Rare pupil anomalies (PT3)
Other Pupil Anomalies
LIGHT-NEAR DISSOCIATION:
The afferent pathway for the pupil near reflex is different from the afferent pathway for the pupil light reflex.
Some patients may present with anomalous reactions to light but a normal near response.
Examples include Argyll Robertson pupils, Dorsal mid-brain syndrome, and amaurotic pupils.
Argyll Robertson Pupils
Bilateral, irregular, miotic pupils (small pupils) where the light reflex is absent, but the near reflex is preserved.
In dim light, both pupils are small and may be irregular.
In bright light, neither pupil constricts, but on accommodation (focusing on a near target), both constrict.
Cause: A midbrain lesion that interrupts the pupillary light reflex pathway but spares the more ventral pupillary near reflex pathway.
Commonly caused by neurosyphilis.
Other possible causes include diabetes and alcoholism.
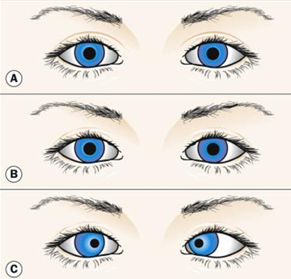
A - dim illumination, B - bright illumination, C - near work
Characteristics:
Absent light reaction.
Small pupils in ambient light.
Brisk reaction preserved to accommodation.
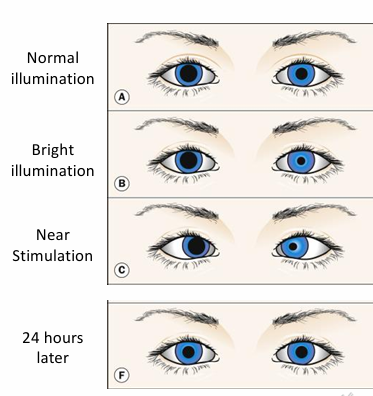
Dorsal Midbrain Syndrome
Light-Near Dissociation occurs when afferent pupil fibers are affected in the midbrain (pretectal) area.
Light reaction may be diminished or lost, while the near reaction is maintained.
Pupils tend to be mid-sized or dilated and frequently unequal.
Normal near reflex but no light reflex bilaterally.
May be associated with impairment of upgaze due to damage of the vertical gaze center and convergence retraction nystagmus.
Causes:
Pineal tumor (pinealoma).
Hydrocephalus, meningitis.
Stroke or multiple sclerosis.
Amaurotic Pupils (Absolute Afferent Pupil Defect)
Caused by a complete optic nerve lesion where the involved eye is completely blind (i.e., no light perception).
Both pupils are of equal size.
No light reaction occurs when the affected eye is stimulated.
Both pupils react normally when the contralateral normal eye is stimulated.
Reaction of both pupils to near is normal.
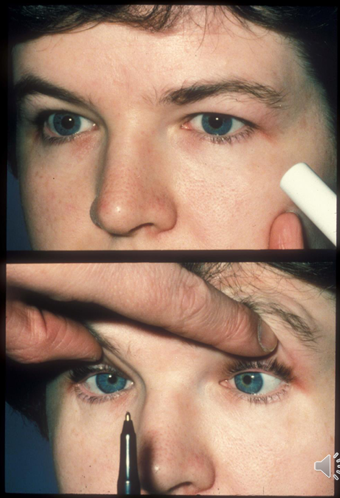
Benign Episodic Unilateral Mydriasis
Uncommon cause of intermittent/transient anisocoria (unequal pupil sizes).
Isolated benign, idiopathic cause of pupil asymmetry.
Most common in young adult females.
Often associated with a migraine attack, or patients may have a history of past migraines.
May be due to:
Parasympathetic insufficiency.
Sympathetic hyperactivity.

Parasympathetic Form:
Pupil enlarged and poorly reactive.
Poor reaction of dilated pupil to light and near stimuli.
Reduced accommodation.
No ocular motor dysfunction or ptosis.
Duration is typically 15 minutes to several hours.
Sympathetic Form:
Pupil transiently enlarged.
Pupil may be distorted (tadpole pupil) due to a segmental spasm of the iris dilator.
Brisk reaction to light, normal accommodation.
Often asymptomatic.
Possibly blurred vision, increased light sensitivity.
Duration is typically 15 minutes to several hours.
