Hypertension
what is hypertension?
raised blood pressure
Systolic >140MM Hg
160mm Hg in isolated systolic hypertension
Diastolic >90mm Hg
THIS IS NOT AN INDIVIDUAL MEASUREMENT AS WHAT IS CATASTROPHIC FOR ONE IS HEALTHY FOR ANOTHER - EACH INDIVIDUAL IS DIFFERENT
Hypertension measurement
Hypertension is measured using 3 separate measurements at 3 separate times, sitting & rested for roughly 15mins to get a view of BP over time and under moderate standardised conditions.
Important to note that medicine is considering that dynamic BP and mean arterial pressure is more useful than the systolic and diastolic which changes momentarily - for that reason ambulatory BP monitoring devices are given to pat to wear over 24 or 72hrs to allow doctor to see how BP changes in a range of different settings.
Known risk factors for hypertension
age - increase with age
race
Obesity - increase BP
Alcohol - increase BP
family history - genetics
Pregnancy - complicate pregnancies
stress
drugs - non steroidal, corticosteroids, oral contraceptives, sympathomimetics
Hypertension is difficult to define and will vary from person to person.
Disease outcome linked to hypertension
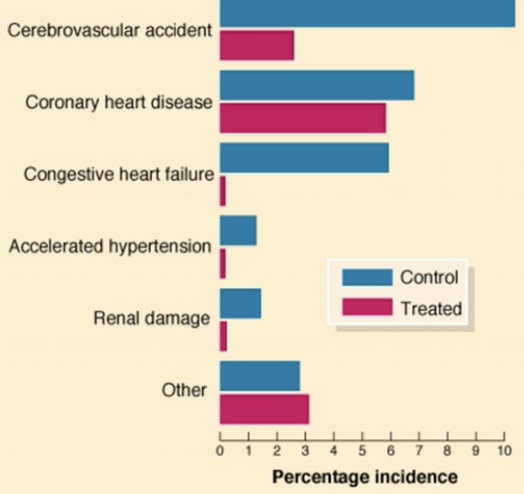
Diagram shows the biggest risk from uncontrolled hypertension is CVA or stroke, second is coronary heart disease, then congestive heart failure.
Treatment for coronary heart disease has little benefit to the pat risk whereas in heart failure there is a significant improvement in risk when treating the hypertension.
Coronary heart disease (atherosclerosis) which causes pat to have a heart attack is a low and long process, therefore if pat has had hypertension for 10+ years before diagnosis then reversing the pressure will not reverse the atherosclerotic changes that have built up in the blood vessels - therefore risk will remain
CVA is directly related to pressure.
risk of having a heart attack from high blood pressure is related to the duration of hypertension and not directly to the pressure itself. Therefore, it is not reversible by treating the blood pressure.
Heart failure is very quickly improved by treating the hypertension as it reduces the work load of the heart. therefore, making muscle more able to cope.
Outcome from Hypertension
ACCELERATED ATHEROSCLEROSIS
Myocardial infraction (heart attack)
stroke
peripheral vascular disease
RENAL FAILURE - which increases hypertension
Why do people get hypertension
Common triggers included:
essential hypertension- non usually found as it is most likely genetic changes interacting with the pat environment
genetic failure of auto regulation control of blood vessel wall constriction
Rare triggers include:
renal artery stenosis
endocrine tumours - pheochromocytoma (adrenaline - vasoconstriction), cronns’ syndrome (aldosterone - increases circulating blood volume), cushings syndrome (cortisol - increases circulating blood volume)
Signs and symptoms
usually none
Headache - unusual and more common in ‘malignant hypertension where BP is rapidly accelerating
Transient ischaemic attacks - TIA (mini stroke), full neurological return in 24hours
Indication for further indication
patients with hypertension are normally 40+ therefore unusual:
young patient (20/30years)
resistant hypertension despite ‘adequate’ treatment
accelerated hypertension
‘unusual history’
Pheochromocytom
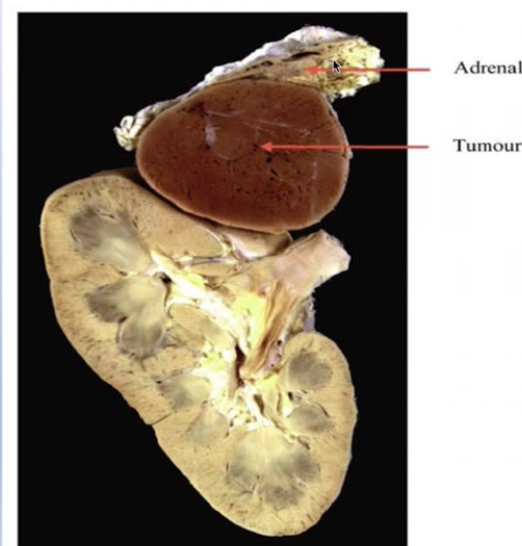
Diagram shows andranergic tumour (tumour on the adrenal gland) releasing adrenaline into the circulation causing vasoconstriction and hypertension.
adrenal is in the region of the kidneys but it is not considered a renal disease.
Cushing’s syndrome
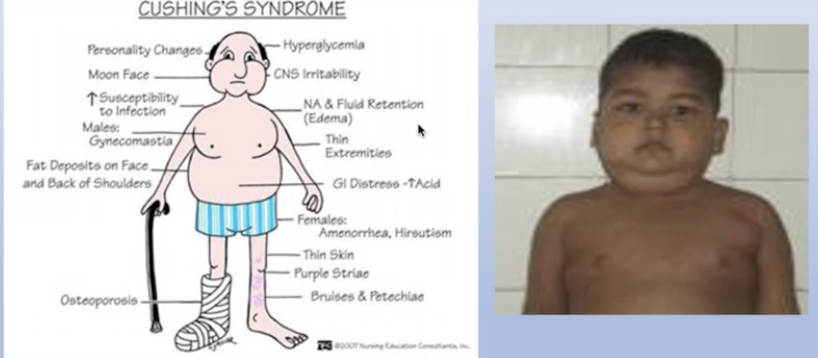
diagram shows pat with salt and water retention which leads to excess fluid within the circulation.
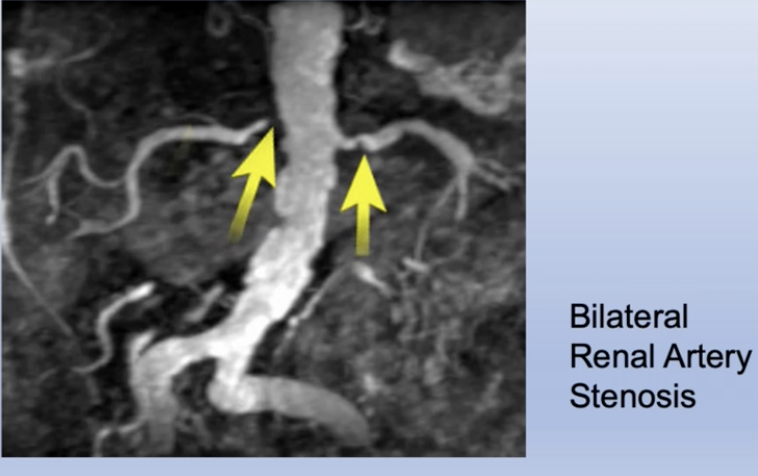
Renal Artery Stenosis
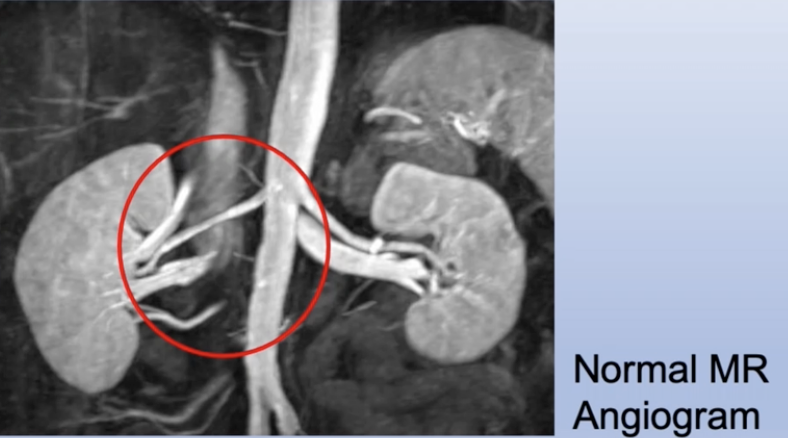
diagram shows a narrowing of Blood flow into the kidneys making the auto regulation system think blood pressure has dropped due to hypokalemia. Therefore, body will release renen and through the renen antigen system aldosterone will be released and salt and water will be retained.
 Investigations
Investigations
Urinalysis
serum biochemistry (electrolytes, urea & creatinine)
serum lipids
ECG
Renal ultrasound, angiography & hormone estimations (cortisol/adrenaline levels) - occasionally
Treating hypertension
aim of treatment - BP <120/90mm Hg
modify risk factors - weight loss/exercise
single daily dose improves compliance with medicine (side effects)
- Thiazide diuretic (GOUT)
- Beta blocker (COPD & asthma)
- Calcium channel antagonist (gingival hyperplasia)
- ACE inhibitors (Peripheral Vascular Disease)
add multiple drugs if needed for control
Monitoring
treatment will need change over time - review 2/3 months until adequate regime is found then annually when patient is stable
Particularly important in the elderly
monitor blood biochemistry effects of drugs - dehydration, Thiazide diuretic drug can affect sodium & potassium changes and if left to extreme circumstances can affect cardiac conduction and ECG