ANAT Upper Limb
ANAT1451- Upper limb
LO1 To identify anatomical features of the bones of the pectoral girdle and arm
Pectoral Girdle:
- Clavicle (collarbone)
- Scapular
- Connected to acromioclavicular joint (acromial end of scapula/clavicle – back end)
- Girdle connected to axial skeleton (midline – skull, vertebral column) at sternoclavicular joint
- Girdle connected to the rest of the upper limb (arm) at glenohumeral joint (humerus and scapular articulate – shoulder joint)
Articulate – 2 bones at a joint
Clavicle:
- S shape
- Convex anterior
- Concave posterior
- Shaft/body is main part of bone between the ends
- Superior surface is smooth
- Inferior surface has lumps/bumps, rough patches (tubercle) at lateral end – posterior – attachment of conoid
- Impression for costoclavicular ligament – (costo – rib, costal cartilage, join to sternum). 1st costal cartilage
- Subclavian groove – beneath the clavicle – subclavius muscle present
- Trapezoid line – lateral – attachment of trapezoid
Tubercle – bump/lump
Ligament – connect 2 bones together, restrict too much movement
Scapula:
- Posterior – spine (lump)
- Anterior – nil
- Lateral – shoulder joint
- Angles (pointy) – superior, inferior and lateral
- Borders – superior, medial and lateral – Inferior – lateral – lateral – superior – superior – medial (between angles)
- Processes (stick out bit) – acromion, coracoid (deep, below clavicle), spine (back point – turns into acromion towards shoulder)
- Fossae (bone spaces) – supraspinous (above spine of scapular, infraspinous (below scapular spine) , subscapular (deep below scapular spine), glenoid (cavity for humerus)
- Tubercle – supraglenoid (above glenoid cavity), infraglenoid (below glenoid cavity)
- Movement: Elevation/depression, retraction/protraction (add/abd), lateral(up/ant)/medial (down/pos) rotation
Humerus:
- Proximal attaches to glenohumeral joint (shoulder)
- Neck – anatomical (line along head of bone – head used to be separate bone when growing – growth plate – fuses to shaft of bone), surgical (around bone – narrowest/weakest part of bone – most susceptible fracture – below anatomical neck line)
- Tubercle – greater (next to head, superior), lesser (bilateral posterior of head). Intertubercular sulcus (gap between – turns to lips)
- Lip – medial (closer to midline), lateral (outer)
- Facet (flattened section – muscle attachment) – superior, middle, inferior – visible on posterior
Lo2 To identify key features of the shoulder, pectoral region and the arm on a living person (surface anatomy)
- Items you can palpate on the body
LO3 To understand the structure of the acromioclavicular, sternoclavicular and glenohumeral (shoulder) joints
- 3 mutually dependent joints – movement together
Sternoclavicular:
- Articulating Surfaces: Clavicle (sternal end), manubrium (clavicular notch)
- Disc between aids fit of surfaces – help clavicle articulate better with manubrium
- Synovial saddle joint (modified - rotation)
- Movement: Elevation/depression, protraction/retraction, axial rotation
- Supporting ligaments: anterior and posterior sternoclavicular (between sternum and clavicle), interclavicular (between – runs along top of joint), costoclavicular (between clavicle and first costal cartilage)
- Elevation limited by costoclavicular ligament (stretched when arm lifted) and subclavius (muscle in groove on clavicle)
- Depression limited by interclavicular ligament and disc
Acromioclavicular:
- Articulating Surfaces: clavicle (acromial end) and acromion
- Disc is wedged – doesn’t aid congruency as much
- Synovial plane (gliding) joint (modified - rotation)
- Movement: elevation/depression, protraction/retraction, axial rotation
- Supporting ligaments: superior and inferior acromioclavicular
- Coracoclavicular ligament (2 parts) – conoid ligament (posterior attachment - limit protraction - forward) and trapezoid ligament (anterior attachment – limit retraction - back)
Scapulothoracic ‘Joint’:
- Not a true anatomical joint – not articulation with cartilage between
- Important for positioning of shoulder joint
- Scapula glides against chest wall
- The subscapular/anterior surface of scapula and superolateral surface of the thoracic wall
- Separated by the subscapularis muscle and serratus anterior muscles (and space between)
- Stabilised by muscles
- Movement: elevation/depression, protraction/retraction, medial/lateral rotation
Glenohumeral:
- Articulating surfaces: head of humerus (large and spherical), glenoid fossa (cavity - shallow, small, pear-shaped, 1/3 size of humerus)
- Incongruent joint – unstable, big range of motion
- Synovial ball and socket
- Movement: flexion/extension, abduction/adduction, medial/lateral rotation, circumduction
- Ligaments: superior, middle and inferior (stronger – longer and thicker – if weak, increase dislocation) glenohumeral (located internally on anteroinferior joint capsule, limit excessive lateral rotation, middle and inferior limit excessive abduction), transverse humeral (capsular lig – between greater/lesser tubercle – holds down tendons on long headed bicep along intertubercular groove), coracohumeral (capsular lig – blends with supraspinatus tendon – between coracoid process to humerus), coracoacromial (accessory lig – helps prevent superior shoulder dislocation – coracoid process and acromion)
- Stabilising Structures: Glenoid labrum (outside of fossa – deepens socket, fibrocartilage rim, triangular in cross section, tendon of long head of bicep brachii blends with labrum), Coracoacromial arch (fibro-osseous – ligament and 2 bones), formed by coracoid process, acromion, and coraco-acromial ligament, strong to prevent superior dislocation
- Joint capsule – thick but loose (range of motion) around whole bones, attaches beyond labrum anteriorly and inferiorly, to labrum posteriorly and superiorly, to the anatomical neck of humerus, internal surface lined with synovial membrane, filled with synovial fluid, tendon of long head biceps (to supraglenoid tubercle) within joint capsule
- Rotator Cuff Muscles – MOST IMPORTANT STABILISERS – tendon blend with joint capsule, dynamic ligaments, from scapular to humerus, close packed of GH joint when in abduction and external rotation (most congruent – tight)
- 4 muscles – Supraspinatus, Infraspinatus, Teres Minor, Subscapularis (TISS – back to front) – strengthen rotator cuff for increase shoulder stability
- Bursae – fluid filled sacs, lined with synovial membrane, and filled with synovial fluid (designed to reduce friction)
- Subdeltoid – deep between joint capsule and deltoid
- Subacromial – deep between coracoacromial arch and acromion
- Subscapular – deep between joint capsule and subscapularis
- Communication/connection between subdeltoid and subacromial, and subscapular and joint cavity – if one affected, both affected
- Bursitis – infection or swelling (overuse)
Capsular ligament – thickening of fibrous joint capsule
Accessory ligament – sit around joins
Lo4 To correlate the structure of the shoulder joint to its functional movements and stability
Rotator Cuff Muscles - Posterior:
Supraspinatus
- Attached to supraspinous fossa and superior facet of greater tubercle
- Action: Initiate and assist deltoid with abduction and stabilise GH joint
- Nerve Supply: Suprascapular nerve
- In use majority of time
Infraspinatus
- Attached to infraspinous fossa and middle facet of greater tubercle
- Action: Laterally rotate humerus and stabilise GH joint
- Nerve Supply: Suprascapular Nerve
Teres Minor
- Attached to lateral border of scapula and inferior facet of greater tubercle
- Action: Laterally rotate humerus and stabilise GH joint
- Nerve Supply: Axillary nerve (wraps around surgical neck of humerus)
Rotator Cuff Muscles – Inferior:
Subscapularis
- Attached to subscapular fossa and lesser tubercle
- Action: Medically rotate humerus (strongest rotator), stabilise GH joint, assist with adduction
- Nerve Supply: Upper and Lower subscapular nerves
Upper Limb to Vertebral Column (Superficial)
Trapezius:
- Attachments:
- Skull (superior nuchal line and external occipital protuberance) and nuchal ligament
- Vertebral column (Spinous processes C7-T12)
- Clavicle (lateral 1/3)
- Scapula (acromion and spine)
- Actions (unilateral):
- Superior/lateral rotates glenoid fossa (abduction)
- Retracts scapula
- Elevate scapula (upper part)
- Depress scapula (lower part)
- Laterally flex neck
- Actions (bilateral):
- Extend neck
- Nerve Supply:
- Spinal accessory nerve (motor)
- C3-C4 (pain and proprioception)
Latissimus Dorsi:
- Attachments:
- Vertebral Column (spinous processes of T6-T12, thoracolumbar fascia, iliac crests)
- Humerus (floor of intertubercular groove)
- Actions:
- Adducts arm
- Medially rotates arm
- Extends a flexed arm
- Raises body towards arm
- If humerus is fixed, can pull trunk forward and ‘hitch’ hips
- Nerve Supply:
- Thoracodorsal nerve
Upper Limb to Vertebral Column (Deep)
Levator scapulae:
- Attachments:
- Vertebral Column (transverse processes C1-C4)
- Scapula (medial border, superior to root of spine)
- Actions:
- Elevate scapula
- Medially rotate scapula
- Nerve Supply:
- Dorsal scapular nerve
- Anterior rami C3-C4
Rhomboid Major:
- Attachments:
- Vertebral Column (nuchal ligament and spinous processes C7-T1)
- Scapula (medial border adjacent to root of spine)
- Actions:
- Elevates scapula
- Retracts scapula
- Medially rotates glenoid fossa
- Nerve Supply:
- Dorsal scapular
Rhomboid Minor:
- Attachments:
- Vertebral Column (spinous processes T2-T5)
- Scapula (medial border inferior to root of spine)
- Actions:
- Elevates scapula
- Retracts scapula
- Medially rotates glenoid fossa
- Nerve Supply:
- Dorsal scapular
Upper Limb to Scapula
Teres Major:
- Attachments:
- Scapula (lower 1/3 lateral border)
- Humerus (medial lip of intertubercular groove)
- Actions:
- Adducts arm
- Medially rotate arm
- Nerve Supply:
- Inferior subscapular nerve
Deltoid:
- Attachments:
- Clavicle (lateral 1/3)
- Scapula (acromion and spine)
- Humerus (deltoid tuberosity)
- Actions:
- Flexes and medially rotates arm (anterior fibres)
- Abducts arm (middle fibres)
- Extends and laterally rotates arm (posterior fibres)
- Nerve Supply:
- Axillary Nerve
Upper Limb to Scapula (Anterior)
Biceps Brachii:
- Attachments:
- Scapula – long head: supraglenoid tubercle and labrum
- Short head – coracoid process
- Radius (radial tuberosity and deep forearm fascia)
- Actions:
- Weak flexor of shoulder
- Short head resists shoulder dislocation
- Supinates forearm
- Flexes forearm
- Nerve Supply:
- Musculocutaneous nerve
Coracobrachialis:
- Attachments:
- Scapula (coracoid process)
- Humerus (middle 1/3 of shaft medially)
- Actions:
- Assists in flexion of shoulder
- Assist in adduction of shoulder
- Nerve Supply:
- Musculocutaneous nerve
Upper Limb to Scapula (Posterior)
Triceps Brachii:
- Attachments:
- Scapula – long head: infraglenoid tubercle
- Humerus (posterior): lateral head – superior to radial groove, medial head – inferior to radial groove
- Ulna – proximal end of olecranon (elbow lump – blend together) and deep fasica
- Actions:
- Extends shoulder (weakly as it crosses the shoulder joint)
- Extends forearm
- Nerve Supply:
- Radial nerve
Upper Limb to Thoracic wall
Serratus Anterior:
- Attachments:
- Ribs (lateral aspects of ribs 1-8)
- Scapula (anterior surface of medial border) SCAPULOTHORACIC ‘JOINT’
- Actions:
- Protract scapula
- Superior/lateral rotation of scapula
- Nerve Supply:
- Long thoracic nerve
Pectoralis Major:
- Attachments:
- Clavicle (medial ½ anterior surface)
- Sternum (anterior manubrium and body)
- Costal cartilages 1-6
- Humerus (lateral lip of intertubercular groove)
- Actions:
- Adducts arm
- Medially rotates arm
- Clavicular head flexes arm
- Sternocostal head extends arm (when flexed)
- Assists latissimus dorsi to raise trunk towards arms
- Nerve Supply:
- Medial and lateral pectoral nerves
Pectoralis Minor (deep to Major):
- Attachments:
- Ribs 3-5
- Scapula (coracoid process)
- Actions:
- Stabilises scapula (holds against thorax)
- Nerve Supply:
- Medial pectoral nerve
Accessory Muscle
Subclavius:
- Attachments:
- Junction of rib 1 and its costal cartilage
- Clavicle (subclavian groove)
- Actions:
- Depress clavicle
- Nerve Supply:
- Nerve to subclavius
Clavicle:
- ROM – permitted by movements at the sternoclavicular joint
- Synovial Saddle joint (modified)
- Circumduction requires coordinated movements at pectoral girdle and glenohumeral joint
Abduction Cycle (arm from side to up next to ear):
Stage 1 –
- Glenohumeral movement alone 1st 30 deg, inferior angle of scapula should not move
- Max 3mm upward displacement of humeral head
- Lateral rotation of the humerus occurs by stage 1
Stage 2 –
- Scapular elevation and upward rotation points glenoid fossa superiorly
- Humeral head glides inferiorly by 90 deg revealing a sulcus
Stage 3 –
- Scapula glides around rib cage (scapulothoracic)
- Inferior angle of scapula should not protrude further than 1cm from chest wall
Shoulder Joint:
- Flexion/extension
- Abduction/adduction
- Medial/lateral rotations
- Circumduction (combination of all)
Scapulohumeral Rhythm (2°:1°):
- Abduction of shoulder joint
- Total range is ~180 deg
- 120 performed by movement at GH
- 60 performed by lateral rotation of scapula
- For every 3 of abduction, 2 at shoulder, 1 at scapulothoracic joint (2:1)
Scapular Rotation:
Lateral:
- Serratus anterior
- Trapezius (upper and lower fibres)
Medial:
- Levator scapulae
- Rhomboids
- Pectoralis minor
LO5 To understand how stability and function of the shoulder joint can be altered as a result of dislocation, fractures and muscular injuries
LO6 To identify normal anatomical features and injuries on radiographs of the shoulder and pectoral girdle
On X-ray: Bones – white, Soft tissue – grey, Air – black
Clavicle Fracture:
- Caused by direct force to shoulder or indirect force transmitted from an outstretched hand
- Weakest part of clavicle is the junction of its middle and lateral thirds
- Sternal end pulled up (sternocleidomastoid muscle)
- Gravity, pectoralis major pulls medial-lateral end down
- Minor fractures (clean break) – sling only, pull clavicle back up to align
Dislocation of AC Joint:
- Caused by direct force to shoulder or indirect force transmitted from an outstretched hand
- Can be accompanied by rupture of coracoclavicular ligament (serious fracture)
- Will be able to palpate - Acromial end will be pulled upwards (higher = more damage)
Dislocation of GH Joint:
- Can be caused by direct or indirect trauma
- Can involve nerve damage (typically axillary or radial)
- Overarm throw – abduction, lateral rotation – shoulder joint stable and tight – very susceptible to knocks and dislocation
- Head of humerus moves downwards due to gap in rotator cuff (blocked on all other sides by structures)
- Called anterior dislocation due to final muscle pull (end location)
- Once dislocated, joint capsule is weakened and more susceptible to further dislocations
Rotator Cuff Tendinopathy or Tear:
- Caused by repetitive use
- Cuff is impinged on coracoacromial arch
- Results in degenerative tendinosis of rotator cuff
- Most commonly in supraspinatus (muscle built up, increase in size – reduced gap, tight fit, bursae swell)
- May be caused due to sudden strain of muscles
- TEST: slowly lower arm from ear to side. May be sudden drop close to 15° from side. Also, resistance test (abduction vs push down)
LO7 To know the muscles that attach to the scapula and humerus (attachments, nerve supply & functions)
- Nerves – supply body structures with electrical impulse to muscle fibres to shorten and contract – hence movement
- Veins – thin walled, deoxygenated blood back to heart
- Arteries – thick walled, oxygenated blood to limbs
LO8 To know the blood vessels of the scapular and pectoral regions and understand lymphatic drainage of the upper limb
- Subclavian artery supplies upper limbs
Left:
- Left subclavian and left carotid artery directly off aorta
Right:
- Brachiocephalic trunk branches into right subclavian and carotid
- Becomes axillary artery at lateral border of first rib
- Continues underneath (pec Major) arm until inferior border of teres major becomes Brachial artery
- Branches to subscapular artery
- Branches to 2
- Circumflex scapula – posterior – anastomose with dorsal scapular
- Thoracodorsal – posterior to Lat Dorsi – join to dorsal scapular
- Follows til elbow and splits into
- Radial artery on lateral side
- Ulnar artery on medial
- Hand supplied by both radial and ulnar arteries
Subclavian Artery:
- Branches into thyrocervical trunk, then suprascapular and transverse cervical (travel towards scapular)
Suprascapular:
- Travels posterior
- Gives off small branches to supraspinous and infraspinous fossa
Transverse cervical:
- Branches into 2
- Only interested in dorsal scapular artery
- Comes down medial border – anastomose with suprascapular and subscapular (from axillary)
Major joints have anastomoses: Connection between 2 arteries
- Offers blood an alternative route to a destination (if a path is blocked)
- Ligature – blocking, blood clot – tightening of blood vessel
Venous Draining
Superficial – visible underneath skin
- Superficial venous palmar arch drains to
- Basilic (medial) drains to Axillary
- Cephalic (lateral) – between deltoid and pectoralis – deltopectoral groove – drains to
- Axillary
Deep – same name as arteries
- Deep venous palmar arch
- Ulnar
- Radial
- Brachial join to form Axillary
- Axillary*
- Subclavian*
- Brachiocephalic
*Only 1 artery and vein
Lymphatic Drainage of Upper Limb (not tested)
- Many lymph nodes in axillary area and drain up towards subclavian area
- Drain into right or left Venus angle (subclavian meets internal jugular vein)
BRACHIAL PLEXUS and ARM
LO1 To identify anatomical features of the humerus
LO2 To identify key features of the arm and elbow region on a living individual (surface anatomy)
- Deltoid tuberosity on mid latera shaft
- Posterior surface – radial groove. Radial nerve travels through
Distal End:
- 1 Condyle
- Capitulum: rounded ball (little head) – lateral. Articulate with radius
- Trochlea: pulley. Articulate with ulnar – medial
- 2 Epicondyles
- Medial
- Lateral
- 3 Fossae
- Radial: (anterior) little pit for radius to sit in (during elbow flexion)
- Coronoid: (anterior) Ulnar has coronoid process sits here (during elbow flexion)
- Olecranon: (Posterior) pointy bit of elbow is olecranon (during extension of elbow)
Medial supracondylar ridge: Medial edge of bone. Muscles attach
Lateral supracondylar ridge: Lateral edge of bone. Muscles attach
LO3 To know the muscles of the arm (attachment, nerve supply and actions)
- Arranged into 2 compartments: Anterior and Posterior
- Separated by intermuscular septum (wall between 2 groups of muscle)
- Anterior: Supplied by musculocutaneous nerve
- Posterior: Supplied by radial nerve
Anterior Group:
Coracobrachialis:
- Attachments:
- Scapula (coracoid process)
- Humerus (middle 1/3 of shaft medially)
- Actions:
- Assists in shoulder flexion
- Assists in shoulder adduction
- Nerve Supply:
- Musculocutaneous Nerve
Biceps Brachii:
- Attachments:
- Scapula:
- Long Head: supraglenoid tubercle and labrum
- Short Head: coracoid process
- Radius (radial tuberosity and deep forearm fascia)
- Actions:
- Weak flexor of shoulder
- Short head resists shoulder dislocation
- Supinates forearm
- Flexes forearm
- Nerve Supply:
- Musculocutaneous Nerve
Brachialis:
- Attachments:
- Humerus (anterior distal ½)
- Ulna (coronoid process and ulnar tuberosity)
- Actions:
- Prime flexor of elbow joint
- Nerve Supply:
- Musculocutaneous Nerve
Posterior Group:
Triceps Brachii:
- Attachments:
- Scapula: Long head – infraglenoid tubercle
- Humerus (posterior):
- Lateral head: superior to radial groove
- Medial head: inferior to radial groove
- Ulna: (lateral and medial heads blend) proximal end of olecranon and deep fascia
- Actions:
- Extend shoulder (weak)
- Extend forearm
- Nerve Supply:
- Radial Nerve
Anconeus:
- Attachments:
- Humerus (lateral epicondyle)
- Actions:
- Extend forearm
- Nerve Supply:
- Radial Nerve
Trauma and Pathology:
- Fracture of surgical neck: Commonly result of fall on outstretched hand (anterior and posterior circumflex artery, axillary nerve)
- Fracture of shaft: Result from direct blow or torsion. Produce various types of fractures (Profunda brachii, radial nerve)
- Avulsion fracture of greater tubercle: Bone section torn off/pulled away. Common in middle-aged and elderly.
- Rupture of Tendon of Biceps Brachii:
- Usually result of ‘wear and tear’
- Tendon is weakened by friction as it passes through the intertubercular groove
- Rupture results from repetitive overhead motions (eg. Baseball, cricket, swimming)
- Occurs in individuals >35 years old
- Tendon is torn from its superior attachment to the scapula (coracoid process and supraglenoid tubercle)
- Associated with popeye deformity (head of muscle has slipped down towards elbow)
LO4 To describe the boundaries, contents and clinical relevance of the cubital fossa
- Located on anterior aspect of elbow region
- Triangular in shape
- Boundaries:
- Superior: Imaginary line between epicondyles
- Medial: lateral border of pronator teres
- Lateral: medial border of brachioradialis
- Roof: deep fascia and bicipital aponeurosis
- Floor: brachialis, supinator and elbow joint
- Contents:
- Medial to Lateral - Median nerve, Brachial artery, Tendon of biceps brachii
- Close relationship to fossa (not within) – ulnar nerve, redial nerve
Clinical Relevance:
- Veins and arteries are subcutaneous
- Cephalic and basilic vein meet at make median cubital vein
- Median Cubital vein: prominent, used for drawing blood, injections
- Not everyone has one. Natural variation in superficial vein pattern
- Brachial Artery: Used to take blood pressure
LO5 To know the blood vessels of the arm and forearm
Axillary Artery:
- 2 major branches: anterior and posterior circumflex humeral
Brachial Artery:
- Origin: Axillary artery
- Begins at inferior border of teres major
- Course:
- Travels medial with median nerve
- Passes anterior to trochlea of the humerus to enter lateral side the cubital fossa
- Terminates by branching into radial and ulnar artery
- Major Branches:
- Profunda brachii
- Ulnar collateral branches
Radial Artery:
- Origin: Branches from brachial artery
- Course:
- Travels deep to brachioradialis with superficial branch of the radial nerve and veins
- Sits between the tendons of the brachioradialis and flexor carpi radialis in the wrist
Ulnar Artery:
- Origin: Branches from Brachial Artery
- Course:
- Passes between flexor digitorum superficialis and flexor carpi ulnaris
- Travels with the ulnar nerve and ulnar veins
Deep Veins of the Arm and Forearm
Paired Veins:
- Each artery is usually accompanied by smaller paired veins called ‘venae comitantes’
- They have the same names as the arteries (eg. Brachial, radial, ulnar)
Unpaired Veins:
- Subclavian and axillary veins do not have associated venae comitantes and have a single vein associated with them
- Together with the jugular veins the, subclavian veins form the right and left brachiocephalic veins that drain into the superior vena cava
Superficial Veins of the Arm and Forearm
Superficial Veins:
- Located in subcutaneous layer
- Highly variable
- Drian into axillary vein (can be variable)
- Cephalic (located in anterior antebrachium, travels in deltopectoral groove)
- Basilic (located at the medial border of biceps)
- Median Cubital
Venous Drainage:
- Superficial Veins (subcutaneous)
- Perforating Veins (subcutaneous to deep)
- Deep Veins (usually paired and have same name as arteries)
LO6 To describe the structure of the brachial plexus
- Spinal cord runs between each vertebra and down to lumbar region
- Spinal nerves come off spinal cord and become peripheral nerves. Go off to supply muscles, joints, limbs
- Cervical (C1-C8), thoracic (T1-T12), lumbar, sacral, coccygeal
- C5, C6, C7, C8, T1 make up brachial plexus
- Brachial plexus pass under clavicle
- Plexus: coming together and share nerve fibres
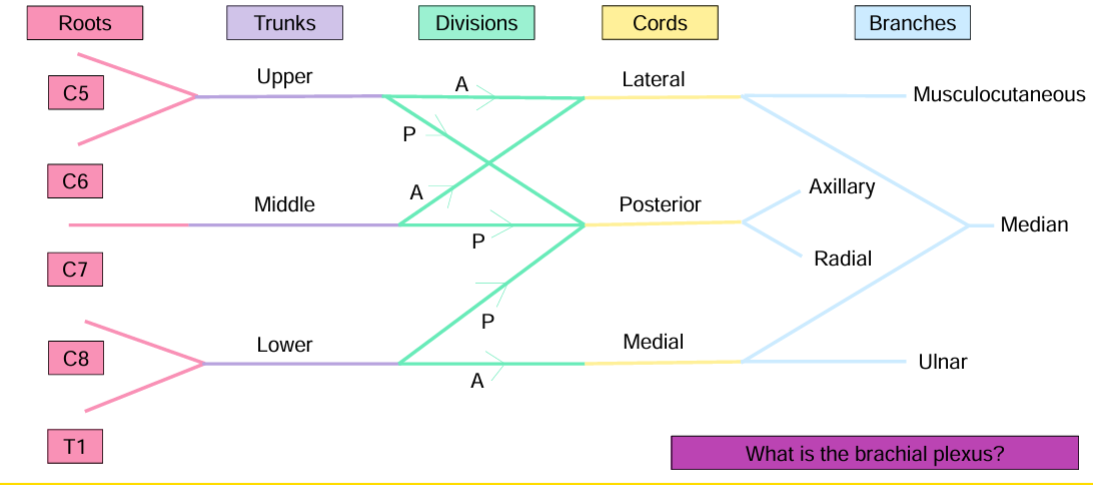
- REMEMBER TO DRINK COLD BEER (RTDCB)
- Roots: Anterior rami of vertebral levels C5-T1 make up brachial plexus
- Trunks: Located between anterior and middle scalene muscles (in neck)
- Division: Every trunk has Anterior and Posterior.
- All posterior divisions join together
- Upper/Middle anterior join. Lower does not move
- Cords: Named according to their position around axillary artery
- Posterior branches travel behind
- Ulnar is medial on arm, hence, medial cord
- Branches: Supply skin and muscles of the arm, forearm and hand
LO7 To describe the formation, course and distribution (structures supplied) by the branches of the brachial plexus
LO8 To correlate lesions of the branches of the brachial plexus to functional and sensory deficits
- Nerves supply all muscles and skin of the upper limb
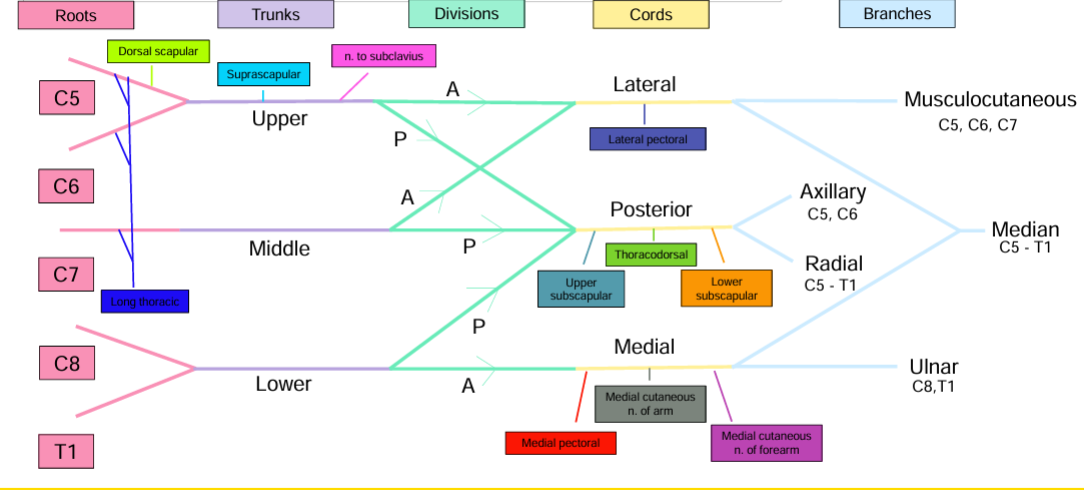
Roots:
- Long Thoracic (C5, C6, C7): Serratus anterior
- Dorsal Scapula (C5): Rhomboid major, rhomboid minor, Levator scapulae
Trunks:
- Upper:
- Suprascapular (C5, C6): Supraspinatus, Infraspinatus
- Subclavius (C5, C6): Subclavius
Divisions:
Cords:
- Lateral:
- Lateral pectoral (C5, C6, C7): Pectoralis Major, Pectoralis Minor
- Posterior:
- Thoracodorsal (C5, C6, C7): Latissimus Dorsi
- Upper Subscapular (C5, C6, C7): Subscapularis
- Lower Subscapular (C5, C6, C7): Subscapularis
- Medial:
- Medial cutaneous nerve of arm: Skin
- Medial cutaneous nerve of forearm: Skin
- Medial pectoral (C5, C6, C7): Pectoralis Major
Branches from the Posterior Cord:
Axillary (C5-C6):
- Supplies:
- Deltoid
- Teres Minor
- Skin covering the lateral upper arm
- Course:
- Passes through quadrangular space
- Winds around the surgical neck of the humerus with posterior circumflex humeral artery
- At risk with a fracture of the surgical neck of the humerus
- Also at risk with dislocation of the glenohumeral joint
- Lesions of the Axillary Nerve affect:
- Flexion beyond first 15°
- Sensation over the lateral upper arm
Radial (C5-T1):
- Supplies:
- Extension of arm and forearm
- Skin over the extensors and dorsum of the hand
- Course in the shoulder and arm:
- Passes through the triangular interval with the profunda brachii artery
- Sits between medial and lateral heads of triceps
- Travels in the intertubercular groove towards the cubital fossa
- Course in cubital fossa:
- Sits between brachialis and brachioradialis
- In front of the lateral epicondyle it divides into superficial and deep branches
- **NOTE: Triceps innervation occurs high in the arm
- Course in forearm and wrist:
- Superficial Branch:
- Sensory
- Travels on anterolateral forearm
- Travels deep to the brachioradialis muscle with the radial artery and veins
- Sits in anatomical snuffbox (located on dorsal surface of the hand)
- Deep Branch:
- Muscular and articular
- Pierces the supinator muscle
- Changes name to posterior interosseous nerve
- Travels along the posterior surface of the interosseous membrane (between radius and ulnar)
- Radial Nerve at risk of:
- Mid-shaft humeral fracture
- Supracondylar fracture
- Penetrating wound to the posterior forearm
- Lesions of the Radial Nerve affect:
- Function of the extension of the arm and forearm
- Sensation over the dorsal surface of the hand, particularly in the area known as the anatomical snuffbox (radial fossa)
Branches from the Lateral Cord:
Musculocutaneous (C5, C6, C7):
- Supplies:
- Muscles of the anterior compartment of the arm
- Skin over the lateral aspect of the anterior forearm
- Course in shoulder and arm:
- Passes through the coracobrachialis muscle
- Travels inferiorly between brachialis and biceps brachii muscles
- Emerges lateral to these muscles and changes its name to the lateral cutaneous nerve of the anterior forearm
- Lesions of the Musculocutaneous Nerve affect:
- Weakened elbow flexion
- Sensory loss in lateral half of anterior forearm
- Reduced biceps reflex
Branches from the Medial Cord:
Ulnar (C8-T1):
- Supplies:
- The flexor carpi ulnaris and the medial ½ of flexor digitorum profundus in the forearm
- The intrinsic muscles of the hand except for the thenar group of muscles and the lateral 2 lumbricals
- Skin over the medial 1½ digits (palmar and dorsal surface)
- Course in arm:
- Passes medial to the brachial artery
- Travels posterior to the medial epicondyle
- Course in forearm and wrist:
- Travels on the medial side of forearm deep to the flexor carpi ulnaris muscle
- Travels with the ulnar artery and veins
- DOES NOT pass through carpal tunnel
- Enters palm on medial side
- Lesions of the Ulnar Nerve affect:
- ELBOW: the flexor carpi ulnaris and the flexor digitorum profundus muscles of the forearm
- The intrinsic group of muscles and medial 2-digit muscles in hand
- WRIST: Sensation over the lateral 1 ½ digits (palmar and dorsal surfaces)
- A person’s ability to form a fist or grip an item
- At risk with medial epicondylar fractures, compression in wrist
- Can cause: Claw Hand
Branch from Lateral and Medial Cords:
Median (C5-T1):
- Supplies:
- The anterior muscles of the forearm except flexor carpi ulnaris and flexor digitorum profundus
- The intrinsic group of muscles in the hand expect for the medial 2 muscles, (supplied by ulnar)
- Skin over palmar the surface of the lateral 3 ½ digits, including finger tips
- Course:
- Travels anteriorly in the arm
- Travels with the brachial artery, beginning lateral to it and then crossing to its medial side
- In cubital fossa: lies between the biceps brachii muscle and the brachial artery
- In forearm: passes between heads of pronator teres
- Travels between the flexor digitorum profundus and flexor digitorum superficialis
- In wrist and hand: passes through carpal tunnel
- Gives off palmar cutaneous branches to the intrinsic group of muscles and the lateral 2 thenar muscles
- Lesions of the Median Nerve affect:
- A person’s ability to form a fist or grip an item
- Hand of Benediction
- Pronator syndrome
- Carpal tunnel syndrome
- At risk with:
- Supracondylar fracture or deep penetrating wound to forearm
- Compression at elbow or wrist
LO9 To describe the difference between dermatomes and myotomes
LO10 To know the myotome, dermatome and peripheral nerve distribution of the upper limb
Dermatome:
- Area of skin supplied by a single spinal nerve
- Severing a spinal nerve will cause loss of sensation over a particular area of skin
- Lots of overlaps of dermatomes in trunk but more defined nerve supply in limbs
- Number and Letter – eg C5
Peripheral Nerve:
- Named nerve eg. Radial nerve
- Input from multiple spinal nerves
- When a spinal nerve enters plexus, their fibres are exchanged and redistributed
- Although some spinal nerves enter plexuses, others do not and the dermatomal pattern remains
Myotome:
- Mass of muscle supplied by a single spinal nerve
- Motor fibres travel in the same peripheral nerves as sensory fibres
- Therefore, upper limb muscles receive motor fibres form several spinal cord levels (or myotomes)
Elbow and Forearm
Lo1 To identify anatomical features of the bones of the forearm
Ulna:
- Medial in forearm
- Large proximal, small distal end
- Olecranon: pointy bit of elbow
- Trochlear notch: articulate with trochlear of humerus
- Coronoid process: stick out ridge on anterior
- Radial notch: head of radius sits there (lateral side)
- Supinator crest and fossa: associated with supinator muscle (lateral side)
- Tuberosity of ulna: on anterior, brachialis attaches here
- Roughening for Anconeus: lateral side for Anconeus muscle
- Interosseous border: (lateral) border between ulna and radius – pointed/sharp
- Head (distal)h: rounded lump
- Styloid process: top of head
Radius:
- Small proximal, large distal end
- Head (proximal)
- Fovea: pit on head, articulate with capitulum of humerus
- Radial tuberosity: biceps brachii attaches here
- Interosseous border: medial and sharpest border – border between radius and ulna
- Ulnar notch: ulna sits there
- Styloid process: lump of bone on lateral side
- Dorsal tubercle: (posterior) can palpate
- Articulates with scaphoid and lunate bone
Lo2 To identify key features of elbow region and forearm on a living person (surface anatomy)
- Medial and lateral epicondyle of humerus
- Olecranon
- Posterior border of ulna
- Styloid process of ulna
- Dorsal tubercle of radius
- Styloid process of radius
- First layer of forearm muscles (digits 2-4 on supinated forearm)
- Palmaris longus
- Flexor carpi radialis
- Flexor carpi ulnaris
- MAYBE: ulnar nerve and artery
- Extensor digitorum tendon on dorsal surface of hand
- Anatomical snuffbox (medial wrist)
Lo3 To understand the structure and function of the elbow and radioulnar joints
Elbow Joint:
- During flexion, coronoid process in coronoid fossa
- During extension, radius in radial fossa
- Articular surfaces:
- Trochlea of humerus with trochlear notch of ulna
- Capitulum of humerus with fovea of radius
- Type:
- Synovial hinge
- Capitulum/fovea is similar to ‘ball and socket’
- Movements:
- Flexion and extension
Elbow Joint Space:
- Communicates with proximal radioulnar joint
- Cushioned with fat pads (protect bone-bone connection during flexion)
- Lined with synovial membrane (continuous with synovial membrane of the proximal radioulnar joint)
- Sacciform recess (filled with synovial fluid, prevents friction between bone and ligament) extends deep to the annular ligament
- Joint capsule is reinforced medially and laterally
- Radius is free from capsular attachment
Elbow Ligaments:
- Lateral (radial) collateral:
- Y-shaped
- From the lateral epicondyle to the annular ligament
- Medial (ulna) collateral:
- Triangular
- 3 bands: anterior, posterior and oblique
- From the medial epicondyle to the coronoid process and olecranon
Bursae:
- Many around the elbow
- Intratendinous olecranon bursa
- Subtendinous olecranon bursa
- Subcutaneous olecranon bursa – deep to skin, elbows rested on hard surface, most clinically relevant
Carrying Angle:
- Ulna axis deviates laterally from that of the humerus in full extension
- Angle keeps arm out from side
- Makes the forearm diverge laterally forming the carrying angle
- Approximately: 10-15° in males, 10-25° in females
Radioulnar Joints:
- Between radius and ulna
- 3 joints
- Bones orientate differently depending on whether arm is in pronation or supination
- Elbow joint capsule does not attach to radius (radius would not be able to move)
Proximal:
- Articular surfaces:
- Head of radius and radial notch of the ulna
- Ligaments:
- Annular:
- Ring-shaped
- Attached to anterior and posterior margins of radial notch
- Holds head of radius against ulna
- Quadrate:
- Attached to lower border or radial notch and medial surface of neck of radius
- Other features:
- Sacciform recess: Prevents friction between radius and annular ligament
- Joint Type:
- Synovial pivot
- Movement:
- Rotation of radius
- Referred to as supination and pronation of the forearm
- Head of radius rotates in the ‘socket’ formed by the annular ligament and the radial notch of the ulna
- Both movements require rotation of the radius around its longitudinal axis
- Pronation = palm of hand faces posteriorly, and dorsum faces anteriorly
- Supination = palm of hand faces anteriorly and dorsum faces posteriorly
Middle:
- Articular surfaces:
- Interosseous borders of the radius and ulna
- Function:
- Holds radius and ulna together during pronation and supination
- Force transfer
- Muscle attachment
- Joint Type:
- Fibrous - syndesmosis
- Movement:
- Most fibrous joints are immovable
- However, a small amount of movement occurs
Distal:
- Articular surfaces:
- Head of ulna and ulna notch of radius
- Function:
- Holds radius and ulna together during pronation and supination
- Force transfer
- Muscle attachment
- Joint Type:
- Synovial pivot
- Movement:
- Articular disc (TFCC – triangular fibrocartilage complex)
- Palmar and dorsal capsular ligaments
- Sacciform recess
Lo4 To correlate the structure of the elbow and radioulnar joints to their functional movements and stability
Interosseus Membrane (between radius and ulna):
- Compression Force:
- Force transmitted through wrist, mainly via radius (larger at wrist)
- Force tightens (central band)
- Force transferred to ulna (as now larger head)
- Force transferred to humerus
- Distraction Force:
- Force loosens the central band of the interosseous membrane
- Oblique cord (proximal – run from radius to ulna), annular ligament and brachioradialis tighten to support the load
Lo5 To understand how stability and function of the elbow and radioulnar joints can be altered as a result of dislocation, fractures and muscular injuries
Dislocation of proximal radioulnar joint:
- Common in young children
- Caused by distraction forces applied to forearm and hand
- Head of radius displaced anteriorly
- Head may be palpated in cubital fossa
- Can cause tearing of annular ligament
- Treatment consist of supination of forearm while elbow is flexed
Dislocation of Elbow Joint:
- Posterior dislocation is most common (easy to push ulna backwards)
- Caused by hyperextension of blow that pushes ulna posteriorly
- Often associated with a fracture of the coronoid process
- Can also have an associated fracture of the radial head or olecranon
Bursitis:
- Can be injured during falls on elbows, exposed to infection from abrasions of skin covering olecranon, inflamed by excessive pressure and friction
- Subtendinous olecranon bursa can also be inflamed by repeated flexion-extension of the forearm
Colles Fracture:
- Extra-articular fracture of the distal radius
- Referred to as ‘broken wrist’ (not actually wrist)
- Caused by falling on an outstretched wrist (pronation, extension of wrist and forearm)
- Particularly common in elderly females (osteoporosis)
- Often results in ‘dinner fork’ deformity
Tennis Elbow:
- Lateral epicondylitis
- Repetitive use of extensor muscles, particularly ECRB
- ECRB stabilises wrist when elbow is extended, and hand is pronated (eg. During backhand in tennis)
- Overuse causes micro-tears in ECRB where it attaches to the lateral epicondyle
- Pain felt over the lateral epicondyle on wrist extension
- Pain when gripping and reduced grip strength
- Also common in labourers that use heavy tools, workers that grip or lift repetitively, painters
Golfers Elbow:
- Medial epicondylitis
- Cause by repetitive use of flexor and pronator muscles
- Causes micro-tears in the common flexor tendon
- Pain felt over the medial epicondyle on the wrist flexion (eg gold swing)
- Pain when gripping and reduced grip strength
- Also common in, tennis players with powerful forehand with lots of topspin,
- Athletes with poor throwing, weightlifting or stroke techniques in racquet sport,
- Admin staff with a lot of typing,
- Occupations with forceful gripping actions, heaving lifting, or constant exposure to vibrations at the elbow
Pronator Syndrome:
- Entrapment of median nerve
- Compression of nerve between heads of pronator teres
- Trauma or muscle hypertrophy
- Pain in proximal anterior forearm
- Hypesthesia of the palmar aspects of the lateral 3 ½ digits and adjacent palm (or pins and needles)
- Often occurs during activities with repeated pronation
- Weakness in deeper muscles – FPL, FDP, PQ (and deep hand muscles supplied by median nerve)
Lo6 To identify normal anatomical features and injuries on radiographs of the elbow and radioulnar joints
Elbow ROM:
- Activities of daily living (ADL)
- Need ~30-130° of flexion
- 0° in extension
Wrist ROM:
- Between 50° of pronation and 50° of supination
- Mostly in pronation throughout daily living
Normal elbow:
- Extension: tip of olecranon and epicondyles in a straight line
- Flexion: epicondyles form the base of a triangle, olecranon forms the apex
- Important for diagnosing dislocation
Lo7 To know the muscles of the elbow region and forearm (attachments, nerve supply & functions)
Muscles of Elbow Joint:
Arranged into 2 compartments: anterior and posterior
Anterior:
- Shoulder flexors
- Elbow flexors
- Biceps brachii, coracobrachialis and brachialis
- Supplied by musculocutaneous
Biceps Brachii:
- Attachments:
- Scapula:
- Long Head: supraglenoid tubercle and labrum
- Short Head: coracoid process
- Radius (radial tuberosity and deep forearm fascia)
- Actions:
- Weak flexor of shoulder
- Short head resists shoulder dislocation
- Supinates forearm
- Flexes forearm
- Nerve Supply:
- Musculocutaneous Nerve
Brachialis:
- Attachments:
- Humerus (anterior distal ½)
- Ulna (coronoid process and ulnar tuberosity)
- Actions:
- Prime flexor of elbow joint
- Nerve Supply:
- Musculocutaneous Nerve
Brachioradialis (forearm):
- Attachments:
- Humerus (proximal 2/3 of supracondylar ridge)
- Radius (distal, lateral to styloid process)
- Actions:
- Flexes forearm (especially in mid-pronation)
- Pronation (return to mid-pronation)
- Supination (return to mid-pronation)
- Nerve Supply:
- Radial Nerve
Flexion:
- Brachialis: recruited first
- Biceps Brachii: stronger when flexed and supinates simultaneously (used when resistance applied)
- Brachioradialis (forearm): assists with flexion, places hand into mid-pronation
Posterior:
- Shoulder extensors
- Elbow extensors
- Triceps brachii and anconeus
- Supplied by radial
Triceps Brachii:
- Attachments:
- Scapula: Long head – infraglenoid tubercle
- Humerus (posterior):
- Lateral head: superior to radial groove
- Medial head: inferior to radial groove
- Ulna: (lateral and medial heads blend) proximal end of olecranon and deep fascia
- Actions:
- Extend shoulder (weak)
- Extend forearm
- Nerve Supply:
- Radial Nerve
Anconeus:
- Attachments:
- Humerus (lateral epicondyle)
- Actions:
- Extend forearm
- Nerve Supply:
- Radial Nerve
Extension:
- Anconeus: recruited first
- Triceps Brachii (main extensor): medial head = workhorse, lateral head = recruited next, long head = recruited last (back-up)
Muscles of Radioulnar Joints:
- Supination
- Supinator – recruited first
- Biceps brachii – when supinating against resistance
- Brachioradialis – when in pronated position
Supinator:
- Attachments:
- Humerus (lateral epicondyle)
- Ulna (supinator crest and supinator fossa)
- Radius (proximal 1/3 of anterior, lateral and posterior surface)
- Actions:
- Supinate forearm
- Nerve Supply:
- Radial nerve (deep branch)
Biceps Brachii:
- Attachments:
- Scapula:
- Long Head: supraglenoid tubercle and labrum
- Short Head: coracoid process
- Radius (radial tuberosity and deep forearm fascia)
- Actions:
- Weak flexor of shoulder
- Short head resists shoulder dislocation
- Supinates forearm
- Flexes forearm
- Nerve Supply:
- Musculocutaneous Nerve
Brachioradialis:
- Attachments:
- Humerus (proximal 2/3 of supracondylar ridge)
- Radius (distal, lateral to styloid process)
- Actions:
- Flexes forearm (especially in mid-pronation)
- Pronation (return to mid-pronation)
- Supination (return to mid-pronation)
- Nerve Supply:
- Radial Nerve
- Pronation
- Pronator quadratus – (smaller) recruited first
- Pronator teres - when pronating against resistance
- Brachioradialis – when in supinated position
Pronator Quadratus:
- Attachments:
- Ulna (distal ¼ of anterior surface)
- Radius (distal ¼ of anterior surface)
- Actions:
- Pronate forearm
- Nerve Supply:
- Median Nerve
Pronator Teres:
- Attachments:
- Ulna (coronoid process)
- Humerus (medial epicondyle)
- Radius (lateral surface of radial shaft)
- Actions:
- Pronate forearm
- Flexes forearm (weakly)
- Nerve Supply:
- Median Nerve
Muscles of the Forearm:
- Arranged into 2 compartments – anterior and posterior
- Anterior: wrist flexors, forearm pronators, pronantor teres, FCR, palmaris longus, FCU, FDS, FDP, FPL, pronator quadratus
- Supplied by median or ulnar nerve
- Posterior: wrist extensors, forearm supinators, brachioradialis, ECRL, ECRB, ED, EDM, ECU, supinator, APL, EPB, EPL, EI
- Supplied by radial nerve (deep branches)
Anterior Compartment:
- 4 layers
- Superficial to deep, 4:1:2:1 muscle arrangement
- 1st and 2nd layer muscles have attachment to medial epicondyle (common flexor origin)
- ALL supplied by MEDIAN NERVE
- EXCEPT flexor carpi ulnaris and medial ½ of flexor digitorum profundus (ulnar)
Anterior Layer 1:
Pronator Teres:
- Attachments:
- Ulna (coronoid process)
- Humerus (medial epicondyle)
- Radius (lateral surface of radial shaft)
- Actions:
- Pronate forearm
- Flexes forearm (weakly)
- Nerve Supply:
- Median Nerve
Palmaris longus (NOT ALWAYS PRESENT):
- Attachments:
- Humerus (medial epicondyle)
- Flexor retinaculum (distal ½)
- Palmar aponeurosis (apex)
- Actions:
- Flex wrist
- Tenses palmar aponeurosis
- Nerve Supply:
- Median Nerve
Flexor Carpi Radialis (FCR):
- Attachments:
- Humerus (medial epicondyle)
- Metacarpals (base of 2nd)
- Actions:
- Flexes wrist
- Abducts hand
- Nerve Supply:
- Median Nerve
Flexor Carpi Ulnaris (FCU):
- Attachments:
- Humerus (medial epicondyle)
- Ulnar (olecranon and posterior border of ulna)
- Pisiform
- Hook of hamate
- 5th metacarpal
- Actions:
- Flexes wrist
- Adducts hand
- Nerve Supply:
- ULNAR Nerve
Anterior Layer 2:
Flexor Digitorum Superficialis (FDS):
- Attachments:
- Radius (superior ½ of anterior border)
- Humerus (medial epicondyle)
- Ulna (coronoid process)
- Hand (shaft of middle phalanx of digits 2-5)
- Actions:
- Flexes PIP joints of digits 2-5
- Nerve Supply:
- Median Nerve
Anterior Layer 3:
Flexor Digitorum Profundus (FDP):
- Attachments:
- Ulna (proximal ¾ of medial and anterior surfaces)
- Interosseous membrane
- Base of distal phalanges digits 2-5
- Actions:
- Flexes DIP joints of digits 2-5
- Nerve Supply:
- Medial ½ = ULNAR nerve
- Lateral ½ = median nerve
Flexor Pollicis Longus (FPL):
- Attachments:
- Radius (anterior surface)
- Interosseous membrane
- Base of distal phalanx of 1st digit (thumb)
- Actions:
- Flexes PIP and DIP joint of 1st digit
- Nerve Supply:
- Median Nerve (anterior interosseous nerve)
Anterior Layer 4:
Pronator Quadratus:
- Attachments:
- Ulna (distal ¼ of anterior surface)
- Radius (distal ¼ of anterior surface)
- Actions:
- Pronate forearm
- Nerve Supply:
- Median Nerve
Posterior Compartment:
- Superficial (6 muscles) and deep (5 muscles)
- ECRB, ED, EDM, ECU and supinator: attach to lateral epicondyle (common extensor origin)
- ALL muscles supplied by radial nerve (deep branches)
Posterior Superficial:
Brachioradialis:
- Attachments:
- Humerus (proximal 2/3 of supracondylar ridge)
- Radius (lateral surface of distal end, proximal to styloid process)
- Actions:
- Weak flexion of forearm (especially in mid-pronation)
- DOES NOT CROSS WRIST JOINT
- Nerve Supply:
- Radial Nerve
Extensor Carpi Radialis Longus:
- Attachments:
- Humerus (lateral supracondylar ridge
- 2nd metacarpal (base of dorsal aspect)
- Radius (lateral surface of radial shaft)
- Actions:
- Extend wrist
- Abduct wrist
- Nerve Supply:
- Radial Nerve
Extensor Carpi Radialis Brevis:
- Attachments:
- Humerus (lateral epicondyle)
- 3rd metacarpal (base of dorsal aspect)
- Actions:
- Extend wrist
- Abduct wrist
- Nerve Supply:
- Radial Nerve
Extensor Digitorum:
- Attachments:
- Humerus (lateral epicondyle)
- Extensor expansion (of digits 2-5)
- Actions:
- Extend digits 2-5 at MCP and IP joints
- Nerve Supply:
- Radial Nerve
Extensor Digiti Minimi:
- Attachments:
- Humerus (lateral epicondyle)
- Extensor expansion of digit 5 (pinky)
- Actions:
- Extend digit 5 at MCP and IP joints
- Nerve Supply:
- Radial Nerve
Extensor Carpi Ulnaris:
- Attachments:
- Humerus (lateral epicondyle)
- Ulna (posterior border)
- 5th metacarpal (base of dorsal aspect)
- Actions:
- Extend wrist
- Abduct wrist
- Nerve Supply:
- Radial Nerve
Posterior Deep:
Supinator:
- Attachments:
- Humerus (lateral epicondyle)
- Ulna (supinator crest and supinator fossa)
- Radius (proximal 1/3 of anterior, lateral and posterior surface)
- Actions:
- Supinate forearm
- Nerve Supply:
- Radial nerve (deep branch)
Abductor Pollicis Longus:
- Attachments:
- Ulna (posterior surface, proximal ½)
- Radius (posterior surface, proximal ½)
- Interosseous membrane
- 1st metacarpal (base of dorsal aspect)
- Actions:
- Abducts 1st digit
- Extends CMC joint of 1st digit
- Nerve Supply:
- Radial nerve (posterior interosseous branch)
Extensor Pollicis Brevis:
- Attachments:
- Radius (posterior surface of distal 1/3)
- Interosseous membrane
- Proximal phalanx of 1st digit (base of dorsal aspect)
- Actions:
- Extends CMC and MCP joints of 1st digit
- Nerve Supply:
- Radial nerve (posterior interosseous branch)
Extensor Pollicis Longus:
- Attachments:
- Ulna (posterior surface of middle 1/3)
- Interosseous membrane
- Proximal phalanx of 1st digit (base of dorsal aspect)
- Actions:
- Extends 1st digit at MCP and IP joints
- Nerve Supply:
- Radial nerve (posterior interosseous branch)
Extensor Indicis:
- Attachments:
- Ulna (posterior surface of distal 1/3)
- Interosseous membrane
- Extensor expansion (of digit 2)
- Actions:
- Extends digit 2
- Nerve Supply:
- Radial nerve (posterior interosseous branch)
Lo8 To know the blood vessels and nerves of the forearm
- Median nerve travels between anterior layers 3 and 4
Ulnar artery:
- Origin:
- Branches from the brachial artery
- Course:
- Passes between the flexor digitorum superficialis and flexor carpi ulnaris
- Travels with the ulnar nerve and veins
Ulnar Nerve:
- Origin:
- Medial cord of the brachial plexus
- Course:
- Travels posterior to the medial epicondyle
- Travels on the medial side of the forearm deep to the flexor carpi ulnaris
- Travels with ulnar artery and veins
- Supplies:
- Flexor carpi ulnaris and the medial ½ of the flexor digitorum profundus
Radial Artery:
- Origin:
- Branches from the brachial artery
- Course:
- Travels deep to brachioradialis with the superficial branch of the radial nerve and radial veins
- Sits between the tendons of brachioradialis and flexor carpi radialis in wrist
Radial Nerve:
- Origin:
- Posterior cord of the brachial plexus
- Course:
- Sits between brachialis and brachioradialis
- In front of the lateral epicondyle it divides into superficial and deep branches
- Superficial:
- Travels on anterolateral forearm
- Travels deep to the brachioradialis with radial artery and veins
- Deep:
- Pierces supinator
- Changes name to posterior interosseous nerve
- Travels along posterior surface of interosseous membrane
- Supplies:
- Superficial: skin over the anterior of the arm and forearm and dorsum of hand
- Deep: extension of the wrist and fingers
Median Nerve:
- Origin:
- Medial and lateral cord of the brachial plexus
- Course:
- Lies between biceps brachii the and the brachial artery
- Passes between heads of pronator teres
- Travels between flexor digitorum profundus and flexor digitorum superficialis
- Supplies:
- The anterior and intrinsic muscles of forearm EXCEPT flexor carpi ulnaris and medial ½ of flexor digitorum profundus
- Skin over palmar surface of lateral 3 ½ digits, including fingertips
Wrist and Hand
Lo1 To identify anatomical features of the bones of the wrist and hand
Distal Radius:
- Dorsal tubercle on posterior. Extensor pollicis longus tendon runs around
- Ulnar notch
- Styloid process on lateral side
- Distal view has facet for scaphoid and lunate bone (Lateral to medial)
- Interosseous border = sharp
- Posterior border = pointed
- Anterior border= smooth/round
Distal Ulna:
- Head
- Styloid process (attachment of articular disc)
- Posterior border = sharp (follow olecranon down)
Carpal Bones:
- 8 bones – 4 in distal row, 4 in proximal row
- Proximal – (L to M) Lunate and Scaphoid (articulate with radius), triquetrum and pisiform
- Distal – (L to M) Trapezium (thumb), trapezoid, capitate, hook of hamate
Skeleton of Hand:
- 8 carpal bones in wrist
- 5 metacarpals
- 5 proximal phalanges
- 4 middle phalanges
- 5 distal phalanges
- All have base, body, head (proximal to distal)
Lo2 To identify key features of the wrist and hand on a living person (surface anatomy)
- Dorsal tubercle
- Styloid process (radius and ulna)
- Pisiform
- Hook of hamate
- Palmaris longus
- Flexor carpi ulnaris
- Flexor carpi radialis
- Radial artery
- Thenar eminence
- Hypothenar eminence
- Anatomical snuffbox
- Cephalic vein (lateral side)
- Dorsal venous network (wrist posterior)
- Extensor digitorum tendons
Lo3 To understand the structure and function of the radiocarpal joint and the joints of the hand
Wrist Joint (Radiocarpal Joint):
- Articular surfaces
- Distal radius and the lunate and scaphoid
- Articular disc and the radius and ulna
- Ulna is NOT part of joint
- Type
- Synovial Condyloid
- Movements
- Flexion/Extension
- Abduction/Adduction
- **Circumduction
Ligaments:
- Ulnar collateral carpal ligament: Stabilise ulna side of joint
- Radial collateral carpal ligament: Stabilise radial side of joint
- Dorsal radiocarpal ligament
- Palmar radiocarpal ligament
- Palmar ulnocarpal ligament
- Intercarpal ligaments
Midcarpal and Intercarpal Joints:
- Synovial plane
- Stabilised by intercarpal ligaments
- Supplement movement at the wrist joint and increase overall ROM
- Intercarpal: between each carpal bone
- Midcarpal: between the proximal and distal row of carpal bones
Interphalangeal Joints (PIP and DIP):
- Synovial hinge
- Flexion/extension
Metacarpophalangeal Joint (MCP):
- Synovial Condyloid
- Flexion/extension
- Adduction/abduction
Carpometacarpal Joints (CMC):
- Synovial plane
- EXCEPT 1st CMC is saddle synovial
- Flexion/extension
- Adduction/abduction
- Axial rotation (Opposition)
Intermetacarpal Joints:
- Synovial Plane
Ligaments:
- Collateral Ligaments:
- On sides of metacarpophalangeal and interphalangeal joints
- Stabilise side of joints
- Palmar Ligaments/Plates:
- Fibrocartilage plate
- Firmly attached to proximal phalanx
- Loosely attached to metacarpal
- Protect joint surfaces
- Help prevent the tendons in the forearm flexors getting impinged in the joint (during flexion)
- Deep Transverse Metacarpal Ligaments:
- Bind the heads of metacarpals 2-5
- Attach to palmar plates
- Limit abduction of digits 2-5
Lo4 To correlate the structure of the radiocarpal joint and the joints of the hand to their functional movements and stability
- Medial:
- Flexor carpi ulnaris
- Extensor carpi ulnaris
- **Adduct wrist
- Lateral:
- Flexor carpi radialis
- Extensor carpi radialis longus
- Extensor carpi radialis brevis
- **Abduct wrist
Movement Axis:
- Midline through capitate, lunate and radius
- Slightly more flexion than extension (small difference)
- 7° abduction vs 30° adduction – styloid process of radius inhibits abduction, more proximal and smaller styloid process at ulna
Lo5 To describe the attachment points of the long flexor and extensor tendons in the hand
Synovial Sheaths:
- Wrap around tendons to stop friction
Extensor Retinaculum:
- Band of fibrous tissue
- Holds tendons against bone
- ~1 per extensor tendon
Flexor Retinaculum:
- Forms roof of carpal tunnel
- 1 synovial sheath for all flexor tendons
- 1 separate sheath for flexor pollicis longus
- Attach to hook of hamate, pisiform, scaphoid tubercle, trapezium tubercle
Flexor Sheath (Fibrous Digital Sheath):
- Form tunnel for long flexor tendons to pass through
- Hold tendons close to phalanges to prevent ‘bowstrings’
- A synovial sheath encloses the tendons to prevent friction
- Sheaths have 2 fibre patterns; transverse (straight across), cruciate (cross)
Extensor Tendons:
- Surrounded by synovial sheaths
- Pass deep to extensor retinaculum
- Can attach to:
- Carpals
- Metacarpals
- Proximal phalanges
- Distal phalanges
- Extensor expansion
Extensor Expansion (Dorsal Digital Hood):
- Flattened triangular expansion of extensor digitorum tendons
- Passes around the sides of the MCP joint and assists in stabilising the joints
- Important attachment point for some intrinsic muscles of hand:
- Lumbricals
- Interossei
Lo6 To describe the anatomical snuffbox and carpal tunnel including structure, contents and clinical relevance
Carpal Tunnel:
- Pass deep to flexor retinaculum
- Except palmaris longus (attaches to retinaculum and palmar aponeurosis) or flexor carpi ulnaris, flexor carpi radialis
- Most pass-through carpal tunnel:
- 4 tendons of flexor digitorum superficialis
- 4 tendons of flexor digitorum profundus
- Tendon of flexor pollicis longus
- Median nerve
- Formed by: distal row of carpal bones, flexor retinaculum
Anatomical Snuffbox:
- Triangular depression on the posterolateral wrist formed by the extensor tendons passing into the thumb
- *Identifiable when thumb in hitch-hiking position
- Borders:
- Lateral: Extensor pollicis brevis and abductor pollicis longus
- Medial: Extensor pollicis longus
- Floor: Scaphoid and Trapezium
- Contents: Radial artery (pulse can be felt)
- Passing subcutaneously:
- Superficial branch of radial nerve
- Origin of cephalic vein
Lo7 To describe the fascia of the hand and associated pathologies
Palmar Aponeurosis (Fascia):
- Triangular shape
- Apex located proximally
- Base located distally
- Fibres run in two directions; longitudinal (follow finger) and transverse (between longitudinal)
- Connected to skin
- Blends with digital sheaths of the flexor tendons
- Palmaris longus attaches
Dupuytren’s Contracture:
- Often bilateral
- Tends to occur in men >50 years
- Usually affects 4th and 5th digits
- Progressive changes in palmar aponeurosis:
- Shortening (pull digits toward palm)
- Thickening
- Fibrosis
- Treatment involves surgical excision of all fibrotic parts of the palmar aponeurosis
Lo8 To describe traumas and pathologies associated with the wrist and hand
L11 To identify normal anatomical features and injuries on radiographs of the wrist and hand
Scaphoid Fracture:
- Most frequently fractured carpal bone
- Caused by fall on outstretched hand
- Most common fracture site is ‘waist’ (narrowest)
- Pain and tenderness located:
- Anatomical snuffbox
- Palpating floor of snuffbox will cause pain
- Initial X-ray may not reveal fracture.
- Cut off blood supply to proximal end, leading to necrosis and bone shrinkage
Lo9 To know the muscles of the hand (nerve supply and functions)
- Perform intricate and precise movements of the hand
- Arranged into 5 compartments
- Thenar: Move 1st digit, Median nerve
- Central: Move 2-5th digits. Median or Ulnar nerve
- Hypothenar: Move 5th digit. Ulnar nerve
- Adductor: Move 1st digit, Ulnar nerve
- Interosseous: Move 1-5th digits, Ulnar nerve
**Don’t need to know attachments
Thenar Muscles:
Abductor Pollicis Brevis:
- Attachments:
- Flexor retinaculum
- Scaphoid
- Trapezium
- Base of proximal phalanx of thumb (lateral side)
- Action:
- Abduct thumb
- Assists with opposition
- Nerve Supply:
- Median Nerve
Flexor Pollicis Brevis:
- Attachments:
- Flexor retinaculum
- Scaphoid
- Trapezium
- Base of proximal phalanx of thumb (lateral side)
- Action:
- Flexes thumb
- Nerve Supply:
- Median Nerve
Opponens Pollicis (deep):
- Attachments:
- Flexor retinaculum
- Scaphoid
- Trapezium
- 1st metacarpal (lateral side)
- Action:
- Opposes thumb (medially rotate and draws 1st metacarpal to centre of palm)
- Nerve Supply:
- Median Nerve
Central Muscles:
Lumbricals 1 and 2:
- Attachments:
- Lateral 2 tendons of FDP (unipennate)
- Extensor expansion of digits 2-5 (lateral side)
- Action:
- Flexes MCP joints digits 2-5
- Extend IP joints digits 2-5
- Nerve Supply:
- Median Nerve
Lumbricals 3 and 4:
- Attachments:
- Medial 3 tendons of FDP (bipennate)
- Extensor expansion of digits 2-5 (lateral side)
- Action:
- Flexes MCP joints digits 2-5
- Extends IP joints of digits 2-5
- Nerve Supply:
- Ulnar Nerve
Hypothenar Muscles:
*may see palmaris brevis covering hypothenar muscles (supplied by Ulnar)
Abductor Digiti Minimi:
- Attachments:
- Pisiform
- Base of proximal phalanx of digit 5 (medial side)
- Action:
- Abduct digit 5
- Assists with flexion
- Nerve Supply:
- Ulnar Nerve
Flexor Digit Minimi Brevis:
- Attachments:
- Flexor retinaculum
- Hook of hamate
- Base of proximal phalanx of digit 5 (medial side)
- Action:
- Flexes proximal phalanx of digit 5 (medial side)
- Nerve Supply:
- Ulnar Nerve
Opponens Digiti Minimi (Deep):
- Attachments:
- Flexor retinaculum
- Hook of hamate
- 5th metacarpal (medial side)
- Action:
- Draw 5th metacarpal anteriorly and rotate towards centre of palm
- Nerve Supply:
- Ulnar Nerve
Adductor Pollicis:
- Attachments:
- Transverse head: shaft of 3rd metacarpal (anteriorly)
- Oblique head: base of 2nd and 3rd metacarpals, capitate and adjacent carpals
- Base of proximal phalanx of thumb (medial side)
- Action:
- Adduct thumb
- Nerve Supply:
- Ulnar Nerve
Interossei Muscles (deep and between bones):
Dorsal Interossei (4):
- Attachments:
- Adjacent sides of 2 metacarpals (bipennate)
- Bases of proximal phalanges
- Extensor expansion of digits 2-4
- Action:
- Abduct digits 2-4
- Assist with flexion of MCP joints
- Assist with extension of IP joints
- Nerve Supply:
- Ulnar Nerve
**DAB – Dorsal abduct
Palmar Interossei (3):
- Attachments:
- Palmar surface of 2nd, 4th and 5th metacarpals (unipennate)
- Bases of proximal phalanges
- Extensor expansion of digits 2, 4, 5
- Action:
- Adduct digits 2, 4, 5
- Assist with flexion of MCP joints
- Assist with extension of IP joints
- Nerve Supply:
- Ulnar Nerve
**PAD – Palmar adduct
L10 To describe the purpose of different hand grips including types of power and precision grips
Prehension (Grip):
- The way in which hand grips an object depends on shape, size, weight and use
- Generally, 2 types:
- Power:
- Thumb, finger and palm involved
- Used when considerable force required
- Precision:
- Thumb and fingers involved
- Object usually small and fragile
Power Grip:
- Long flexors and extensors fix the position of wrist
- Long finger flexors and intrinsic muscles grip the object
- Oblique Palmar: most powerful, hand and fingers wrap around object whose long axis lies across palm
- Ball: ball shaped and enclosed by palm
- Span: palm may not make contact increasing power needed in fingers and thumb
- Cylinder: object held transversely across palm, digits and thumb
- Hook: secure but only 1 direction, thumb not involved in true hook
Precision Grip:
- Object held between pads of digits
- Action involves rotation at CMC and MCP joint of thumb
- Also involve rotation at MCP joints of digits
- Pincer: tips of pads or nails used, finest and most precise
- Tripod: palmar surface of thumb, digit 2 and possible other digits (hold pen)
- Pinch: pads of thumb and digit 2 oppose, tested by pulling sheet of paper out of grip
- Key: pad of thumb presses against side of digit 2, less fine but strong
L12 To know the blood vessels and nerves of the wrist and hand, and understand the effects of nerve lesions on the function of the wrist and hand
Superficial and Deep Palmar Arches:
- Formed by anastomosis of the radial and ulnar arteries
- Superficial is easy to view, lies mid-palm and more distal
- Deep is close to bone
Median Nerve:
- Course:
- Passes through carpal tunnel
- Gives off branches to the thenar group of muscles and the lateral 2 lumbricals
- Lesion Affects:
- Sensation over dorsal surface of the lateral 3 ½ digits and tips of fingers
- Ability to form a fist or grip an object
Carpal Tunnel Syndrome:
- Causes increase in the size of the structures passing through tunnel.
- Including fluid retention, infection, swelling of tendons or synovial sheaths
- Compress the median nerve
- May result in
- Paraesthesia
- Hypoesthesia
- Anaesthesia
- Progressive loss of coordination and strength of thumb
- Atrophy of thenar eminence
Hand of Benediction:
- Caused by lesion of median nerve
- Symptoms:
- When the person tries to form a fist, the ‘hand of benediction’ is formed instead
- Flexion of the PIPs of digits 1-3 is lost and weakened in digits 4-5
- Flexion of the DIPs of 2-3 is also lost
- Thenar muscle function is also lost
- Sensation over the lateral palm and palmar surface and finger tips of the lateral 3 ½ digits is also affected
Ulnar Nerve:
- Course:
- Travels with ulnar artery and veins
- DOES NOT go through carpal tunnel
- Enters palm on medial side
- Gives off branches to the hypothenar group of muscles and the medial 2 lumbricals (3 and 4)
- Also supplies palmar and dorsal interossei
- Lesion Affects:
- Sensation over medial 1 ½ digits
- Ability to form a fist or grip an item
- Ability to flex and extend digits
Claw Hand:
- Caused by lesion of ulnar nerve
- Symptoms:
- At elbow:
- Wrist adduction impaired
- Flexion at wrist causes hand to move laterally
- At wrist:
- When person attempts to form fist, ‘claw’ hand is formed
- Hyperextended 4th and 5th MCP joints
- Unable to flex the DIP of the 4th and 5th digits
- Ability to form fist or grip an item
- Loss of sensation over medial 1 ½ digits
- **Also adductor pollicis
Radial Nerve:
- Course:
- Superficial:
- Sensory
- Travels deep to the brachioradialis muscle with radial artery and veins
- Sits in region known as anatomical snuffbox on dorsum of hand
- Deep:
- Muscular and articular
- Ends at wrist after supplying all extensor muscles of forearm
- Lesion Affects:
- Sensation over the lateral side of dorsum aspect of hand
- Sensation over the anatomical snuffbox
Wrist Drop:
- Caused by mid-shaft humeral fracture, supracondylar fracture, penetrating wound to posterior forearm
- Symptoms:
- Unable to extend wrist
- Unable to extend 1st digit and MCP joints of digits 2-5
- **AT wrist, only superficial branch impacted. ONLY sensation lost