Lung Resistance and Neonatal Distress
Learning Objectives
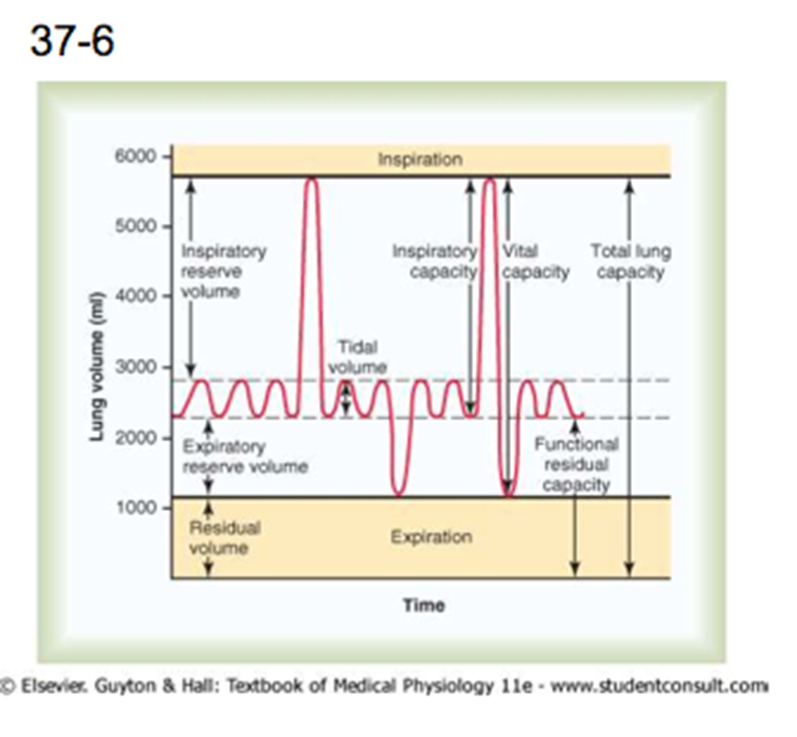
•Describe the volume (V) and pressure (P) changes in the respiratory cycle and the PV relationship
•Compare ‘compliance’ and ‘elastance’ in terms of definition, mathematical calculation, and relevance to the respiratory system
•Describe pressure-volume curve, relate this to the work of breathing and explain influential factors and their consequences on the curves
•Explain types of respiratory resistance
•Describe the composition and secretion of surfactant and explain its physiological benefits
•Define neonatal respiratory distress syndrome and describe causations, pathogenesis, signs and symptoms and aim of treatment regimes
Airway Resistances
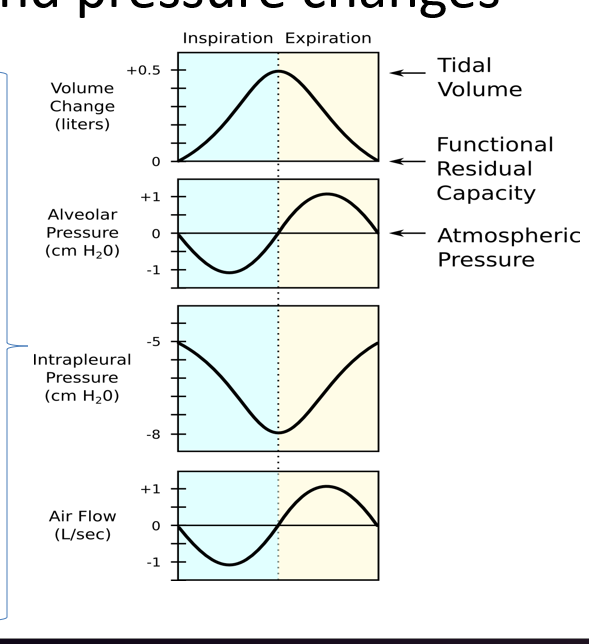
Volume and Pressure Changes
Respiratory muscles initiate changes in the intrapleural pressure which sets up a partial pressure gradient and enables air to flow.
1cm diaphragm movement creates a change in 3cm H20 which is enough.
The more muscular effort the more work.
Ideally the lungs would be ‘stretchy’ to allow inflation.
Breathing work
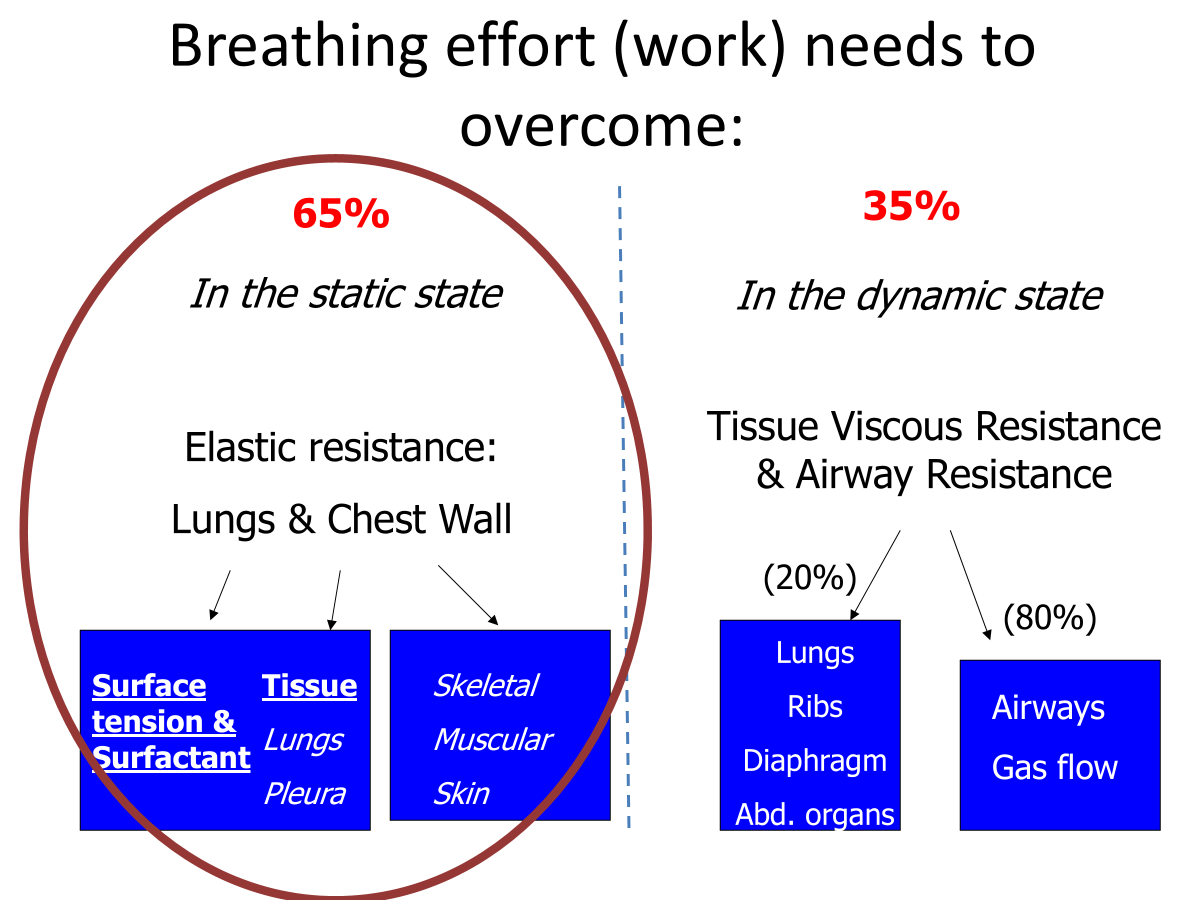
Elastic work: Physical tendency of an object to resist stretching.
Elastic and collagen in lung parenchyma.
Resting position for lungs is to recoil inwards.
Dynamic: Only when the system is in motion and air is moving.
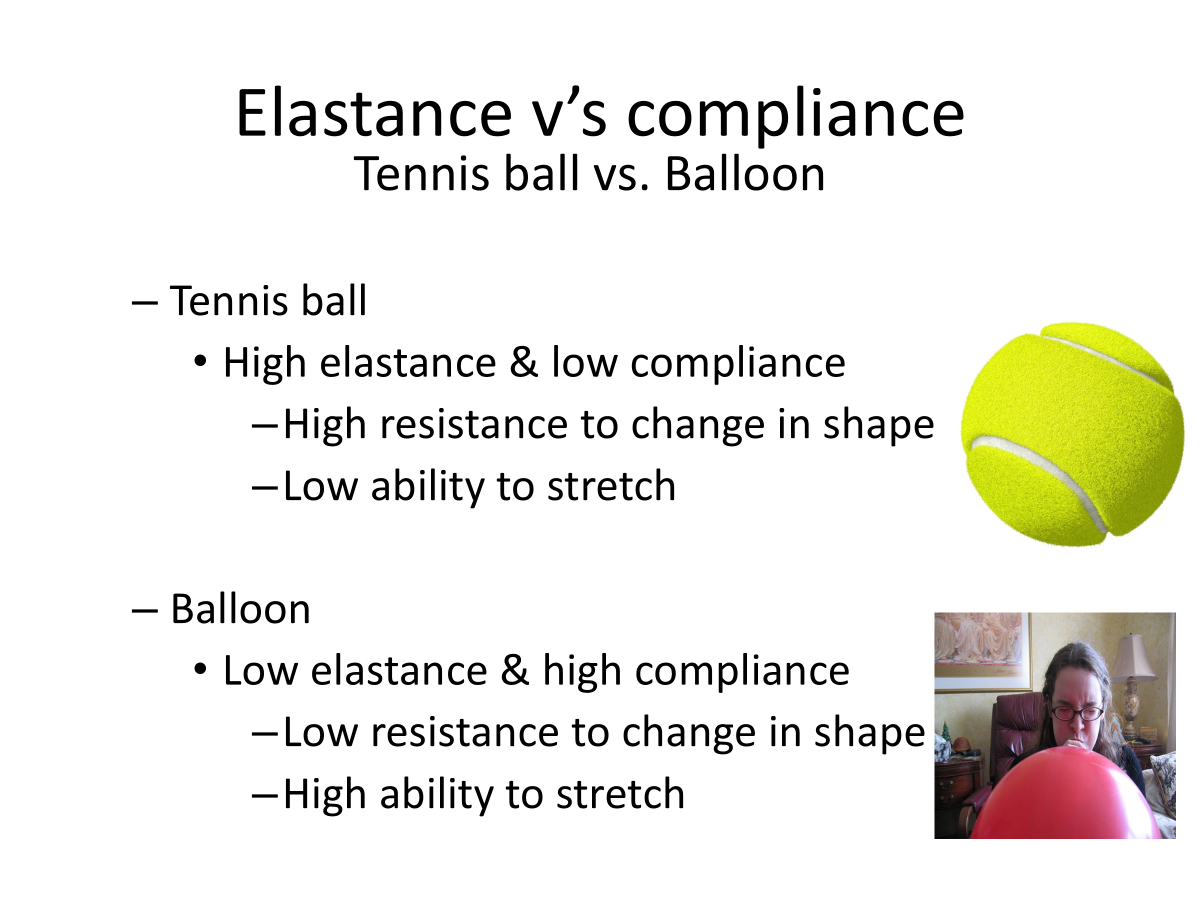
Compliance and elastance
Compliance: Distensibility (stretch) of the lung i.e the change in lung volume that occurs with each unit change in transpulmonary pressure i.e V/P
For both lungs this is 200mL/cm H20 i.e 1cmH20 change expands lung by 200ml.
Specific Compliance: Is this corrected for volume at that time i.e compliance/V.
This standardizes compliances for different volumes.
i.e if a lobe is removed(less volume) it shows that the compliance is unaltered
Elastance: Property of resisting deformation (resistance) or desire to return to original shape.
E = 1/C
C = compliance.
V/P compliance relationship
Shows the capacity of the lungs to adapt to transpulmonary pressure changes.
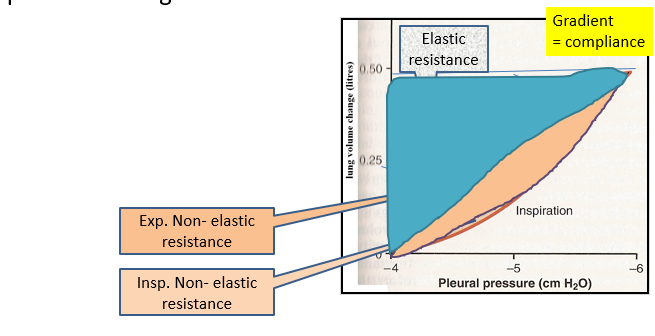
You need the muscular effort so the work of breathing is the area in this loop plus the hatched area. Resistances are overcome.
Static Resistances
Chest wall
‘stiffness’ of chest wall
Force of movement of chest wall is opposite that of lung.
Chest wall has a tendency to expand (pull out) but held by negative pleural pressure.
Unopposed reaches 70% of TLC (total lung capacity) (resting position).
When thorax is intact, in equilibrium with the lungs, its resting level is Functional Residual Capacity (FRC).
Cause of increased chest wall resistance
Structural abnormality → Decreased flexibility/expansion.
Deformities of thorax.
Ossification of costal cartilage.
Paralysis of intercostal muscles.
Chest trauma
Paralysis, strain, pain
Loss of elasticity
Burns
Blockage of the smaller respiratory passages with mucus or fluid.
Raised abdominal pressure
Obesity
Pregnancy.
Lungs
Elastic recoil is the tendency of an elastic structure to oppose stretching.
The lung naturally has a tendency to collapse because of recoil. They are held by the negative intrapleural pressure (established my lymphatic pumping of fluid).
Collapse caused by:
Elastin and collagen in lung tissues (1/3 of this)
Interwoven in lung parenchyma.
Tendency to oppose stretching - why?
Surface tension (2/3 of this resistance).
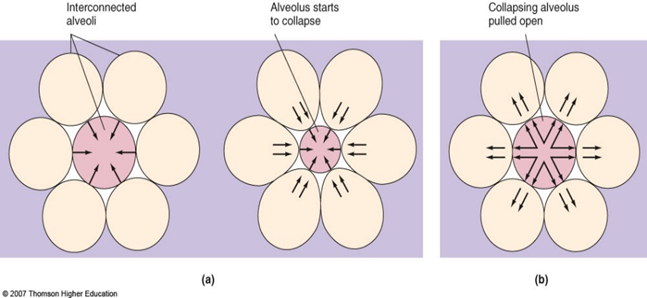
Small alveoli are unstable and have a greater tendency to collapse and empty its air into connected larger alveoli (i.e atelectasis).
Reduction of ST forces allows interdependent/stability
Surfactant
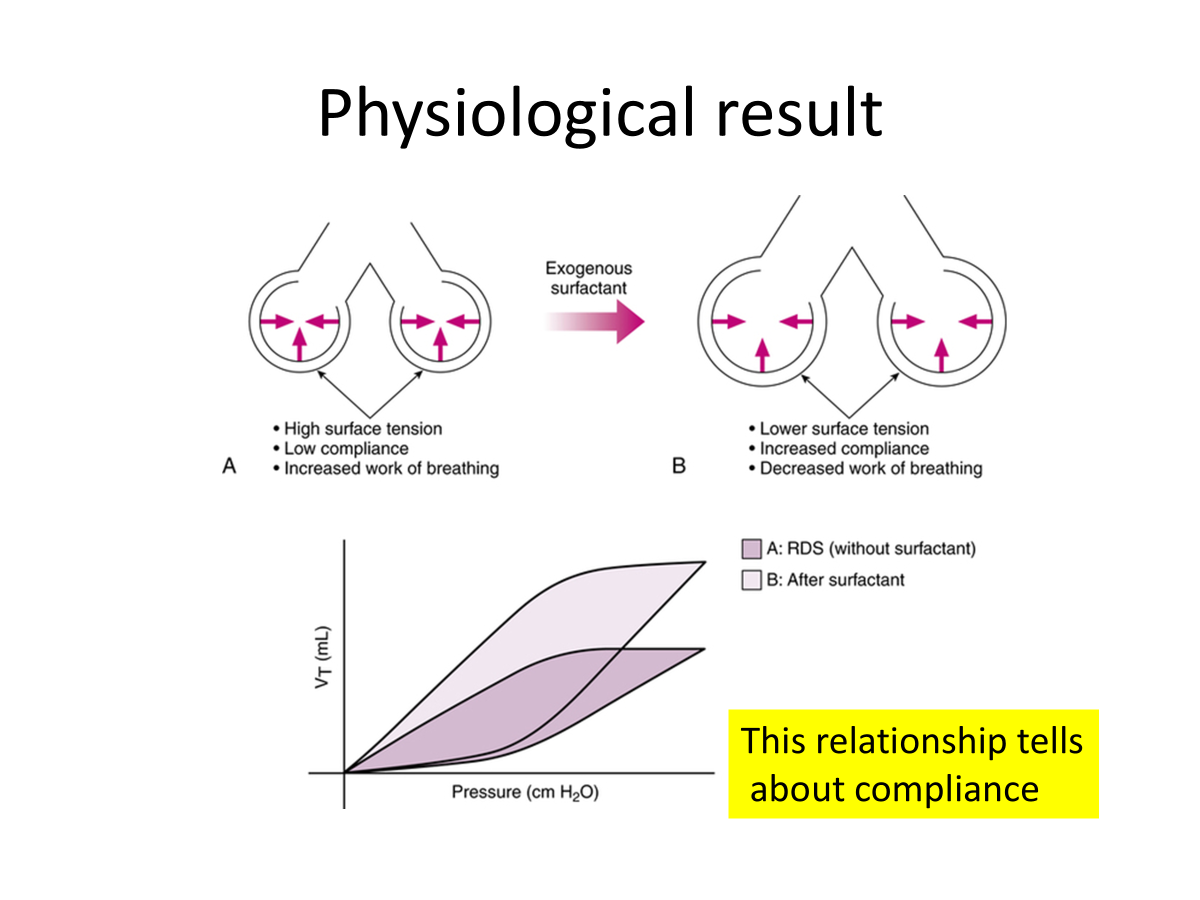
3x less transmural pressure is needed to expand lungs.
Keeps alveoli dry
Lowers the inwardly directed pressure which draws water into the alveoli.
Maximizes area for ventilation and perfusion.
ST of small alveoli are reduced more than larger alveoli as surfactant molecules crowd into the smaller space.
Maintains ‘alveolar interdependence’
Aided by fibrous tissue septal and septal walls between alveoli of different sizes which act as additional splints.
Disorders influencing ST
Prematurity (Neonatal respiratory distress syndrome, NRDS)
Adult respiratory distress syndrome
Oxygen toxicity
Neonatal Distress Syndrome
A 1.5 kg male baby is delivered preterm at 33 weeks. The child is cyanotic and shows increased work of breathing including tachypnea, nasal flaring, chest retractions and grunting. Their pulse is 160 beats/min. It is obvious that the baby is in respiratory distress.
NRDS: Increasing respiratory distress, commencing at, or shortly after birth and increasing in severity until progressive resolution occurs among survivors, usually around 2nd to 7th day. Caused by deficiency of surfactant.
Can be primary or secondary.
Incidence and severity is inversely proportional to gestational age.
Symptoms:
Tachypnea (>60bpm)
Grunting
Nasal flaring
Intercostal recession
Cyanosis
Reduced entry of air
Causes and contributor factors of NRDS
Fetal head injury during birth.
Aspiration of blood or amniotic fluid.
Excessive sedation of mother during birth.
Maternal diabetes → excess insulin suppresses surfactant production.
Cold stress
More common in males
Genetic disorders e.g abnormalities in proteins B and C or transport proteins ABC transporter 3 [ABCA3]
Pathogenesis of NRDS
Starts with immature and damaged Type II pneumocytes due to risk factor or specific cause.
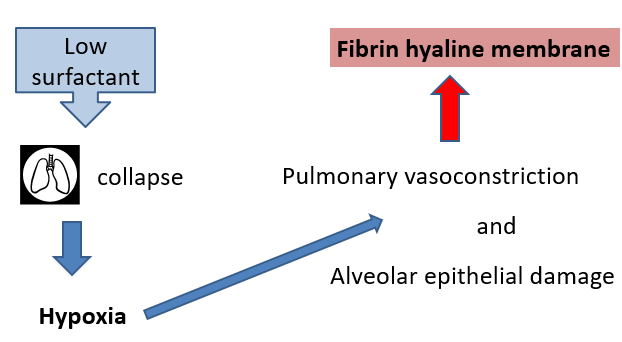
Consequences
Inflammation, so neutrophils in the lungs
Atelectasis
Leads to VQ mismatch.
Right to left shunting.
Arterial hypoxemia.
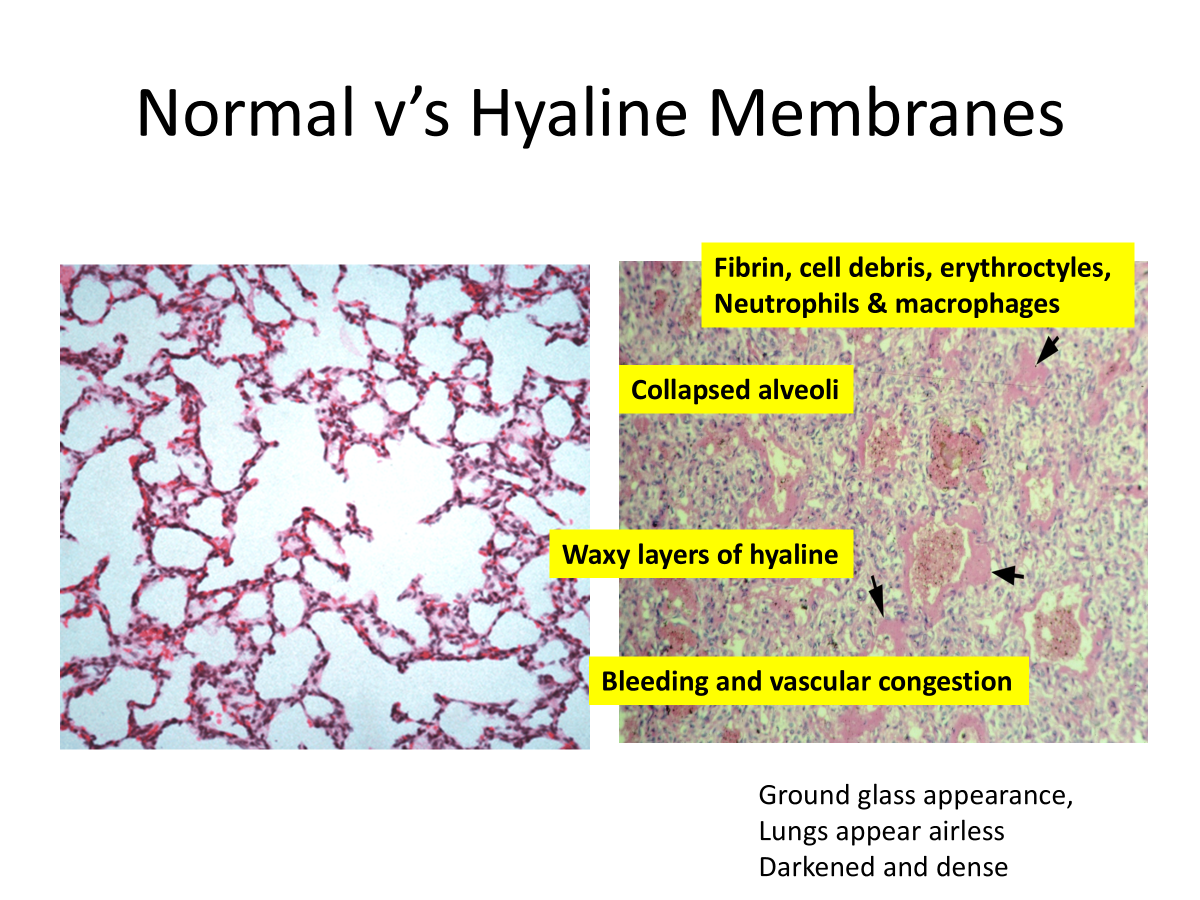
Hyaline membrane
Epithelial necrosis
Decreases fluid absorption and lung edema
May hemorrhage.
Can lead onto complications e.g hypoxic related, intracerebral bleeding, GIT necrosis, failure to close the ‘hole in heart’ and also some fibrosis due to fibrin exudation.
Treatment
In affected babies:
Synthetic surfactant therapy
Assisted ventilation.
Supportive care e.g thermoregulation, fluid management and nutrition.
Pre-term mothers
i.v betamethasone 26-28 weeks gestation.
Physiological result