EMT Notes
Airway, Respiration and Ventilation
Airway Steps
Open → head tilt chin lift (medical) OR jaw thrust maneuver (trauma)
Clear → is suction required? (up to 15 seconds)
Keep→OPA (mouth to ear/jaw) vs NPA (nose to ear)
Vent → BVM at 15 lpm / 1 breath every 5-6 seconds / E+C Grip
Abnormal Respiratory Patterns
Rate / Depth of Breathing
What can influence this?
Rate / Depth go up (ex: anxiety or pain)
Metabolic acidosis
Anxiety =/ Pain
Hypoxemia
Rate / Depth go down
Metabolic alkalosis
CNS depression
Opiate overdoses
Agonal → “gasping” patient in arrest; no respirations
Bradypnea →below 12 : respiratory depression (chest wall injury / drug overdose)
Tachypnea → above 20 : pain + anxiety, pulmonary embolism / pneumothorax
Ataxic → irregular with pauses, strokes and trauma damage to medulla oblongata
Cheyne-Stokes → Trauma, tumors, heart failure (fast shallow to heavy deep respirations)
Kussmaul → DKA response, constant deep + rapid breathing pattern
Respiratory Distress vs Failure
Severity of Respiratory Emergencies
Respiratory Distress: Increased work of breathing because the respiratory emergency caused inadequate gas exchange (CPAP)
Respiratory Failure: Respirations begin to slow, patient gets tired, oxygenation/ventilation can’t support the demands of the body. Going to need ventilation by me.
Respiratory Arrest: Patient stops breathing, the heart could still be beating.
Respiratory Depression: Some event (emergency, overdose) has caused the patient’s respiratory drive to become slowed. Ex: opiates will “depress” your respirations. Patients have slow respirations.
Respiratory Distress (happens 1st)
Still alert but agitated or anxious
Airway is open (can still speak, 1-2 word sentences)
RR is high (ex: 28)
Tachycardia
Pale
Retractions (pulling of the skin between the ribs)
Accessory muscle use
Nasal Flaring
Tripod position (in peds could also be head bobbing)
Low SPO2
Respiratory Failure
Confusion, AMS
Airway not patent
RR is low (ex: 8)
Bradycardia
Cyanosis
Slow, sluggish respirations (tired)
Nasal Cannula, Non-Rebreather Mask, Bag-Valve Mask
Ventilation - air in/out of the lungs
vs
Oxygenation - how well oxygen binds to hemoglobin on red blood cells (SPO2 levels)
Nasal Cannula - O2, 1-6 lpm (low SPO2, but mild symptoms)
Non-Rebreather - O2, 15 lpm (Respiratory distress with low SPO2)
Bag-Valve Mask - ventilation, 25 lpm, unable to manage own airway, most commonly unresponsive with low RR (I need to breathe for them)
EXAMPLE:
RR Respiratory Rate - 20
O2 (SPO2 / Pulse oximeter) - 92%
Words / Sentence - 4-5
Labored? - Sitting, but SOB
Trial a nasal cannula first. Low SPO2, but not in respiratory distress yet. Work your way up. (2 - 4 - 6).
RR Respiratory Rate - 28
O2 (SPO2 / Pulse oximeter) - 90%
Words / Sentence - 1-2
Labored? - Tripod position, accessory muscle use
They need a nonrebreather. You can give a BVM if the RR is too high, but the patient needs to be unresponsive.
RR Respiratory Rate - 8
O2 (SPO2 / Pulse oximeter) - 85%
Words / Sentence - 0 (unresponsive, no ability to control their airway)
Labored? - Failure
BVM!!
CPAP vs BiPAP
CPAP: brings positive pressure into the airways. This raise in pressure allows the alveoli to remain “open” for gas exchange and push fluid off.
Indicators: CHF, asthma, COPD, pneumonia (pus filled lungs), drownings
CHF has pulmonary edema (fluid in the lungs), you hear rales in their lungs bilaterally. They want to bring in oxygen but they can’t because there’s fluid in the alveoli.
Contrainicators: unresponsive, hypotensive (not enough blood going back to the heart), pneumothorax, N/V, arrest… must be able to follow commands
BiPaP: When the patient inhales, the pressure is similar to CPAP, but when the patient exhales, the pressure drops to make it easier to exhale.
Typical Settings:
IPAP - 10 cmH2O (4 -24) ALWAYS HIGHER
EPAP - 5 cmH20 (2 - 20)
These settings can vary by patients needs. The goal is to withhold ET intubation.
Pressure Support: Spontaneous mode of ventilation, where a ventilator delivers support with a preset valve, based on their RR.
CPAP / BiPAP: Both use PEEP at the end of exhalation. This means that positive pressure at the end of exhalation keeps the alveoli open.
Positive
End
Expiratory
Pressure
Sit patient upright, gain vitals (EKG, end tidal CO2, pulse ox, lung sounds), coach your patient. CPAP (5 - 10 cmH20). Start low and work your way up.
Continuously take lung sounds on the patient, look for spontaneous pneumo or altered mental status.
Lung Sounds
Wheezing (constriction) :
Asthma
Anaphylaxis
COPD
Rhonchi: Pneumonia (infection / mucus)
Rales : CHF (fluid)
Stridor
Stridor - high-pitched upper airway sound (partially obstructed upper airway) around area of epiglottis/trachea.
Croup
Epiglottitis
Foreign body airway obstruction
Inhalation burn
Anaphylaxis
Bonus thought : high MOI trauma
Asthma
1) Bronchoconstriction, mucus
2) Smoking, allergies, pollen, physical exertion
3) Wheezing (AAC), cough with tightness in chest, accessory muscle use, hard time exhaling
4) Oxygen (first thing done), NRB mask, Goal: 94-99% SPO2 // Albuterol Assistance (inhaler) + CPAP - 5-10 cm H20
Anaphylaxis
Allergic Reaction - 1 body system
vs
Anaphylaxis - 2 or more body systems
1) Severe allergic response that can be life-threatening
2) Insects, bees, food, medications
3) Stridor, wheezing, hives, nausea/vomiting
4) Epinephrine (pen) - 0.3 mg IM // Epipen Jr - 0.15 mg IM
(oxygen + albuterol)
COPD
Chronic Bronchitis -
Blue bloaters (nail beds or skin)
Overweight
Productive cough
Excessive mucus
Tight Airways
Emphysema -
Pink Puffers
Thin, barrel chest
Cough only
Pursed lip breathing
Non-elastic alveoli
1) Chronic respiratory disease, bronchoconstriction, mucus production, destruction of alveoli
2) Smoking, Irritants, Hazardous areas
2) Wheezing, Rhonchi, difficulty breathing, tightness of the chest, low SPO2.
4) Treatment:
1 - Oxygen, get patient back to 94% SPO2.
2 - Albuterol
3 - CPAP 5 - 10 cm H2O
Pulmonary Embolism (PE)
1) Thrombosis (when blood clots block your blood vessels) in the pulmonary arteries “Lung Attack”
2) Long rides/travel, surgery, cancer, pregnancy, birth control use, smokers
3) Short of breath, chest pain, tachycardia, hypoxia
4) Oxygen at 15 lpm, maintain 94-99% // Rapid transport
Bonus: Transmit 12 lead ECG
Cardiology + Resuscitation
Heart Anatomy, Physiology, and Pathophysiology
Mammals have four-chambered hearts and double circulation. The heart of a bird or mammal has two atria and two completely separate ventricles. The double-loop circulation is similar to amphibians and reptiles, but the oxygen-rich blood is completely separated from oxygen-poor blood. The left side of the heart handles only oxygenated blood, and the right side receives and pumps only deoxygenated blood. With no mixing of the two kinds of blood, and with a double circulation that restores pressure after blood has passed through the lung capillaries, delivery of oxygen to all parts of the body for cellular respiration is enhanced.
External Anatomy of the Heart
Pericardium - the thin membrane that covers the heart.
Also known as the pericardial sac
A three layer closed sac that surrounds the heart and anchors it
Fibrous outer layer
Parietal Serious (middle layer - lines fibrous layer)
Visceral Serious (inner layer - adheres to the surface itself)
Myocardium
Located in the lower two chambers of the heart (ventricles)
Apex
Tip of the heart
Only the left ventricle extends all the way to the apex
The front of the heart (anterior view) is recognized by a groove (anterior ventricular groove) that extends from the right side of the broad end of the heart diagonally to a point above and to your left of the apex
You can locate the following champers of the heart from this view:
Left Atrium : upper chamber to your right
Left Ventricle : lower chamber to your right
Right Atrium : upper chamber to your left
Left Ventricle : lower chamber to your left
With the heart in the anterior view position we can see the following blood vessels at the broad end of the heart:
Coronary Artery (Right + Left) - this blood vessel lies in the groove on the front end of the heat (LAD) and it branches over the front and back side of the heart to supply fresh blood with oxygen and nutrients to the heart muscle itself. The right and left coronary arteries are the first branches from the aorta.
Pulmonary Artery - this blood vessel branches and carries blood to the lungs to receive oxygen and and can be found curving out of the right ventricle (upper chamber to your left)
Aorta - major vessel located near the right atria and just behind the pulmonary arteries near the lungs; locate the curved part of this vessel known as the aortic arch. Branching from the aortic arch is a large artery that supplies blood to the upper body (3 branches: brachiocephalic trunk [right common carotid and right subclavian]. left common carotid and left subclavian).
Pulmonary Veins - these vessels return oxygenated blood from the right and left lungs to the left atrium (upper chamber on your right)
Inferior + Superior Vena Cava - these two blood vessels are located on your left of the heart and connect to the right atrium (upper chamber on your left). Deoxygenated blood enters the body through these vessels into the right atrium. These vessels do not contain valves to control blood flow.
Internal Anatomy
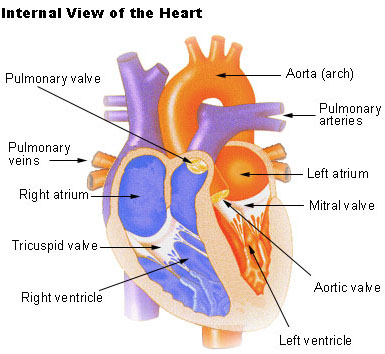
The right atrium has a thin muscular wall and is the first receiving chamber of the heart.
The inferior and superior vena cava enters this chamber and do not contain valves.
Chambers of the Heart
Atria
Right Atrium
Left Atrium
Ventricles
Right Ventricle
Left Ventricle
Valves of the Heart
Atrioventricular Valves
Tricuspid Valve
Mitral Valve
Semilunar Valves
Pulmonary Valve
Aortic Valve
Major Blood Vessels
Aorta
Pulmonary Artery
Pulmonary Veins
Vena Cavae
Conduction System
Sinoatrial Node (SA Node)
Atrioventricular Node (AV Node)
Bundle of His
Purkinje Fibers
Sub-Branches:
Coronary Arteries
Right Coronary Artery
Left Coronary Artery
Septum
Interatrial Septum
Interventricular Septum
Papillary Muscles
Right Ventricular Papillary Muscles
Left Ventricular Papillary Muscles
Heart Blood Flow
Arteries - go away from the heart
Veins - go towards the heart
Superior Vena Cava (SVC) - blood going back to the heart
Inferior Vena Cava (IVC) - blood going back to the heart
Tricuspid Valve - 3 comes before 2
Right Ventricle - get heart O2
Left Ventricle - pump blood to body
Lungs - has our O2
Pulmonary Artery - bridge from the right ventricle to the lungs
Pulmonary Vein - has oxygen and brings it back to the heart from the lungs.
Left Atrium passes down through the mitral valve to the left ventricle and passes to the aorta.
The blood enters the left side of the heart through the PULMONARY VEIN and enters the left atrium. It then passes through the BICUSPID VALVE to enter the left ventricle.
Blood flows in the following sequence in the heart:
Superior Vena Cava/Inferior vena cava, right atrium, tricuspid valve, right ventricle, pulmonic valve, pulmonary artery, lungs, pulmonary veins, left atrium, bicuspid valve, left ventricle, aortic valve, aorta.
Blood that flows through the right side of the heart is deoxygenated. The SVC/IVC lead to the right atrium which leads to the right ventricle which leads to the pulmonary artery because blood needs the oxygen the lungs have brought in.
Congestive Heart Failure (CHF)
1) CHF is when the heart fails as a pump, pulmonary edema (fluid in the lungs) can be life threatening
2) Risk Factors: smoking, diabetes, hypertension, high cholesterol
3) Signs and Symptoms : rales bilaterally, pink sputum with cough (left side) hypertension, fluid in the legs (right side)
4) Treatment:
Oxygen (raise SPO2)
12 Lead ECG (transmit)
CPAP 10 cm H2O (5-10 cmH2O) the range for CPAP is 5-10 cmH2O
When your heart fails as a pump, it is dying and needs help. When the heart fails, blood backs up.
CHF →blood backs up
Left Ventricle backs up → the Left Atrium → backs up to Pulmonary Vein → backs up into the lungs (the pink sputum is from blood in the lungs)
Right Side:
Pulmonary Artery backs into → Right Ventricle backs into→ Right Atrium backs into → Venous System (SVC + IVC), this causes JVD (SVC) and fluid in the legs (IVC)
Cardiac Output + Ejection Fraction
Systole: contraction of the ventricles pumping blood
Diastole: relaxation of the heart + ventricles after moving the blood forward
Preload: amount of blood returning to the heart (think right side return)
nitroglycerin decreases preload
After load: pressure in the aorta, the left ventricle must pump against, if the left ventricle fails, blood backs up and we get pulmonary edema in the lungs
Contractility: the strength of contractions that stretches the ventricles to pump harder
Automaticity: the cardiac muscle cells allow the cell to contract without a stimulus from a nerve (specialized in cardiac muscle cells)
Cardiac Output: amount of blood pumped in one minute (L/min); not the rate, the AMOUNT of blood.
Stroke Volume: amount of blood ejected per contraction (mL)
Heart Rate: heart beats per minute (bpm)
CO = SV x HR
Cardiac Output = Stroke Volume x Heart Rate
L/min = mL x bpm
5-6L/min at rest = 50 - 100 mL x 60-100 bpm
100 mL x 60 bpm = 6000 mL or 6 L/min
75 mL x 72 bpm = 5400 mL or 5.4/mL
Ejection Fraction: 50-75% is normal, how well your heart pumps blood out of the left ventricle.
End-Diastolic Volume: the amount of blood that is in the ventricles before the heart contracts (120 mL)
Stroke Volume: amount of blood ejected per contraction (50-100 mL)
EF % = SV/EDV x 100
EF = 70 mL/120 mL x 100
58% 0.58 × 100
Mean Arterial Pressure
Mean arterial pressure: the average pressure going through the arteries during heartbeats
When we are giving fluid, or trying to get a blood pressure back to “normal limits” we are trying to target the systolic blood pressure and the mean arterial pressure.
Important for calculating how much fluid to give a patient who may have lost blood or is severely dehydrated. We also look at systolic blood pressure.
We are trying to get the mean arterial pressure up to 60 and the systolic up to 90. If the patient is below 90 they are hypotensive. We don’t want to make the blood of a patient pink because IV fluids cannot carry oxygen.
Blood pressure is 80/68
SP - DP: Pulse Pressure, normal is around 40 (120 - 80 = 40)
MAP = DP + 1/3(SP - DP)
MAP = 68 + 1/3(80 - 68)
MAP = 68 + 1/3(12)
MAP = 68 + 4 = 72
Blood pressure is 80/68
MAP = DP x 2 = ______ + SP = _____ / 3
72 = 68 × 2 = 136 + 80 = 216 / 3 = 72
Blood pressure is 76/40 (Patient is in septic shock)
MAP = DP + 1/3(SP - DP)
MAP = 40 + 1/3(76 - 40)
MAP = 40 + 1/3(36)
MAP = 40 + 12 = 52
Types of Angina
Stable Angina - pain stops with rest
Unstable Angina - pain persists even with rest
The coronary arteries are associated with a myocardial infarction (MI).
Clot (classic myocardial infarction)
vs
Constriction (vasoconstriction of an artery) “prinzmetal angina”
Myocardial Infarction (MI)
MI is when a coronary artery is blocked, causing no blood flow to the heart muscle
Myo - muscle
Cardiac - heart
Infarction - dying
Risk factors: (SAD CHF) smokers, age 50+, diabetes, high cholesterol, high blood pressure, family history
Symptoms: crushing chest pain, left arm/shoulder/jaw pain, nausea/vomiting, weakness/malaise, back pain.
Treatment:
Oxygen (goal 94% or higher)
Aspirin 324 mg (4 81 mg chewable baby aspirin)
Assist with nitroglycerin
Transmit 12 lead ECG
Major Pulse Points
1) Temporal Pulse - next to ear
2) Carotid - On the neck
3) Apical - space down the front part of the chest and slide to the left 5th intercostal space (space between 4th and 5th rib)
4) Brachial - where you get your blood pressure
5) Radial - inside of wrist
6) Femoral - deep in the groin
7) Popliteal - bend the knee, it is behind it
8) Posterior Tibial - inside of the ankle
9) Dorsalis Pedis - top of the foot
Stroke (Cerebrovascular accident)
1) Blockage / hemorrhage of a cerebral artery that supplies blood to the brain. Can be ischemic (clot in one of the brain’s arteries) or hemorrhagic (when a vessel bursts and blood is not being received to the brain). You will not know what the stroke is in the field.
2) Risk Factors: Smoking, diabetes, hypertension, high cholesterol, atrial fibrillation (when the heart beats too fast), previous stroke/clot
3) Symptoms:
Balance, does it appeal normal
Eyes, blurred vision, nystagmus (fluttering of the eyes when looking up)
Facial droop?
Arm drift?
Speech
Time, last seem normal (3 - 4.5 hrs TPA)
4) Treatment: oxygen and get a blood glucose level, if both are normal, it is a stroke.
Stroke Scales
Cincinnati Prehospital Stroke Scale
Balance
Eyes
Facial Droop
Arm drift
Speech
Time
Los Angeles Prehospital Stroke Scale
Age older than 45
No history of seizures
Symptoms less than 24 hours
Not wheelchair/bed bound
GCL 60 - 400
Obvious Asymmetry in any of the following exams:
Facial Smile
Grip
Arm Strength
Basic Cardiac Life Support
Early Recognition of Cardiac Arrest
Early CPR (layperson chest compressions only)
Early AED/defibrillation
Post resuscitation care
Steps for Cardiac Arrest:
Scene Safe + PPE
Get AED and request ALS
Check pulse/breathing (no more than 5-10 seconds)
No breathing : Rescue breaths
All good : monitor + place in recovery position
Arrest : begin CPR (100-120 bpm)
30 : 2 for adults and children
15 : 2 for infants with 2 rescuers
AED → shock or no shock in 2 minute cycles
AAA: Abdominal Aortic Aneurysm
AAA → a tear / rupture of the aorta. THe blood goes into the peritoneum and causes peritonitis.
Cardiac Risk Factors:
Smoking
Age 60 - 70 yearsDiabetes
Cholesterol high
Hypertension
Family history
Symptoms: unexplained hypotension, pale skin, abdominal pain, syncope, bradycardia
Treatment: Oxygen, IV fluids, rapid transport (ALS)
Trauma
Trauma Overview
Trauma Assessment
Bleeding
Hematoma - Bleeding
Place patient forward for nosebleeds
Tourniquets are applied high and tight
Three Types of Bleeding:
1) Arterial Bleeding
2) Venous Bleeding
3) Capillary Bleeding
You can not lose more than 20% of blood volume
Soft Tissue Injuries
Avulsion - when a flap of skin is hanging off
Crush Injuries - Do not move the patient right away; they could go into cardiac arrest; call ALS
Compartment Syndrome - can lead to tissue death
Eviscerations - DO NOT PUT BACK IN
Penetrating Injuries - DO NOT TAKE OUT
Burns : Degrees, Types + Zones
1st degree -
2nd Degree -
3rd Degree -
Types:
Chemical -
Radiation -
Thermal -
????
3 Zones :
Burns : Rule of 9s, Treatment
Trauma to the Head, Neck, and Spine
Nervous System and Skeletal Systems
Nervous System
Nervous System - provides overall control of thought, sensation, and the body’s voluntary and involuntary motor functions
Peripheral Nervous System - the nerves that enter and exit the spinal cord between the vertebrae, the 12 pairs of cranial nerves that travel between the brain and organs without passing through the spinal cord, and all of the body’s other motor and sensory nerves
Central Nervous System - the brain and the spinal cord
Anatomy of the Head
The skill is made up of the cranium and the facial bones.
Temporomandibular joint - the moveable joint between the mandible and the temporal bone, also called the TMJ.
Anatomy of the Spine
The spinal cord is a bundle of nervous tissue about the width of a thumb that extends out about 18 inches from the brain stem down to the small of the back.
33 irregularly shaped bones, called vertebrae (singular vertebra), surround the cord and provide it with bony protection. The vertebrae are stacked on top of another and interlock to form the spinal column.
From top to bottom they are:
7 cervical (in the neck)
12 thoracic (to which the ribs attach)
5 lumber (mid-back)
5 sacral (lower back)
4 coccygeal (in the coccyx, or tailbone)
Both the sacral and coccygeal vertebrae are fused together, forming the posterior portion of the pelvis.
Cerebrospinal fluid (CSF) - the fluid that surrounds the brain and spinal cord
Injuries to the Skull and Brain
Scalp Injuries
The scalp has many blood vessels, so any scalp injury may cause profuse bleeding.
Control Scalp Bleeding by applying direct pressure.
Skull Injuries
With head injuries, the words open and closed refer to the cranial bones.
There is not a lot of distance between the skin and the skull.
Whenever you suspect a skull or brain injury, also suspect a spine injury (C-Spine
Brain Injuries
The brain sits in fluid inside of the skull. You can bleed in the brain, in-between the brain and the meninges, or in the skull.
Direct injuries to the brain can occur:
In open head injuries
With the brain being lacerated, punctured or braised by the broken bones or by a foreign object such as a bullet.
Indirect Injuries to the brain may occur with either closed or open head injuries.
Traumatic Brain Injuries
A traumatic brain injury (TBI) is an injury that disrupts the normal functioning of the brain. It may be a brief (concussion) or longer term condition with permanent damage to the Brian.
Concussion - may be so mild that the patent is unaware of the injury. It is a mild injury, usually with no detectable brain damage. There Amy be a brief loss of consciousness, and headache, grogginess, and short term memory loss.
Contusion - a bruised brain. When the bruising of the brain occurs on the side of the blow, it is called a coup injury when it occurs on the side opposite the blow, it is called a contrecoup injury. Symptoms include unconsciousness, decreased level of responsiveness, and bruising of the brain tissue.
Intracranial Pressure
Intracranial pressure - pressure inside the skull
As the pressure mounts, the brain can be forced downward to the only space available - the foramen magnum, the opening at the base of the skull.
When intracranial pressure increases, the body must increase the blood pressure to overcome the resistance to blood flow in the cranium.
As the hematoma continues to grow, swelling worsens, and the brain is pushed downward towards the foramen magnum, compressing the brain stem. The brainstem regulates our most vital functions including breathing, heartbeat, and blood pressure.
Cheyne - Stokes Breathing - a pattern of breathing characterized by quickening and deepening respirations followed by a period of apnea.
Central Neurogenic Hyperventilation - a pattern of rapid and deep breathing caused by injury to the brain
Ataxic Respirations - a pattern of irregular and unpredictable breathing commonly caused by brain injury.
Multi-System Trauma
Determining Patient Severity
Patient Priority / Severity
Whether to limit screen time or not
Which hospital and/or transport method is best for your patient
Determining Severity : Physiologic Criteria
Altered Mental Status (GCS below 14) is a significant indicator of head injury
Hypotension (systolic blood pressure less than 90 mmHg) is a definitive sign for shock and indicates some sore of internal bleeding or other circulatory disturbance
Do not look just at the number
Abnormal respiratory rates are also indicative of serious injury
Abnormally slow rates (below 10) May indicate head injury or later stages of shock
Determining Severity : Anatomic Criteria
Multiple musculoskeletal injuries (more than two long-bone fractures means multiple trauma)
Amputations
Severely mangled extremities
Pelvic injuries are associated with significant internal bleeding
CDC Trauma Triage Guidelines : Anatomic Criteria
All penetrating injuries to head, neck, torso, and extremities proximal to elbow and knee
Chest wall instability or deformity (e.g., flail chest)
Two or more proximal long bone fractures
Crushed, degloved, mangled, or pulseless extremities
Amputation proximal to the wrist or ankle
Pelvic fractures
Open or depressed skull fracture
Paralysis
Determining Severity : Mechanism of Injury (MOI)
In the absence of physiologic or anatomic criteria, significant forces have acted on the body causes EMTs to act in a more cautious manner.
DOA - Dead on Arrival
CDC Trauma Triage Guidelines: Mechanism of Injury Criteria
Falls
Adults: > 20 feet (6 meters) (One story is equal to 10 feet [3 meters]. )
Children: > 10 feet (3 meters) or 2-3 times the height of the child
High-Risk Auto Crash
Intrusion (including roof) > 12 in. (30 cm) occupant site; > 18 in (45 cm) any site
Ejection (partial or complete) from automobile
Death in same passenger compartment
Vehicle telemetry data consistent with high risk of injury
Determining Severity : Special Patients and Considerations
Older adult patients do not compensate for shock efficiently
Children respond differently
May benefit from transport to a pediatric specialty
Patients on anticoagulants (blood thinners) or who are pregnant may require transport to a trauma center
Managing the Multisystem Trauma Patient
When does the EMT recognize that the patient has multiple injuries?
What body systems would the EMT suspect have been affected by this patient’s injuries?
What is the EMT’s first decision about managing those injuries, and why would you make it?
What actions would you take to support the affected body systems?
What priorities would you set for this patient?
An OPA can be used with a broken neck.
General Principles of Multisystem-Trauma Management
Golden Hour - the need for critical trauma patients to get to surgery within 1 hour of injury (not 1 hour from when you get to the patient)
Limit Scene Treatment to:
Stabilizing the cervical spine during all intervention
Suctioning the airway
Ventilating with a bag-valve mask
OPA and connected to O2
Administering high concentration oxygen
Controlling bleeding
Direct pressure → tourniquet
This also includes:
Scene Safety
Ensure an open airway
Perform urgent or emergency moves as necessary
Adapt to the situation
It is not good patient care to arrive at the hospital with the world’s best packaged corpse.
Pediatric patients will need additional emotional support since younger patients may not understand what is occurring to them and around them.
Trauma Scoring
Revised Trauma Score (RTS) contains:
Glasgow Coma Scale (GCS)
Systolic blood pressure
Respiratory Rate
Environmental Emergencies
How the body loses heat
Conduction - the transfer of heat from one material to another through direct contact
Convection - Carrying away of heat by currents of air, water, or other gases or liquids
Radiation - sending out energy, such as heat, in waves into space
Evaporation - the change from liquid to gas. When the body perspires or gets wet, evaporation of the perspiration or other liquid into the air has a cooling effect on the body.
You can be become hypovolemic from sweating
Generalized Hypothermia
Exposure to cold reduces body heat
Those under the influence of alcohol or other drugs also then to be affected more rapidly and more severely than others.
The words thing you can do is go inside + then back out
Every drowning you go to is a cold water drowning
If you lose blood, you lose heat
Obvious and Subtle Exposure
Overdose or Poisoning
Major Trauma
Outdoor resuscitation
Decreased ambient temperature (for example, room temperature)
Patient Assessment
Shivering - body trying to create heat
Numbness or reduced or loss sense of touch
Drowsiness and/or unwillingness or inability to do even the simplest activities
Similar to CO poisoning
Rapid breathing and rapid pulse in early stages, and slow or absent breathing and pulse in prolonged cases
Loss of motor coordination - similar to intoxication
Joint/muscle stiffness. or muscular rigidity
In prolonged cases skin is pale or cyanotic
Geriatric Note - old people can’t take the cold. Old people who live on fixed incomes might not heat their homes.
Kid Note - Infants lose 80% of body heat through their head. They are bad at handling the cold. Kids can‘t shiver like adults
Fahrenheit Celcius Symptoms | ||
99 - 96 | 37 - 35.5 | Shivering |
95 - 91 | 35.5 - 32.7 | Intense shivering, difficulty speaking |
90 - 86 | 32 - 30 | Shivering decreases and is replaced by strong muscular rigidity. Muscle coordination is affected, and erratic or jerky movements are produced. Thinking is less clear, general comprehension is dulled, and total amnesia is possible. Patient generally is able to maintain the appearance of psychological contact with surroundings. |
85 - 81 | 29.4 - 27.2 | Patient becomes irrational, loses contact with the environment, and drifts into a stuporous state. Muscular rigidity continues. Pulse and respirations are slow and cardiac dysrhythmias may develop. |
80 - 78 | 26.6 - 20.5 | Patient loses consciousness and does not respond to spoken words. Most reflexes cease to function. Heartbeat slows further before cardiac arrest occurs. |
Extreme Hypothermia
The heart rate can slow to fewer than 10 beats per minute
Assess the carotid pulse for at least 60 seconds. If there is no pulse, start CPR immediately and prepare to apply the AED.
You’re not dead until you’re warm and dead
Anyone with frostbite or cold hands → do not rub them together!
It cuts their skin from the inside out have them hold their hands under their armpits + separate the fingers
Active Rewarming
Heat water to between 100 and 105
Do not allow the limb to refreeze
Transport as soon as possible with the affected limb slightly elevated
Effects of Heat on the Body
Heat cramps or firefighter cramps
Heat exhaustion
Heat stroke (life-threatening emergency)
Stopped sweating
Water-Related Accidents
These may include:
Airway Obstruction
Cardiac Arrest
Signs of heart attack
Injuries to the head and neck
Generalized cooling, or hypothermia
Substance abuse
Drowning
Diving Accidents
Most diving accidents involve the head and neck, but you will also find injuries to the spine, hands, feet, and ribs in many cases.
Emergency care for diving-accident patients is the same as for all accident patients if they are out of the water.
An air embolism - more accurately called an arterial gas embolism (AGE) - is the result of gases leaving a damaged lung entering the bloodstream. These are most often associated with divers who hold their breath because of inadequate training, equipment failure, underwater emergency, or attempt to conserve air during a dive. Decompression sickness occurs when a diver comes up too quickly from a deep, prolonged dive. This takes 1 to 48 to appear, with about 90 percent of cases occurring within 3 hours of the dive.
Air Embolism (Rapid Onset - typically in less than 15 minutes - of Signs and Symptoms)
Frothy blood in the mouth or nose
Chest pain
Decompression Sickness ( 1 - to 12-Hour Onset of Symptoms)
Confusion, altered mental status, headache, visual disturbances, vertigo, nausea/vomiting, staggering gait.
Fatigue (may be extreme)
Pain in the muscles and the joints (the “bends”)
Itchy blotches or mottling of the skin
Numbness or paralysis
Choking, coughing, dyspnea, substernal pleuritic chest pain
Labored breathing
For this patient you should:
Maintain an open airway
Administer the highest possible concentration of oxygen by non rebreather mask.
Keep the patient warm
Position the patient either supine or on either side with the head down. Continue to monitor the patient.
Water Rescue
Reach
Throw and tow
Row
Go
Do not jump in the water after them!
Ice rescue
The number one rule in ice rescue is to protect yourself.
You can throw a flotation device to the patient.
Treat for hypothermia according to local protocols, and treat for any injuries.
High-Altitude Cerebral Edema
Headache that worsens over time
Loss of balance and coordination
Severe fatigue
Seizure
Altered mental status
Loss of consciousness
High-Altitude Pulmonary Edema
Tachypnea
Tachycardia
Middle fever up to 100.4
Respiratory failure and arrest
Bites and Stings
Those who are hypersensitive develop severe anaphylactic shock that is quickly life-threatening. Although all spiders are venomous, most species cannot get their fangs through human skin. The black widow spider and brown recluse, or fiddleback, spider are two that can , and their bites can produce medical emergencies.
Spider Bites
Symptoms:
Localized pain or itching
Numbness in a limb or body part
Burning sensations are the site followed by pain spreading throughout the limb
Redness
Headache and dizziness
Chills
Fever
Nausea and Vomiting
Muscle cramps, chest tightness, joint pain
Excessive saliva formation, profuse sweating
Anaphylaxis
Patient Care:
Treat for shock
Remove the stinger or venom sac
Remove jewelry from the patient’s affected limb
Keep the limb immobilized
Snake Bites
Symptoms:
Progressive general weakness
Vision problems (dim or blurred)
Nausea and vomiting
Seizures
Drowsiness or unconsciousness
Patient Care:
Remove any rings, bracelets, or other constricting items on the bitten extremity
Keep any bitten extremities immobilized - the application of a splint will help. Do not elevate the limb above the level of the heart
Transport the patient, carefully monitoring vital signs
Never suck the venom from the wound using your mouth
As a student, it is crucial to remember that snake bites can have severe consequences if not treated promptly and correctly. It is essential to act quickly and efficiently in providing care to the patient. Remember to stay calm and reassure the patient while following the necessary steps to ensure their safety. Additionally, always seek medical help as soon as possible to receive proper treatment and antivenom if required. By being knowledgeable and prepared, you can make a significant difference in the outcome for the patient.
As a student, it is crucial to understand the importance of staying updated on first aid protocols and procedures, especially when dealing with emergencies like snake bites. Continuous learning through courses, workshops, and practical training sessions can enhance your skills and confidence in handling such situations effectively. It is also essential to stay composed and focused during emergencies, as panicking can hinder your ability to provide timely and appropriate care. By staying informed, practicing regularly, and seeking guidance from experienced professionals, you can develop the necessary expertise to respond efficiently to medical emergencies and potentially save lives.