Heart Failure Presentation and Investigation
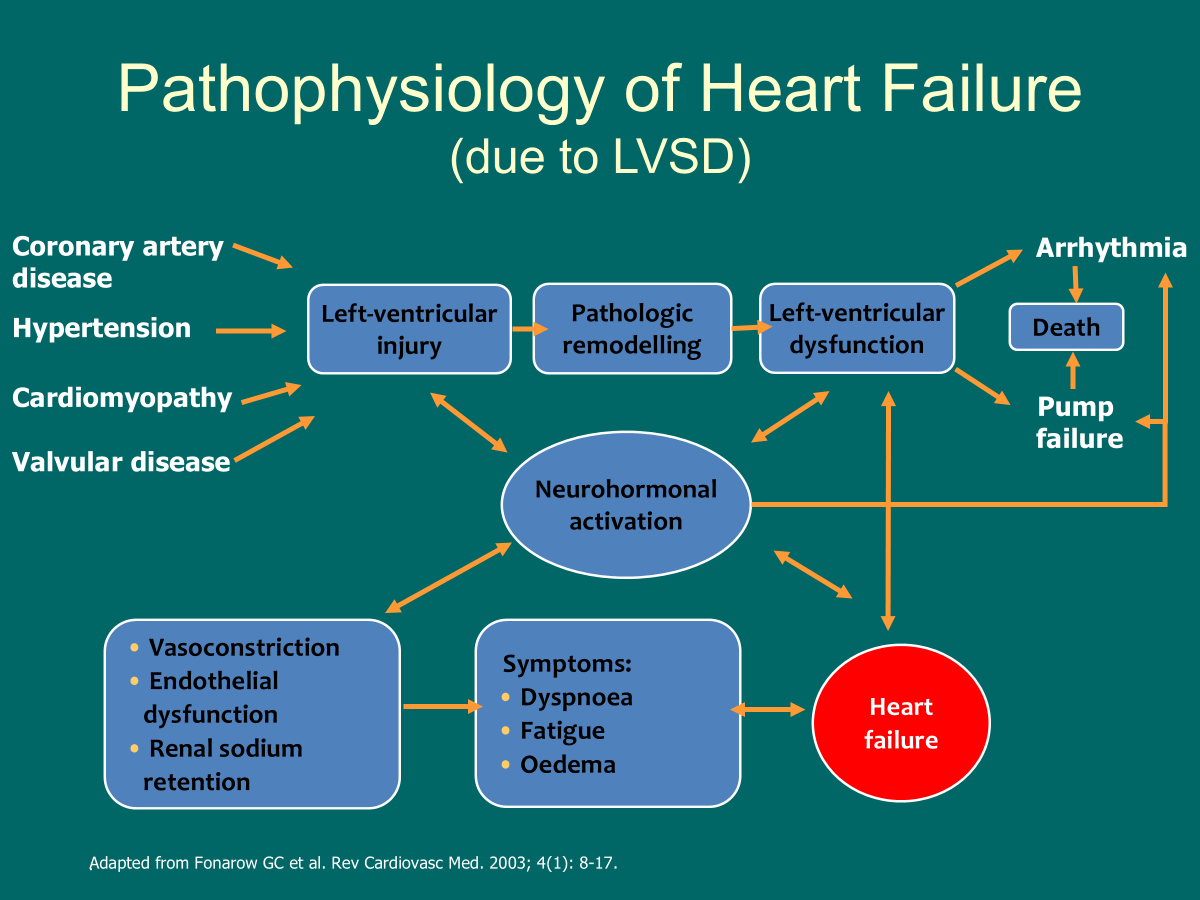
heart failure defined as a clinical syndrome comprising of dyspnoea, fatigue or fluid retention due to cardiac dysfunction, either at rest or on exertion, with accompanying neurohormonal activation
relatively common, increasing, more common in elderly
biggest cost is in hospital stay
up to two weeks admission time
primarily admitted due to acute breathlessness, peripheral oedema
high re-admission rate, happen early in the first week
high morbidity and mortality
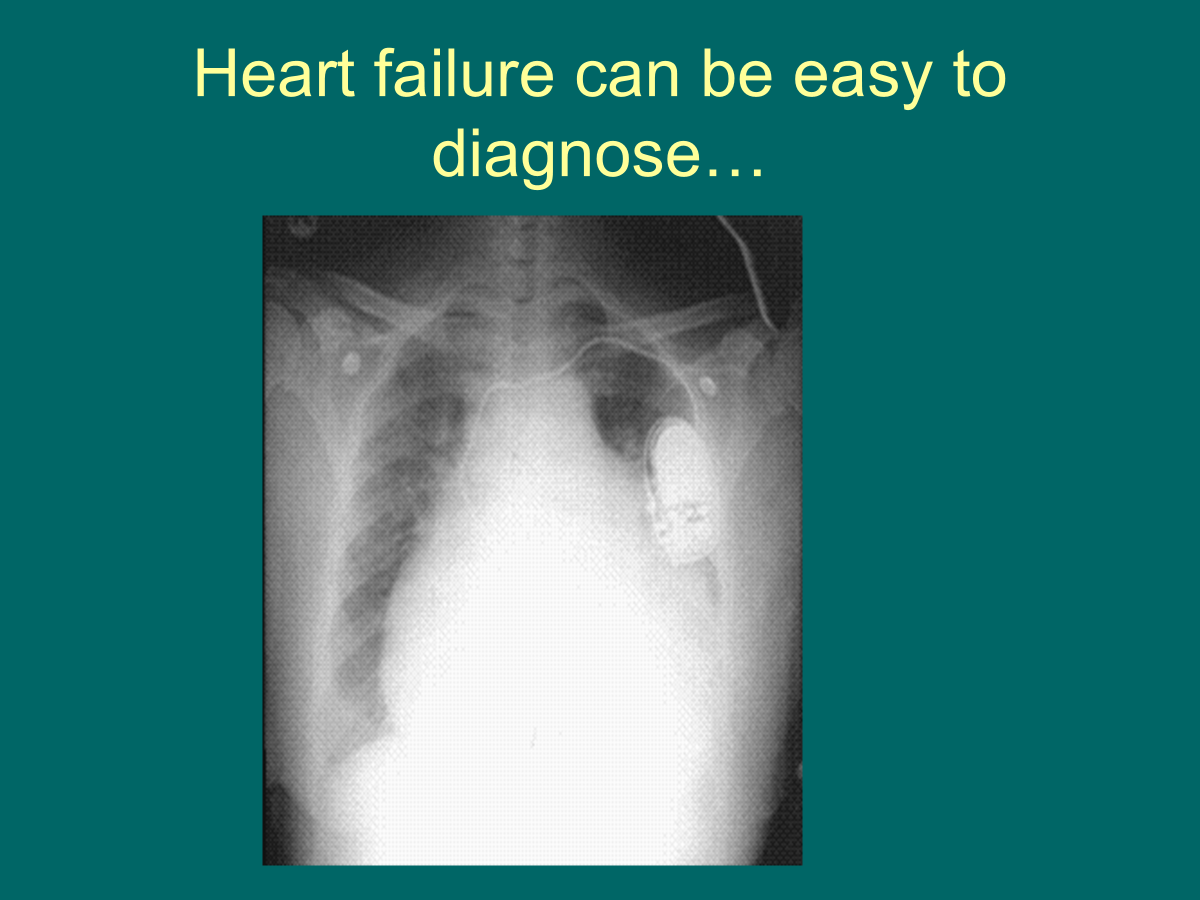
massively enlarged heart, congested lungs- easily diagnose heart failure
objective evidence of cardiac dysfunction mandatory
-echocardiography *main, radionuclide ventriculography, MRI, left ventriculography
potential screening tests - 12 lead ECG
-BNP, peptide rises when heart in stress or strain, if BNP is low heart failure unlikely, if BNP moderate or high heart failure more likely
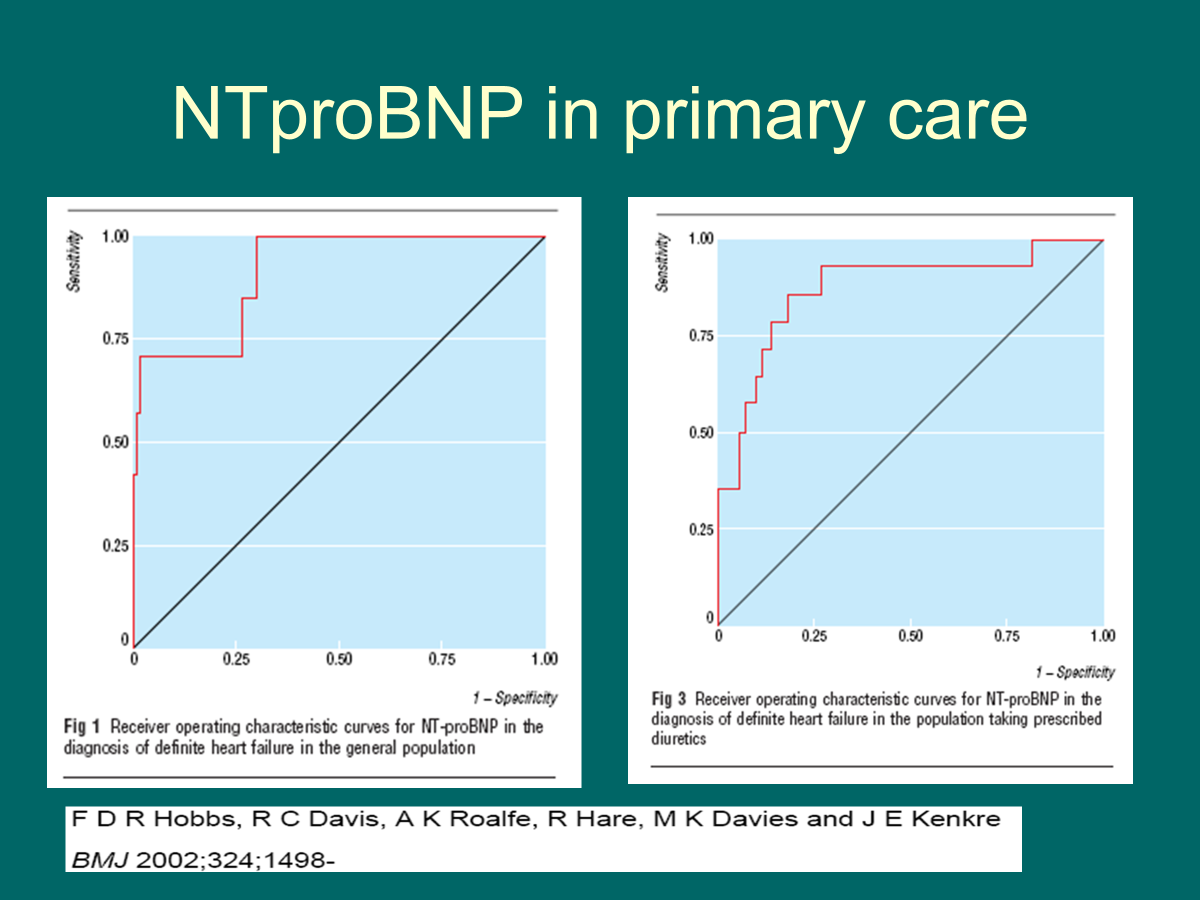
looking for high sensitivity
sensitivity of 1 and specificity of 1 preferable
larger area under curve, more accurate the test is as a diagnostic test
BNP predicts mortality and morbidity
if sufficiently severe almost any structural cardiac abnormality will cause heart failure
take a detailed history to evaluate patients if they have Left ventricular systolic dysfunction, as they are many causes the detailed history should make more causes more likely than others
always ECG, sometimes CXR, ECHO
consider coronary angiography if chest pain, not really for those >70
LV ejection fraction is a continuous biological variable
–Disease / physiological changes can both decrease and increase the LVEF
–The LVEF may be lower than previous but not pathologically low
–Analagous to Haemoglobin / anaemia
•eg. fall in Hb from 17g/dL to 14.5g/dL
LV function assessment and LVEF
normal 55-70%
mild 40-55%
moderate 30-40%
severe <30%
Cardiac MRI has better image quality
more impaired left ventricular function, worse prognosis
grading the severity of HF:
-degree of LV impairment
-NYHA class i.e. severity of symptoms
-degree of elevation of BNP
heart failure does not equal reduced cardiac output (at rest)
angiotensin receptor and neprolysin inhibitor -pharmacological therapy, same sort of effect as ACE inhibitor
neprolysin blocks the breakdown of BNP