Hematology
Hematology Overview
Hematology- the study of blood. The system is used to transport oxygen, waste, electrolytes, and maintains intramuscular volume. Coagulates blood, and fights infection.
Hematology: Study of blood and blood-forming tissues.
Major components include:
Bone marrow
Blood
Spleen
Lymphatic system.
Structures and Functions of Hematologic System
Hematopoiesis: Blood cell production. All blood starts off as hematopoietic, and then develops into myeloid cells. (T and B lymphocytes)
Occurs in bone marrow. The soft material that fills the central core of bones. Two types: Yellow (Adipose), and Red.
Produces:
Red blood cells (RBCs)
White blood cells (WBCs)
Platelets.
Develops from stem cells, which are non differentiated immature blood cells.
Bone Marrow
Soft material filling the central core of bones.
Types of bone marrow:
Yellow marrow: Contains adipose tissue.
Red marrow: Hematopoietic; involved in blood cell formation.
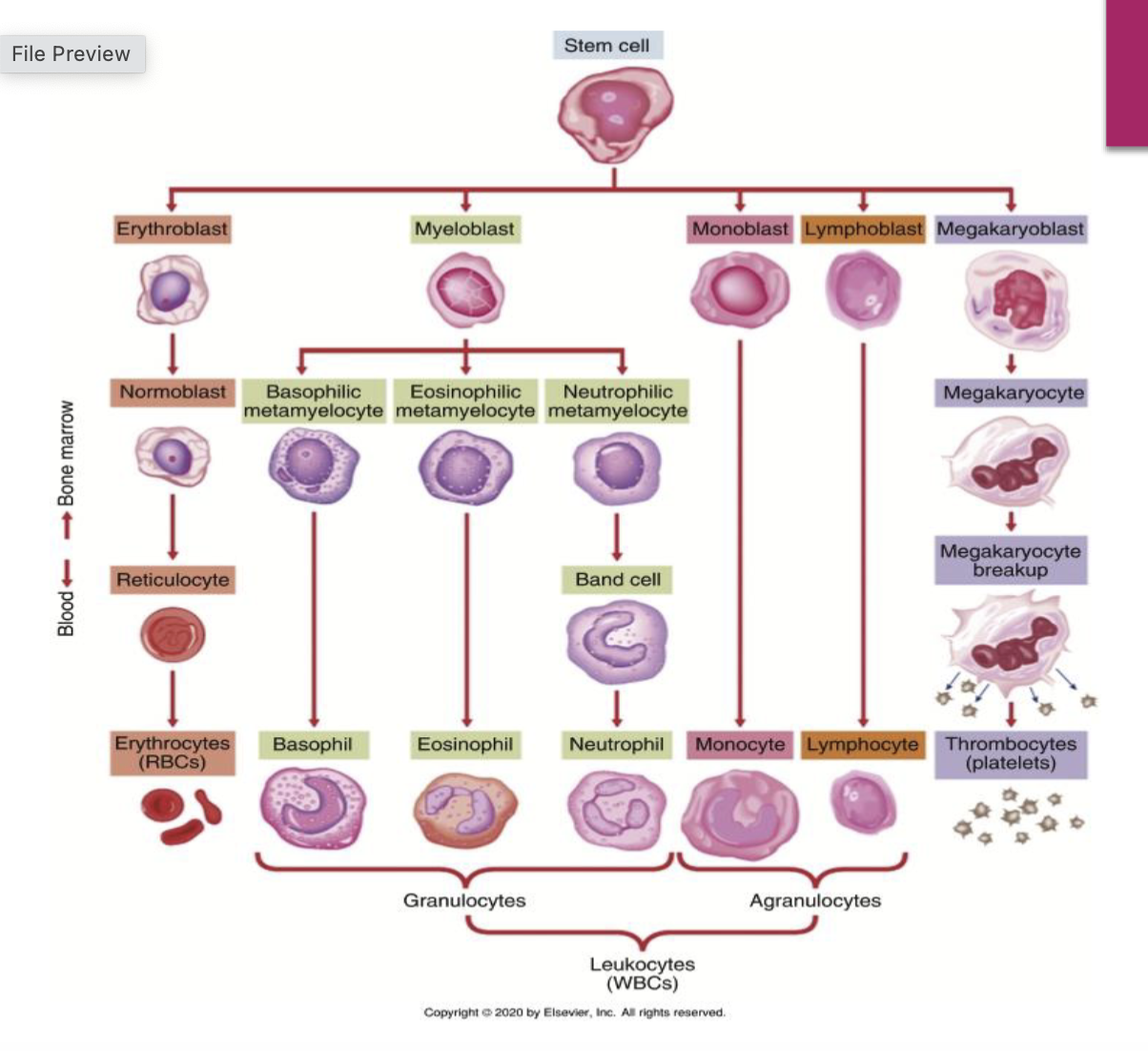
Blood Cell Development
Key stages in blood cell development include:
Stem cell transformation into:
Erythroblasts (red cells)
Myeloblasts (granulocytes)
Monoblasts (monocytes)
Lymphoblasts (lymphocytes)
Megakaryoblasts (platelets).
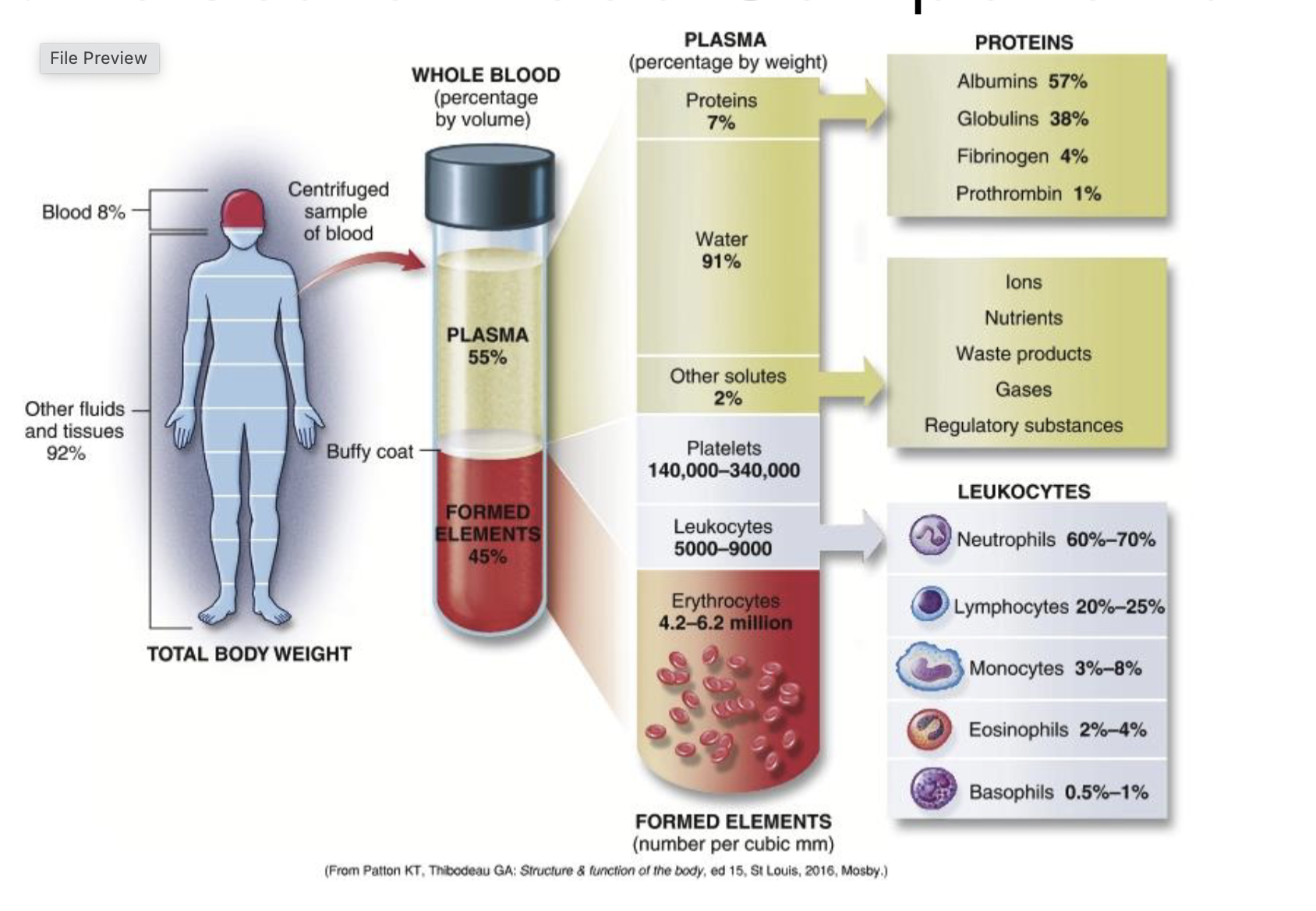
Blood Component Values
Whole Blood Composition:
Total body weight: 8%
Plasma: 55% (91% water, 7% proteins, 2% other solutes).
Formed Elements:
Platelets: 140,000 - 340,000 per cubic mm.
Leukocytes: 5,000 - 9,000
Erythrocytes: 4.2 - 6.2 million.
Distribution of leukocytes:
Neutrophils: 60%-70%
Lymphocytes: 20%-25%
Monocytes: 3%-8%
Eosinophils: 2%-4%
Basophils: 0.5%-1%.
Erythrocytes (RBCs)
Functions:
Transport O2 and CO2
Maintain acid-base balance.
Hemoglobin: Composed of iron and protein.
Oxyhemoglobin: oxygen bound with iron.
Thrombocytes (Platelets)
Functions:
Initiate the clotting process. They produce at the site of injury
Plug capillary openings.
Help in clot shrinkage and retraction.
Development begins with stem cells transforming into megakaryocytes, which fragment into platelets.
They must be available in enough numbers and be structurally and metabolicallly sound for blood clotting to occur.
Thrombopoietin partially regulates platelet production. TPO is a growth factor that acts on bone marrow to stimulate platelet production.
Produced in the liver, kidney, smooth muscle, and bone marrow.
Life span: 8-10 Days.
Hemostasis Process
Vascular injury leads to vasoconstriction and subendothelial exposure.
Adhesion: Platelets adhere to the exposed sites due to loss of endothelial tissue. adhesive glycoproteins from.
Activation of the clotting cascade.
Formation of blood clot, followed by clot retraction and dissolution.
Hemostasis Details
Initial Response: Vasoconstriction reduces blood leakage and provides time for platelet and clotting factor responses.
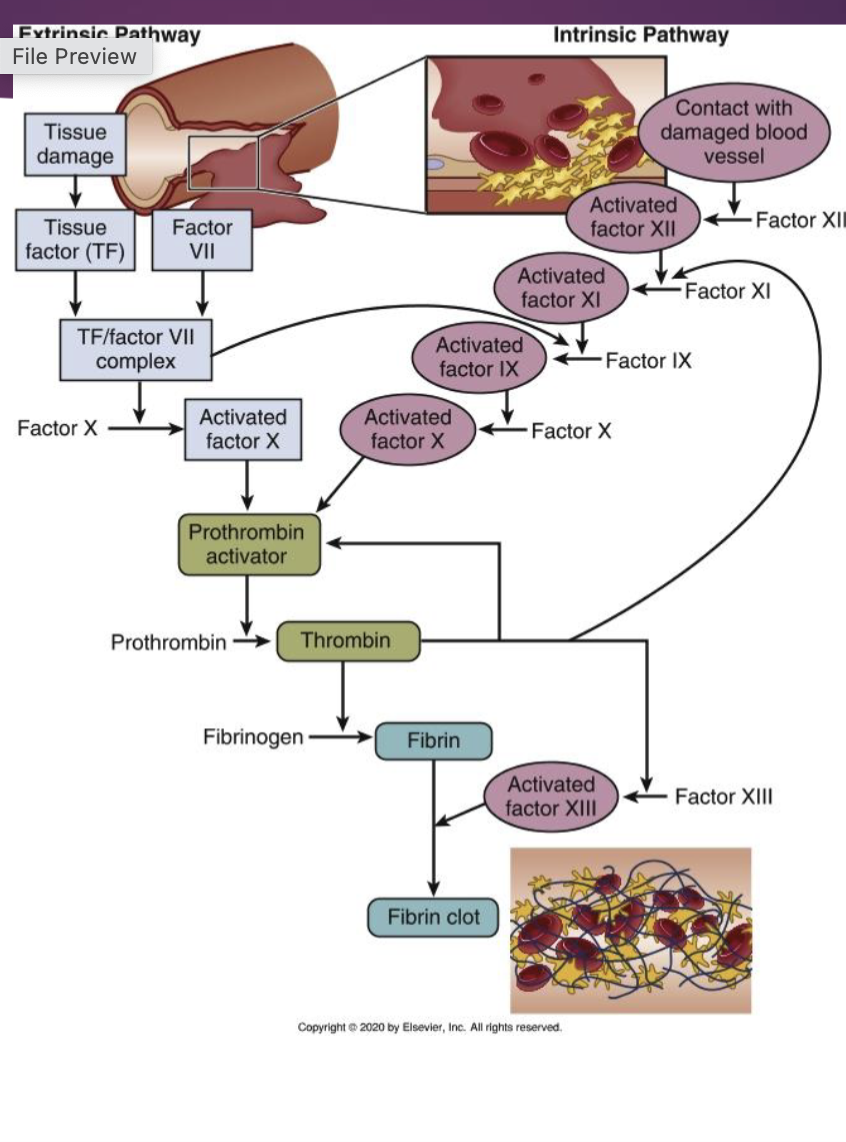
Clotting Cascade Activation:
Platelet adhesion triggers changes in platelet shape and activates binding to adhesive proteins; this leads to the release of granules that activate further clotting.
Clotting is initiated by:
Intrinsic pathway: Triggered by damage to blood vessels. Both pathways start at the same level, and end at the same place.
Extrinsic pathway: Triggered by tissue factor release. Activated by collagen exposure.
Clot retraction and dissolution
Procoagulants
Foster coagulation
Anticoagulants
Interfere with clotting
Assessment of Hematologic System
Subjective Data: Includes health history, medications (non prescription, heral supplements, substances, functional health patterns, and assessment of current health status. Nonprescription drugs: OTC, vitamins, herbal products, dietary
supplements
Subjective data: Functional health patterns
Health perception–Health management pattern
Usual and present state of health
Demographic data
Family history and genetically linked disorders
High-risk behaviors
Genetic risk alert
Objective Data: Physical assessment focusing on skin, lymph nodes, spleen, and liver for signs of hematological disorders (e.g., petechiae, ecchymoses).
Subjective data: Functional health patterns
Nutritional–metabolic pattern
Weight, dietary pattern, history of cardiac or pulmonary diseases
Changes in skin texture, color or temperature
Characteristics of lumps in neck, armpits, or groin
Elimination pattern
Bleeding is significant
Subjective data: Functional health patterns
Activity–exercise pattern
Sleep–rest pattern
Fatigue not relieved by sleep should be evaluated
Subjective data: Functional health patterns
Sexuality–reproductive pattern
Menstrual history, impotence, or high-risk sexual
behaviors
Objective data:
Physical assessment
Diagnosis of hematologic disorders often requires considering presenting symptoms in context of broader clinical assessment findings and risk factors
Of particular importance are examination of skin, lymph nodes, spleen, and liver
Objective data
Physical examination
Skin assessment
Systematic head-to-toe order
Petechiae
Ecchymoses
Spider nevus- Spider Veins
Clubbing of fingers- Oxygen issue
Assessment Components
Health History: Previous anemia, other blood disorders, and medications.
Physical Examination: Skin assessment for signs of bleeding or bruising.
Nutritional and Cardiac Assessments: Important for evaluating anemia.
Anemias
Anemia leads to insufficient oxygen delivery to tissues due to:
Blood loss
Inadequate RBC production
Increased RBC destruction. RBC are destroyed faster than they can be replaced.
Pathophysiology of Anemias
Physiology review- Dry Mouth (Chilitis), pale conjuctiva
Amount of oxygen that reaches tissues depends on:
Available oxygen in alveoli
Diffusing surface, capacity of lungs
Number of RBCs, amount and type
of hemoglobin they contain
Ability of cardiovascular system to
transport blood and oxygen to
tissues
Blood loss
Inadequate RBC production
Increased RBC destruction
Insufficient or defective hemoglobin
within RBCs
Health history and physical exam
Laboratory data- Hemoglobin, Reticulocyte, Hematocrit
Presence of symptoms and impact of those symptoms on
patient’s life; fatigue, weakness, malaise, pain. Dry Mouth, Pale conjunctiva
Nutritional assessment
Medications
Cardiac and GI assessment- TachyCardia, Low blood viscosity leading to heart murmurs, orthostatic hypotension, hypoxia, dyspnea(SOB)
Blood loss: menses, potential GI loss
Neurologic assessment- confusions, headache, ataxia, loss of control of your body moments.
Cobalamin (Vitamin B12) Deficiency
Characterized by large RBCs (megaloblasts) due to impaired DNA synthesis.
Treatment includes parenteral or intranasal cobalamin administration, critical for preventing death in untreated individuals.
Caused by absence of intrinsic factor (IF)
Insidious onset
Begins in middle age or later
Predominant in Scandinavians and blacks
Red beefy tongue, abdominal pain, nasuea and vommiting, impaired cognition, ataxia
Folic Acid Deficiency
Contributes to megaloblastic anemia.
Similar manifestations to B12 deficiency; treated with folate replacement therapy.
Aplastic Anemia
Characterized by pancytopenia (decreased RBCs, WBCs, and platelets).
Diagnosis confirmed by laboratory findings and examination of bone marrow.
Prognosis is poor if untreated but improved through treatments such as immunosuppressive therapy.
Thrombocytopenia
Reduced platelet count leading to increased bleeding risk.
Managed based on underlying causes; can include conditions like ITP and HIT.
Lymphomas
Hodgkin's Lymphoma and Non-Hodgkin's Lymphoma are prevalent lymphatic cancers characterized by different cellular abnormalities and genetic features.
Diagnosis and prognosis vary widely based on subtype and staging.
Treatment regimens include chemotherapy, targeted therapy, and monitoring for secondary cancers after treatment.
Conclusion
This lecture presented foundational concepts of hematology, emphasizing the vital understanding of blood cell development, hematopoiesis, and related disorders for effective assessment and management strategies in clinical practice.