Module 4: Endocrinology
Lecture 1: Endocrine Lecture
1. What the Endocrine System Is
Endocrine system = hormone‑based control system.
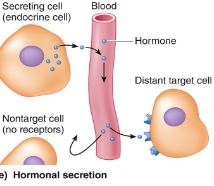
Hormones are cell signaling molecules secreted by endocrine cells → travel via blood → act on distant target cells that express specific receptors.
Specificity comes from receptor expression, not hormone distribution.
→ specify = which means that cells can express the receptors (that’s correct) for a specific hormone to take effect
“Hormones travel everywhere… what gives specificity… is whether cells express the receptor for that hormone.”
2. Modern View of Endocrinology
Historically: focus on classic endocrine glands (pituitary, thyroid, adrenal).
Now: many tissues are recognized as endocrine, e.g. GIT, heart, adipose tissue, bone.
“We used to think… the heart didn’t produce hormones, now we know it does… fat produces hormones… bone produces signalling molecules.”
Endocrinology is now understood as cell‑to‑cell communication, not just “glands”.
3. Types of Cell Communication
Local (short range)
Juxtracrine – direct contact (adhesion molecules, gap junctions).
Autocrine – acts on same cell.
Paracrine – acts on nearby cells.
How does juxtracrine differ from paracrine?
Juxtracrine requires direct physical contact between adjacent cells, while paracrine relies on the release of chemical signals into the extracellular space
Long‑distance
Endocrine – hormones in blood.
Nervous system – neurotransmitters.
Neuroendocrine – neurons release hormones into blood.
“Neurons release hormones… neurohormones… travel in blood to distant targets.”
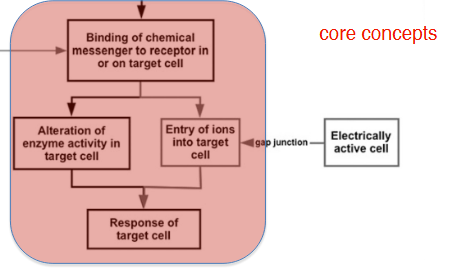
4. Core Concepts in Cell Signalling
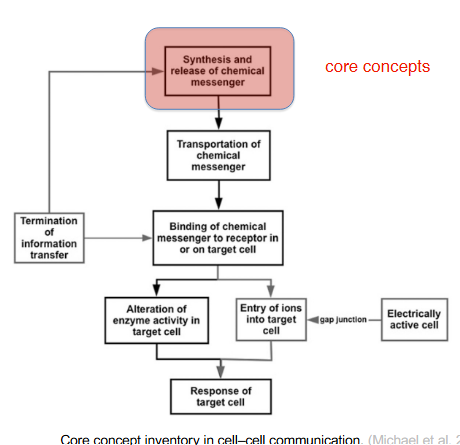
The lecture uses the “core concept inventory” diagram to emphasise:
Synthesis & release of messenger
Transport
Binding to receptor
Signal transduction
Cellular response
Termination of information transfer
These steps apply to all chemical messengers.
5. Chemical Classes of Messengers
Cell synthesizes and release a chemical messenger → and they are either stored in vesicle or escape via diffusion
Messenger molecules include:
Peptides / polypeptides / proteins
Steroids
Amines (catecholamines, indoleamines)
Lipids
DNA, RNA, metabolites (modern expansion)
“When I learnt endocrinology, I didn’t learn that DNA and RNA… could be chemical messengers.”
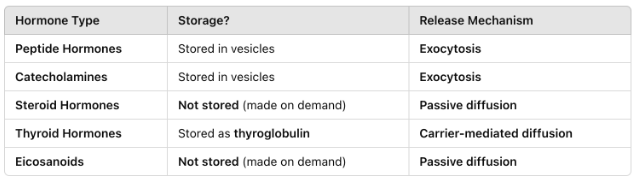
6. Storage & Secretion
Stored in vesicles → released by exocytosis
Peptide hormones
Catecholamines
Not stored → diffuse out immediately
Steroid hormones
Eicosanoids
Special case
Thyroid hormones stored as thyroglobulin; released via carrier‑mediated diffusion.
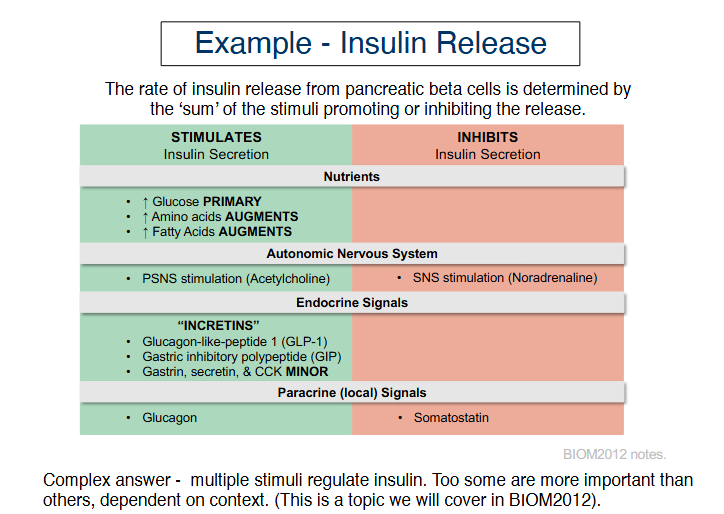
7. Key Concept: Secretion = SUM of Stimuli
Hormone release is determined by net stimulatory vs inhibitory inputs, not a single trigger.
“It’s the sum of all the stimulatory and inhibitory factors… exactly like summation in neurons.”
Example: Insulin secretion
Core concept: Transportation of chemical messenger
Transport depends on solubility:
Hydrophilic messenger (peptides, catecholamines)
they dissolve easily in aqueous solution
Travel freely in plasma
Sometimes they still bind to:
Binding proteins → to protect them from being broken down too quickly
Exosomes → tiny membrane vesicles that can carry signalling molecules
Hydrophobic messenger (steroids, thyroid hormones)
Travel bound to plasma proteins
if travelling on its own clump together or get stuck to membrane)
So they must travel with carrier proteins, such as:
Binding proteins
Plasma proteins (e.g., albumin)
“Most circulate bound… only the free fraction can bind to receptors.”
9. Plasma Hormone Levels = Balance of 4 Processes
Secretion
Activation (some hormones secreted inactive → require cleavage)
Binding to plasma proteins (lipophilic hormones)
Inactivation & excretion (liver metabolism, renal excretion)
“Circulating hormones are the balance of secretion and metabolism… some require cleavage to become active.”
Sensitivity of Target Cells
Sensitivity depends on:
Number of receptors
Receptor affinity
Downstream signalling capacity
This determines how strongly a cell responds to a given hormone concentration.
11. Receptors & Signal Transduction
Hormones bind to receptors on or inside cells.
Receptor types mentioned
GPCRs (oxytocin, GHRH, somatostatin, dopamine)
Tyrosine kinase receptors (insulin, IGF‑1)
Cytokine receptors (prolactin, GH, leptin, EPO)
Steroid receptors (oestrogen)
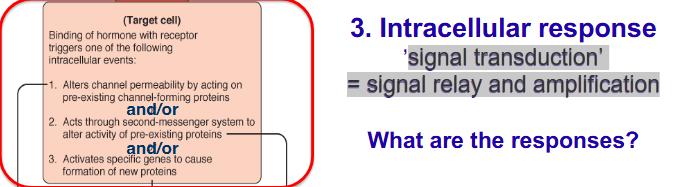
12. Intracellular Responses
Signal transduction = signal relay and amplification
Hormone binding can cause:
Altered ion permeability (very fast)
Activation of enzymes/proteins (fast)
Gene expression changes (slow)
Second messengers (e.g., cAMP) allow rapid amplification.
“Second messengers are transient… allow rapid amplification.”
13. Signal Amplification
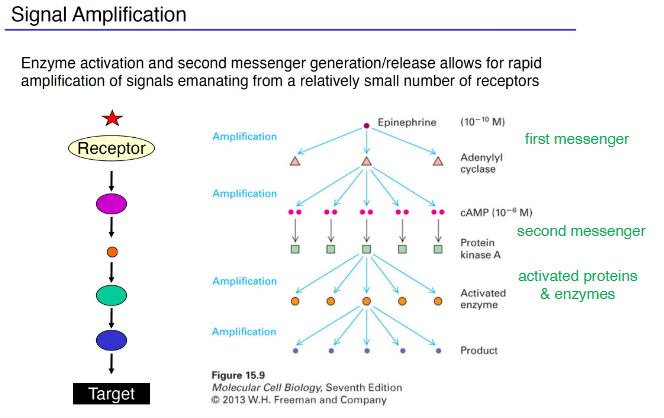
Small hormone concentration → large cellular response.
Example from lecture:
Epinephrine (10⁻¹⁰ M) → cAMP (10⁻⁶ M) → massive enzyme activation.
14. Summary of Key Principles
Hormones are chemical messengers for long‑distance communication.
Only free hormone is biologically active.
Hormone levels reflect secretion vs metabolism/excretion.
Some hormones require activation after secretion.
Target cell response depends on receptor presence + sensitivity.
Signal transduction pathways determine speed and type of response.
Endocrinology is fundamentally cell‑to‑cell communication.
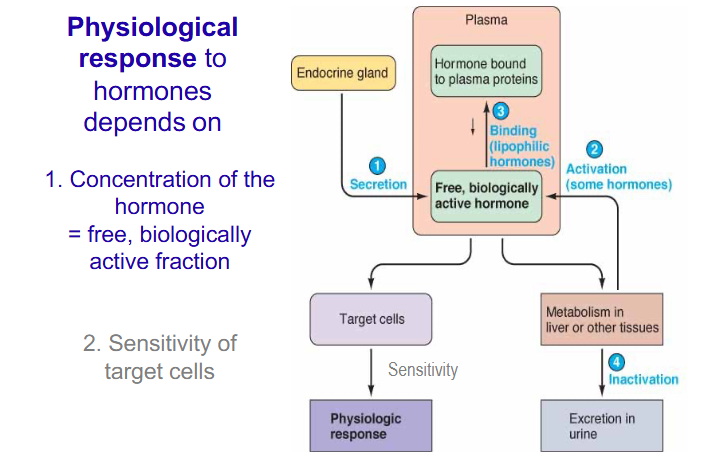
Lecture 2: Physiological response to hormones depends on
Physiological Response Depends On Two Major Factors
1. Concentration of free, biologically active hormone
Determined by:
Secretion from endocrine gland
Activation (some hormones secreted inactive → require cleavage)
Binding to plasma proteins (lipophilic hormones)
Metabolism & inactivation (mainly liver)
Excretion (mainly kidney)
Only free hormone can bind receptors and produce effects.
2. Sensitivity of target cells
Receptor number
Receptor affinity
Integrity of intracellular signalling pathways
2. Hormone Insensitivity (Hormone Resistance)
Cells show reduced physiological response despite normal or high hormone levels.
Example: Type II diabetes (insulin resistance)
Three levels where insensitivity can occur
1. Molecular recognition (ligand binding)
↓ receptor expression
Receptor mutations → poor binding
2. Activation of receptor
Receptor cannot undergo conformational change
GPCR polymorphisms: G protein-coupled receptor polymorphisms is variations in the genetic sequences of genes that code for GPCRs (rare but possible)
3. Intracellular signaling defects
Definitions: when a cell fails to properly process or transmit chemical messages from its surface to its internal machinery
↓ signaling components
↑ inhibitors (e.g., inflammation → inhibitory molecules block insulin signaling)
Multiple defects can coexist simultaneously.
3. Endocrine Diseases: Too Little vs Too Much Hormone Activity
Too little hormone activity
Hyposecretion
Increased clearance (rapid removal)
Tissue insensitivity (common)
Increased plasma protein binding (rare)
Too much hormone activity
Hypersecretion
Reduced clearance (e.g., kidney failure → hormone accumulation)
Reduced plasma protein binding (malnutrition → ↑ free hormone)
Excessive tissue response (rare)
Plasma protein binding: the attachment of chemicals to plasma proteins in the blood
4. Hypothalamus (Part 1) — Structure & Function

Neural tissue + endocrine gland
Contains:
Nuclei (clusters of neuronal cell bodies)
Nerve tracts (axons)
Inputs
Neural (cortex, limbic system)
Humoral (blood‑borne signals: hormones, metabolites, glucose)
Outputs
Neural (autonomic nervous system)
Hormonal (neurohormones)
5. Hypothalamic Roles
Behavioural regulation
Feeding
Reproductive behaviours
Rage
Driven by higher brain centres (cortex, limbic system).
Vegetative (homeostatic) regulation
Automatic, subconscious:
Temperature
Hunger/satiety
Water balance
Stress
Growth
Reproduction
Hypothalamus integrates multiple signals → compares to set‑point → generates coordinated
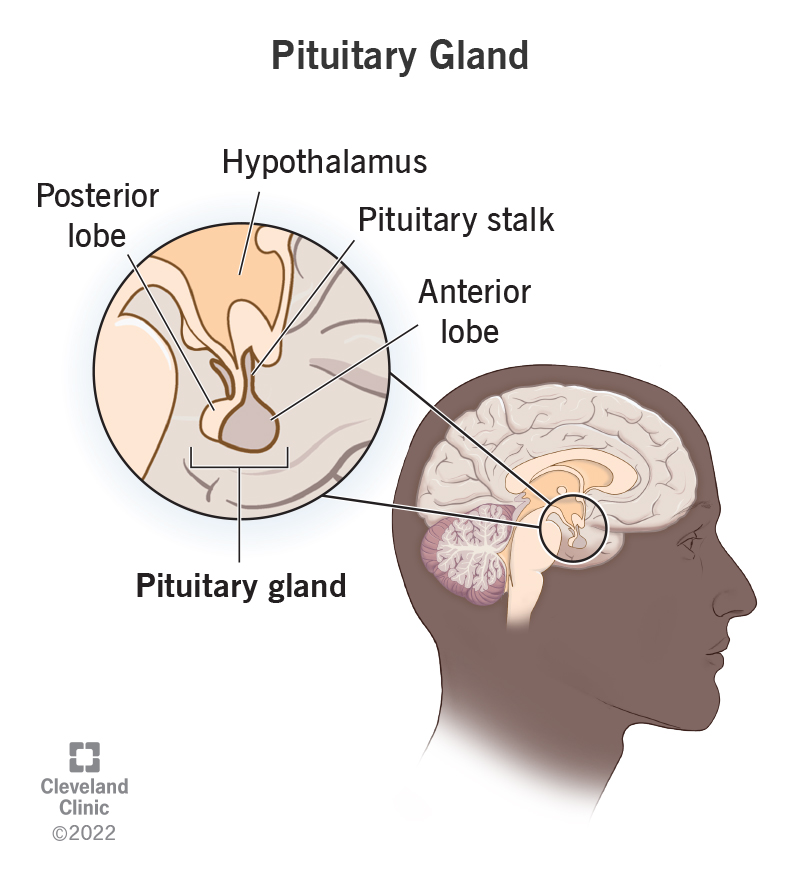
Lecture 3: Pituitary gland
1. Posterior Pituitary Gland
Releases two neurohormones made in the hypothalamus:
1. Vasopressin (AVP / ADH)
Peptide hormone produced in the hypothalamus and released by the pituitary gland. Its two primary functions are regulating the amount of water in the body and constricting blood vessels, which helps control blood pressure
9‑aa peptide
Actions:
↓ water excretion (anti‑diuretic) and keeps water in body (reabsorbing)
Vasoconstriction
Regulated by:
ECF osmolality (osmoreceptors)
Blood volume (stretch receptors)
2. Oxytocin (OT)
a powerful hormone and neuropeptide produced in the hypothalamus and released by the posterior pituitary gland. Known as the "love hormone" or "bonding hormone," it plays a vital role in social connection, reproduction, and childbirth
9‑aa peptide (differs from AVP by 2 residues)
Synthesised in:
Paraventricular nucleus (PVN)
Supraoptic nucleus (SON)
Axons project to posterior pituitary → release OT into blood.
2. Oxytocin — Actions
Smooth muscle contraction during:
Parturition (uterine myometrium) - child birth
Milk ejection (myoepithelial cells)
Stimulated by
Cervical stretch (baby in birth canal)
Suckling
Positive emotional inputs
Inhibited by fear/anxiety
Both are positive feedback loops.
Other roles
CNS neurotransmitter
Bonding, trust, social behaviour
Sexual function (orgasm)
3. Milk Ejection Reflex Sequence:
Suckling → sensory input to hypothalamus
↑ firing of OT neurons
OT released from posterior pituitary
OT → myoepithelial contraction → milk ejection
Emotional state modulates reflex.
4. Oxytocin Signal Transduction
OT receptor = GPCR (Gq)
Activates PLC → PIP₂ → IP₃ + DAG
IP₃ → Ca²⁺ release from ER
Ca²⁺ → myosin phosphorylation → contraction
5. Anterior Pituitary Gland
Contains 5 endocrine cell types:
Cell Type | Hormone |
|---|---|
Somatotrophs | GH (Growth hormone) |
Lactotrophs | PRL (Prolactin) |
Gonadotrophs | LH, FSH (luteinizing hormone) (follicle-stimulating hormone) |
Thyrotrophs | TSH (Thyroid-Stimulating Hormone) |
Corticotrophs | ACTH (adrenocorticotropic Hormone) |
Two functional groups
Tropic/trophic hormones (act on other endocrine glands)
ACTH, TSH, LH, FSH
Direct‑acting hormones
GH, PRL
→ these two are the focus of the other lectures
6. Hypothalamic Control of Anterior Pituitary
the glandular front lobe of the pituitary gland, a pea-sized organ at the base of the brai. Often called the body’s "master gland," it produces and secretes crucial hormones that regulate fundamental processes like growth, metabolism, reproduction, and stress responses.
Small‑bodied neurons release releasing hormones into median eminence
Travel via hypophyseal portal system
Act on anterior pituitary cells
Releasing hormones
GHRH
TRH
CRH
GnRH
Somatostatin (inhibits GH)
Dopamine (inhibits prolactin)
7. Pituitary Stalk Section Experiment
If the hypothalamus is disconnected:
RF = Releasing Factor → A hypothalamic hormone that stimulates pituitary secretion.
RIF = Releasing Inhibitory Factor → A hypothalamic hormone that inhibits pituitary secretion.
Hormone | Releasing factors | Releasing inhibitory factors | Result |
|---|---|---|---|
Prolactin | — | Dopamine | ↑ PRL (loss of inhibition) |
GH | GHRH | — | ↓ GH |
TSH | TRH | — | ↓ TSH |
ACTH | CRH | — | ↓ ACTH |
LH/FSH | GnRH | — | ↓ LH/FSH |
Shows primary regulation by hypothalamic releasing factors.
1. Prolactin
RF? → None (no releasing factor)
RIF? → Dopamine
Dopamine = Prolactin Inhibitory Factor (PIF)
Effect when stalk cut: Prolactin ↑ (loss of inhibition)
2. Growth Hormone (GH)
RF: GHRH = Growth Hormone–Releasing Hormone
RIF: Somatostatin (also called GHIH = Growth Hormone–Inhibiting Hormone)
Effect when stalk cut: GH ↓ (no GHRH)
3. Thyroid-Stimulating Hormone (TSH)
RF: TRH = Thyrotropin-Releasing Hormone
RIF: Somatostatin (also inhibits TSH)
Effect when stalk cut: TSH ↓
4. Adrenocorticotropic Hormone (ACTH)
RF: CRH = Corticotropin-Releasing Hormone
RIF: None
Effect when stalk cut: ACTH ↓
5. LH & FSH
RF: GnRH = Gonadotropin-Releasing Hormone
RIF: None
Effect when stalk cut: LH/FSH ↓
8. Growth Hormone (GH)
Structure
191‑aa single‑chain polypeptide
Produced by somatotrophs
Secretion pattern
Pulsatile - does not release constantly but rather every few hours
Peaks during slow‑wave sleep - largest GH surge of the entire day happens during deep sleep
Abolished by sleep deprivation → Restored by daytime sleep
9. GH Regulation
Hypothalamic control
GHRH (stimulates)
Somatostatin (SS) (inhibits)
Both released in pulses
GH secretion is controlled by alternating pulses of GHRH (stimulates) and somatostatin (inhibits). Their rhythmic release produces the characteristic pulsatile GH secretion pattern, with the largest GH pulse occurring during slow‑wave sleep.
Somatotroph signalling (two method)
GHRH → GPCR → ↑ cAMP → ↑ Ca²⁺ → GH release
SS → GPCR → ↓ cAMP → inhibition
GHRH Pathway stimulates the release of GH
GHRH binds its receptor on somatotrophs
Receptor is Gs‑protein coupled
Activates adenylyl cyclase
↑ cAMP
Activates PKA
PKA opens voltage‑gated Ca²⁺ channels
↑ intracellular Ca²⁺
Ca²⁺ triggers exocytosis of GH‑containing vesicles
Somatostatin (ss) pathway inhibts the GH
SS binds its Gi‑coupled receptor
Inhibits adenylyl cyclase
↓ cAMP
↓ PKA activity
Ca²⁺ channels stay closed
No Ca²⁺ influx → no GH release
Feedback
GH exerts short‑loop negative feedback on hypothalamus.
10. GH Actions
GH promotes growth, builds muscle/protein, burns fat, and increases blood glucose.
Growth by
↑ cell number & size
↑ bone length & thickness
Metabolic
Distinct from growth effects
(Details covered in later lectures)
11. GH Receptor Signalling (JAK‑STAT Pathway)
straight chain of events from GH binding → gene transcription.
GH binds GH receptor
Receptor conformational change - changes shape so inside can activate signaling
JAK2 activation
JAK2 phosphorylates receptor
STATs dock - STAT proteins attach to these phosphorylated sites.
STATs phosphorylated - JAK2 phosphorylates the STATs.
STAT dimers form
STATs enter nucleus - The STAT dimers move into the nucleus.
Gene transcription (e.g., IGF‑1 in liver) - They turn on GH‑responsive genes — most importantly IGF‑1 in the liver.
Lecture 4: Growth Hormone (GH), IGF‑1 & Growth Regulation
1. GH: Structure, Source & Secretion Pattern
Structure & Production
GH is a polypeptide hormone synthesized and secreted by somatotrophs in the anterior pituitary.
Transcript: “growth hormone is polypeptides… synthesised and secreted by the somatotroph cells in the anterior pituitary gland”
Hypothalamic Control
GHRH (43 aa peptide) → stimulates GH.
Somatostatin (14 & 28 aa forms) → inhibits GH.
Both act via GPCRs on somatotrophs:
GHRH receptor → Gs → ↑cAMP → PKA → Ca²⁺ influx → GH exocytosis.Transcript: “GS stimulates adenylyl cyclase… cyclic AMP activates PKA… opening of calcium channels… exocytosis of growth hormone”
Somatostatin receptor → Gi → ↓cAMP → inhibition of GH release.
Pulsatile Secretion
GHRH is released pulsatilely → each pulse produces a GH pulse.
Interpulse interval dominated by somatostatin.Transcript: “A pulse of GHRH gives you a pulse of GH… in the interpulse interval… somatostatin being dominant”
Lifespan Changes
High GH in neonates → maintained in childhood → peaks at puberty → declines in adulthood.
Adults retain mainly one large nocturnal pulse.
2. GH Feedback Regulation
Short‑loop Negative Feedback
GH feeds back to hypothalamus:
↑GH → ↑somatostatin, ↓GHRH.Transcript: “High levels of growth hormone… switch on somatostatin, switch off GHRH”
Long‑loop Negative Feedback
IGF‑1 (from liver + other tissues) inhibits GH secretion at pituitary & hypothalamus.
Integrated Hypothalamic Inputs
Metabolic: high amino acids, low fatty acids, hypoglycaemia.
Neural: exercise, slow‑wave sleep, stress, malnutrition.
Hormonal: sex steroids (pubertal rise).
3. GH Receptor & Signalling (JAK‑STAT Pathway)
Receptor Type
GH receptor = Class I cytokine receptor (shared with prolactin, EPO, ILs).
Mechanism
GH binds two receptor arms → conformational change.
Activates JAK2 (autophosphorylation).Transcript: “conformational change results in activation of JAK2… autophosphorylates”
JAK2 phosphorylates tyrosine residues on receptor.
STATs (mainly STAT5) dock and are phosphorylated.
STAT dimers translocate to nucleus → bind STAT response elements → gene transcription (e.g., IGF‑1 in hepatocytes).
Amplification occurs via multiple STAT molecules (not shown in simple diagrams).
Other Pathways
GH can also activate MAPK in some tissues.
4. IGF‑1: Structure, Receptors & Actions
Structure
IGF‑1 is structurally similar to insulin (shared homology in B and A domains).
Receptor
IGF‑1 receptor = tyrosine kinase receptor (autophosphorylates).
Signals via:
PI3K–AKT pathway → survival, protein synthesis.
MAPK pathway → proliferation.
Actions
Hypertrophy (↑cell size)
Hyperplasia (↑cell number)
↑Cell survival
5. Somatomedin Hypothesis (Classic vs Modern)
Classic (1950s)
GH does not directly stimulate growth.
GH → liver → IGF‑1 → systemic growth.
Modern Understanding
GH has direct effects on many tissues (GH receptors are widespread).
IGF‑1 comes from:
Liver (endocrine)
Local tissues (paracrine) e.g., bone, muscle.
Local IGF‑1 can spill into circulation.
Both GH + IGF‑1 are required for normal growth.
Evidence
Knockout of IGF‑1 in muscle → 30% drop in circulating IGF‑1, showing non‑liver contribution.Transcript: “knocked out IGF1 in muscle… mice had a 30% decline in circulating IGF‑1”
6. GH & IGF‑1 in Bone Growth
Epiphyseal Plate Zones
Proliferation zone: GH + IGF‑1 stimulate chondrocyte division.
Hypertrophy zone: mainly IGF‑1 increases chondrocyte size.
Osteoblasts replace cartilage with bone → elongation.
Growth Plate Closure
Occurs after puberty due to oestrogen (in both sexes).
After closure:
GH/IGF‑1 cannot increase bone length.
Can still increase bone thickness (acromegaly).
7. GH Metabolic Actions (Direct via GH‑R)
Muscle
↑Amino acid uptake
↓Glucose uptake
↓Protein breakdown
↑Muscle mass
Adipose Tissue
↓Glucose uptake
↑Lipolysis → ↓fat stores
Liver
↑Protein synthesis
↑Gluconeogenesis
↑Blood glucose
Overall
GH is anti‑insulin for glucose & fat metabolism but anabolic for protein.
8. Growth Patterns Across Life
Two Major Postnatal Growth Spurts
Infancy: birth → 24–36 months
Puberty:
Girls: 8–13 years
Boys: 10–15 years
IGF‑1 Peaks at Puberty
Peak IGF‑1 levels correspond to peak height velocity.
Determinants of Stature
GH allows achievement of genetic potential.
Nutrition is a major modulator.
9. GH Disorders
GH Deficiency
Children: pituitary dwarfism
Short stature (~1.2 m), normal proportions, poor muscle development, ↑subcutaneous fat.
Recombinant GH restores near‑normal growth if treated before puberty.
Adults: minimal symptoms.
GH Excess
Children: gigantism (very tall, proportional growth).
Adults: acromegaly
Enlarged hands, feet, jaw; thickened soft tissues; deep voice.
Treatment: somatostatin analogues or surgery.
10. Hormonal Interactions Required for Normal Growth
Thyroid hormones
Sex steroids (T, E)
Insulin
Glucocorticoids (excess inhibits growth)
Lecture 5: Growth hormone GH
1. GH Structure, Source & Secretion Pattern
GH = polypeptide hormone secreted by somatotrophs in anterior pituitary. Transcript: “growth hormone is polypeptides… synthesised and secreted by the somatotroph cells”
Circulates unbound (water‑soluble).
GH receptors are widely expressed → GH has direct actions on many tissues.
Pulsatile secretion
GHRH pulses → GH pulses. Transcript: “A pulse of GHRH gives you a pulse of GH”
Somatostatin dominates interpulse intervals → suppresses GH.
Pulsatility changes across lifespan: high in neonates, stable in childhood, peak at puberty, decline in adulthood.
2. Hypothalamic Regulation of GH
Releasing factor
GHRH (43 aa)
Receptor = Gs‑coupled GPCR
↑Adenylyl cyclase → ↑cAMP → ↑PKA → Ca²⁺ influx → GH exocytosis
Inhibitory factor
Somatostatin (14 & 28 aa forms)
Receptor = Gi‑coupled GPCR
↓cAMP → ↓Ca²⁺ influx → ↓GH secretion
Convergence
GHRH and somatostatin converge on cAMP levels inside somatotrophs. Transcript: “this… is what we call convergence… levels of cyclic AMP determine secretion”
3. GH Feedback Regulation
Short‑loop negative feedback
GH → hypothalamus:
↑Somatostatin
↓GHRH Transcript: “High levels of GH… switch on somatostatin, switch off GHRH”
Long‑loop negative feedback
IGF‑1 (liver + other tissues) inhibits GH at pituitary & hypothalamus.
Other regulators
Metabolic: high AA, low FAs, hypoglycaemia
Neural: exercise, slow‑wave sleep, malnutrition
Hormonal: sex steroids (pubertal rise)
4. GH Receptor & JAK‑STAT Signalling
GH receptor = Class I cytokine receptor (shared with PRL, EPO, ILs).
Mechanism
GH binds two receptor arms → conformational change
Activates JAK2 (autophosphorylation)
JAK2 phosphorylates receptor tyrosines
STATs (mainly STAT5) dock and are phosphorylated
STAT dimers → nucleus → bind STAT response elements
↑Transcription of growth‑related genes (e.g., IGF‑1 in hepatocytes) Transcript: “one of the key targets… regulate IGF‑1”
Amplification
Many STATs activated → large transcriptional response.
Other pathways
GH can also activate MAPK in some cells.
5. IGF‑1: Structure, Receptor & Actions
IGF‑1 = polypeptide structurally similar to insulin (shared homology in B & A domains).
Receptor = tyrosine kinase receptor (autophosphorylates).
Signalling:
PI3K–AKT → survival, protein synthesis
MAPK → proliferation
Actions
Hypertrophy (↑cell size)
Hyperplasia (↑cell number)
↑Cell survival
6. Somatomedin Hypothesis (Classic → Modern)
Classic (1950s)
GH does not directly stimulate growth.
GH → liver → IGF‑1 → systemic growth.
Modern understanding
GH has direct effects on many tissues (GH‑R widely expressed).
IGF‑1 comes from:
Liver (endocrine)
Local tissues (paracrine) e.g., bone, muscle
Local IGF‑1 can spill into circulation.
Key evidence
Muscle‑specific IGF‑1 knockout → 30% drop in circulating IGF‑1. Transcript: “those mice had a 30% decline in circulating IGF‑1”
Conclusion
Growth = combined actions of GH + IGF‑1 (endocrine + paracrine).
7. GH in Bone Growth
Epiphyseal plate
Proliferation zone: GH + IGF‑1 stimulate chondrocyte division
Hypertrophy zone: IGF‑1 increases chondrocyte size
Osteoblasts replace cartilage → bone elongation
Growth plate closure
Occurs after puberty due to oestrogen.
After closure: GH/IGF‑1 cannot increase bone length → only thickness.
8. GH Metabolic Actions (Direct via GH‑R)
Muscle
↑AA uptake
↓Glucose uptake
↓Protein breakdown
↑Muscle mass
Adipose
↓Glucose uptake
↑Lipolysis → ↓fat stores
Liver
↑Protein synthesis
↑Gluconeogenesis
↑Blood glucose
Overall: GH is anti‑insulin for glucose/fat metabolism but anabolic for protein.
9. Growth Patterns
Two major postnatal growth spurts:
Infancy (0–2/3 years)
Puberty (girls 8–13, boys 10–15)
IGF‑1 peaks at puberty → peak height velocity.
10. GH Disorders
GH deficiency
Children: pituitary dwarfism
Short stature (~1.2 m), normal proportions, poor muscle development, ↑subcutaneous fat
Recombinant GH restores near‑normal growth
Adults: minimal symptoms
GH excess
Children: gigantism
Adults: acromegaly
Enlarged hands/feet/jaw, thickened soft tissues, deep voice
↑CVD risk, ↑T2DM risk
Loss of IGF‑1 negative feedback
Treatment: surgery or somatostatin analogues (e.g., octreotide)
Lecture 6: Prolactin (PRL)
1. Structure, Synthesis & Secretion
PRL = polypeptide hormone (199 aa).
Produced by lactotrophs in anterior pituitary.
Regulation
Inhibited by dopamine (PIF)
Dopamine from hypothalamic arcuate nucleus
Acts via D2 (Gi) receptors → ↓cAMP → ↓Ca²⁺ influx → ↓PRL secretion Transcript: “Dopamine… inhibits secretion, synthesis, lactotroph proliferation”
Stimulated by PRF (identity unknown; TRH/VIP suggested but not physiologically dominant except in stress/lactation)
Spontaneous secretion
Lactotrophs show intrinsic spontaneous activity:
↑cAMP
Membrane depolarisation
Ca²⁺ influx
PRL exocytosis (Shown in Stojilkovic data)
2. Prolactin Signalling
PRL receptor = Class I cytokine receptor (same family as GH‑R).
Main pathway: JAK2–STAT5
STAT5 → nucleus → transcription of milk‑related genes
STAT1/3 also activated in some contexts.
3. Prolactin Actions
Mammary gland
Development
Puberty: oestrogen + GH
Pregnancy: PRL + oestrogen + progesterone → alveologenesis
Lactation (lactopoiesis)
↑Milk protein synthesis (β‑casein, WAP, α‑lactalbumin)
↑Milk fat secretion
Regulates ion transport + tight junction integrity
↑Lactose synthesis → major osmotic driver of milk volume
Milk ejection vs milk production
Oxytocin → milk ejection (myoepithelial contraction)
Prolactin → milk synthesis/secretion Slides: “Oxytocin = ejection; Prolactin = secretion”
Non‑reproductive roles
Immune modulation
Behavioural effects
4. Feedback Regulation
Short‑loop negative feedback
PRL → hypothalamus → ↑dopamine → ↓PRL
No long‑loop feedback (mammary gland does not produce a hormone).
Non‑lactating individuals
High dopamine tone keeps PRL low. Slides: “Dopamine constantly suppresses PRL… main regulator is inhibitory factor”
Lactation
Suckling → ↓dopamine + ↑PRF → ↑PRL
PRL surge prepares milk for next feed (feed‑forward).
Oestrogen during pregnancy ↑PRL mRNA.
5. Suckling Reflex
Nipple mechanoreceptors → hypothalamus
↓PIF (dopamine)
↑PRF
↑PRL (milk synthesis)
↑Oxytocin (milk ejection)
6. Prolactin Disorders
Hyposecretion
Failure to lactate
Possible immune/metabolic effects
Hyperprolactinaemia
Causes:
Prolactinoma (benign pituitary tumour)
Antipsychotics (dopamine antagonists)
Effects:
Females: galactorrhoea, amenorrhoea
Males: gynecomastia, low libido
PRL inhibits HPG axis → ↓GnRH → ↓LH/FSH
Treatment:
Dopamine agonists (e.g., bromocriptine, cabergoline)
Surgery (transsphenoidal)