reaching CSF
As rate of H rises in CSF, rate and depth of Resp increase until minute ventilation stabilizes (occurs in mins and control blood gas tension)
Non-Volatile acids (lactic acid)do not pass BBB
Central chemoreceptor is stimulated by hypercarbia and hypoxemia but is depressed by profound hypercarbia and hypoxemia.
Peripheral chemoreceptors
Reside in carotid bodies at bifurcation of common carotid artery and present in transverse aortic arch
Monitor hypoxemia PaO2 < 60mmHg
Carotid Enterectomy severs the afferent limb of the hypoxic ventilatory response. Don’t do B CEA
Sub anesthetic doses of inhalation and intravenous anesthetics (0.1 MAC) depress hypoxic ventilatory drive cause risk of hypoxemia in PACU.
Anemia and Carbon Monoxide poisoning affect tissue oxygenation but do not impair hypoxic ventilatory response.
The Hering-Breuer inflation reflex prevent alveolar over distention by stopping inhalation when lung volume is too large.
Hering-Breuer deflation reflex activates resp drive when lung vol is too small to prevent atelectasis.
J receptors or pulm C fiber receptors increase the resp rate in setting of pulmonary embolism or CHF. Causes tachypnea
Paradoxical reflex of head cause a newborn to take first breath
Hypoxic Pulmonary vasoconstriction
HPV is local reaction that occurs in response to a reduction in alveolar oxygen tension not arterial PO2
Goal is to improve matching of ventilation and perfusion to minimize shunt during atelectasis or one lung ventilation
The pulmonary vascular bed is the only region in the body that responds to hypoxia with vasoconstriction
Inhibited by volatile anesthetics >1.5 MAC, PDE, Dobutamine, hypervolemia, excessive PEEP and large tidal volumes
NOT inhibited by IV anesthetics: ketamine, propofol, and opioids
Excessive PEEP or high tidal volumes increase dead space and reduce V/Q matching
Respiratory acidosis activates H/K pump buffer CO2 acids in exchange cause K to be released in Plasma
Respiratory PathoPhysiology
Control of Airway diameter
Radius of the airway has most significant contribution to airflow resistant (radius 4)
PNS Vagus nerve= bronchoconstriction
Mast cells and non cholinergic PNS= bronchoconstriction
Non cholinergic PNS (nitric oxide)=bronchodilation
SNS (circulating catecholamines)= bronchodilation
Vagus nerve CN 10 supplies parasympathetic innervation to airway smooth muscle
Stimulation of the (Ache to) M3 receptor produces bronchoconstriction from Ca release
Beta 2 receptors= airway smooth muscle
Pulmonary Function testing
Normal FEV1 value is > 80% of predicted value
Normal FVC 4.8 Males & 3.7 Females
Normal FEV1/FVC ratio is > 75-80% of predicted value- useful in diagnosing obstructive (70%) vs restrictive
Lung vols and capacities are measured with spirometry
Forced expiratory flow at 25-75% vital capacity (mid maximal expiratory flow rate) is the most sensitive indicator of small airway disease reduced with obstructive
Postoperative Pulm Complications
Independent risk factors for PPC:
Old age, COPD, CHF and smoking
Surgery >2hrs, GA, abdominal or aortic thoracic
albumin <3.5g/dL
NON increased risk factors:
Asthma
ABG
PFT
Short term benefits of smoking cessation include reduction in carboxyhemoglobin improved P50 with in 12 hrs, Carbon monoxide- 4-6hrs , short term doesn’t reduce pulmonary complications
Intermediate effects of stopping smoking:
Return of pulm function test 6 wks:
airway function
mucociliary clearance
Sputum production
pulm immune function
hepatic enzyme induction also subside after 6 weeks
Risk reduction strategies:
Quit smoking > 6 wks
Employ alveolar recruitment + PEEP
Treat expiratory flow obstruction with bronchodilator and corticosteroids
Treat active infections (prophylaxis for pulm infection is not indicated)
Consider other anesthetic options beside GA
Teach pulm recruitment maneuver to patient
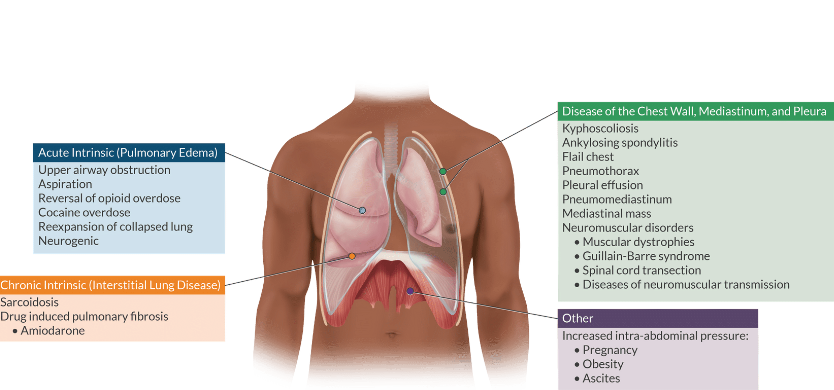
Obstructive vs restrictive
Obstructive have normal or decreased FEV1 and FVC and FEV1/FVC ratio is always decreased
Restrictive disease have decreased FEV1/and FVC but FEV1/FVC ratio is normal
Alpha-1 antitrypsin deficiency is most common metabolic disease in affecting the liver and causes a relative increase in alveolar protease activity. Degrades pulm connective tissue and leads to panlobular emphysema. Only treatment is live transplantation
Anesthetic management of COPD
Consider regional for procedures involving extremities and lower abdomen
No to neuraxial if patient requires blockade > T6
Interscalene causes paralysis of the ipsilateral hemidiaphragm
Caution with excessive sedation and ventilatory response
Select Volatile with low blood: gas solubility
All halogenated anesthetics are bronchodilators Sevo and Iso are better than Des
Volatile impair HPV > 1.5 MAC and increase shunt. Unless shunt is sever it can be overcome by increasing FiO2
NO is associated with rupture of pulm blebs→ pneumothorax
Use tidal volume 6-8mL/kg IBW
Use longer expiratory time
Add PEEP stay alert for dynamic hyperinflation
Anesthetic management of Restrictive lung disease
Minimize risk of barotrauma
smaller tidal volume 6ml/kg/IBW rr 14-16
Peak insp pressure <30cm H20
Prolong inspiratory time 1:1
Aspiration Pneumonitis and Ventilator-Associated Pneumonia
Lead to airway obstruction bronchospasm impaired gas exchange and bacterial respiratory infection
Risk factors:
pregnancy
trauma
emergency surgery
GI obstruction
peptic ulcer dx
hiatal hernia
ascites
cricoid pressure
seizures
Mendelson’s syndrome:
chemical aspiration first described in OB patients with roisl factors:
Gastric pH< 205
Gastric volume > 25mL (0.4mL/kg)
Phar Prophylaxis:
antacids
H2 antagonist
GI stimulants
proton pump inhibitors
antiemetics
s/s
hypoxemia ** hallmark
dyspnea
tachypnea
cyanosis
Treatment
tilting head downward or to the side
suctioning airway
securing airway
applying PEEP to reduce shunt
bronchodilators reduce wheeze
IV lidocaine to reduce neutrophil response
Patient who aspirate must be observed in PACU at least for 2hrs with out:
New cough or wheeze
Radiograph evidence of pulmonary injury
SpO2 decrease > 10% of preoperative values on room air
A-a gradient > 300mmHg
Pneumothorax and Flail Chest
Closed, communicating and tension
Tension:
hyposemia
increaased airway rpessure
tachcardia
hyPoTN
elevated CVP
ultrasound lack of sliding lung and absence of comet tails
mediastinal shift
DC NO immediately
Emergency treatment insertion of 14g angiocath into 2nd intercostal space at midclavicular line or the 4th or 5th intercostal space at the anterior axillary line
Flail chest = blunt trauma with multiple rib fractures= paradoxical movement of chest wall a the site of the fractures
alveolar collapse
hypoventilation
hypercarbia
and hypoxia
Tx= reduce pain= epidural or intercostal nerve block or mechanical ventilation and surgical fixation
Venous Air Embolism
Risk due to position: sitting>supine>prone> lateral
TEE most sensitive diagnostic tool
s/s:
observed on TEE
millwheel murmur on precordial
decreased EtCO2
increased EtN2
hypotension
dysrhythmias
hypoxemia cyanosis
cardiovascular collapse
tx:
100% O2
flooding surgical field
dc insufflation
Durant method- Left lateral decubitus position
support with vasopressors, inotropes and IV fluids
Air trapped in the pulmonary circulation decreases left ventricular preload/cardiac output and leads to asystole and cardiovascular collapse
Pulmonary HTN
Defined as PaP> 25mmHg
avoid increases in PVR:
hypoxemia
hypercarbia
acidosis
hypothermia
pain
SNS stim
hypothermia
PEEP
atelectasis
Nitrous oxide
ketamine
Desflurane
mechanical ventilation
Decreases PVR
increased PaO2
hypocarbia
Alkalosis hyperventilation
spontaneous ventilation
prevent coughing straining
Inhaled nitric oxide
Nitroglycerin
PDE inhibitors
Prostaglandins PGE1 & PGI2
CCB
ACE inhibitors
Anesthetic considerations:
Do not hold prop op meds that reduce PVR
CO is fixed pts are sensitive to inadequate preload
Treat hypotension aggressively
Epidural anesthesia is better tolerated than spinal anesthesia
Inhaled nitric oxide
High frequency jet ventilation
Elevated RA pressure can open Foramen Ovale causing R-L shunt
Epidural is better than spinal for Pulm HTN
Too much preload can be bad. Uterine contraction push sig amt of blood toward heart and worsen PAH and RV function =Use Nitroglycerin*
Equation PVR= PaP-PAOP * 80/ CO
Carboxyhemoglobin
binds on hemoglobin 200x than Oxygen
shifts oxyhemoglobin curve to Left starving tissues of oxygen causes metabolic acidosis
at risk patients: burn victims, smoker, pts exposed to desiccated soda lime
pulse ox cannot measure and give falsely elevated result, need coximeter to diagnose
Oxygen administration 100% (until CoHgb <5%) and Hyperbaric oxygen therapy is treatment (if CoHgb >25% of total hgb)
Desiccated soda lime risk is greatest with DES>ISO>SEVO
Soda lime hydrated 13-15%
Desiccated soda lime with Sevo forms compound A and increases risk of fire
Indications for Mechanical Ventilation
Strong:
Vital capacity <15mL/kg
Inspiratory force < 25cm/H2O
Pa O2<200mmHg on 100% Fio2
A-s gradient> 450mmHg on 100% fiO2
PaCO2> 60mmHg
Respiratory rate > 40 or <6 bpm
Drug ETT administered NAVEL= narcan, atropine, vasopressin, epinephrine, lidocaine
One lung Ventilation
Best predictors for pul complications having pulm surgery
FEV1< 40% predicted
DLCO < 40% predicted
VO2max< 15mL/kg/min
Absolute indications for one-lung ventilation:
Infection
massive hemorrhage
bronchopleural fistula
Relative indications for one-lung ventilation:
Improved surgical exposure
pulm edema
severe hypoxemia due to lung disease
Left sided tuba is preferred.
Right sided tube used when Left main bronchus has distorted anatomy (tumor TAA) and surgical procedures : left pneumonectomy, left transplant or left sleeve resection
NO DLT for 8< use bronchial blocker or single lumen tube in to the main bronchus
Age 8-9 size 26
Age 10 +28 or 32
Female-35-37
Male- 39-41
Initiating OLV:
Fio2 100%
Tidal vol 6-8ml/kg/IBW
RR 12-15
Alveolar recruitment before OLV
PEEP 5-10 cm H2O
Adjust I:E if exp flow limitation
Consider TIVA vs Volatile
Addressing Hypoxemia in OLV
Verify 100% oxygen
Check position of tube/bronchial blocker via fiberoptic
Rule out causes: reduced CO, bronchospasm, mucus plug, pneumothorax of dependent lung
Apply CPAP to non-dependent lung or use suction catheter to insufflate oxygen
Apply PEEP 5-10 to dependent lung
Alt options:
Intermittently reinflate the non-depended lung
Ligate the pulm art
Eliminate drugs the inhibit HPV (Volatiles )
Placement complications:
DLT too far in of correct side= upper lobe not ventilated
DLT not deep enough in trachea= no lung separation
DLT is in wrong bronchus=wrong lung collapses
Bronchial blocker
Slow to collapse lung
Can contaminate or block ventilation if it slips
Can be used in children <8 yrs
can insufflate oxygen into non ventilated lung
Can be used to suction air from the non ventilated lung
Cannot suction blood, pus, or secretions from non ventilated lung
Can use with nasotracheal intubation
can use with tracheostomy
can use with existing ETT
Mediastinoscopy & trachea resection
Diagnose lung cancer
Most serious complications: 1. hemorrhage & 2. pneumothorax
Absolute contraindication = previous mediastinoscopy
Relative= Tracheal deviation, Thoracic aortic aneurysm, Superior vena cava obstruction
Compression of the innominate artery can impair cerebral perfusion R side of circle of Willis
The innominate artery is also known as the brachiocephalic artery or brachiocephalic trunk (BCT). It's the first branch of the aortic arch and supplies blood to the head, neck, and upper extremitiesPlace pulse ox or art line on right upper extremity. If the scope compresses the innominate the waveform will dampen or disappear.
Place NIBP on LUE to measure BP
Large bore IV access PRBC available
Associate with Oat cell carcinoma and Eaton Lambert syndrome
sensitive to succinylcholine and non depolarizers
Indications for tracheal resection include tracheal stenosis, tracheomalacia, tumor and vascular lesions and congenital malformations
Reduce tension on the tracheal anastomosis, maintain flexed position for several days after surgery. Use flexible fiber optic if reintubation is needed.
Preop trachea resection:
asses for airflow limitations
Eval CT scan and flow-vol loop
If at risk for airway obstruction, preserve spon ventilation (sevo)
ETT, jet ventilation, ECMO
ARDS
Non cardiogenic pulm edema
Pneumonia most common etiology and sepsis most common extra pulm etiology
Caused by inflammation injury mediated by neutrophils and platelets leading to diffuse alveolar destruction
Pathology:
protein rich pulm edema
loss of surfactant
hyaline membrane formation
possible long term lung injury
CXR reveal B opacities not explained by effusions, lobar/lung collapse or nodules. Diffuse patchy alveolar infiltrates appear peripherally about 12 hrs after initial insult which can lead to alveolar consolidation.
Prone position may improve V/Q matching used in patients with severe ARDS
Strategy for mechanical ventilation:
Pressure control
low tidal vol 4-6ml
PEEP titrate with fio2 below 50% if possible
Plateau pressure <30cmH2O
RR 6-35 per min ok for permissive hypercapnia
I:E ratio 1:1-1:3
Target Oxygen goals=PaO2 55-80 or SpO2 88-95%
Conditions associated with difficult airway
Ludwig’s angina-bacterial infection characterized by rapid progressing cellulitis in the floor of mouth. Most significant concern is posterior displacement of the tongue resulting in complete supraglottic airway obstruction.
Best method of securing airway=awake nasal intubation or awake tracheostomy