Animal Coordination, Control and Homeostasis
Unit 1: IVF
I. IVF: Development and Treatment Issues
1. Drawbacks of Fertility Treatment
Fertility treatment, while beneficial for many, presents several drawbacks that need to be considered:
a. Emotional and physical stress
Fertility treatment is often a last resort for individuals facing fertility issues, leading to heightened emotional strain.
Patients may invest significant hope in the treatment, intensifying the emotional toll.
b. Low success rates and cost
Fertility treatments come with no guarantee of success and can be financially burdensome.
The success rates of such treatments are relatively low, contributing to stress and disappointment.
c. Risk of Multiple births
Fertility treatments increase the likelihood of multiple births, such as twins or triplets.
Managing multiple births can be challenging for both the mother and the infants, adding to the complexity of the situation.
d. Ethical concerns
Unused embryos created during fertility treatment may be destroyed, raising ethical dilemmas regarding the potential for life.
Genetic testing of embryos before selection raises further ethical questions for some individuals.
II. Drugs, IVF, and AI for Infertility
1. Infertility
Infertility refers to the inability to conceive a child or carry a pregnancy to term after attempting to do so for a certain period. It can arise from various factors, including hormonal imbalances, structural issues, and medical conditions.
2. Treating Infertility
Addressing infertility involves several approaches:
a. Fertility Treatment Overview
Fertility treatment aims to enhance the chances of conception for individuals facing infertility issues.
Assisted Reproductive Technology (ART), including techniques like In Vitro Fertilization (IVF) and Artificial Insemination (AI), is commonly employed.
b. Risks and Side effects
Fertility treatments carry risks such as ovarian hyperstimulation syndrome (OHSS), multiple pregnancies, and birth defects.
Patients should discuss these risks with their healthcare provider before undergoing treatment.
c. Chances of success
Lifestyle modifications, stress management, and medical intervention can improve the success rates of fertility treatments.
Consulting with a fertility specialist experienced in treating specific types of infertility can also enhance success rates.
3. Fertility Drugs
a. FSH and LH
Fertility drugs containing Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH) stimulate egg maturation, facilitating fertilization.
These drugs are particularly useful for individuals who struggle to produce sufficient FSH for egg maturation.
b. Infertility drugs
Medications used to stimulate ovulation or regulate menstrual cycles, often in conjunction with other fertility treatments like IVF or AI.
4. In Vitro Fertilization (IVF)
a. Procedure overview
IVF involves fertilizing eggs with sperm in a laboratory setting before transferring resulting embryos into the uterus.
It is recommended for individuals with fertility issues involving blocked oviducts or sperm-related issues.
Strict eligibility criteria, including age and unsuccessful attempts at conception, are often applied.
b. Process steps
Stimulation of sex cell production with FSH and LH drugs. Fertilization of eggs with sperm in a lab.
Growth of fertilized eggs into embryos.
Implantation of selected embryos into the mother's uterus.
c. Success rate
The success rate of IVF varies depending on factors such as the age of the woman undergoing treatment, the cause of infertility, and the specific IVF clinic. On average, the success rate of IVF is estimated to be around 40-50% per cycle.
5. Artificial Insemination (AI)
a. Procedure overview
AI, often performed via intrauterine insemination (IUI), involves directly inserting sperm into the woman's uterus or cervix, circumventing fallopian tubes.
Hormone-containing fertility drugs may be used alongside this procedure.
b. Success rate
The success rate of AI varies based on factors such as the cause of infertility and the woman's age, averaging around 10-15% per cycle.
Unit 2: Hormonal Contraception: The Pill, Patches & Implants
I. Contraception
Contraception refers to interventions aimed at preventing pregnancy, which can be hormonal or non-hormonal.
Some interventions are used before sexual intercourse (e.g. condoms), whereas others may be used after fertilisation takes place (e.g. the pill).
The interventions can be hormonal or non-hormonal. Hormonal interventions involve targeting the reproduction hormones we discussed in the previous tutorial.
II. Hormonal Interventions
Target the reproductive hormones to prevent pregnancy.
Hormonal contraceptives are effective in preventing fertilization by altering the body's hormonal balance. However, they come with both positive and negative effects.
1. Positive Effects
Effective in preventing fertilization by altering the body's hormonal balance.
2. Negative Effects
Alterations in hormonal balance can lead to side effects such as weight gain, acne, changes in blood pressure, and mood changes.
III. Oral Contraceptives
Oral contraceptives, commonly known as the Pill, inhibit Follicle-Stimulating Hormone (FSH) production, thereby preventing egg maturation and ovulation.
IV. Progesterone
Progesterone-based contraceptives, available in various forms such as injections, implants, or slow-release patches, inhibit egg maturation and release.
V. Social Implications of Contraception
1. Side effects
Hormonal contraceptives may have side effects, which can vary from person to person.
2. Population control
Contraception plays a vital role in controlling the global population by reducing family sizes.
3. Prevention of STDs
Condoms, a form of contraception, help prevent the spread of Sexually Transmitted Diseases (STDs).
4. Ethical and Religious Considerations
Some individuals or religious groups may oppose the use of contraception on ethical or religious grounds.
Unit 3: Non-Hormonal Contraception
I. Barrier Methods
Barrier methods prevent fertilization by blocking the egg from fusing with the sperm.
1. Condoms
Placed on the penis, condoms prevent sperm from entering the female reproductive tract. They are about 95% effective and also provide protection against sexually transmitted infections (STIs).
2. Femidoms
Similar to condoms, femidoms are placed within the vagina to prevent sperm from passing through.
3. Diaphragms
Inserted into the vagina before sex, diaphragms cover the cervix to prevent sperm from entering. They are effective about 92-96% of the time but may increase the risk of infections like cystitis. They do not protect against STIs.
II. Intrauterine Devices
IUDs, also known as coils, prevent the implantation of an embryo into the uterus by releasing copper. This alters the chemical makeup of cervical mucus, making it more difficult for sperm to implant. They are fitted by a doctor or nurse and may lead to heavier periods.
III. Spermicidal Agents
Spermicides kill or disable sperm, preventing fertilization. While effective, some individuals may be allergic to them.
IV. Abstaining from Intercourse
Abstaining from intercourse during specific times of the menstrual cycle, such as when the egg is in the oviduct, can prevent fertilization. This method requires careful planning and tracking of fertility indicators like body temperature and cervical mucus production to determine fertile periods. Misjudging timing can increase the risk of pregnancy.
Unit 4: Hormonal Interactions in the Menstrual Cycle
Hormones work together in the menstrual cycle:
For example:
The release of FSH from the pituitary gland stimulates the release of oestrogen. High levels of estrogen then suppress FSH, creating a negative feedback loop.
Estrogen stimulates the release of LH when its levels are high, leading to the release of the egg cell.
Progesterone inhibits both LH and FSH. When estrogen and progesterone levels are high, the uterus is prepared for pregnancy. If fertilization doesn't occur, hormone levels drop. As estrogen and progesterone decrease, the inhibition of FSH ends, allowing a new follicle to be stimulated and initiating a new menstrual cycle.
Unit 5: Hormones
I. Menstrual Cycle
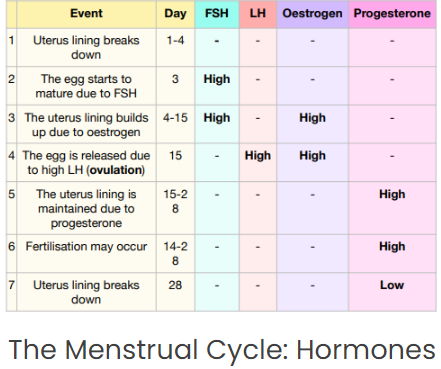
The menstrual cycle is the period during which an egg develops and is released, typically lasting around 28 days. It involves several hormonal changes and stages:
1. Uterus lining breaks down
This marks the beginning of the menstrual cycle, with the uterus shedding its lining over 3-4 days, resulting in bleeding.
2. Egg maturation due to FSH
Follicle-stimulating hormone (FSH) prompts the growth of follicles in the ovary, where egg cells mature.
3. Uterus lining builds up due to estrogen
Estrogen helps rebuild the uterus lining in preparation for the new egg.
4. Egg release due to high LH
High levels of luteinizing hormone (LH), triggered by estrogen, lead to ovulation, where the egg is released from the follicle.
5. Uterus lining maintenance due to progesterone
After ovulation, the follicle produces progesterone, which maintains the uterine lining for potential pregnancy.
6. Fertilization may occur
If fertilization occurs, the fertilized egg implants in the uterus lining, starting pregnancy.
7. Fertilization might not occur
If fertilization doesn't occur, progesterone levels drop around day 28, leading to the breakdown of the uterine lining, completing the cycle.
This table below corresponds with the 7 steps above. We have indicated where the hormone levels are high or low, but an empty box means that the levels are moderate (not zero).
II. Hormones during the Menstrual Cycle
1. Luteinizing Hormone (LH)
Released mainly during day 14
Produced by pituitary gland
Key in ovulation
Estrogen stimulates a surge in LH levels to cause release of the egg from the follicle
2. Follicle Stimulating Hormone (FSH)
Released mainly during days 2-3
Produced by pituitary gland
Key in egg maturation
It stimulates the egg to mature in the follicle
3. Estrogen
Released mainly during days 4-15
Produced by ovaries
Key in growing uterus lining (endometrium)
It helps the uterus lining grow and develop
Key in ovulation
Estrogen stimulates a surge in LH (and fall in FSH) to cause release of the egg from the follicle
4. Progesterone
Released mainly during days 15-27
Produced by follicle in the ovaries
Key in maintaining uterus lining (endometrium)
It prevents breakdown of the uterus lining from day 15 onwards
Key in the end of the menstrual cycle
The fall in progesterone at day 28 leads to the breakdown of the uterus lining
III. Hormones during Pregnancy
FSH and LH are inactive.
Estrogen and progesterone levels remain high to maintain the uterus lining and stimulate breast growth and milk duct development.
The placenta also produces estrogen and progesterone.
IV. Hormones in Human Reproduction
Hormones are chemical messengers that regulate various processes in the human body, including reproduction.
V. Hormonal Imbalances
Hormonal imbalances can disrupt the menstrual cycle by altering hormone levels, leading to irregular periods or other related issues.
Unit 6: Puberty and Hormones
I. Reproductive Hormones
Reproductive hormones are crucial for reproduction, driving the process entirely. They play various roles in growth, puberty, and fertility.
1. Changing during Adolescence
During adolescence, reproductive hormones lead to significant changes, marking the transition to adulthood:
a. Secondary sex characteristics
Hormones trigger the development of secondary sex characteristics, distinguishing between genders but not directly involved in reproduction.
b. Production of sex cells
Hormones stimulate the production of sex cells—sperm in males and eggs in females—essential for reproduction.
2. Testosterone in Males
Testosterone, the primary male reproductive hormone, is produced in the Leydig cells of the testes. During puberty, it brings about several changes:
Increased hair growth on face, body, pubic area, and underarms
Muscle growth
Deepening of voice
Onset of sperm production
Development of penis and testes
3. Estrogen in females
Estrogen, the main female reproductive hormone, is produced in the ovaries. It also exists in small amounts in males. During puberty, estrogen induces numerous changes in females:
Increased growth of underarm and pubic hair
Development of sexual organs
Formation of breasts
Widening of hips
Slight deepening of voice
Additionally, estrogen triggers ovulation, the release of an egg from the ovaries. This marks the beginning of the menstrual cycle, a 28-day process where eggs mature, culminating in the release of one egg into the fallopian tube.
Unit 7: Kidney Transplantation
I. Kidney Donation
Kidney transplants represent the sole cure for kidney disease. A healthy kidney is obtained from a consenting donor, either living or deceased, who has indicated their willingness to donate through a donor card or registration.
II. Organ Rejection
Rejection of the donated kidney by the recipient's body is possible due to immune system recognition issues. The recipient's immune system may perceive the transplanted kidney as foreign and produce antibodies that attack it. Measures to prevent rejection include finding a closely matched tissue type and administering immunosuppressive drugs to suppress the immune response.
Unit 8: Osmoregulation & The Kidney
I. Osmoregulation
The process by which organisms regulate the balance of water and solutes in their bodies to maintain a stable internal environment.
The Kidney plays a key role in Osmoregulation by filtering waste and excess fluids from the blood and regulating the balance of water and electrolytes in the body.
II. Kidney Failure
Kidney failure results in the accumulation of toxins within the body due to the kidney's inability to filter waste products. Treatment options, such as kidney transplant or dialysis, become necessary when both kidneys are impaired.
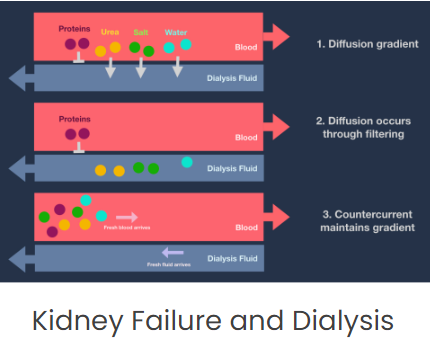
III. Dialysis Machines
Dialysis, the standard treatment for kidney failure, involves the use of a machine to artificially filter blood outside the body. This process aims to balance salt and glucose concentrations through the following steps:
1. Blood Extraction
Unfiltered blood is withdrawn from the patient's arm and mixed with thinning agents to prevent clotting.
2. Filtration
The blood is directed into a dialysis machine, featuring a circuit for blood and surrounding dialysis fluid separated by a semi-permeable membrane mimicking the nephron.
3. Waste Removal
Waste products, including ions, water, and urea, diffuse from the blood into the dialysis fluid, while glucose levels are maintained for cellular respiration.
4. Countercurrent System
Blood and dialysis fluid flow in opposite directions, facilitating diffusion by maintaining a concentration gradient. For example, urea moves from blood to dialysis fluid due to the concentration gradient.
III. Negatives of Dialysis
Although dialysis serves as a temporary solution until kidney transplantation, it presents several drawbacks:
1. Painful procedure
Dialysis is a painful process that significantly impacts the patient's quality of life.
2. Inconvenience
Patients must undergo dialysis sessions 2-3 times weekly for 4-6 hours, necessitating frequent hospital visits.
3. Dietary restrictions
Patients must adhere to strict dietary restrictions to prevent excess intake of amino acids or salts, which can elevate urea levels.
Unit 9: Anti-Diuretic Hormone
I. Functions
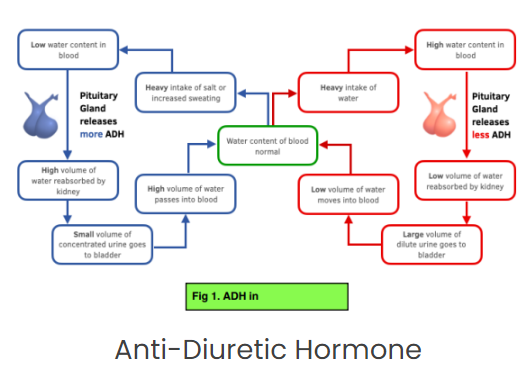
ADH, also known as vasopressin, is released by the pituitary gland and primarily targets the kidneys. It plays a crucial role in water control within the body through a negative feedback mechanism. The brain detects changes in water levels in the blood and regulates ADH release accordingly. ADH affects the permeability of kidney tubules, increasing water reabsorption and reducing water excretion.
II. ADH in Dehydration
During dehydration:
The pituitary gland releases more ADH due to increased plasma concentration.
Kidney tubules become more permeable to water, leading to increased water reabsorption.
Urine becomes less dilute.
III. ADH in Over-Hydration
During over-hydration:
Less ADH is released as the plasma concentration decreases.
Kidney tubules become less permeable to water, resulting in reduced water reabsorption.
Urine becomes more dilute.
IV. ADH in Special States
1. Alcohol
Alcohol decreases ADH production, leading to more dilute urine and dehydration.
2. Urea concentration
Urea concentration remains constant in urine during changes in water content.
V. Bodily Changes Cause Urine Composition to Change
Urine composition and concentration can change due to osmotic challenges or temperature changes:
1. Sweating
Dehydration from sweating triggers increased ADH release, resulting in more concentrated urine. Thirst signals are also activated to encourage water intake.
2. Over-drinking
Over-hydration reduces ADH release, leading to more diluted urine.
3. High salt intake
Higher salt intake increases salt excretion, producing concentrated urine.
VI. Too much ADH
Can cause water retention and swelling.
VII. Too little ADH
Results in excessive urination and dehydration.
VIII. Regulating ADH
ADH release is regulated by the body's thirst and water balance mechanisms, responding to changes in water and electrolyte concentration.
IX. Factors affecting ADH levels
ADH levels can be influenced by factors such as stress, illness, and certain medications.
X. ADH imbalances
Imbalances in ADH levels can lead to health issues like diabetes insipidus or edema, emphasizing the importance of regular monitoring and appropriate treatment.