touch
stimuli: mechanical pressure
receptors: a number of different types of receptors in the skin
actually responding on how the world impacts your skin
active vs passive touch: when investigating object w touch we actively move our hands over it, perception is an active process
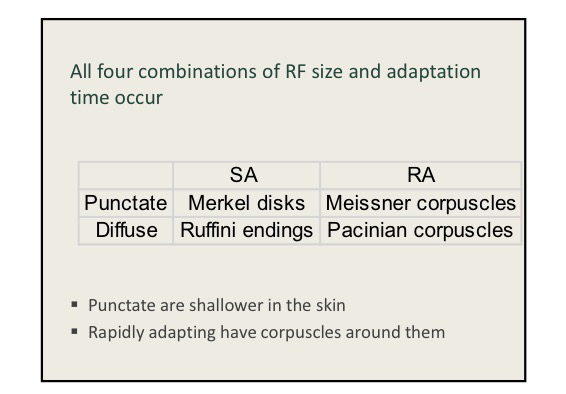
receptors have different rates of adaptation
SA - slowly adapting fibers
RA - rapidly adapting fibers
receptors have different sized receptive fields
punctate fibers - have small RFs, sharp borders
diffuse fibers - large RFs, fuzzy borders
somatosensory and motor cortex:
output: motor cortex (left hemisphere section controls the body’s right side)
input: sensory cortex (left hemisphere section receives input from the body’s right side)
how do we know where our limbs are in space?
out flow theory - no
joint receptors (tendon organs) - a little
cutaneous receptors (responding to the stretching of skin) - a little
muscle spindles - yes
pain receptors: nociceptors
free nerve endings - 4 types
mechanical pain
thermal: hot
thermal: cold
polymodal (any noxious high intensity stim)
hot and cold don’t overlap
cold also responds to very hot…so an isolated very hot stimulus may seem cold
nociceptors: specialized receptors for pain (noxious stimuli)
thermal and mechanical nociceptors
separate class for each type of stimulus but only respond to high stimulus
thinly myelinated (slower than normal touch, faster than polymodal)
associated w sharp/pricking pain
polymodal nociceptors
respond to any high intensity noxious stimulus (pressure, temp, chemicals)
no myelination (relatively slow; could take 1-3 sec to feel pain from your toe)
associated w dull aching/burning pain
transduction? dont know but we think each type of noxious stimulus has a distinct method - can change the threshold to one type of stimuli without effecting threshold of another
hyperalgia: when burn hurts again in warm shower, pain doesn’t adapt
when tissue gets damaged blood vessels leak and damaged tissue releases chemicals which produce inflammation
histamine directly excited nociceptors
prostaglandin lowers threshold of nociceptors
referred pain: pain receptors on organs, share spinal pathway w pain receptors on skin
pain is multimodal: sensation - connection to somatosensory cortex, insula, and anterior cingulate cortex
emotional reaction and drive - connections between pain and the hypothalamus and limbic system
watching someone else get hurt and social rejection both activate pain
pain control:
NSAIDs (aspirin) - block production of prostaglandin - mostly peripheral effects
opioids - bind to opioid receptors in CNS
inhibit glutamate and substance P in spinal cord
hyperpolize pain cells makes them less likely to find, also impacts throughout the brain
Gate theory of pain: stimulation of touch can block pain signals - inhibition within the spinal cord - top down control
analgesia based on gate control theory
rubbing painful spot
acupressure
transcutaneous electrical nerve stimulation
placebo effect has 25-33% reduction in pain
naloxone (no reduction) - blocks endorphins from binding, suggests placebo effect works by producing release of endorphins
mood effects - angry people (opioid issues) have lower thresholds