Lecture 4: E-Cigarettes
these papers discusses the safety issues, we cannot just compare them to doing nothing, more useful to compare them to something else, which is commonly smoking tobacco
do they aid in quitting smoking: they are useful for those smoking tobacco but still ambiguity, and we need to think of the different groups using them, if it was just those that used to smoke tobacco then there wouldn’t be such an uproar, it is now used by young people that do not smoke
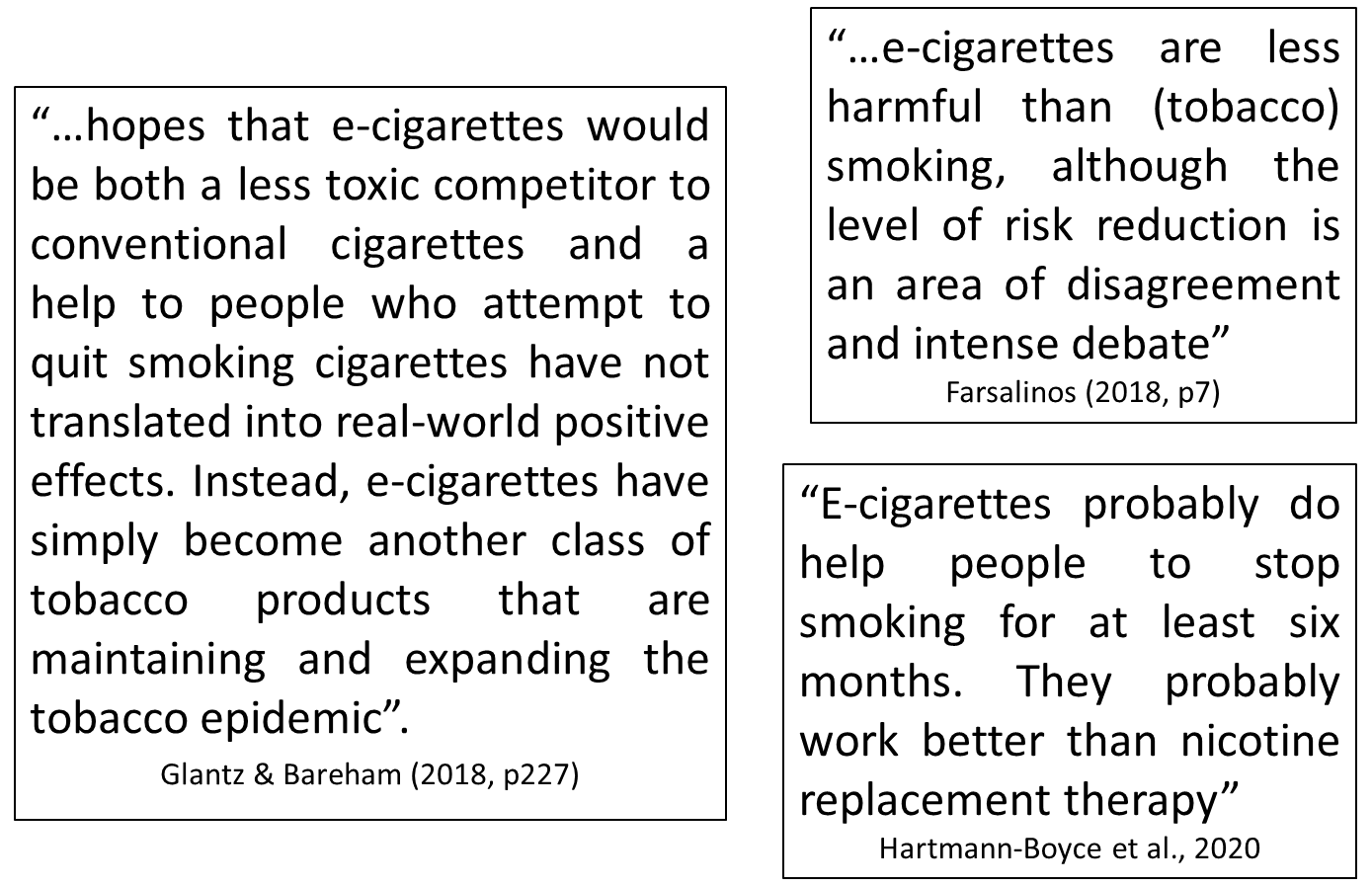
polarising views of e-cigarettes
this is a paper from the US and quite old
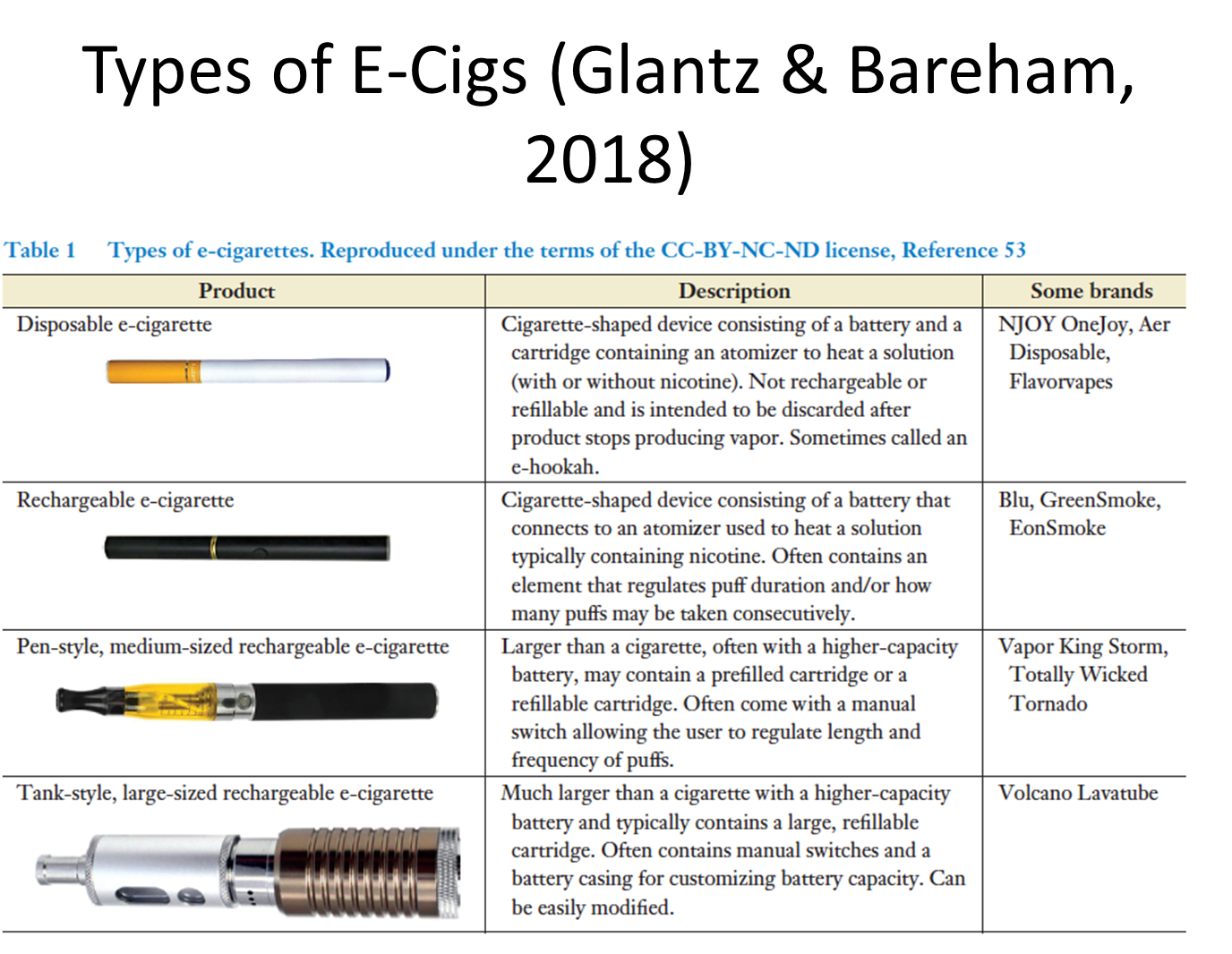
there are lots of different types, they were introduced about 20 years ago, 2004, were developed in China as a less dangerous alternative
early devises looked like a conventional cigarette, including a small tip that lit up when the user puffed
they were generally inefficient at delivering nicotine
somewhat due to the particle size of the aerosol (too big to penetrate the lungs)
newer versions had replaceable/ refillable reservoirs and rechargeable batteries that generate smaller particles and more efficient nicotine delivery
refillable systems allow users to separately purchase the e-cig liquid that contains varying levels of nicotine
nowadays the market has settled down and there are relatively less types of vapes available
there used to be many different types, rechargeable ones: pen style with a prefilled cartilage, and then a tank one that looks like a shot gun, disposable ones
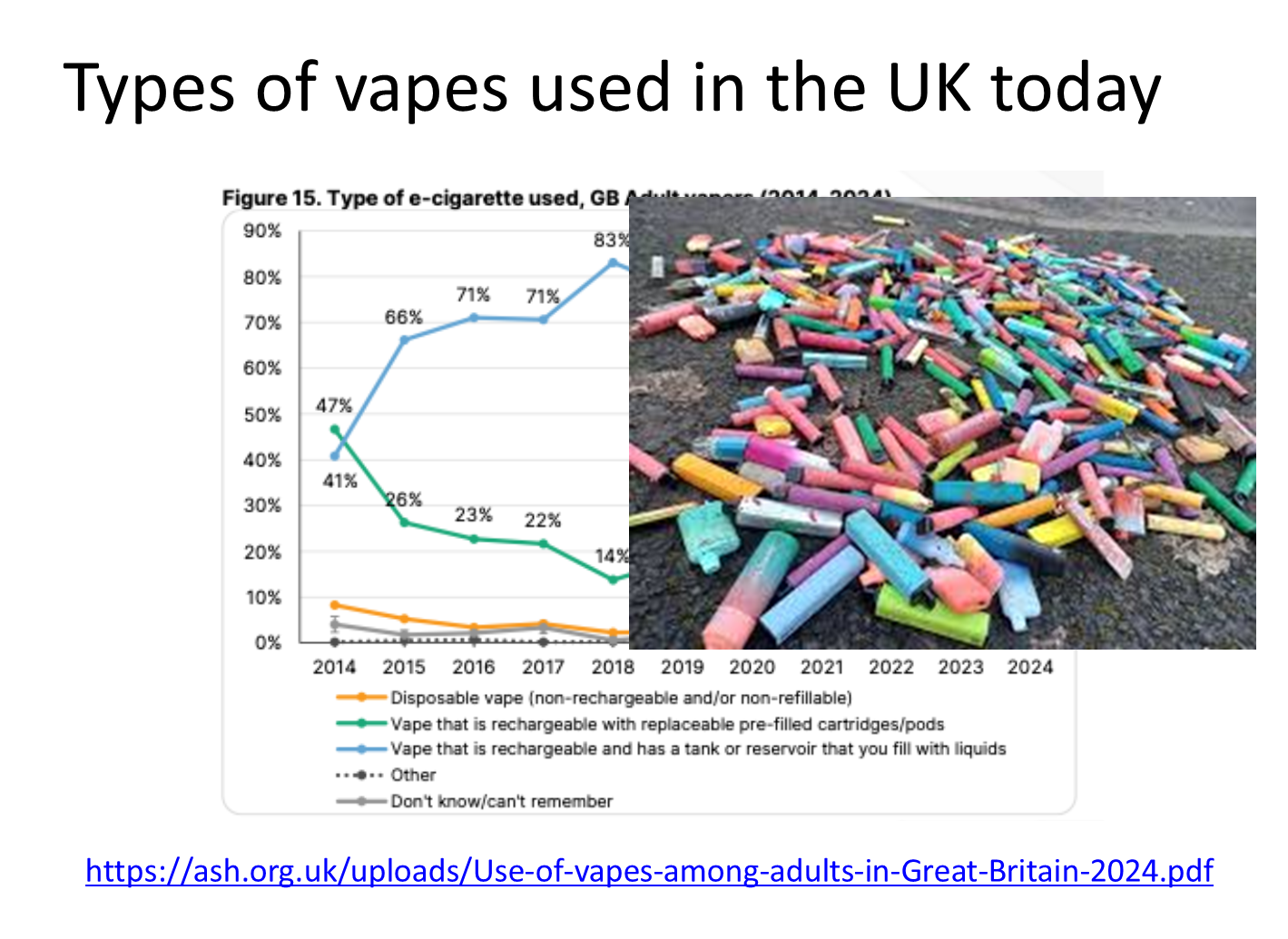
among adults, rechargeable vapes with a tank are the most popular
approx ten years ago, rechargeable vapes with replaceable pods were most popular but this drops drastically in popularity (47% to 15% by 2024)
disposable vapes became drastically more popular (lower than 10% in 2014 to 30% in 2024)
there was concern because of their relatively cheap cost and the bright packaging makes it particularly appealing to young children, this is why they were banned last year
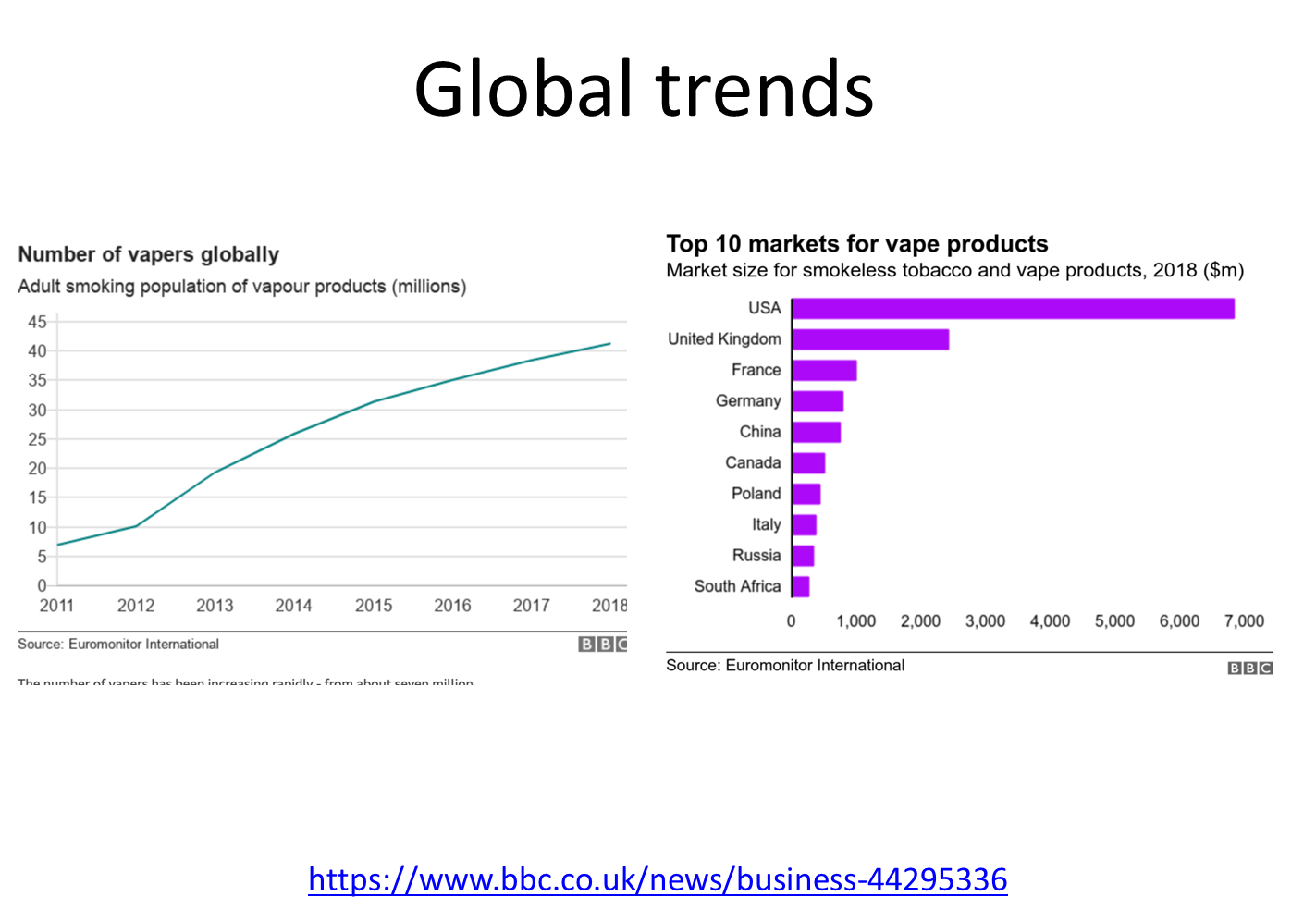
about 7 million adults smoked vapes in 2011,
mostly consumed in the USA and UK
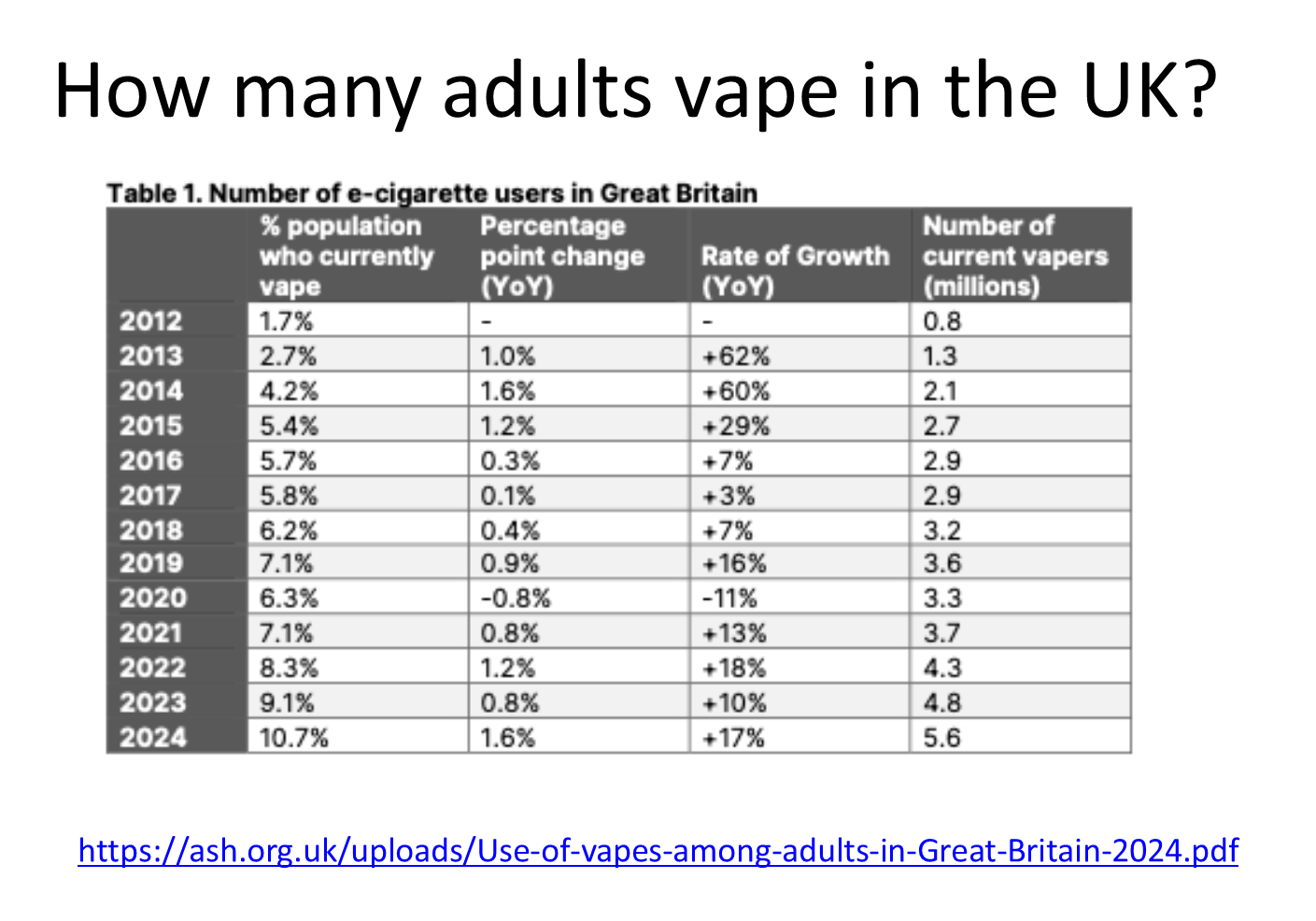
% of adult pop who vape in 2012 was about 1.2% not it is about 1 in 10
we now have 5.6 million vapers
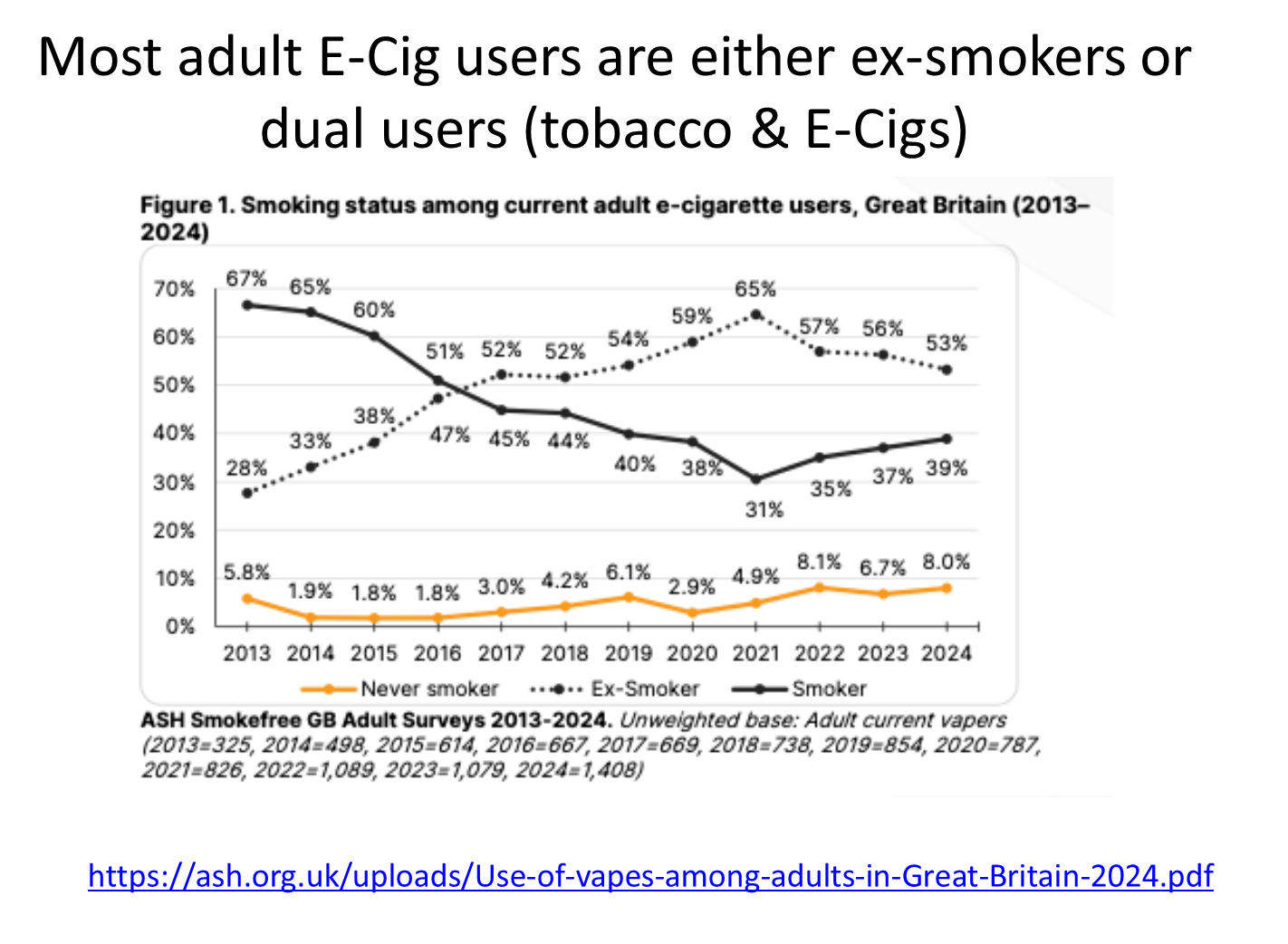
everyone on this graph is a regular vaper
looking at the bottom line, less than 10% of vapers have never smoked but continue to vape
the solid black line is dual users, so they smoke tobacco and vape
the solid black and dotted black line move in parallel, aka when people started to quit smoking tobacco they have moved to be an ex tobacco smoker but vape instead
people initially were dual smokers, they’ve now stopped smoking tobacco but continued with e-cigarettes
thus vaping and smoking tobacco are quite closely linked
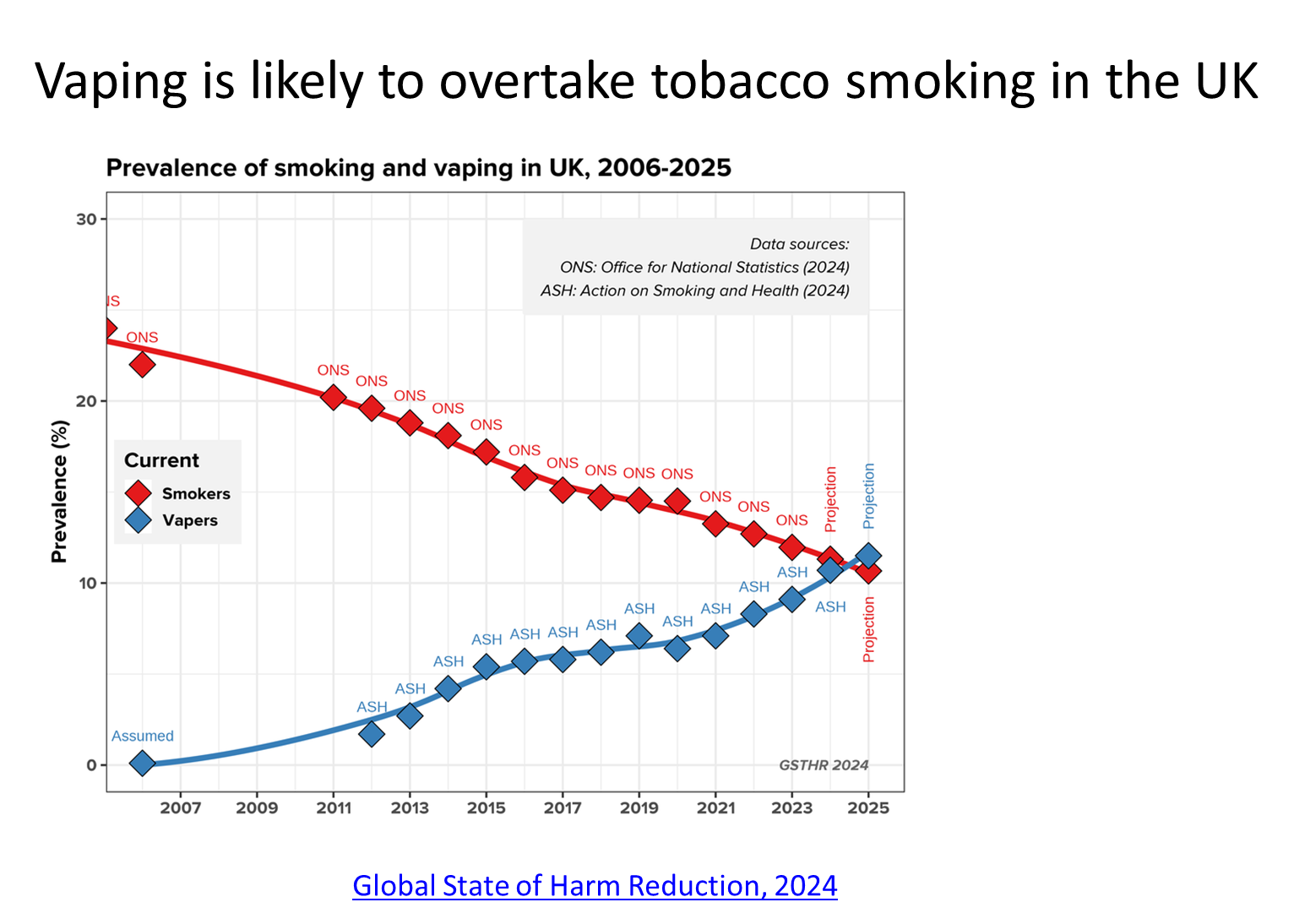
prevalence of tobacco smoking and vape smoking in the UK
overtime the number of adults that smoke have gone down, almost parallel to the number of adults that picked up vaping
very recent trend shows that the total number of vapers had outnumber the amount that smoke
last year was the first year that the number of adults that vape overtook the amount of smokers in the UK
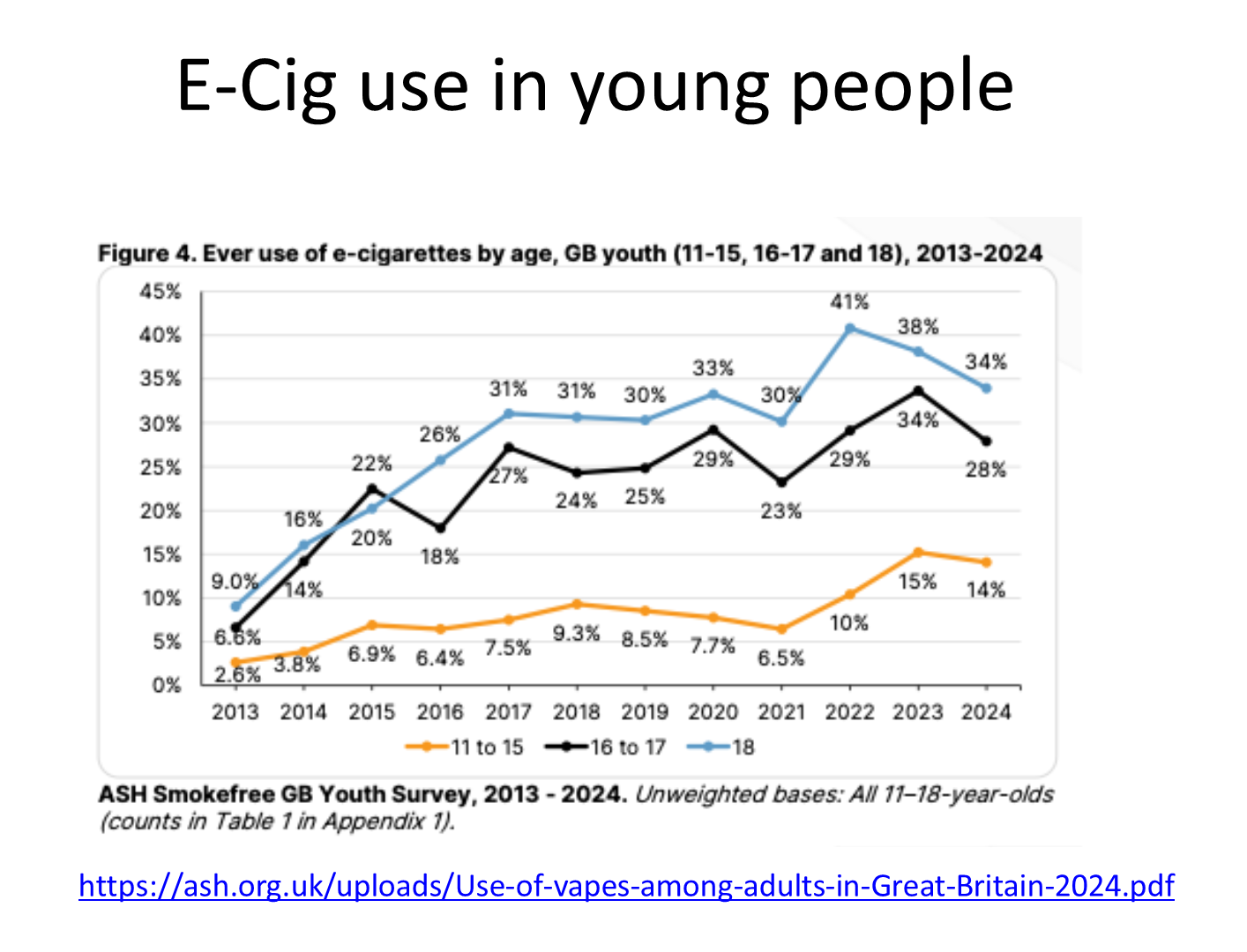
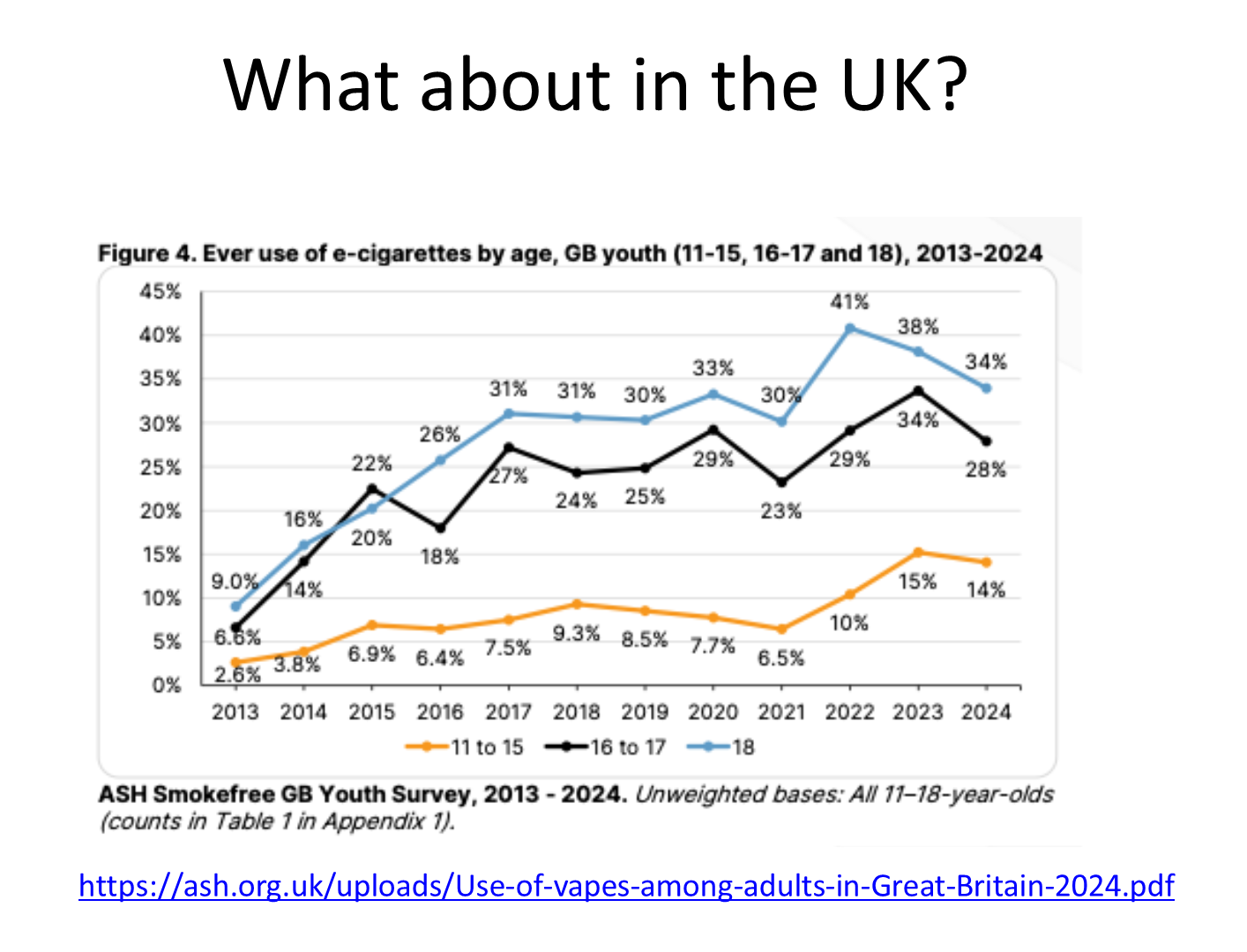
relatively low in 11-15 year olds, but has made a drastic and increasing leap in recent years
getting close to 40% of 18 year olds that have at least tried a vape
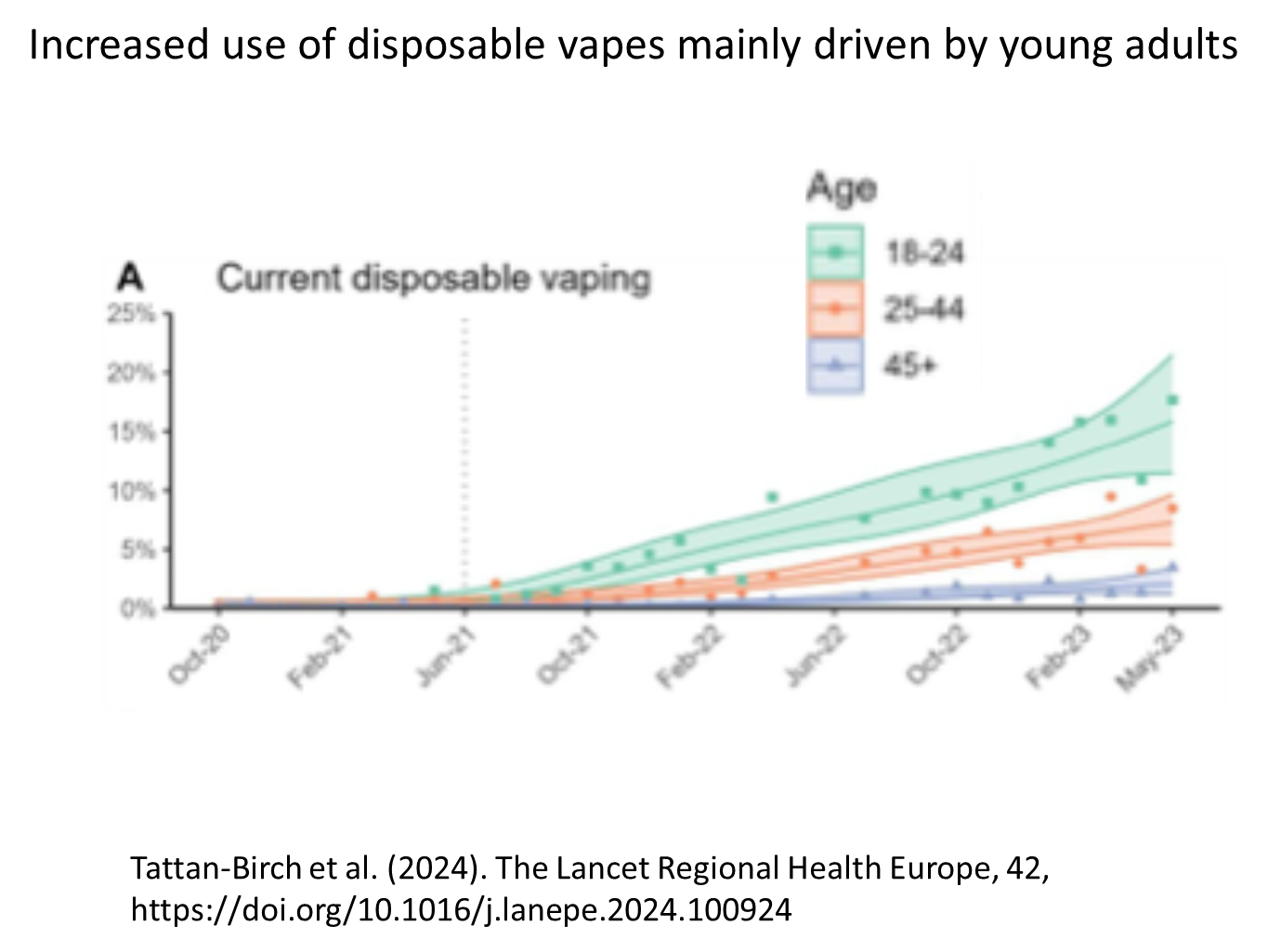
shows its not really older adults that increased use of disposable vapes, but overwhelmingly popular within the younger population
this is why they were banned
there’s multiple ways to ask this, are they objectively safe, but you could do this with any action, no action is going to be actively safer than the comparison of nothing, we need a comparison

one Dr results show that e-cigarettes/ vapers are safer than cigarettes, around 95% less harmful than cigarettes (NOT TRUE)
Influential health organizations in England, including Public Health England, the Royal College of Physicians, the Royal Society for Public Health, and the National Health Service, have stated that e-cigs are 95% safer than conventional cigarettes
This claim originated from a single consensus meeting of 12 people convened by D.J. Nutt in 2014
They reached this conclusion without citing any specific evidence
The Nutt et al. meeting was funded by EuroSwiss Health and Lega Italiana Anti Fumo (LIAF).
EuroSwiss Health is one of several companies registered at the same address with the same chief executive, who was reported to have received funding from British American Tobacco (BAT) for writing a book on nicotine as a means of harm reduction (66) and who also endorsed BAT’s public health credentials
Another of Nutt’s coauthors, Riccardo Polosa, was Chief Scientific Advisor to LIAF, received funding from LIAF, and reported serving as a consultant to an e-cig distributor.
He also received funding from Philip Morris International.
Later in 2015, the BMJ published an investigative report that raised issues surrounding conflicts of interest between individuals involved in the Nutt et al. paper.
as of June 2017, the “95% safer” figure remains widely quoted, despite the fact that evidence of the dangers of e-cigarette use has rapidly accumulated since 2014.
it is the tar in the cigarettes that cause the harmful toxins to enter our bodies, this is not an issue in vapes
they used cotton balls to show the tar build up in the inhale of smoking tobacco Vs e-cigarette, but our lungs are not made up of cotton balls lol
the quote of ‘95% safer’: that figure was made up, came out of a meeting of specialists
one concern, is that when vapes were initially made they were produced by small firms, not massive corporations but as they become more profitable big tobacco firms have bought up smaller vaping firms and created their own
bu 2014 all the major multinational tobacco companies had entered the e-cig market
as part of a larger policy to keep people using recreational nicotine, Philip Morris developed the technology of a modern e-cig
they did not take the product to market to avoid attraction from the USA FDA
The tobacco industry has a long history of denying the negative and harmful consequences of tobacco, but now that they have transitioned their interests into vapes people are concerned and suspicious of a repeat in strategies, denial and refusal of accountability
any claim that e-cigs are safe could be attributed to those that sell the vapes for profit
passive vaping: if you are next to someone vaping, you will inhale/ absorb some of it, possibly to the same extent as someone smoking next to you
policies in countries have made this less of a concern

formaldehyde is used to preserve science specimens
if inhaled they are dangerous, but carbonyls are only released if the e-cigarette is overheated.
this only happens if your towards the bottom of the liquid tank and is much less likely if your liquid tank is full
so this is a lot less likely
definitely dangerous if inhaled
1.79 odds ration: you are 79% more likely to have a heart attack if you are an e-cigarette smoker than someone who is not
2.72: 172% more likely if you are a smoker
nicotine itself probably is not carcinogenic, may speed cancer growth
there is no smoking gun to connect e-cigarettes particularly and specifically to any disease
cardiovascular disease and other harmful health issues only appear after a decade or two, so we would not know the relationship between this and e-cigarettes, because it is too new
we have to wait for these epidemiological studies
a lot of the scents and flavouring or flavourings that have been used in foods, so there is no reason to believe they would be particularly harmful is inhaled
however, this does not directly indicate that they are as safe when inhaled

the vapes produce the carbonyls when you burn the liquid, as said before
so the one observation is that this makes you feel physically sick once it happens, which indicates that it probably is not happening often
we would know if it was happening commonly then because people would have physical symptoms
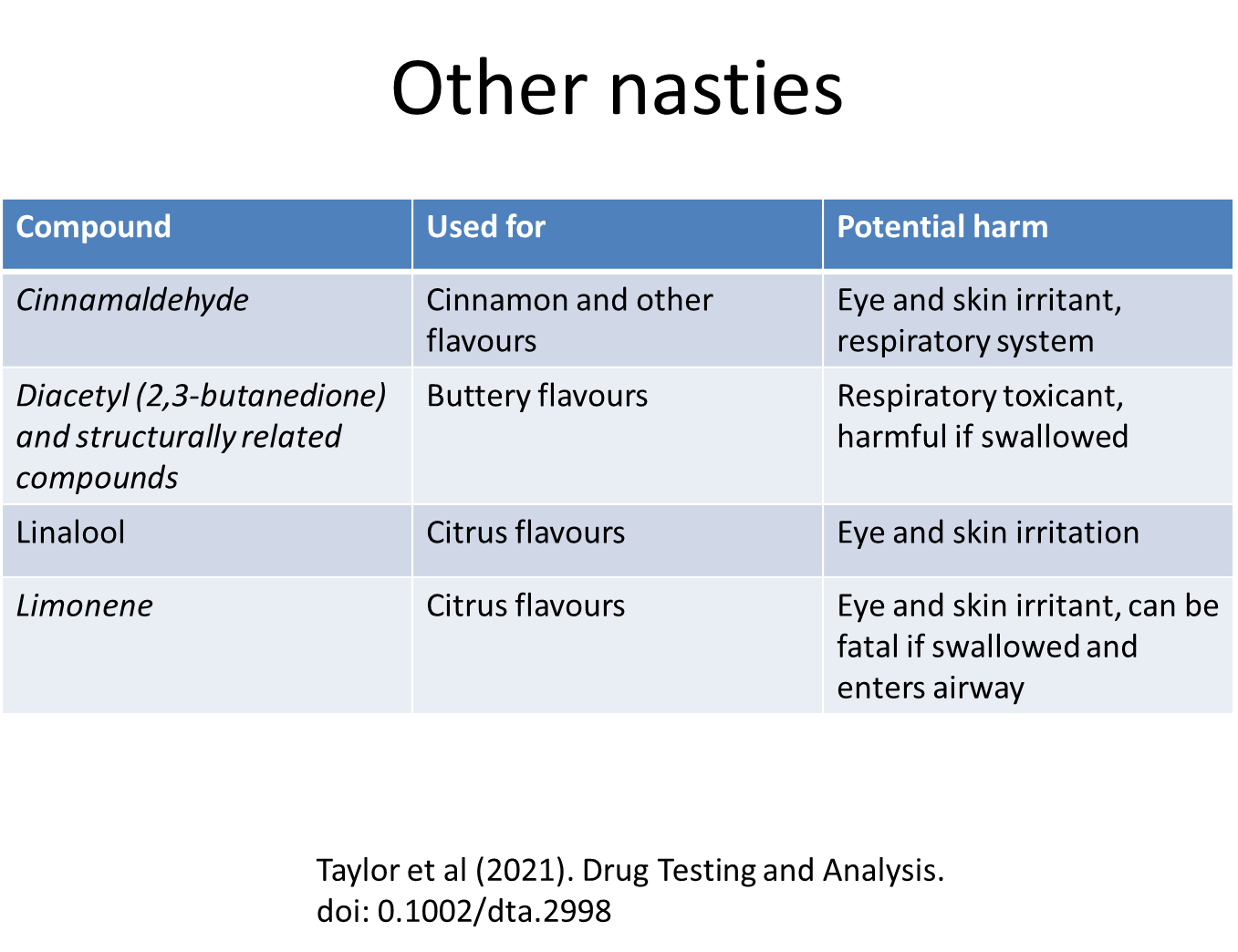
when used as intended, there is not too much evidence of them being severely harmful
most harmful when swallowed or slathered on skin so not common issue
not much evidence that these things are harmless either though
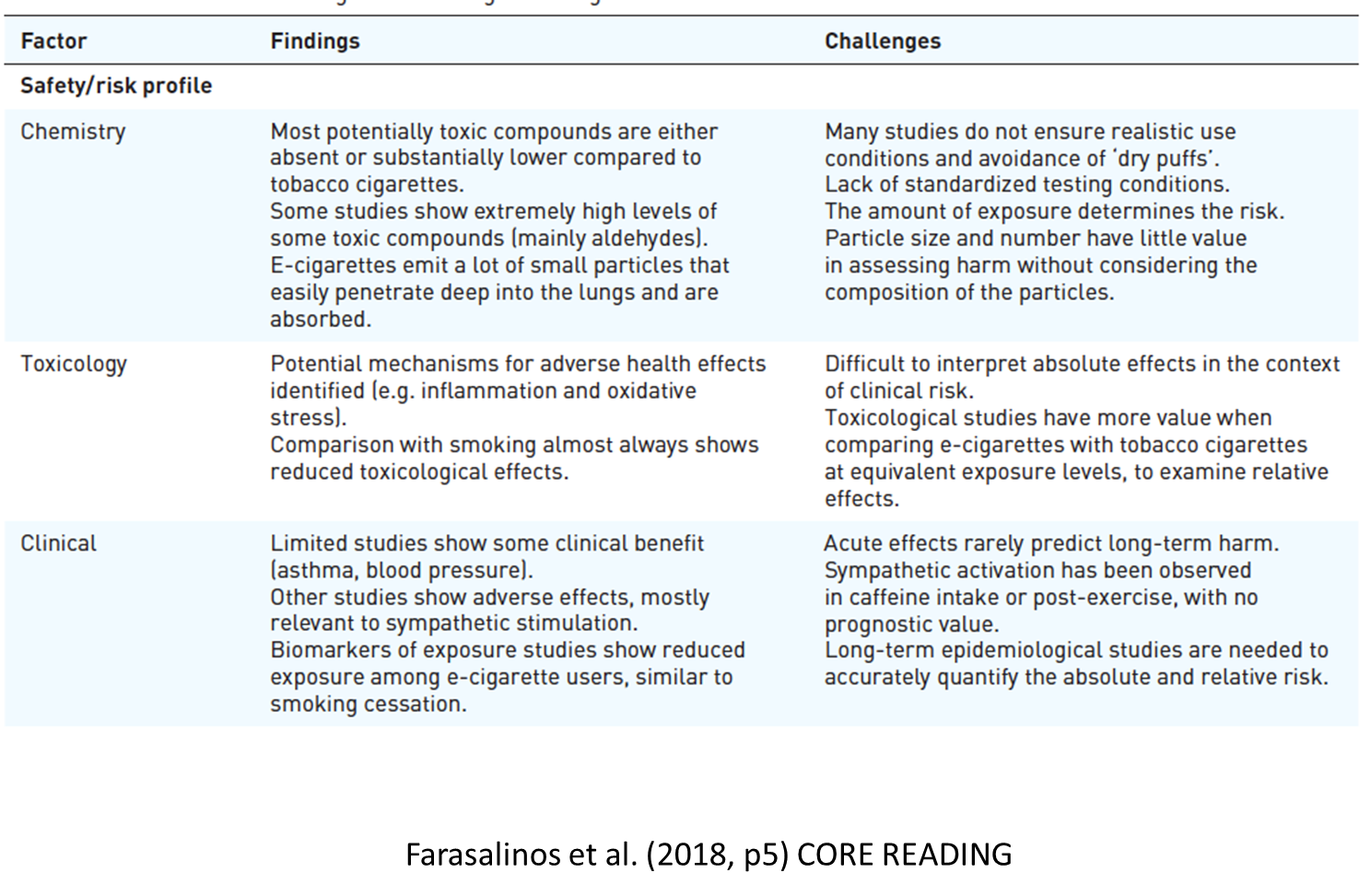
summary slide of the paper to demonstrate the bad things in e-cigarettes but also emphasise that realistically there are different reasons to believe they are harmful and less evidence that they actually are
we have to wait for longer term epidemiological studies
safety/risk profile:
Tobacco cigarette smoke contains thousands of compounds, many of which are officially classified as toxic and carcinogenic.
Smoking is a major risk factor for a plethora of diseases, particularly cardiovascular disease, respiratory disease and cancer of the lungs and other organs
The 10-year fatal cardiovascular risk is approximately doubled in smokers compared to non-smokers, while the relative risk for myocardial infarction in smokers > 50 years is four-fold higher compared to non-smokers of similar age
Smokers also have 3–5-fold higher risk for developing chronic obstructive pulmonary disease compared to non-smokers.
smoking cessation lowers the risk for developing disease or halts disease progression and improves future prognosis
Therefore, we must assess the relative safety of e-cigarettes compared to tobacco cigarettes.
safety/risk profile in absolute terms (i.e. compared to no other product) is important for the residual risk for smokers compared to quitting without the use of any substitute and the risk of e-cigarettes users who were never smokers
This may be of interest for smokers with pre-existing smoking-related disease, since smoking cessation in this population is a very effective secondary prevention measure, but many smokers fail to quit even after they develop such disease
many would say that e-cigarettes and nicotine are as harmful as caffeine
though some would argue against this
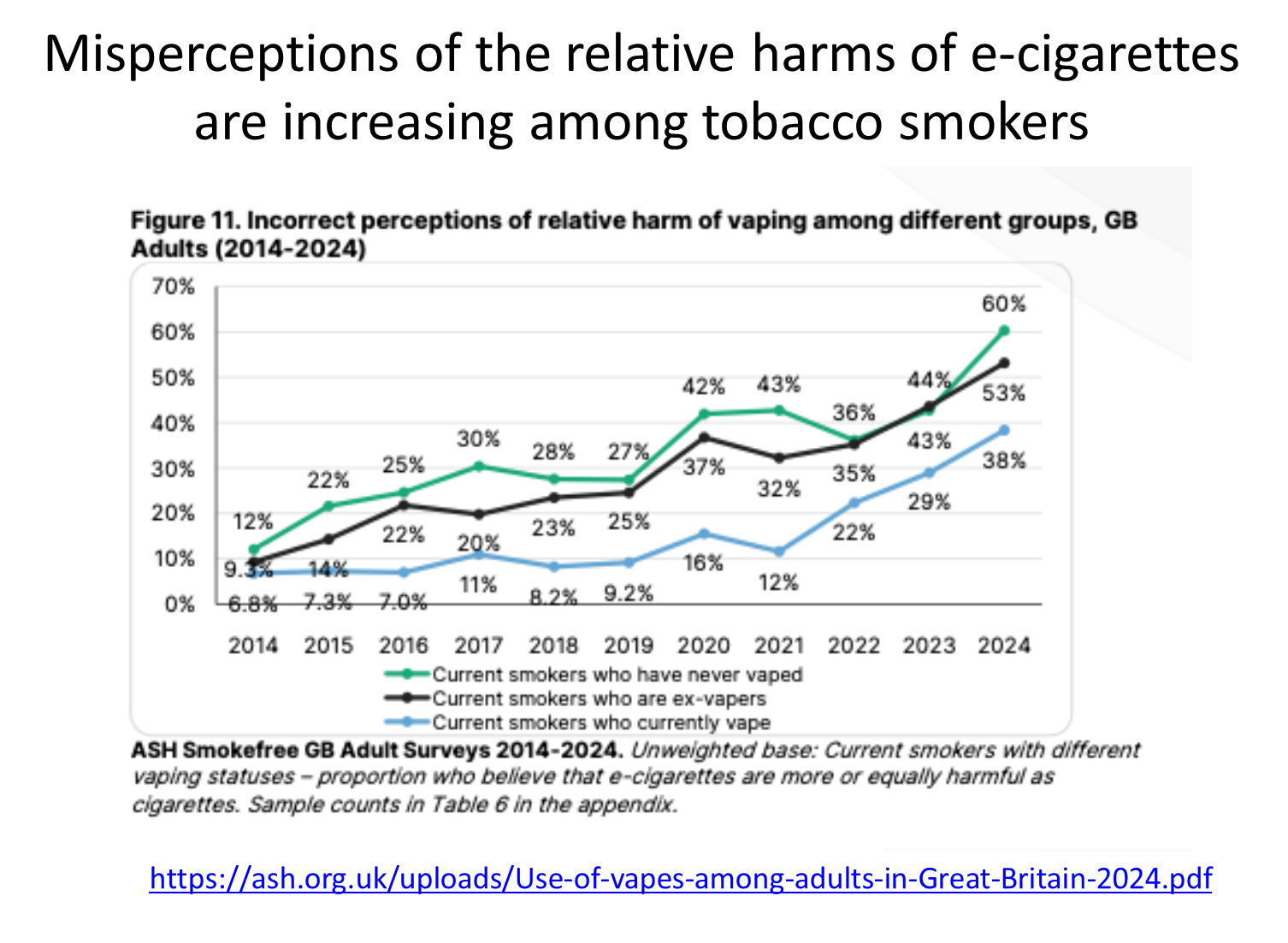
regardless of whether e-cigs are harmful or not, people will have perceptions and opinions about this
back in 2014 very few were incorrect, however, this has increased drastically by 2024
this might have implications for use of e-cigarettes on those that could be trying to stop smoking in the future
increasing change in public opinion that people believe e-cigarettes are more or equally harmful as cigarettes
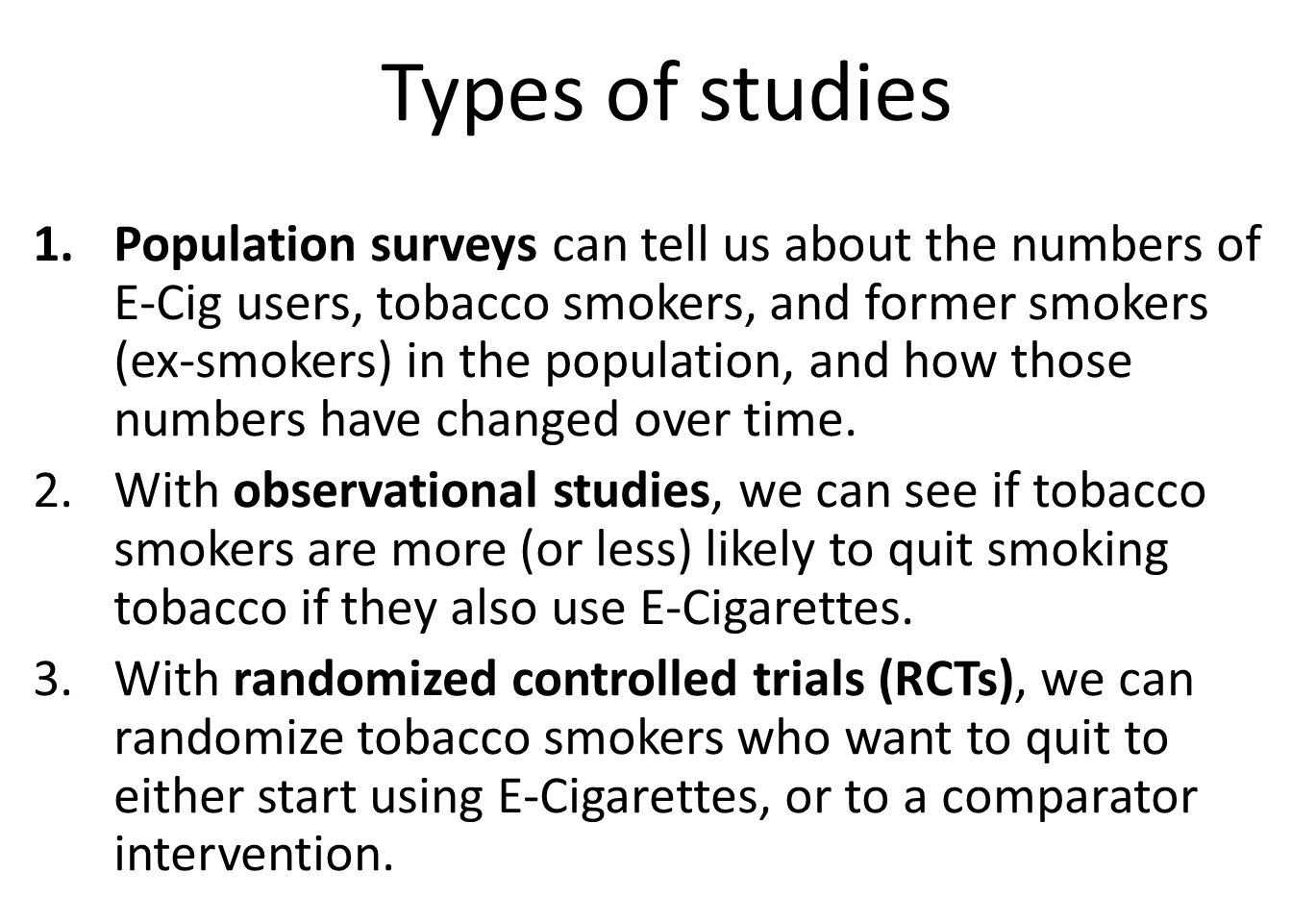

doesn’t follow up overtime, gets people representative of the UK
used a lot in Sheffield, used for smoking and alcohol
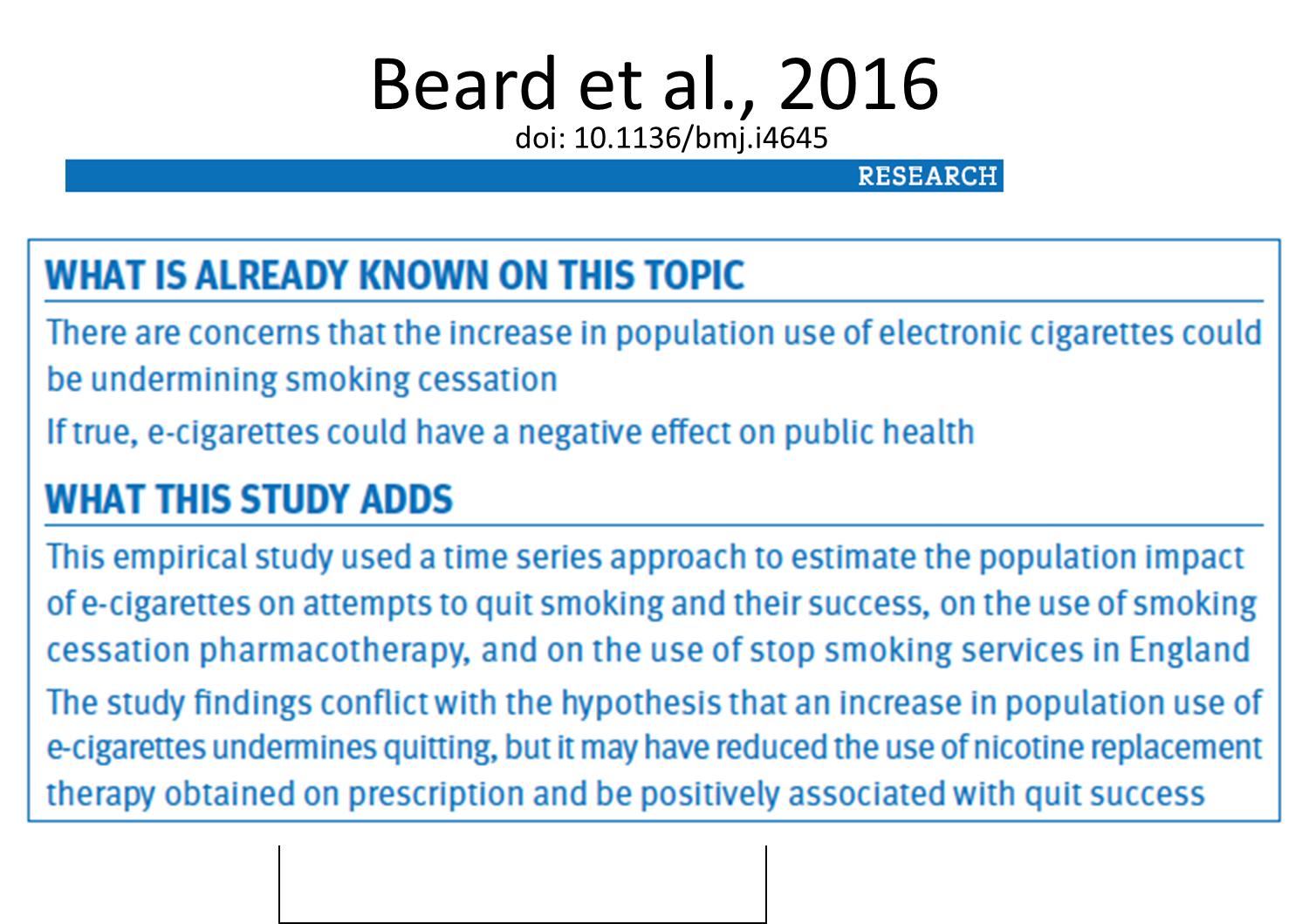
across a ten year time periods, for every 1% increase in the pop prevalence of E-Cig use among tobacco smokers, the success rate of attempts to quit tobacco smoking increased by 0.1%
among tobacco smokers who actually start vaping, they do not find any evidence they are less likely to quit
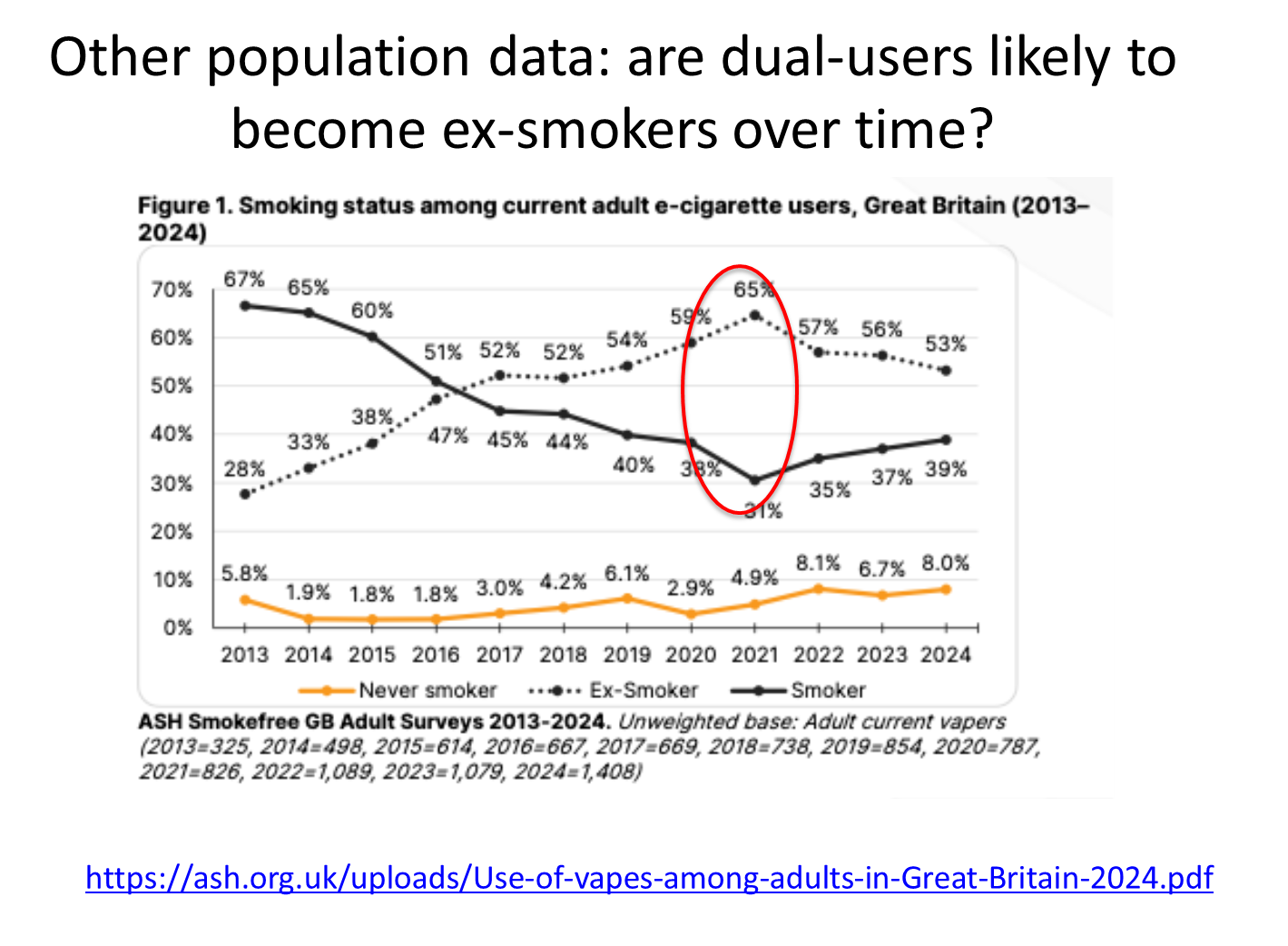
in 2013, a majority of E-Cig users are also smoking tobacco
but at some point this cross over occurs, so in 2024 53% used to smoke tobacco but quit
over time people are leaving the group of vapers who smoke to vapers who used to smoke
most plausible explanation for these observed trends
no manipulation of variables, not that they are always observed
these studies are less informative of cause and effect/ which caused which
could be why longitudinal studies are more helpful
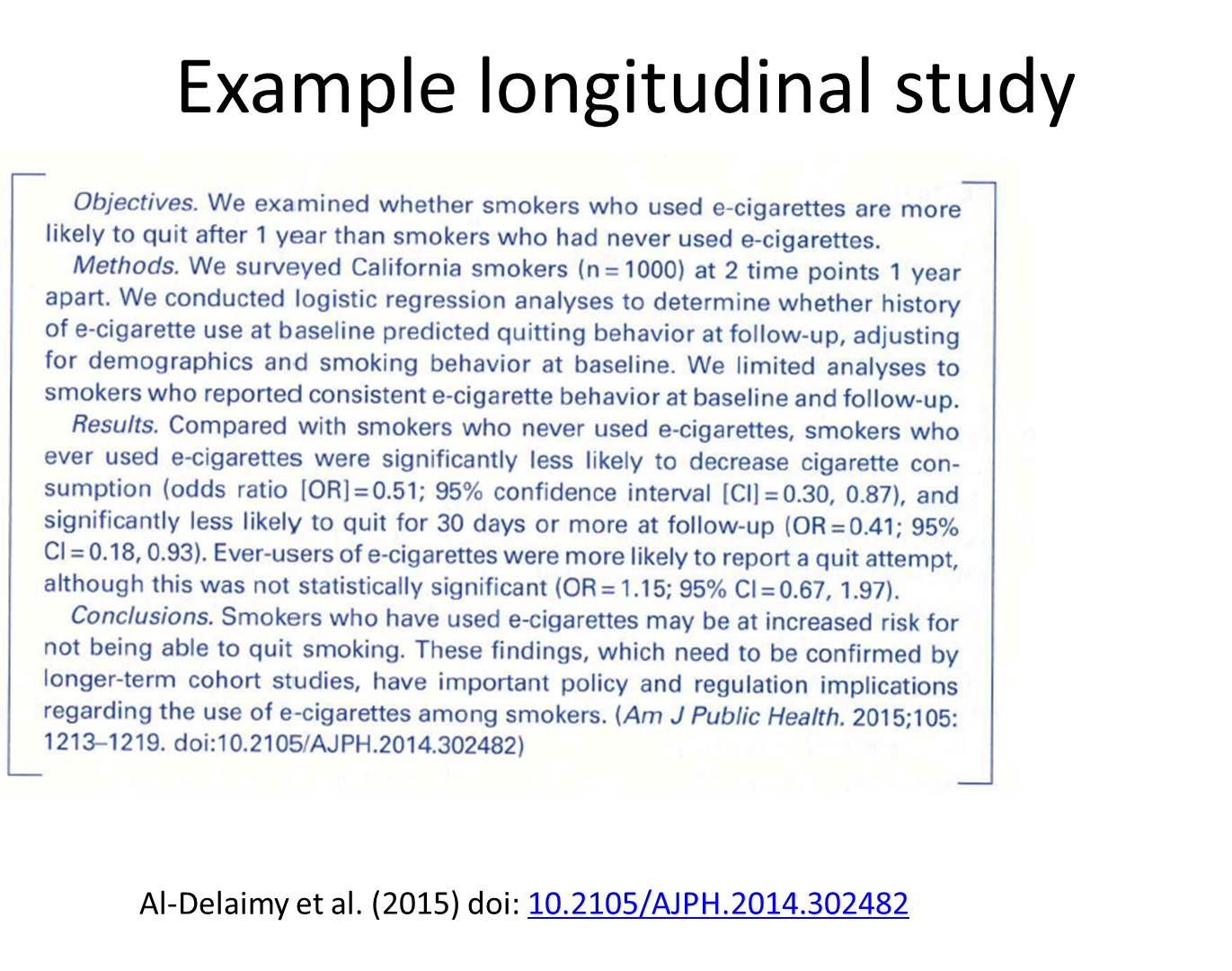
asked people who smoked questions, one year apart
e-cig use reduces the chance of quitting by 27%
smokers who use e-cigs are at a lower probability of stopping smoking
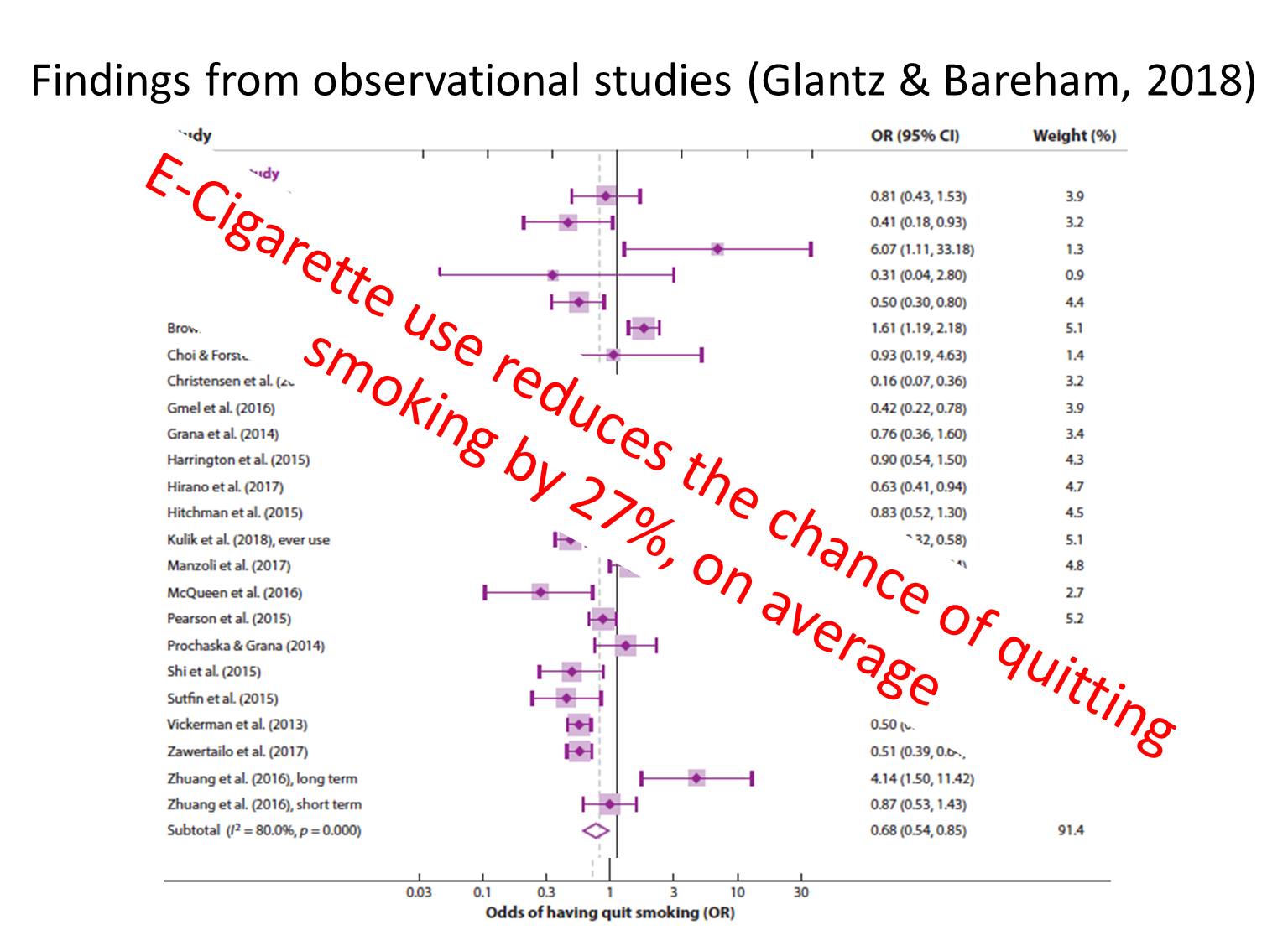
quite a stark findings, suggests that smoking tobacco and advising to quit, you should not suggest e-cigs
These results suggest that e-cigs are contributing to the tobacco epidemic by attracting smokers who are interested in quitting but reducing the likelihood of those smokers to quit successfully.
This effect may be reflected in the fact that in 2015 the number of cigs consumed in the US was higher than in 2014, the first time cigarette consumption increased since 1973
but there are limitations to this study
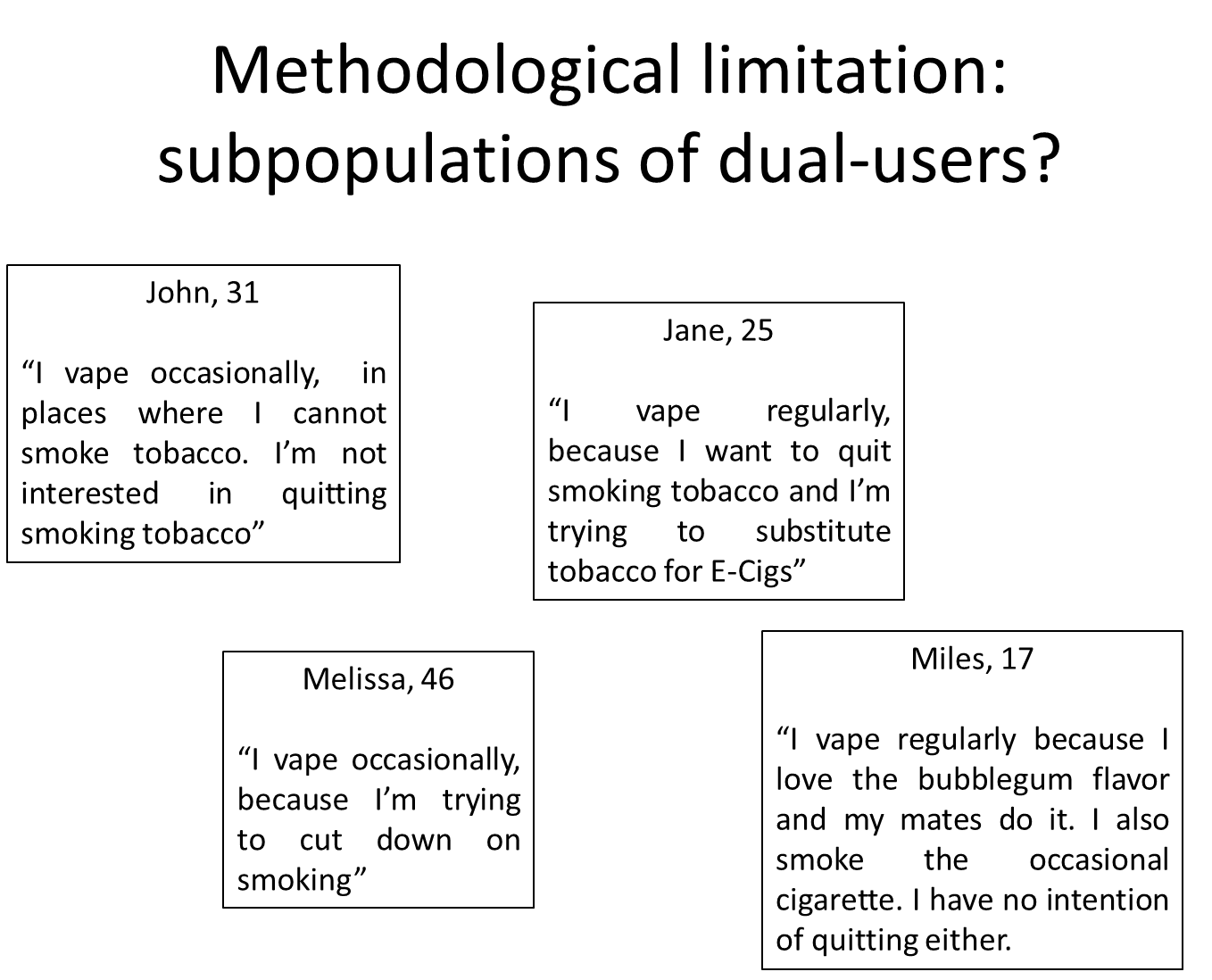
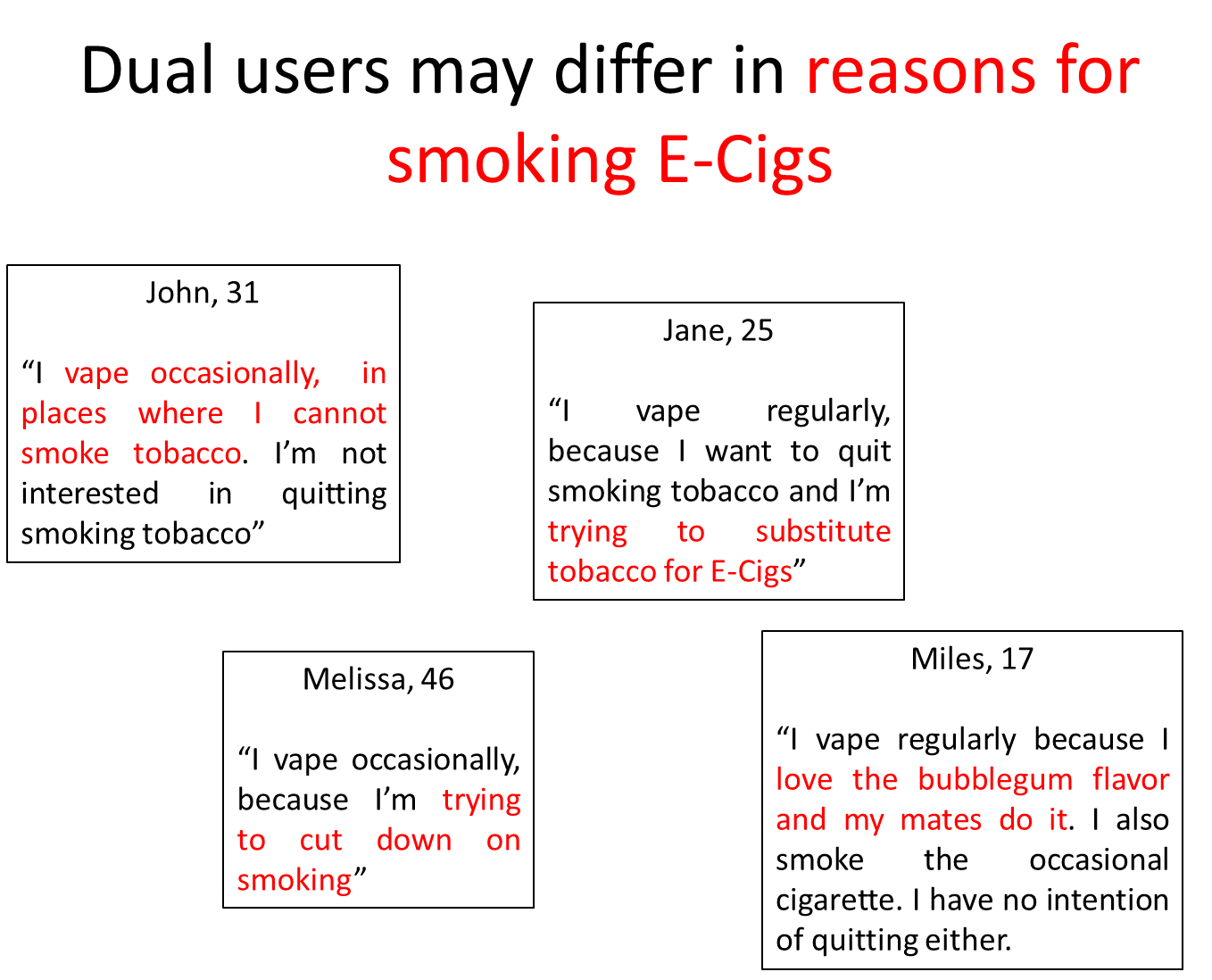
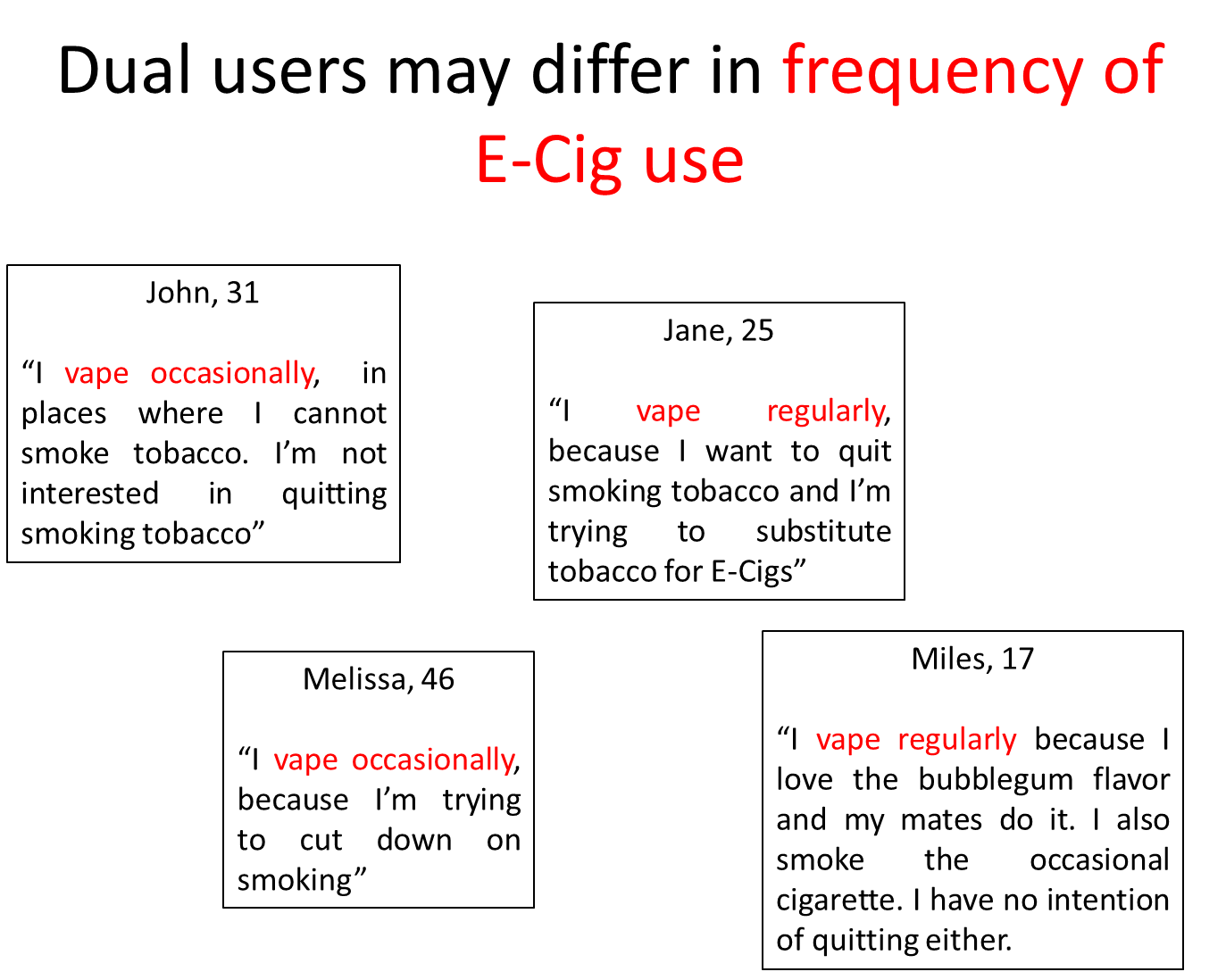
there could be large variation within this study, subpopulations of dual users, such as those with no interest in quitting but smoke e-cigs when they can’t smoke tobacco, or use it to quite
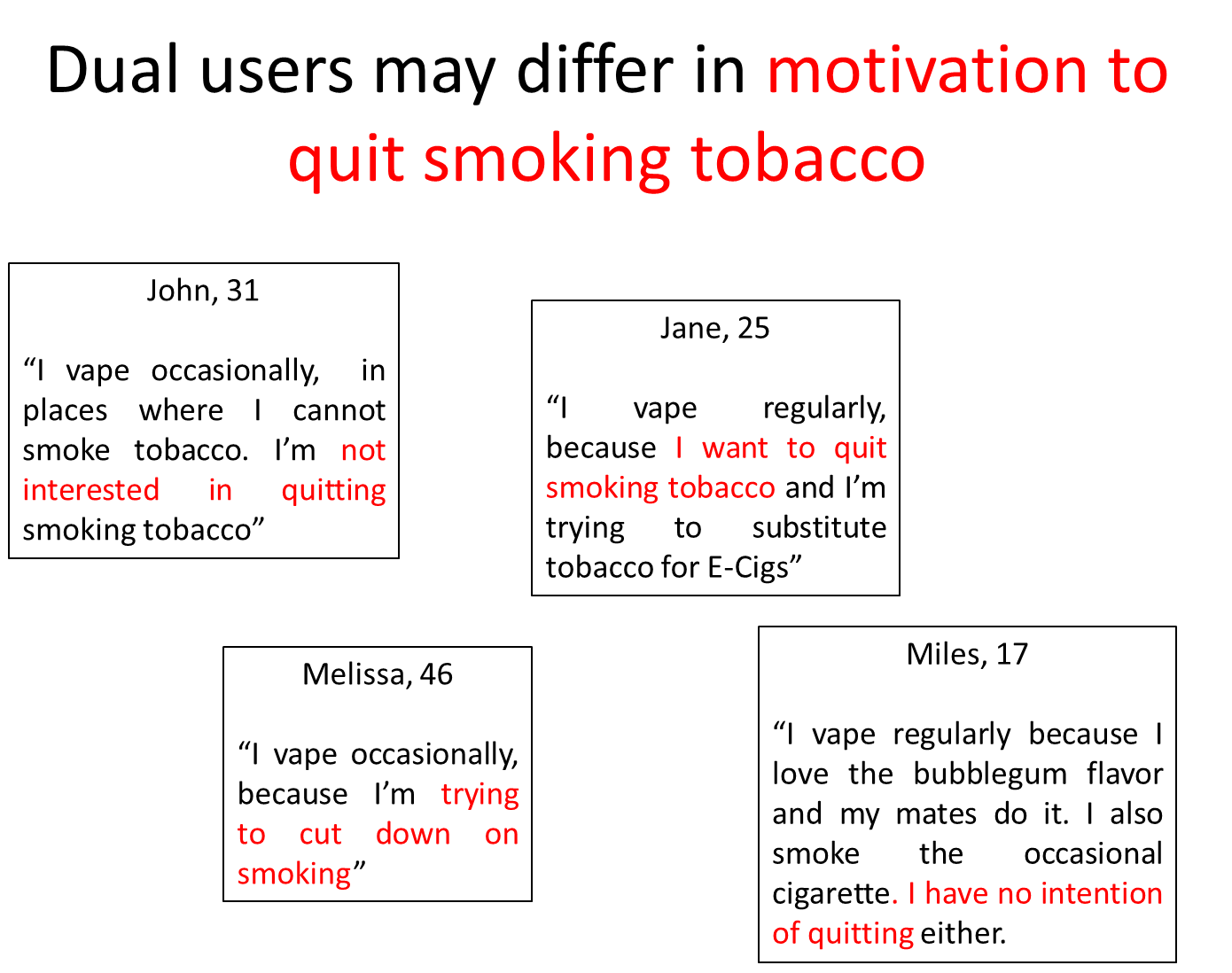
these groups may differ in the extent they want to quit, why they are using e-cigs and the frequency of use
they differ in various ways
thus the results may be influence by individual factors of dual smokers
not everyone’s intention is to stop smoking
they recruited people that use e-cigs sometimes and other times where people relied heavily on them
remember you are observing pps, so the different sample categories might explain why these associations concluded in Glantz’s meta-analysis vary so much
maybe if we just focus on dual smokers who really want to quit, maybe then we would get a different conclusion
maybe if we just focussed on people who used e-cigs and really want ot quit, we could see different results in smoking sensations than included others who have no intention of quitting
since 2018, there has been so many RCT of e-cigs, that there was a cochrane review
this is the gold standard for evidence in medicine, really good quality research
90 studies, most were RCT with typically understandable controls
these are the main findings,
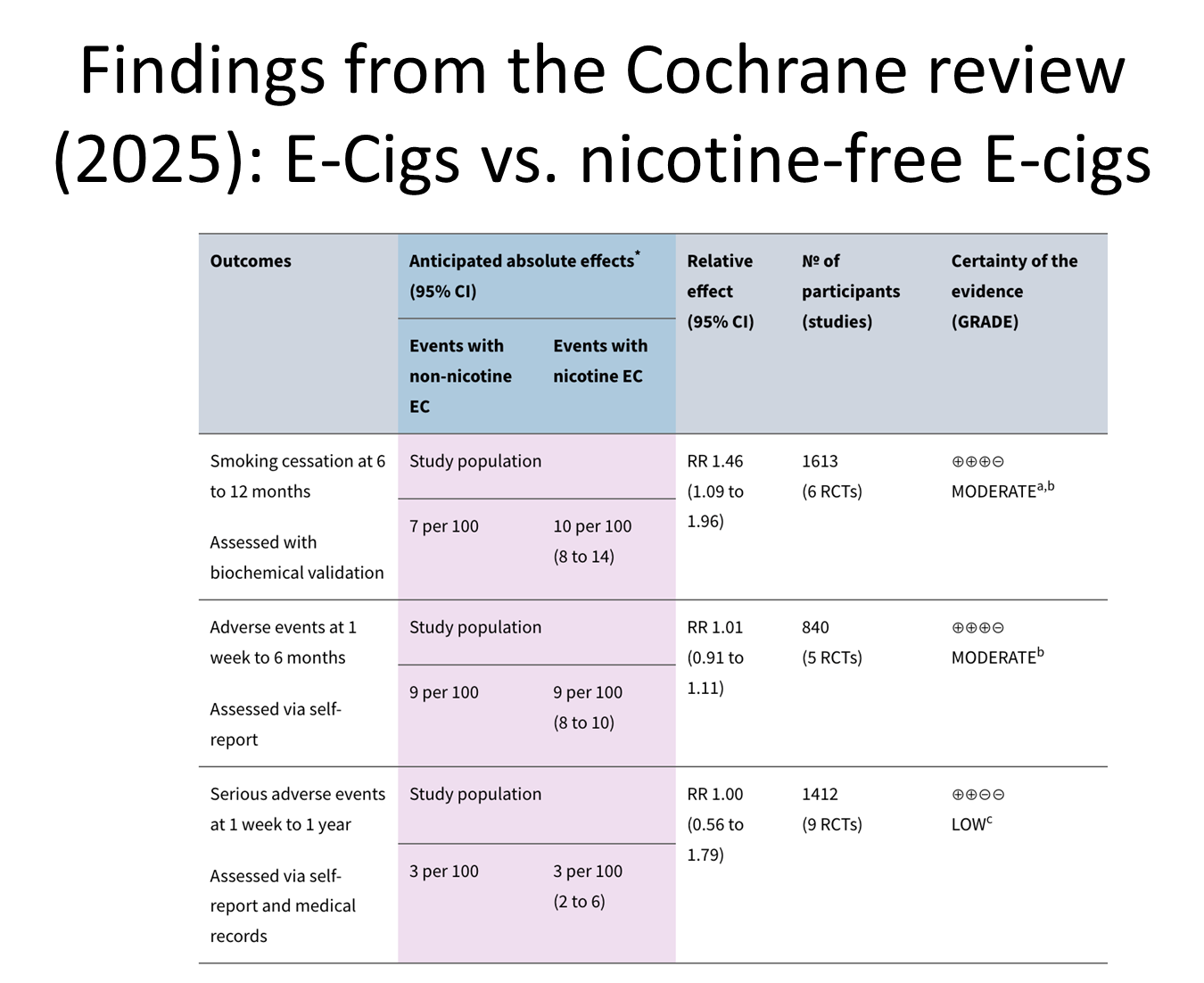
comparison of E-cigs with nicotine to those without
how many quit smoking 6-12 months later: 10 in 100 with nicotine and 7 in 100 in the placebo one
relatively few compare e-cigs with nicotine to placebo
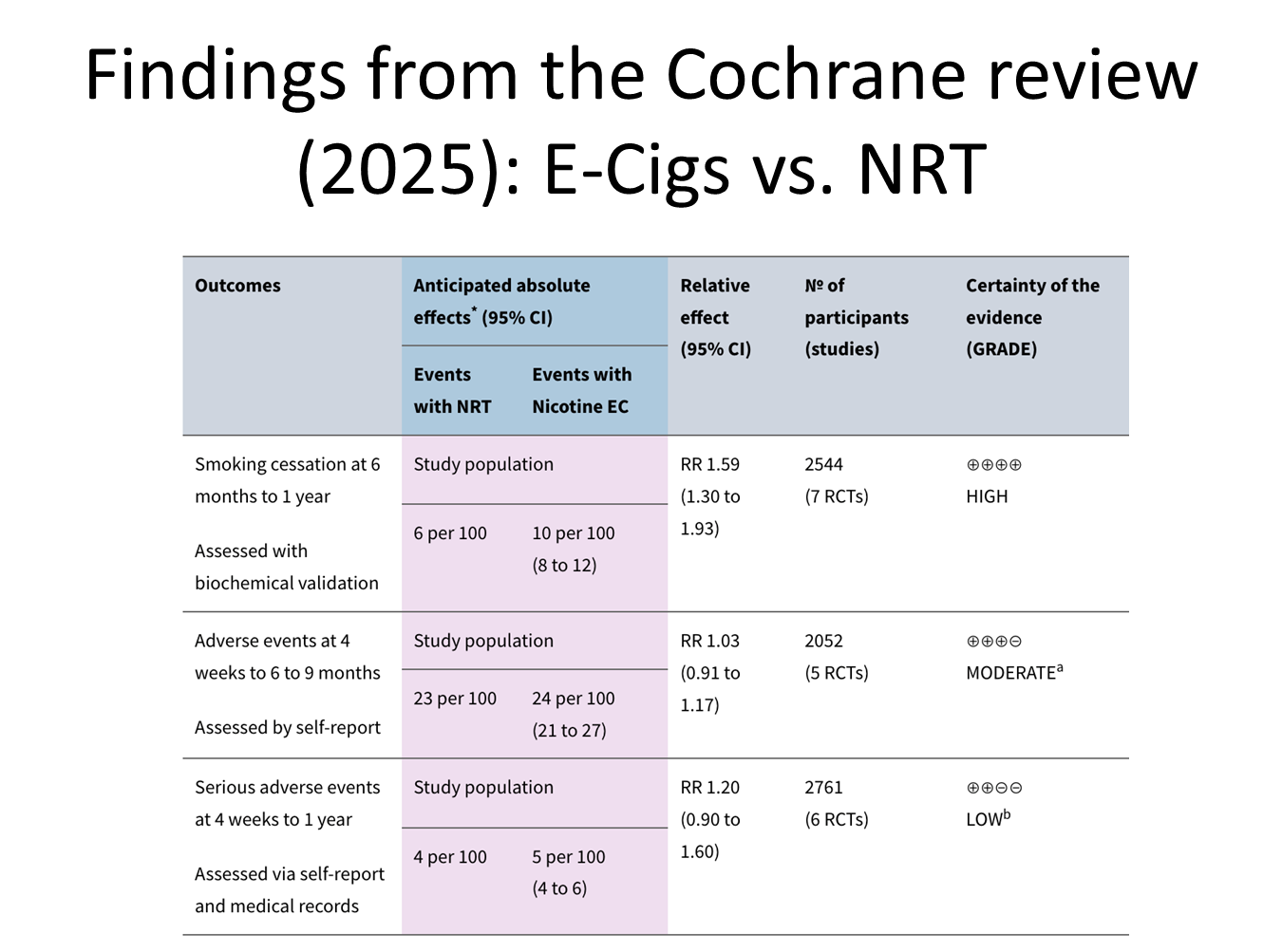
comparing to nicotine replacement therapy: this was and remains the main recommendation
giving the NRT, 6 in 100 will quit 6 in 100, but 10 in 100 for e-cigs
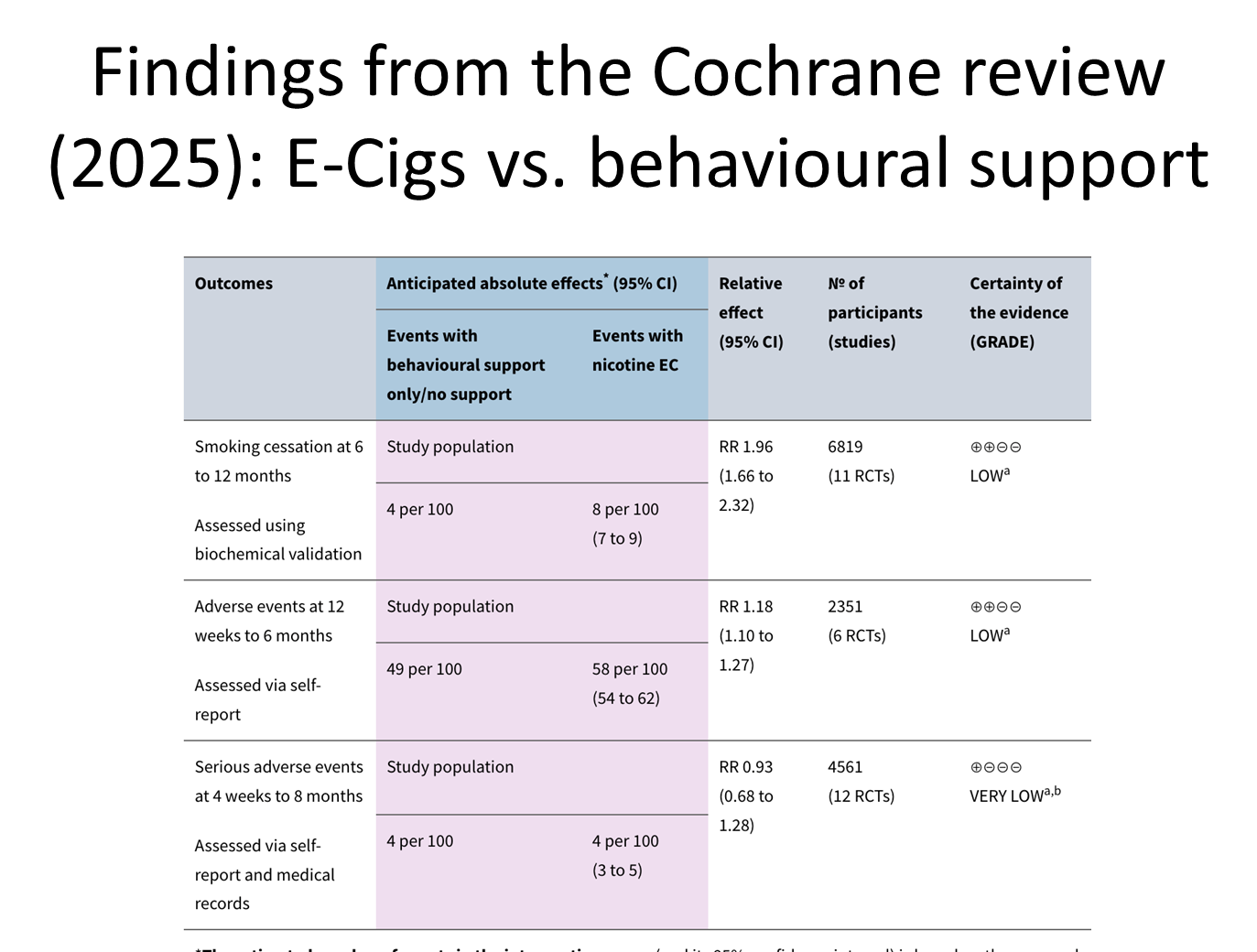
twice as likely to quit if you use an e-cig than behavioural support
if not many people in the sample quit, it is hard to make generalisations
a RCT has to have standardised treatment, but if e-cig technology is rapidly changing, treatment would not be able to keep up with this/ be applicable once published
take home indications, this conclusion is based on the systematic review
only 10 in 100 will quit
an emergence of nicotine products that are attractive to young people
now bigger tobacco firms are investing in the product and aggressively marketing them
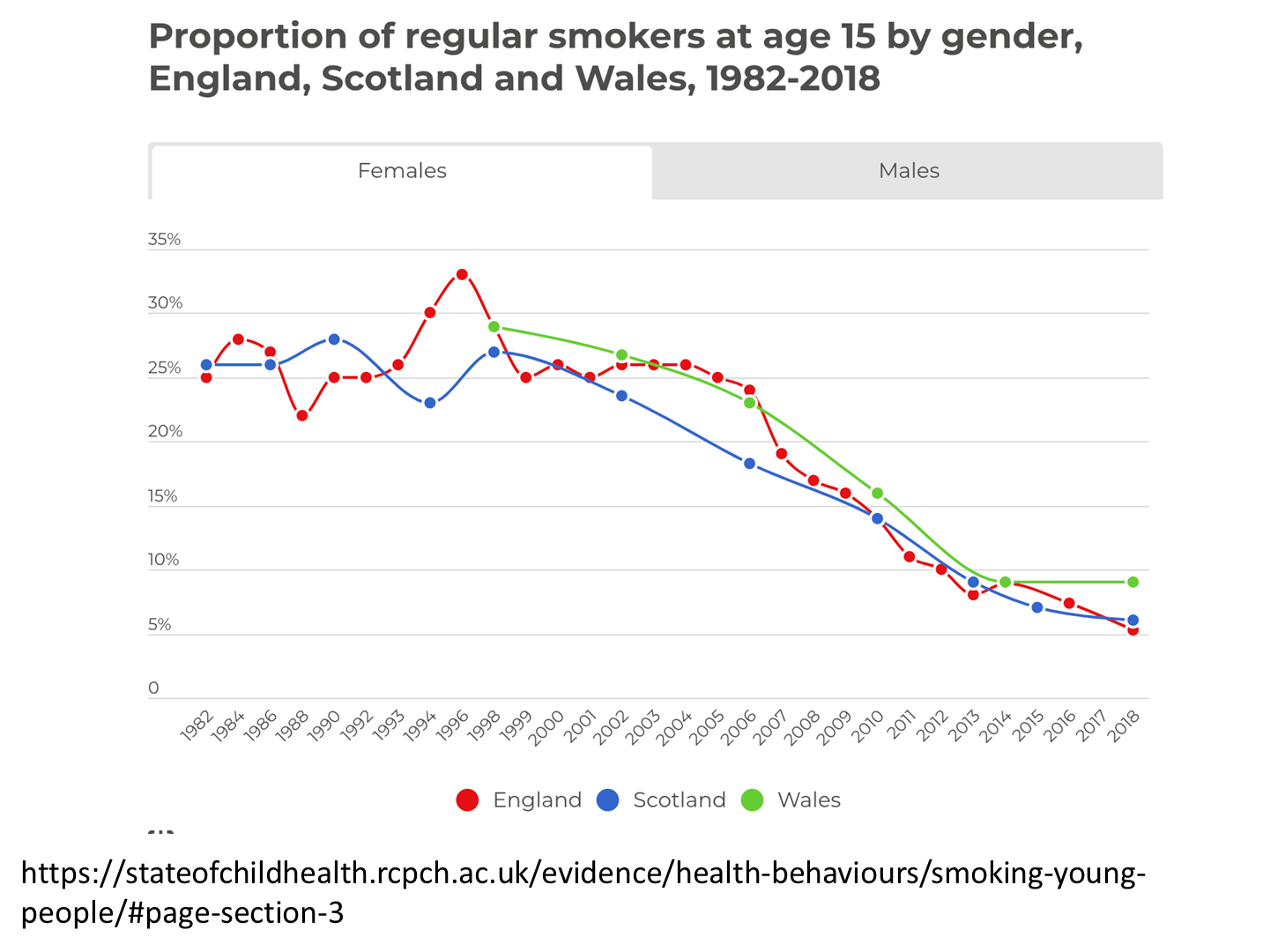
looking at the number of 15 year olds smoking tobacco regularly was approx 25% in the 90s/80s
it has dropped by about 20%, but e-cigs are messing this up
the argument here is if you exclude the people that use e-cigs, the trajectory is encouraging, but if you include them
flavours appear intended to appeal to young peopel
pretty clearly, the answer is yes
young people who use e-cig clearly are argued to have not otherwise started to have smoked tobacco by Glantz
but others argue differently
e-cigs are typically pronounce in the older age group
this leads to the gateway hypothesis
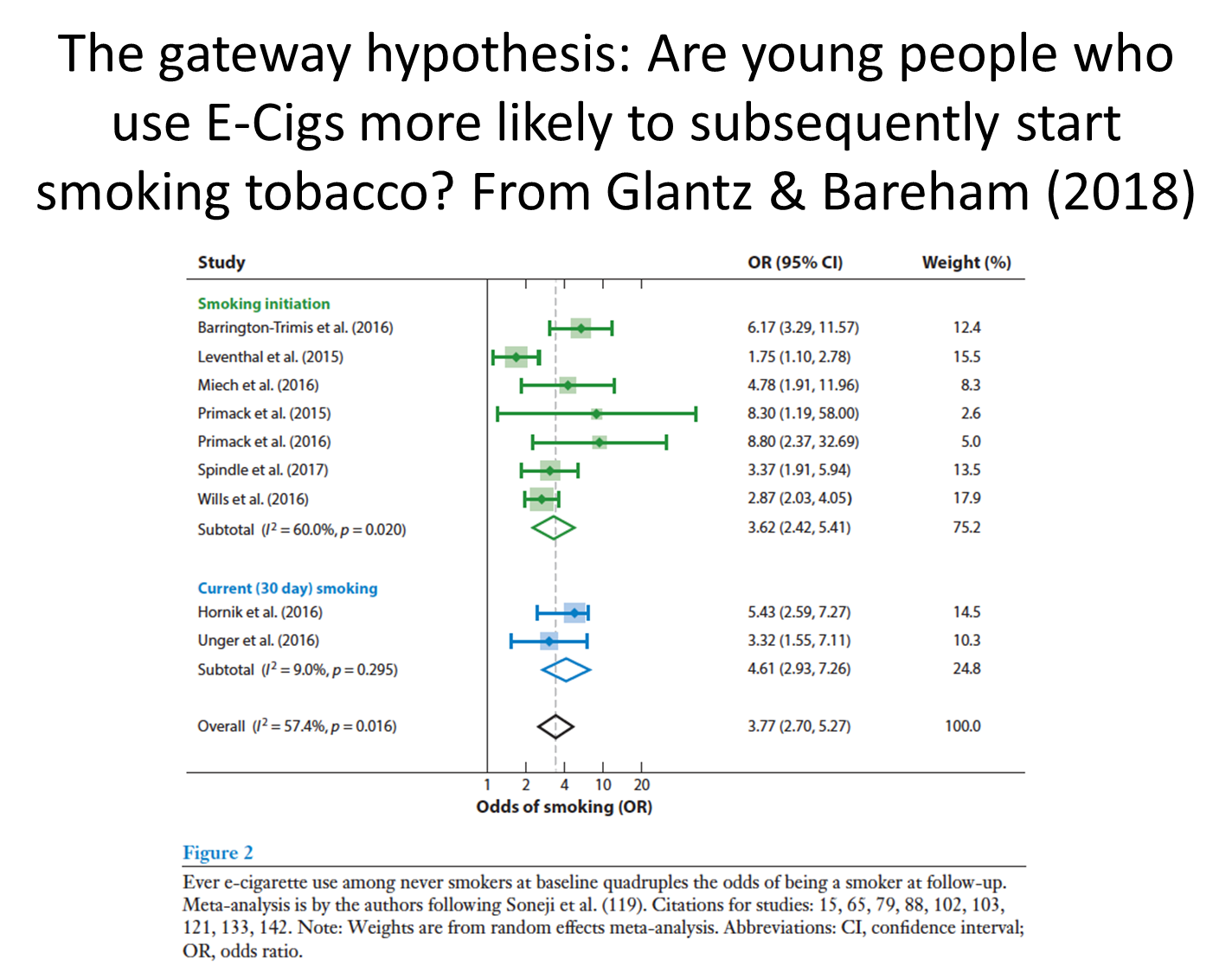
Glantz find evidence that among young people your chances of becoming a smoker of tobacco is quadrupled if you have previously smoked an e-cig
lengthy summary of this analysis of longitudinal experiments
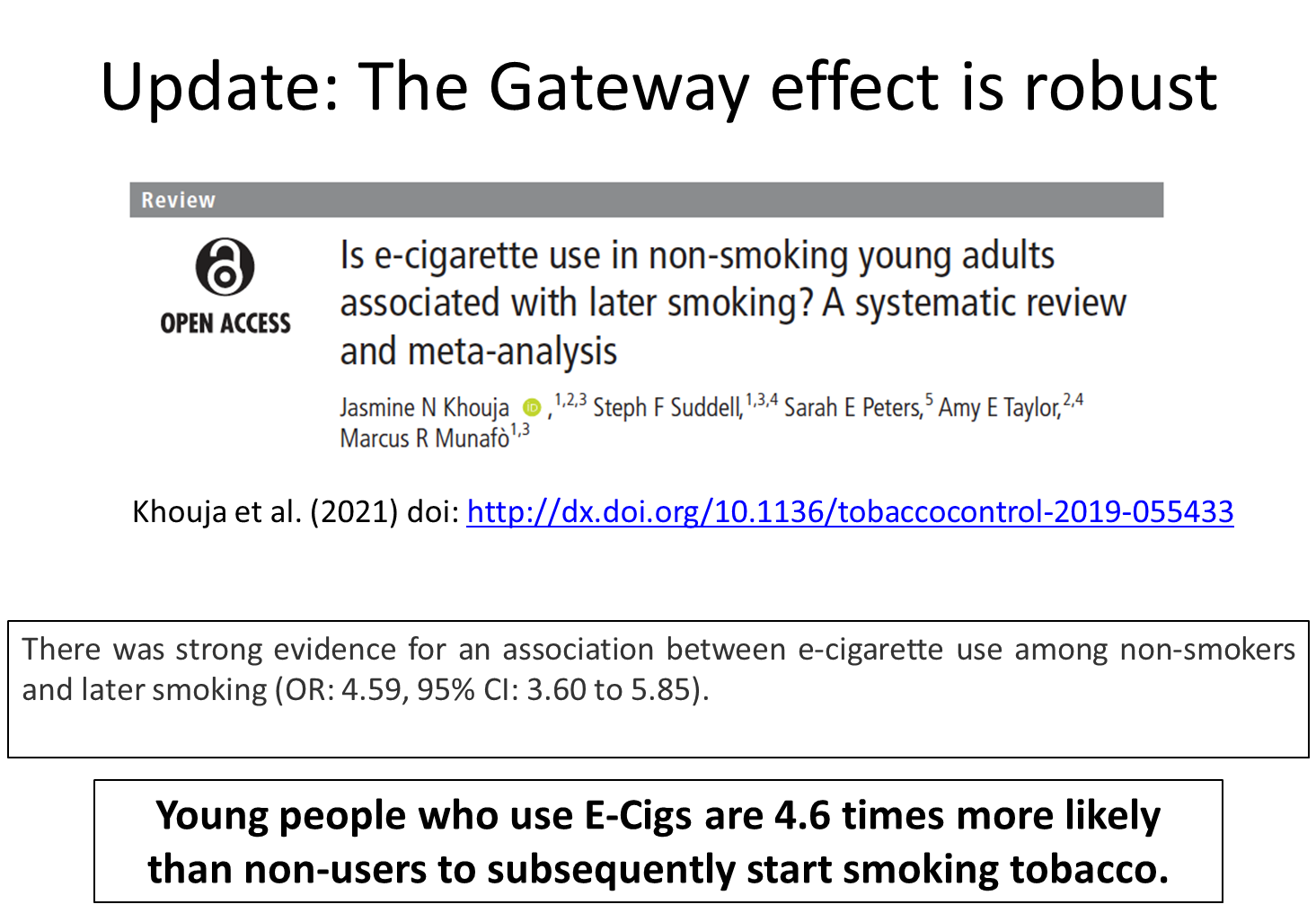
a lot of evidence since then, which explores the gateway effect
they find that the gateway effect is really robust, there is an association between young people who use e-cigs to then use tobacco when compared to those who never touched e-cigs

limitations as nothing is entirely robust
they used self-report measures without biochemical verification
none of the studies used negative controls which would provide stronger evidence whether the association is casual
much of the evidence failed to consider the nicotine content of e-liquid used by non-smokers meaning it is difficult to make conclusions about whether nicotine is the mechanism driving this association
always true for everything we study
lots of reasons to be skeptical
the data for the UK shows the use of e-cigs on young people is increasing
data suggests this is not as a transition from tobacco use
Reading- electronic cigarettes: an aid in smoking cessation or a new health hazard?
Introduction
in 2015, WHO calculated that 22.7% of the global pop > 15 years was smoking tobacco ciggies; represents 1.1 billion people
6 million deaths annually due to smoking
predicted 1 billion will die prematurely from smoke related disease during 21st century
USA smoking causes 1 in 5 deaths, total toll approx 480,000 per year
in europe it is 700,000
to reduce smoking, the WHO developed the framework convention in tobacco control (FCTC)
started 2005
comprised of 168 countries that shared a common dedication to eliminate the tobacco epidemic
their responsibility was to develop guidelines, policy options and recommendations that can be implemented globally
the FCTC created MPOWER in 2008, a collection of policies aiming to reduce demand for tobacco
MPOWER:
Monitor tobacco use and prevent policies
Protect people from tobacco smoke
Offer help to quit tobacco use
Warn about the dangers of tobacco
Enforce bans on tobacco advertising, promotion and sponsorship
Raise taxes on tobacco
These efforts have substantially reduced smoking prevalence in the past
Smoking medication
nicotine replacement therapy
success rate of less than 7% when assessing the smoking status at 1 year
this can be attributed to the low speed of nicotine delivery and to the absence of the ritual associated with the psycho-behavioural aspect of smoking dependence
oral medication
low success rate even in well-designed controlled trials
some smokers do not seek out help from a smoking-cessation service
so the most successful method is quitting without an aid
harm reduction
strategy and policy of reducing adverse health consequences of recreational drug use to those who cannot or are not willing to achieve complete abstinence
mainly developed for psychoactive drugs
proven to reduce health risks and improve QOL
is endorsed by WHO and is now legislation in several countries
has been proposed for decades for smoking, related to the use of e-cigs
The basis for this was first mentioned by Michael A.H. Russell, who noted in 1976 that the combustion process, rather than nicotine, is responsible for smoking-related disease.
Subsequently, smokeless tobacco products were suggested as a harm-reduction approach.
lower-risk alternatives are seen in Sweden, many use snus instead of tobacco cigarettes now
Because of this pattern of tobacco use, Sweden has the lowest death rates from cancer and cardiovascular disease in men compared to any other European Union country
Ramström and colleagues presented aggregate data and reported that the overall prevalence of daily tobacco use among Swedish men was 30.8%
However, the prevalence of daily smoking was 12.3%, while the prevalence of daily snus use was 20.2%
The high prevalence of snus and low prevalence of tobacco cigarette use among tobacco users is at least partly responsible for the lowest death rates from cancer and cardiovascular disease that are observed in Sweden compared to any other European Union country
E-cigs
electronic devices that evaporate a liquid consisting of humectants (mainly propylene glycol and glycerol), flavourings and (can be sold without) nicotine
created in 2004, awareness and use has grown exponentially since 2009
the public health community thinks that e-cigarettes could help smokers to quit and accelerate the smoking decline by supplementing other tobacco control measures, resulting in a net public health benefit
Another part considers e-cigarettes as a threat that could undo the progress made by the tobacco control movement over the past decades by making smoking and nicotine use socially acceptable again
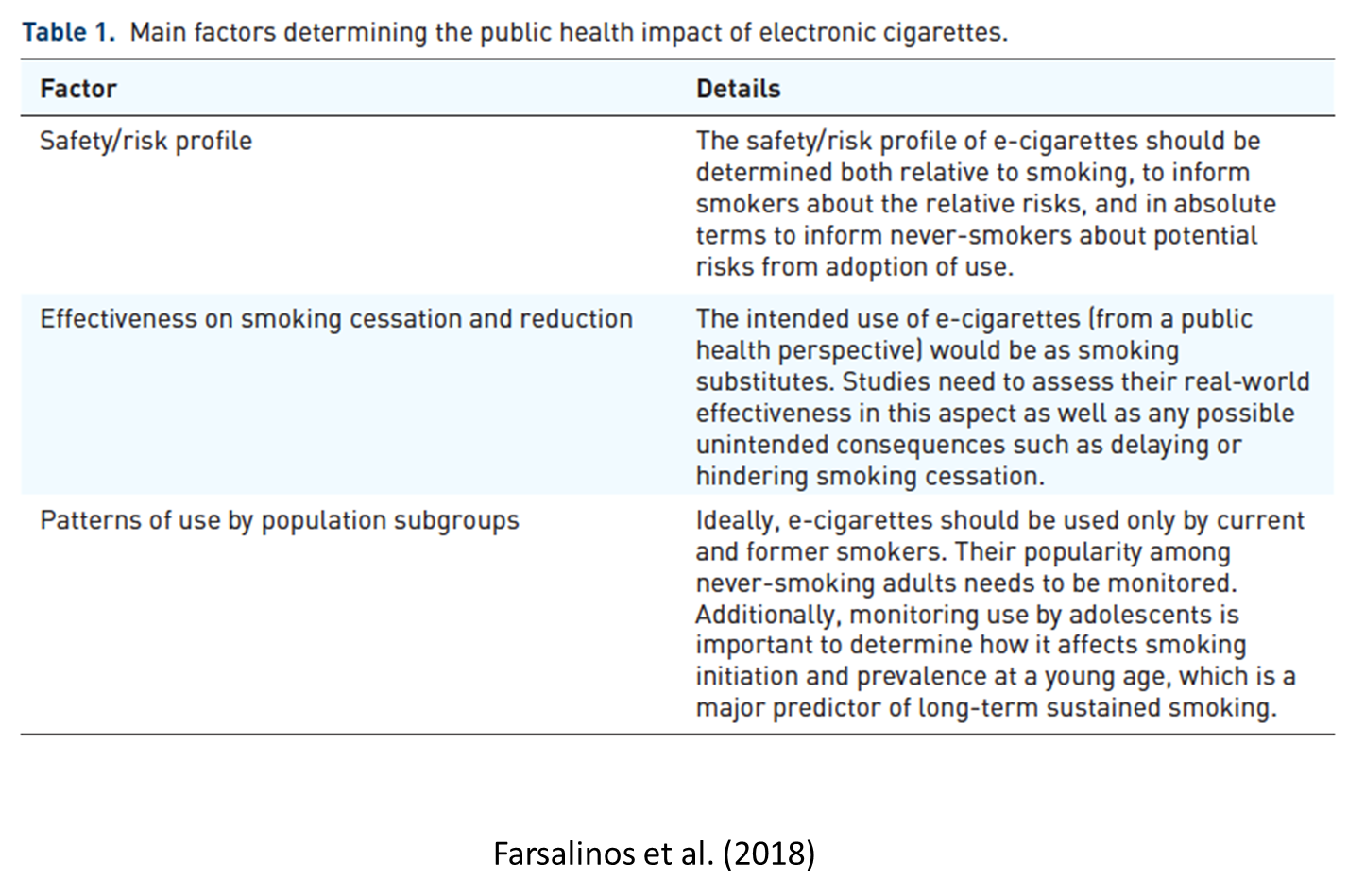
Factors determining the public health impact of electronic cigarettes
That table from the lecture
Second factor: their effect on smoking status and consumption of smokers
The intended role (from a public health perspective) of e-cigarettes is to be used as smoking substitutes
Reduction in smoking consumption is expected to result in some benefit, although it’s less pronounced than complete abstinence.
Third: prevalence and patterns of e-cig use in different subgroups
E-cig use is an inhalational habit that resembles smoking and can deliver nicotine.
thus, could create dependence and sustained long-term use by never-smokers, which would result in added health risk compared to not using any inhalational product
it is important to assess which population subgroups are using e-cigarettes, with particular attention to the smoking status before initiation of e-cigarette use
use by adolescents needs to be monitored. Most long-term smokers start at a young age and early initiation predicts regular smoking in adulthood
Adolescents are prone to engage in risky behaviours, E-cigs could attract their attention but could also theoretically serve as a ‘distraction’ from use of tobacco cigarettes.
Another reason for monitoring the prevalence among never-smokers is the possibility that e-cigs may have a gateway effect to smoking.
people who have never and would have never smoked become addicted to e-cigarettes and then transition to tobacco cigarette use.
important to assess the popularity of e-cigarettes among smokers
To result in significant public health benefit, any smoking cessation aid needs to be not only effective but also acceptable and popular among the intended population subgroup (smokers)
A product that is more attractive for smokers will result in a higher proportion of them quitting or reducing smoking.
There is a table that shows the main findings and challenges in e-cig research (table 2)
Safety of electronic cigarettes
e-cigarettes being available mostly in the past 10 years, it is not unexpected that long-term epidemiological evidence of their health effects is still not available.
However, there is extensive preclinical research, mostly on chemistry and toxicology of e-cigarettes
The main differences between e-cigs and tobacco cigs expected to largely determine the potential risk discrepancies are the lack of combustion and tobacco in the former
E-cigarettes function by evaporating a liquid, which is rapidly condensed into an aerosol and is then inhaled
main ingredients in e-cigarette liquids are compound used extensively in food, pharmaceutical and cosmetic products
to the best of my knowledge, there is no chemical which was specifically developed to be used in e-cigs
Propylene glycol - recognized as safe for use in food products by the US FDA in 1982 and is used in pharmaceuticals
Glycerol - essential for living organisms, has been approved for use in food products since 1959, widely used in cosmetic, pharmaceutical and food products
both are used as solvents and production of visible aerosol
Flavourings are mostly, chemicals approved for use in food products, however, e-cigs introduce a new route of long-term daily exposure to these compounds, through inhalation. There is limited evidence about the effects of inhaling these compounds.
This creates uncertainty mainly for the local effects in the respiratory tract, raising little concern about potential risks.
chemistry profile:
substantially less harmful compared to tobacco cigarettes for toxic compounds such as tobacco-specific nitrosamines, phenols, nitrates, polycyclic aromatic hydrocarbons, aromatic amines and carbon monoxide
Many are absent from e-cigarettes, while others are present in substantially lower levels.
traces of tobacco-specific nitrosamines are present in e-cigarette liquids, resulting in non-detectable levels to the aerosol unless the samples are spiked with standard nitrosamine solutions
Concerns about the emissions of carbonyl compounds from e-cigs, while studies have shown lower levels of formaldehyde, acetaldehyde and acrolein compared to smoking, recent studies have found levels similar to or higher than in tobacco cigarette smoke.
these studies could have been observing ‘dry puffs’ without recognising it, where the liquid overheats
Another issue is the emission of metals
e-cigs are metallic structures that are expected to emit metals to the aerosol
Some metals were found at levels higher compared to tobacco cigarettes.
although, the levels detected are below safety limits for inhalational medications or for occupational exposure and do not seem to represent any substantial health risk, emissions can be further reduced using appropriate materials.
The potential toxicity of the emitted compounds is the major determinant of adverse health effects, while particle size will affect the potential for penetration and exposure of tissues
Therefore, if toxic compounds are transferred in small particles into the lungs, the health risk will be increased compared to larger particles
Toxicological studies have detected several mechanisms through which e-cigarettes could cause adverse health effects, including oxidative stress, inflammation and gene expression
Other studies have found minimal effects when compared with smoking.
It is difficult to interpret in vitro studies in the context of clinical effects, mainly because the in vitro response depends on the level of exposure, and the dose that could represent realistic clinical effects has not been determined.
Such studies have more value in evaluating comparative effects between different products, especially when similar levels of exposure are examined
The majority of studies comparing e-cigarette aerosol with tobacco cigarette smoke have found lower toxicity for e-cigs
The effects of e-cigs
very little studies
Some evaluated the acute effects of use and found elevated blood pressure and aortic stiffness
which are related to the sympathetic effects of nicotine
none of these factors have any long-term adverse health implications
One study identified increased cardiac sympathetic activity in e-cigarette users after abstaining from nicotine intake for several hours
the study did not include a smoking group for comparison
Other clinical studies have shown objective improvement in respiratory function of asthmatics after switching from smoking to e-cig use which was sustained for 2 years, and improvement in blood pressure and hypertension control
Of particular importance are studies evaluating biomarkers of exposure to toxic chemicals
Such studies have long been performed to assess smokers’ exposure and now assess the exposure of e-cigarette users
The studies have shown substantial reductions in biomarkers of exposure, similar to non-smokers or former smokers who use pharmaceutical nicotine products
current evidence suggests e-cigarettes are less harmful than smoking, although the level of risk reduction is an area of disagreement and intense debate
Efficacy in smoking cessation and reduction
A study of vape shop customers objectively assessed the smoking status of participants by measuring exhaled carbon monoxide and identified that 66% of participants had quit smoking
this study did not assess a random sample of users and could over-represent more advanced and dedicated consumers.
cohort studies have shown mixed results, with some showing that e-cigarette use increases the odds of quitting while others show the opposite effect
Several cohort studies suffered from very strong bias, such as failure to examine motivation to quit smoking and reasons for using e-cigarettes and no differentiation between regular versus occasional use and experimentation.
Several meta-analyses have also shown mixed results.
Cochrane reviews reported that e-cigarettes help smokers to quit
However, both analyses indicated that the confidence in the result was rated ‘low’ by GRADE standards due to the small number of trials, low event rates and wide confidence intervals around the estimated means
systematic review found that e-cigarette use was associated with 28% reduced chances of quitting
there were major problems in the studies that were included to the analyses
the 2 RCTs used outdated and poor-quality products that were already withdrawn and replaced by more advanced products at the time of the studies’ publication
classical implementation of randomized controlled trials, using a single product and evaluating the effects compared to placebo, is largely inapplicable to e-cigarette research
Many studies included subjects who had already failed to quit smoking with e-cigs at baseline, resulting in bias of the outcome being present at the start of the study
Population studies
In the European Union, an estimated 6.1 million smokers have managed to quit with the help of e-cigs, while an additional 9.2 million smokers have reduced their smoking consumption
Reported smoking cessation and reduction rates were by far higher when current and daily e-cigarette use was assessed separately from ever-use, which emphasizes the importance of differentiating between experimentation and regular use
A cross-sectional survey assessing use of e-cigarettes as part of a quit attempt found that their use was associated with 60% higher odds of quitting compared to pharmaceutical nicotine products
cross-sectional studies also have serious limitations, such as the lack of temporal association and causality, self-report bias and no objective assessment of the smoking status or the duration of smoking cessation
Also, these studies fail to explore how many would have stopped anyway and how many would have stopped had they used another method.
E-cig use by population subgroups
In the UK in 2017, only 2–3% of current adult users report being never-smokers, with the proportion remaining stable between 2012 to 2017 despite the increased awareness and popularity of e-cigarettes over this period
n the European Union, although 2.3% of never-smokers reported ever e-cigarette use, current use was limited to 0.2%.
Current or past daily nicotine use was confined to 0.09% of never-smokers, while current daily nicotine use was even more infrequent (0.04%)
Daily use was also rare in both never-smokers and former smokers who had quit more than 4 years ago.
Several studies raised the issue of accurately defining regular e-cigarette use
A detailed analysis of frequency of e-cigarette use among ‘current’ users (defined as any past 30-day use) identified that this definition includes a lot of infrequent users, including 89.5% of never-smoking past 30-day e-cigarette users
Dual use:
In Europe in 2014, more than 53% of current daily e-cigarette users were dual users
The PATH study in the US found that, among adult tobacco users, the prevalence of multiple product use was 37.8%, with 69.7% of current e-cigarette users being current smokers
Dual use of tobacco and e-cigarettes is a vague definition with a large variety of different patterns of use
For example, both an occasional e-cigarette user who takes a few e-cigarette puffs per week and smokes daily, and a daily e-cigarette user who also smokes but reduced tobacco cigarette consumption from 20 to 2 cigarettes per day are considered dual users
but the health-risk profile of these people is substantially different
Dual use is unlikely to increase harm since e-cigarette use represents an alternative source for smokers to obtain the nicotine they need; thus, no added exposure is expected.
Studies on biomarkers of exposure have shown that dual use is associated with either no increase or reduction in toxin exposure, depending on the level of smoking reduction
In terms of effects on smoking cessation, dual use represents an expected transition period, which could lead to smoking cessation, although frequently dual users abandon e-cigarette use because they find them unsatisfactory as smoking substitutes
However, long-term dual use is associated with higher quit attempt rates and cessation rates.
Additionally, frequent e-cigarette use is associated with reduced rates of dual use
Use by adolescence
In late 2016, the Surgeon General published a report about e-cigarette use among youth and young adults, presenting an explosive rise in ever-use from 2011 to 2016 and declaring this to be a major public health concern.
It is accurate that ever and current (past 30-day) e-cigarette use have increased over the past few years among US youth.
Use of nicotine with e-cigarettes is expected to increase the likelihood of dependence in non-smokers, while use by the latter determines if e-cigarettes are recruiting new users to an inhalational habit and nicotine intake
An analysis of the NYTS 2014 found that the majority of past 30-day e-cigarette users were ever-users of tobacco products, while less than 0.1% of tobacco never-users had used e-cigarettes for 10 or more days in the past month
That study also presented the issue of poly-tobacco use among youth, which has also been detected in an analysis of the MTF 2014
Is it a gateway?
Several studies have shown that e-cigarette use at baseline predicted tobacco cigarette use at follow up
A meta-analysis estimated that e-cigarette use at baseline was associated with 3–4-fold higher odds of subsequent tobacco cigarette use
The studies and subsequent meta-analysis provide sufficient and worrying evidence that there is a temporal transition from e-cigarette to tobacco cigarette experimentation among never-smoking adolescents
a reverse temporal association has also been established
Leventhal and colleagues found that baseline ever-use of a combustible tobacco product was positively associated with e-cigarette use at both 6- and 12-month follow up
e-cigarettes seem to have both a ‘cause’ and an ‘effect’ role depending on the population studied
use of e-cigarettes ‘cause’ use of conventional cigarettes, but also use of conventional cigarettes ‘causes’ use of e-cigarettes
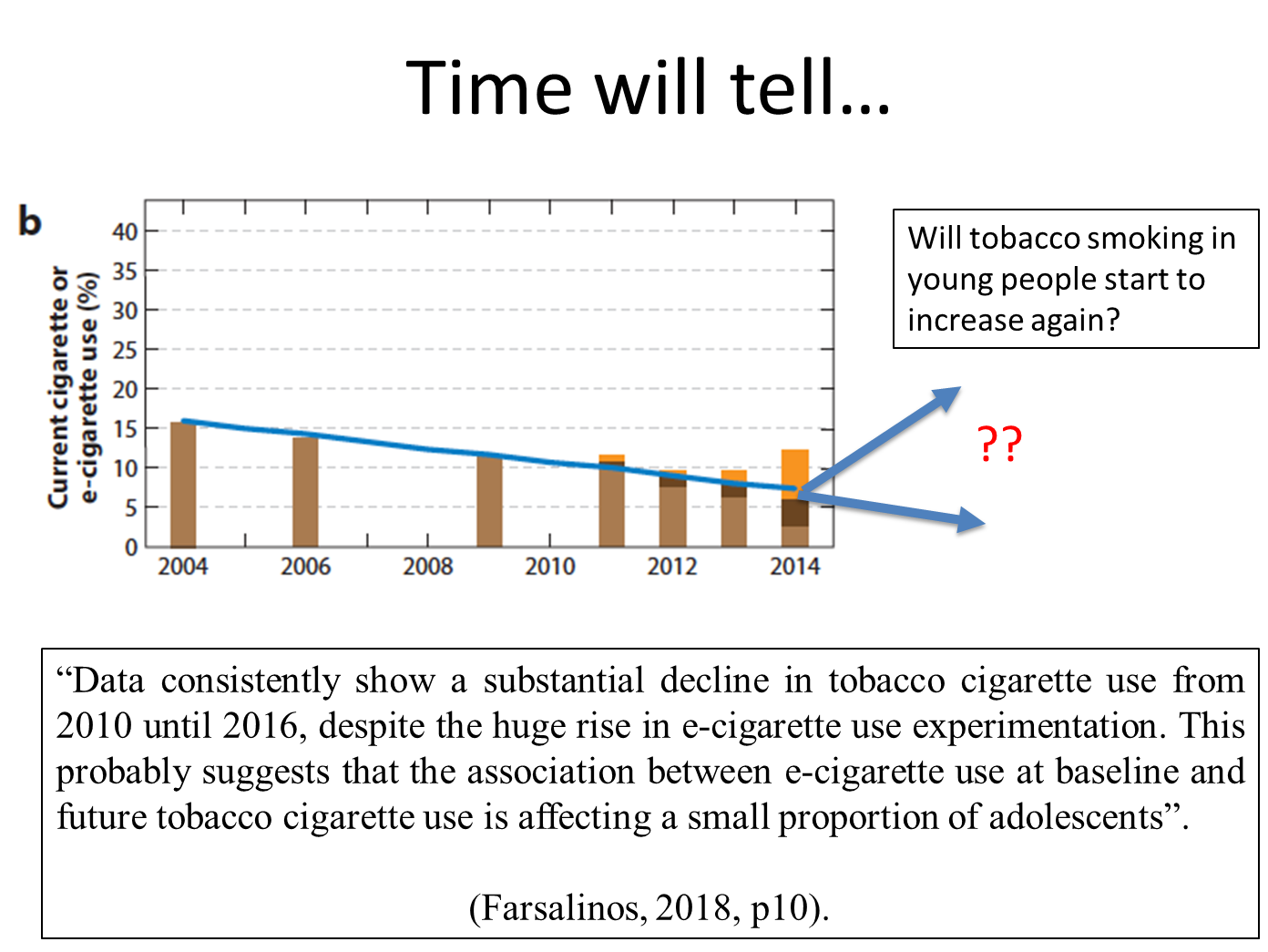
the most crucial factor for public health is the prevalence of smoking, especially regular smoking, in adolescents.
Data consistently show a substantial decline in tobacco cigarette use from 2010 until 2016, despite the huge rise in e-cigarette use experimentation
Reading: E-cigarettes: use, effects on smoking, risks and policy implications
why people use e-cigs:
not subject to the same marketing and promotion restrictions that apply to cigarettes
as a result, e-cig companies are permitted to advertise on television and in mass media as well as through the internet
US e-cigarette marketing expenditures increased from $3.6 million in 2010 to $125 million in 2014
which translated into rapid increases in youth e-cigarette use
Marketing messages echo well-established cigarette themes, including freedom, good taste, romance, sexuality, and sociability as well as messages claiming that e-cigarettes are healthy, are useful for smoking cessation, and can be used in smokefree environments
These messages are mirrored in the reasons that adults and youth cite for using e-cigarettes
Adults:
aid to smoking cessation
safer alt to convention cigs
a way to conveniently get past smokefree laws
most are actually dual users, in 2014 in the US, 93% of e-cig users continued to smoke cigs, 83% in France and 60% in the UK
Youth
attracted the the objects novelty
perception they are harmless/ less harmful than cigs
the thousands of flavours
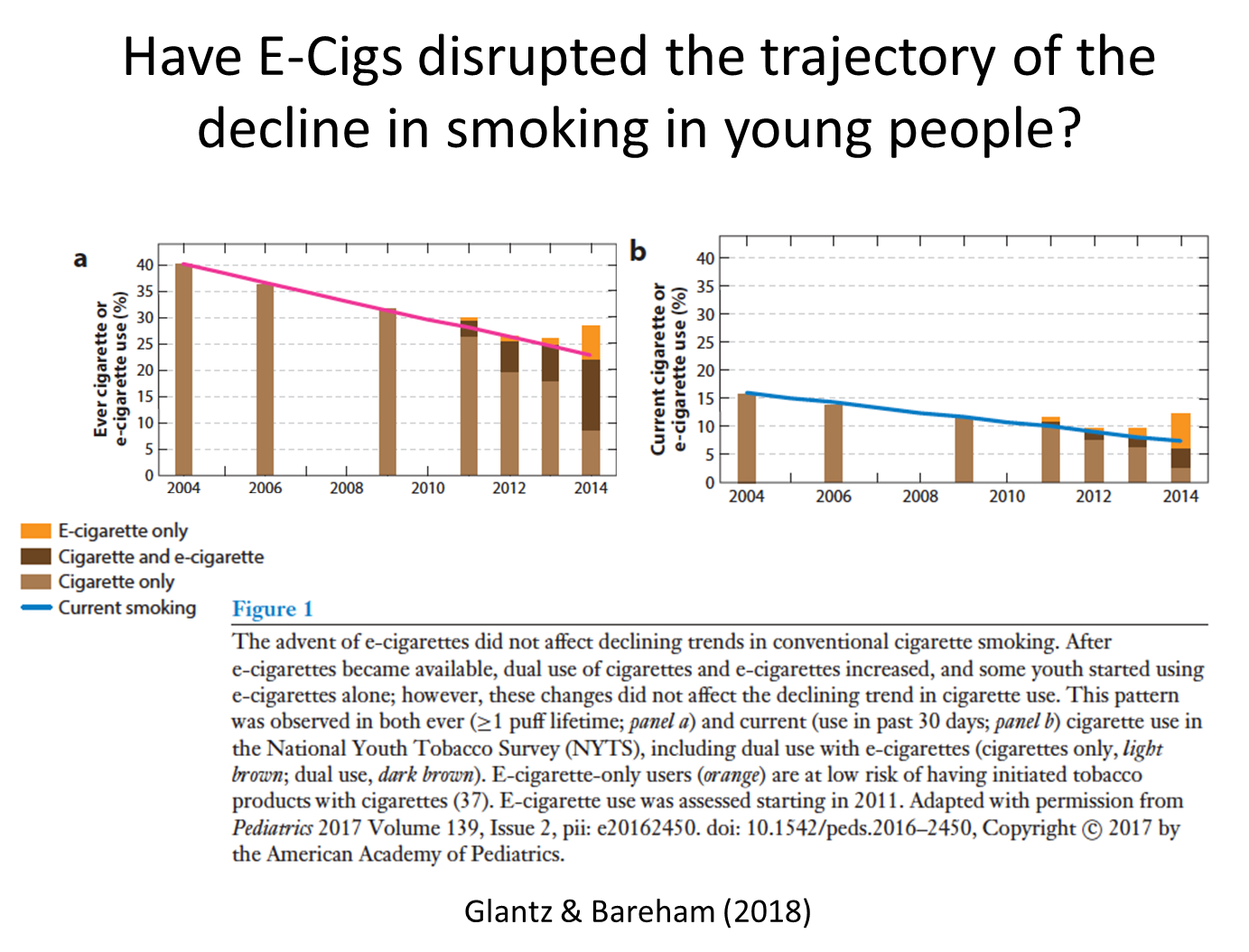
As a result, youth e-cigarette use in the United States doubled or tripled every year between 2011 and 2014, and by 2014, e-cigarette use had surpassed conventional cigarette use in youth.
At the same time that e-cigarette use was increasing, cigarette smoking among youth declined (9, 68), leading some to suggest that e-cigarettes were replacing conventional cigarettes among youth (1, 80, 130) and are contributing to declines in youth smoking. At least through 2014, however, e-cigarettes had no detectable effect on the decline in cigarette smoking among US adolescents (37).
Where as most of the youth who reported smoking cigs in the past 30 days(including dual users of cigarettes and e-cigarettes) in 2011–2014 have demographic and behavioural risk profiles (based on 2004–2009 data) consistent with smoking cigarettes, the risk profiles of the remaining e-cigarette-only users (about 25%ofe-cigarette users) suggested that these individuals would have been unlikely to have initiated tobacco product use with cigarettes (37).
These national results are consistent with regional US studies that also found that e-cig-only users display a lower risk profile than do cigarette smokers for smoking cigarettes (14, 24, 93, 143).
Consistent with this is that, in 2015, in the United States, 40% of 18–24-year-old current e-cigarette users had never smoked conventional cigarettes (27). This rapid increase in e-cigarette-only use among youth and young adults is of concern because youth are more susceptible to developing nicotine dependence than are adults (136). In addition, nicotine has adverse effects on brain development, including that of developing fetuses (41, 134, 136).
e-cigs as a gateway
current cigarette smokers who had ever used e-cigarettes were more likely to intend to quit smoking within the next year but were less likely to have stopped smoking
The same US study found that e-cig use was associated with progression from experimentation with cigarettes to established smoking. Among cigarette experimenters (youth who had smoked at least 1 puff of a cigarette), ever e-cig use was associated with higher odds of becoming an established smoker and with current cigarette smoking
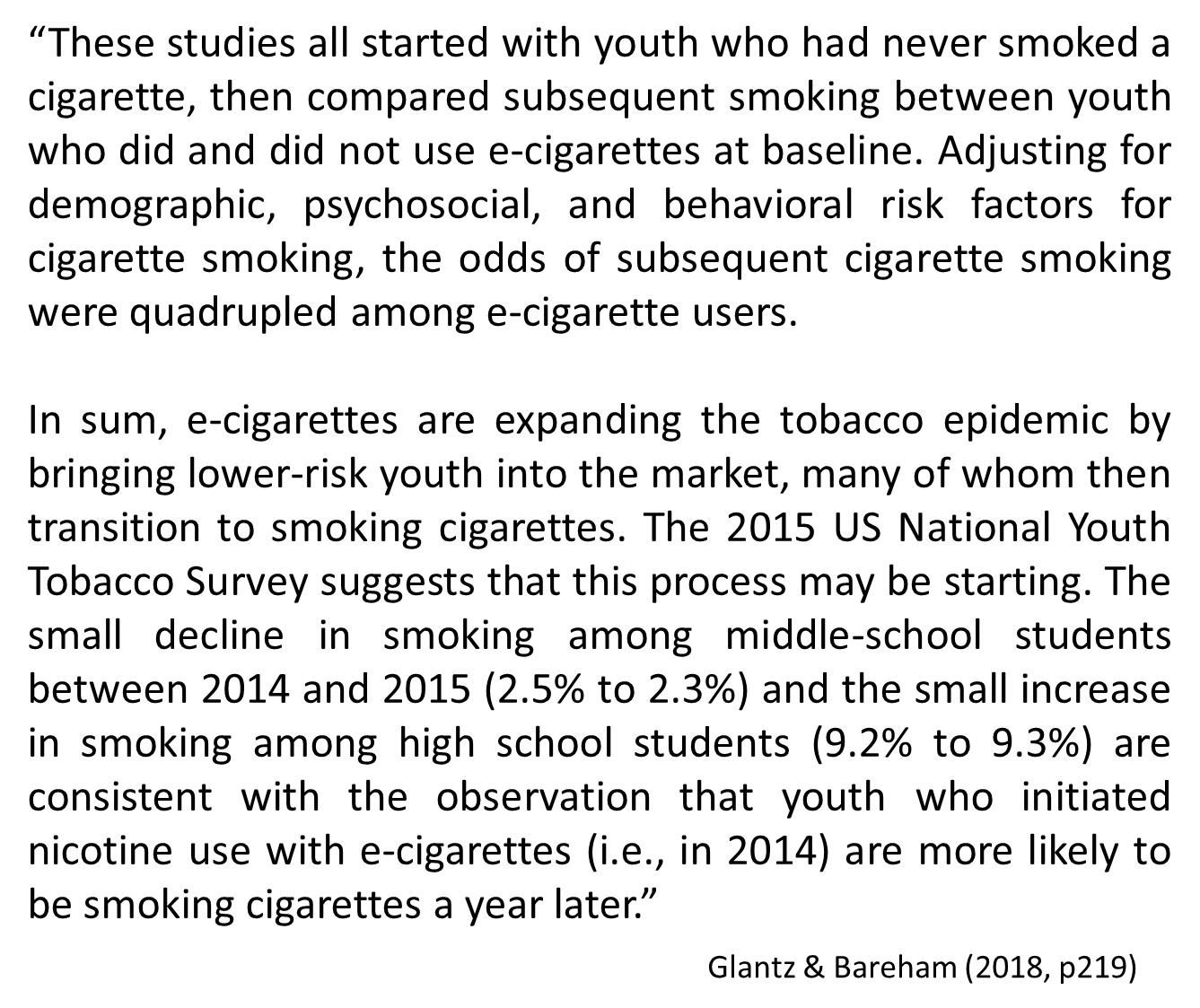
e-cigs are expanding the tobacco epidemic by bringing lower-risk youth into the market, many of whom then transition to smoking cigarettes.
The 2015 US National Youth Tobacco Survey suggests that this process may be starting. The small decline in smoking among middle-school students between 2014 and 2015 (2.5% to 2.3%) and the small increase in smoking among high school students (9.2% to 9.3%) are consistent with the observation that youth who initiated nicotine use with e-cigarettes (i.e., in 2014) are more likely to be smoking cigarettes a year later.
E-cigs and smoking cessation
Unlike nicotine replacement therapy, e-cigs are mass-marketed recreational consumer products; they are not medicine developed to be administered under clinical supervision
should their effects be assessed only among people who are actively using them as part of a smoking cessation attempt or on all smokers who use them regardless of motivation.
This situation is further complicated because a major reason that smokers use e-cigarettes is to continue inhaling nicotine in locations where conventional cig smoking is prohibited
Smokefree environments both motivate and support quit attempts
By potentially dulling the effects of smokefree environments, the real-world use of e-cigarettes could reduce quit attempts and keep people smoking
As more jurisdictions include e-cigs in their smokefree policies and people include them in voluntary smokefree home rules, this effect will likely be diminished.
Most research on the relationship between the use of e-cigs and quitting are from observational studies that compare cigarette use among smokers who use e-cigs with smokers who do not use e-cigs
it does not support the same kind of causal conclusions that an experimental study (i.e., a RCT) would
this approach has the advantage of quantifying the effects of e-cigarettes as actually used, including any indirect effects, such as discouraging cessation attempts
An analysis of 8 cohort observational studies suggested a possible reduction in quit rates with the use of e-cigarettes compared with no use of e-cigarettes
One study (19) found that inter mittent e-cigarette users (more than once or twice but less than daily use) were less likely to quit smoking one year later than none-cigarette users, but those who had used e-cigarettes daily for at least one month were significantly more likely to quit cigarettes
Another study (63) found that all “cig-alike” users and nondaily tank system users had lower odds of quitting cigarettes, whereas daily tank system users were significantly more likely to quit
The third study (151) found that short-term e-cig use was not associated with a lower rate of smoking cessation, but long-term use was
The fourth study (147) found higher quitting smokers specifically using e cigarettes as part of a quit attempt in countries with permissive e-cigarette policies (United States and United Kingdom) than those in countries with restrictive policies (Canada and Australia)
In contrast, in the European Union (including Great Britain, specifically), a study of the relationship between e-cigarette use and having stopped smoking found less quitting among smokers who used e-cigarettes
As of June 2017, there was only one prospective RCT of people using e-cigs to quit smoking. This trial compared giving patients nicotine and non-nicotine e-cigarettes with giving them a voucher for nicotine replacement therapy (NRT).
There was no significant difference in efficacy compared with nicotine patches; both patches and e-cigarettes showed low efficacy. At 6 months, verified abstinence was 7.3% with nicotine e-cigarettes, 5.8% amongthose offered NRT, and 4.1% for those with non-nicotine e-cigarettes.
However, because participants were handed the e-cigarettes and only given a voucher for NRT, these results likely overstated the efficacy of e-cigarettes and understated the efficacy of well-managed NRT.
Another randomized trial (25) that compared nicotine and non-nicotine e-cigarettes found no consistent difference in smoking cessation.
This study did not have a control group of smokers not using e-cigarettes, so it does not provide any information about the effects of e-cigarette use per se on smoking cessation.
Cancer
e-cigs deliver lower levels of carcinogens than conventional cigs
lower levels of carcinogens are found in the bodies of e-cig users than in smokers
this suggest that e-cigs are likely less carcinogenic than conventional cigarettes, however, they do deliver carcinogens that can have effects at very low levels following repeat exposures
E-cigarettes deliver the tobacco-specific nitrosamine and potent lung carcinogen NNK [4-(N-methyl-N-nitrosoamino)-1-(3-pyridyl)-1-butanone, also known as nicotine-derived nitrosamine ketone]
Some evidence indicates that the NNK dose-response curve for cancer is highly nonlinear, with substantial increases in risk at low doses
Known bladder carcinogens have been detected in the urine of e-cigarette users but not in nonusers
In addition, while nicotine is not a carcinogen, it does promote the growth of blood vessels that supply tumors and it speeds tumor growth
Cardiovascular disease
nicotine’s role in this remains debated
e-cigarettes work by creating an aerosol of ultrafine particles to carry nicotine deep into the lungs. These particles are as small as—and sometimes smaller than—those in conventional cigarettes
These ultra fine particles are themselves biologically active, trigger inflammatory processes, and are directly implicated in causing cardiovascular disease and acute cardiovascular events
The dose-response effect for exposure to particles is nonlinear, with substantial increases in cardiovascular risk with even low levels of exposure to ultrafine particles
For example, exposure to second hand cigarette smoke has nearly as large an effect on many risk factors for cardiovascular disease and the risk of acute myocardial infarction as does being an active smoke
e-cigarette users experience increased oxidative stress and increases in the release of inflammatory mediators
E-cigarette aerosol also induces platelet activation, aggregation, and adhesion.
All these changes are associated with an increased risk of cardiovascular disease.
These physiological changes are manifest in rapid deterioration of vascular function following use of e-cigarettes
E-cigarette and traditional cigarette smoking in healthy individuals with no known cardiovascular disease exhibit similar inhibition of the ability of arteries to dilate in response to the need for more blood flow
This change reflects damage to the lining of the arteries (the vascular endothelium), which increases both the risk of long-term heart disease and an acute event such as a myocardial infarction
Using e-cigarettes is also accompanied by a shift in balance of the autonomic (reflex) nervous system toward sympathetic predominance (26, 92), which is also associated with increased cardiac risk
The biological stresses that e-cigarette use imposes on the cardiovascular system are manifest as an increase in risk of acute myocardial infarction
A cross-sectional analysis of data in the US 2014 and 2016 National Health Interview Surveys revealed that daily e-cigarette use was associated with increased odds of having suffered a myocardial infarction
the effect of using e-cigarettes on the odds of myocardial infarction approached what was found with conventional cigarette smoking
Lung disease
As with cardiovascular disease, evidence consistently indicates that exposure to e-cigarette aerosol has adverse effects on lungs and pulmonary function. Repeated exposure to acrolein, which is produced by heating the propylene glycol and glycerin in e-liquids, causes chronic pulmonary inflammation, reduction of host defence, neutrophil inflammation, mucus hypersecretion, and protease-mediated lung tissue damage, which are linked to the development of chronic obstructive pulmonary disease. E-cig aerosol also exposes users to highly oxidizing free radicals. Animal studies have also shown that e-cigarettes increase pulmonary inflammation and oxidative stress while inhibiting the immune system. Consistent with these experimental results, people who used e-cigs experienced decreased expression of immune-related genes in their nasal cavities, with more genes suppressed than among cigarette smokers, indicating immune suppression in the nasal mucosa. E-cigarette use upregulates expression of platelet-activating factor receptor (PAFR) in users’ nasal epithelial cells; PAFR is an important molecule involved in the ability of S.pneumoniae, the leading cause of bacterial pneumonia, to attach to cells it infects (adherence). In light of the immunosuppressive effects observed in nasal mucosa, there is concern that e-cigarette use will predispose users toward more severe respiratory infections, as has been demonstrated in mouse studies. Given these effects, it is not surprising that e-cigarette use is associated with a doubling of the risk of symptoms of chronic bronchitis among US high school juniors and seniors with higher risk associated with higher use; these risks persisted among former users. Similarly, current e-cigarette use was associated with an increased diagnosis of asthma among Korean high school students (among current e cigarette users who were never cigarette smokers). E-cigarette users were also more likely to have had days absent from school due to severe asthma symptoms.
Use of e-cigs in smokefree environments:
Policy issues: