5: Ocular Manifestations of Systemic disease - Thyroid Eye disease
Thyroid Hormone Synthesis and Regulation
Iodine is converted into thyroid hormones T4 (thyroxine) and T3 (tri-iodothyronine).
Iodine is combined with tyrosine to make T4 and T3.
A normal thyroid gland produces about T4 and T3.
Regulation by the pituitary via thyrotrophin (thyroid-stimulating hormone, TSH).
The pituitary is regulated by the hypothalamus via thyrotropin-releasing hormone (TRH).
Graves’ Disease: Overview
Autoimmune disorder resulting in hyperthyroidism and excessive T4 (and T3).
Systemic manifestations: weight loss, tremor, increased sweating, heat intolerance, tachycardia, palpitations, atrial fibrillation, muscle wasting, nervousness, irritability.
Epidemiology: more common in women aged .
Characterised by goitre (enlarged thyroid) and ophthalmopathy.
Eye signs can occur without systemic manifestations (Ophthalmic Graves’ disease or euthyroid Graves’).
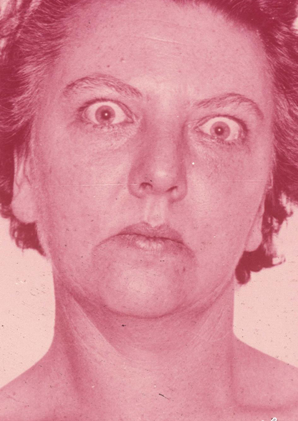
Ocular Signs of Graves’ Disease
Upper lid retraction (Dalrymple’s sign) → overactive mullers muscle or swollen levator muscle.
Staring frightened appearance (Kocher’s sign).
Lid lag on downgaze (von Graefe’s sign).
Imperfect convergence (Mobius’ sign).
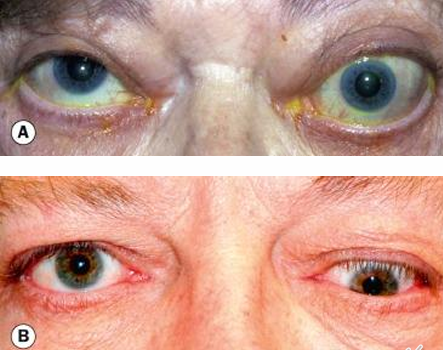
Proptosis (due to inflammation of EOMs).
Conjunctival injection and chemosis.
Corneal exposure with dryness, ulceration, and potential vision loss.
Eyelid edema.
Lacrimation, photophobia, foreign body sensation, retrobulbar discomfort.
May also exhibit Superior Limbic Keratoconjunctivitis (SLK).
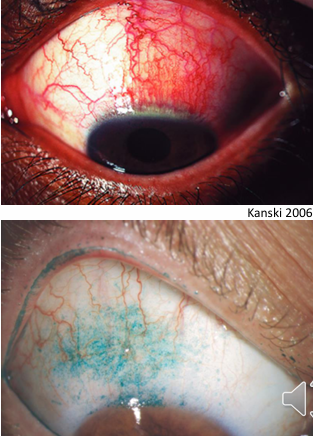
Superior Limbic Keratoconjunctivitis (SLK)
Chronic condition affecting the superior limbus with bulbar and tarsal conjunctiva.
About of sufferers have hyperthyroidism.
Likely due to mechanical effects of the upper lid on the superior bulbar conjunctiva.
Symptoms: chronic irritation, foreign body sensation, burning.
Signs:
red papillae on the upper lid
hyperaemia and staining of the superior bulbar conjunctiva
superior punctate corneal staining
pannus if longstanding.
Treatment:
ocular lubricants
short course of steroids (e.g., FML QID).
Restrictive Thyroid Myopathy
Hyperthyroidism features enlargement of EOMs and increased orbital fat volume.
In TED, 30–50% of patients develop ophthalmoplegia.
Mechanism: inflammation of EOMs with fibrosis in longstanding disease; one or more EOMs are tight.
Symptom: diplopia.
Most common sign: elevation defect (fibrotic defect of inferior rectus, mimicking superior rectus palsy).
Next most common defect: abduction defect (fibrotic medial rectus, mimicking sixth nerve palsy).
Depression defect (fibrosis of superior rectus).
Adduction defect (fibrosis of lateral rectus).
Least commonly involved muscles: the obliques.
Dysthyroid Optic Neuropathy (DON)
Seen in roughly of Graves’ disease cases.
Mechanism: direct compression of the optic nerve or its blood supply at the orbital apex by congested EOMs.
Optic neuropathy can occur with minimal or no proptosis.
Clinical features: slow vision loss, relative afferent pupillary defect (RAPD), colour loss, any pattern of visual field loss.
Fundus findings: vascular congestion, swelling of the optic disc, and choroidal folds.


Treatment of Graves’ Ophthalmopathy and Thyroid Disease
Thyroid dysfunction management:
Anti-thyroid drugs: carbimazole, methimazole, propylthiouracil.
Radioactive iodine therapy.
Thyroidectomy.
Major risk factor for developing TED (and progression to more severe disease) in Graves’ disease: smoking.
Eye disease management:
Smoking cessation.
If mild ocular surface problems: lubricants, ointment at night, and lid taping.
Head elevation at night and cold compresses during the day to reduce lid oedema.
More severe disease: systemic steroids.
Optic neuropathy:
high-dose oral prednisolone (sometimes intravenous).
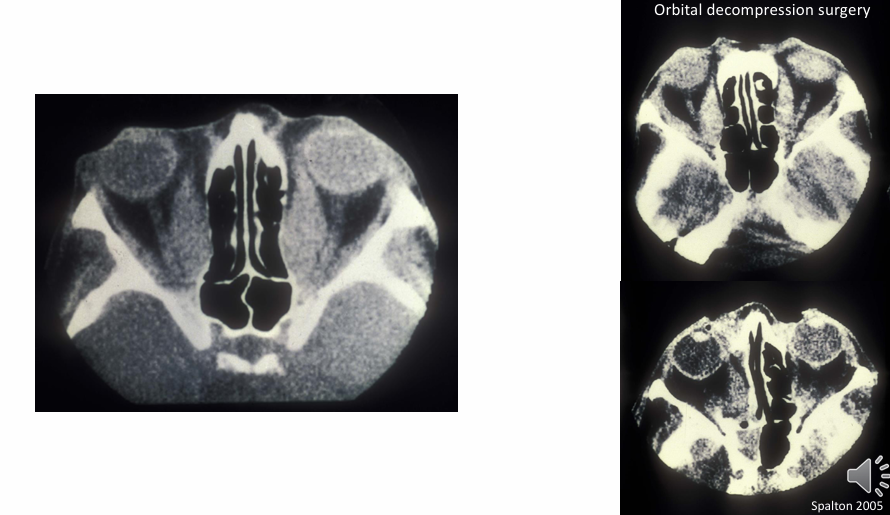
Orbital decompression surgery.
Radiotherapy.
Orbital Decompression Surgery
A therapeutic option for severe TED
makes more room for muscles to sit within the orbit
Hypothyroidism
Reduced thyroid secretion; can be autoimmune or after thyroidectomy.
Epidemiology: most common in middle-aged women.
Clinical features: slowing of body processes (lethargy, sluggishness), reduced cold tolerance, lack of sweating, weight gain.
Physical signs: dry scaly skin, brittle hair and nails, loss of the outer one-third of the eyebrows, swollen eyelids and tongue, swollen ankles.
May have tear deficiency leading to keratoconjunctivitis.
Possible retrobulbar neuritis and optic atrophy.
Treatment: thyroid hormone supplementation typically results in dramatic improvement.