Gastrointestinal Conditions in Children
Gastrointestinal Conditions in Children
Chapter 28: Overview of the Gastrointestinal (GI) Tract
The GI tract functions to transport and metabolize nutrients required for cellular life.
It extends from the mouth to the anus.
Nutrients are broken down into absorbable products by enzymes released from various digestive organs.
Structure of the Gastrointestinal System
Components of the GI System:
Oral cavity
Pharynx
Esophagus
Stomach
Small intestine
Large intestine
Rectum
Anus
Liver
Pancreas
Gallbladder
Developmental Considerations
At birth, a newborn's intestinal tract has incomplete resistance to bacterial and viral infections.
As children grow, their nutritional, metabolic, and energy needs increase.
Children with symptoms like nausea and vomiting can become dehydrated more quickly than adults.
An infant's stomach is small and empties rapidly.
Newborns produce very little saliva until approximately 3 months of age.
Swallowing during the first 3 months is primarily reflexive.
Hepatic function in newborns is immature, often leading to jaundice.
Infants have poor fat absorption due to a limited supply of bile acids.
Clinical Laboratory Evaluations
Necessary tests for GI conditions include:
CBC with differential
Erythrocyte sedimentation rate (ESR)
Comprehensive chemistry panel
Liver function tests
Stool cultures
Imaging studies such as GI series, barium enema, and abdominal X-rays (upper, lower, or entire) and endoscopy are also utilized.
Symptoms of GI Disorders
Systemic Signs:
Failure to thrive (FTT): Failure to develop according to the established growth parameters.
Pruritus: Itching without allergy, potentially indicating liver dysfunction.
Local Signs:
Pain
Vomiting
Diarrhea
Constipation
Rectal bleeding
Hematemesis
Congenital Disorders
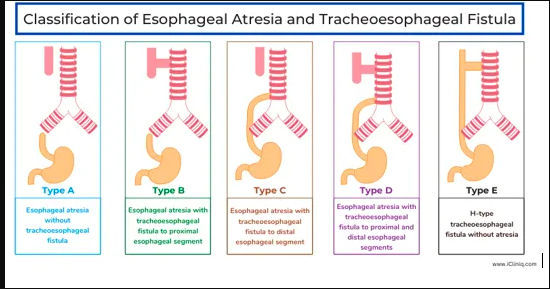
Esophageal Atresia and Tracheoesophageal Fistula (TEF)
TEF is caused by improper separation of GI tract tissues during prenatal development.
Types of TEF:
Type A: Upper esophagus ends in a blind pouch; lower esophagus connected to the trachea.
Type B: Both upper and lower esophagus end in blind pouches.
Type C: Upper esophagus connected to the trachea; lower esophagus also attaches to the trachea.
Type D: Upper esophagus connects to the trachea; lower esophagus ends in a blind pouch.
Manifestations of Tracheoesophageal Fistula
Earliest Sign: Development of polyhydramnios in the mother.
If ending in a blind pouch, the fetus fails to swallow amniotic fluid, causing accumulation.
Upon birth, infants vomit and choke upon first feeding.
Drooling may occur at birth, related to atresia.
If the upper esophagus connects to the trachea, initial feeding can enter the trachea, leading to:
Coughing
Choking
Cyanosis
Apnea
If the lower esophagus connects to the trachea, air may enter the stomach with each breath, causing abdominal distention.
Nursing Care for Tracheoesophageal Fistula
Aim to prevent pneumonia, choking, and apnea during newborn care.
Assess for signs of TEF during the first feeding; use clear water or colostrum for feeding to minimize aspiration risks.
Surgical repair is critical for survival.
Imperforate Anus
Develops due to failure in the perforation of the lower GI tract during fetal development.
Manifestations:
Failure to pass meconium within the first 24 hours.
Presence of stool in the urine or vagina.
Difficulty passing a rectal thermometer.
Treatment:
Prepare the infant for surgery when stable; initial procedures may involve colostomy.
Pyloric Stenosis
An obstruction at the stomach's lower end resulting from muscle overgrowth or spasms.
Typically diagnosed around 2-3 weeks of age.
Symptoms:
Projectile vomiting; may lead to metabolic alkalosis due to hydrogen ion depletion, decreased serum K & Na levels, increased pH, bicarbonate, and decreased chloride levels.
Constant hunger post-vomiting.
Dehydration and possible presence of olive-shaped mass in the upper right abdomen.
Interventions:
Use of thickened formula; burp during feedings.
Slow feeding while positioned on the right side to facilitate feeding weight against the pyloric valve.
Pyloromyotomy is the standard treatment.
Celiac Disease
Also known as gluten enteropathy or sprue, it is the leading malabsorption issue in children.
Often genetically predisposed with environmental triggers.
Symptoms typically emerge between 6 months and 2 years, post-introduction of gluten-containing foods (wheat, barley, oats, rye).
Classifications:
Classic: Villous atrophy, malabsorption, diarrhea, abdominal pain.
Atypical: Mild GI symptoms, manifests as anemia, fatigue, peripheral nerve problems.
Silent: Intestinal atrophy diagnosed via endoscopy or biopsy without symptoms.
Latent: May lack atrophy but exhibits signs of wheat sensitivity (e.g., recurring rash).
Symptoms in the Infant:
Failure to thrive (FTT).
Irritability.
Large, bulky, profuse diarrhea with fat traces.
Diagnosis:
Confirmed by serum immunoglobulin A (IgA) and small bowel biopsy.
Treatment:
Strict, lifelong gluten restriction (wheat, barley, oats, rye).
Parental education by nutritionists is crucial.
Hirschsprung Disease (Aganglionic Megacolon)
Characterized by the absence of ganglionic innervation in a bowel segment, leading to constipation and bowel dilation proximal to an obstruction.
More prevalent in males and children with Down syndrome.
Symptoms:
Newborns may show failure to pass meconium within 24 to 48 hours.
Infants may present with ribbon-like stools, foul-smelling stools, abdominal distention, anorexia, vomiting, FTT.
Diagnostics:
Barium enema, rectal biopsy, anorectal manometry.
Surgery:
Aimed at removing the affected colon section, may require colostomy.
Intussusception
Defined as a slipping of one intestinal segment into another, frequently at the ileocecal junction.
Involves pulling of the mesentery, leading to edema and potentially strangulation.
Symptoms:
Severe abdominal pain, drawing legs to abdomen, bilious vomiting, diminished bowel movements, and currant jelly stools (blood and mucus).
Emergency Situation:
Diagnosis from history/physical; ultrasound-guided hydrostatic reduction is preferred treatment.
Meckel Diverticulum
Common congenital GI malformation associated with a fibrous cord connected to the umbilicus.
Symptoms may appear as painless rectal bleeding, typically diagnosed in children by age 2.
Diagnostics:
Barium enema or radionuclide scintigraphy for diagnosis.
Treatment:
Surgical removal of the diverticulum.
Hernias
Types:
Inguinal: Abdominal contents through the inguinal canal.
Umbilical: Portion of the intestine protrudes through the umbilical ring, presenting as a skin-covered swelling.
Can be congenital or acquired.
Classification: Reducible (can return to place) vs. irreducible (incarcerated) vs. strangulated (compromised blood flow).
Strangulated hernias mandate urgent surgical intervention.
Disorders of GI Motility
Gastroenteritis
Involves inflammation of the stomach and intestines, with colitis referring specifically to colon inflammation.
Common non-infectious diarrhea causes include food intolerance, overfeeding, improper formula preparation, and excessive sorbitol consumption.
Priority care focuses on restoring fluid and electrolyte balance.
Vomiting
Characterized by involuntary contraction of diaphragm and stomach muscles. Persistent vomiting may lead to dehydration and electrolyte imbalances.
Nursing Care:
Monitor feeding practices; place the infant on the side post-feeding to prevent aspiration.
IV fluids may be necessary, and documentation of vomiting characteristics is crucial.
Gastroesophageal Reflux
Resulting from a relaxed or incompetent lower esophageal sphincter, allowing stomach contents to ascend into the esophagus.
Often linked with neuromuscular delays and more prevalent in preterm infants.
Symptoms typically subside with upright positioning and solid food introduction.
Management:
Focused on careful feeding techniques, preventing overfeeding, and medication to relax the pyloric sphincter.
Diarrhea
Defined as an unexpected increase in stool frequency, often fluid-like and colored abnormally (green/mucous/bloody).
Acute cases arise mainly from inflammation and infections, while chronic diarrhea may indicate malabsorption.
Symptoms: Watery stools, weight loss, dehydration signs (sunken eyes, dry tongue), and potential acidosis.
Constipation
Defined as troublesome or infrequent defecation with hard fecal masses. Potentially seen with encopresis (fecal soiling).
Dietary factors, cultural influences, and psychological issues may contribute.
Assessment should include stool frequency, color, and consistency; dietary adjustments may involve increasing fiber-rich foods.
Fluid and Electrolyte Imbalance
Younger children are particularly susceptible to dehydration due to greater surface area and metabolic rate.
Evaluating hydration status is vital as signs and treatment vary. Types of dehydration are classified as isotonic, hypotonic, and hypertonic.
Nutritional Deficiencies
Failure to Thrive (FTT)
Characterized by insufficient weight gain and potential weight loss. Causes may be organic (OFTT - e.g., heart defects) or non-organic (NFTT - such as environmental neglect).
Manifestations may include irritability, feeding disturbances, and developmental delays.
Nursing efforts should focus on support and care to achieve developmental milestones and parental education.
Specific Nutritional Conditions
Kwashiorkor: Severe protein deficiency amid calorie adequacy, prevalent in developing nations.
Rickets: Result of vitamin D deficiency, leading to skeletal malformations and requires sunlight exposure and supplementation for treatment.
Scurvy: Caused by a lack of vitamin C, presenting with joint pain, gum issues—and treated with dietary correction and supplements.
Lead Poisoning (Plumbism)
Resulting from chronic lead exposure, particularly in older urban housing.
Symptoms can progress to neurological deficits if untreated, necessitating environmental interventions and potential chelation therapy.
Foreign Bodies Ingestion
Common in children ages 6 months to 3 years with most items passing through the GI tract uneventfully.
Parents should be advised against laxatives and encouraged to maintain normal diets to alleviate discomfort.
Note: All clinical evaluations and interventions should be based on ongoing assessments and tailored to each child's specific needs, emphasizing safety first in any treatment approach for pediatric gastrointestinal conditions. This involves consistent follow-up and education for caregivers.
Dehydration
▪Causes fluid and electrolyte disturbances - Assessment of fluid balance is the first action to determine severity.
▪Evaluation of type and severity, including clinical observation and chemical analysis of the blood
▪Types of dehydration are classified according to level of serum sodium, which depends on the relative losses of water and electrolytes.
▪ Isotonic
▪ Hypotonic ▪ Hypertonic
Overhydration
The body receives more fluid than it can excrete.
▪ Manifests as edema (excess fluid in interstitial spaces)
▪ Interstitial fluid is similar to plasma but contains little protein
▪ Any factor causing sodium retention can cause edema.
▪ Flow of blood out of the interstitial
compartments depends on adequate circulation of blood and lymph.
▪ Low-protein levels disturb osmotic cellular pressure.
▪ Anasarca is severe generalized edema
Appendicitis:
Most common reason for emergency abdominal surgery
▪ Small appendage arising from the cecum
▪ Lumen may become obstructed with fecal matter or with lymphoid tissue after a viral illness or with parasites
▪ Stasis, increased swelling, edema, and growth of organisms
▪ Initial pain usually in periumbilical and increases within a 4-hour period.
Sudden relief can be an early indication of appendix rupture.
▪ When inflammation spreads to peritoneum, pain localizes in RLQ of abdomen b/n umbilicus and iliac crest at Mc Burney’s point.
▪ Appendix may become gangrenous or rupture.
▪ Can lead to peritonitis and septicemia
Thrust ( Oral Candidiasis)
Usually caused by a fungus, Candida
▪ Anorexia may be present.
▪ Systemic symptoms are generally mild if infection remains in the mouth; can pass into GI tract, causing inflammation of the esophagus and stomach
▪ Responds well to local application of antifungal suspension, such as nystatin
▪ Medication should remain in contact with “patches” as long as possible. Use a sterile applicator to swab on the oral mucosa.
▪ With proper care, the condition disappears within a few days after onset.
Incidence higher in inner-city tenements d/t deteriorating paint in older buildings.