In Class
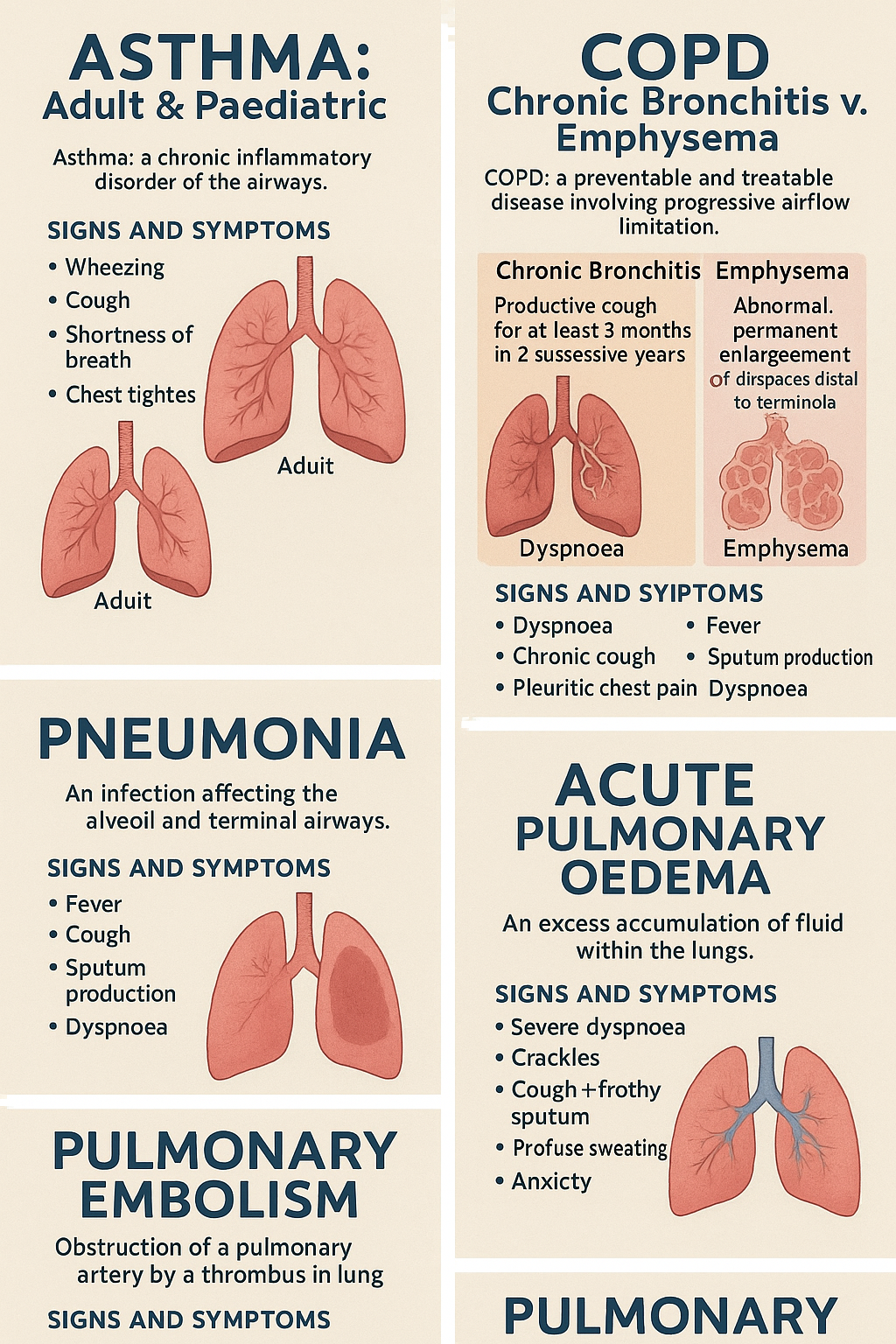
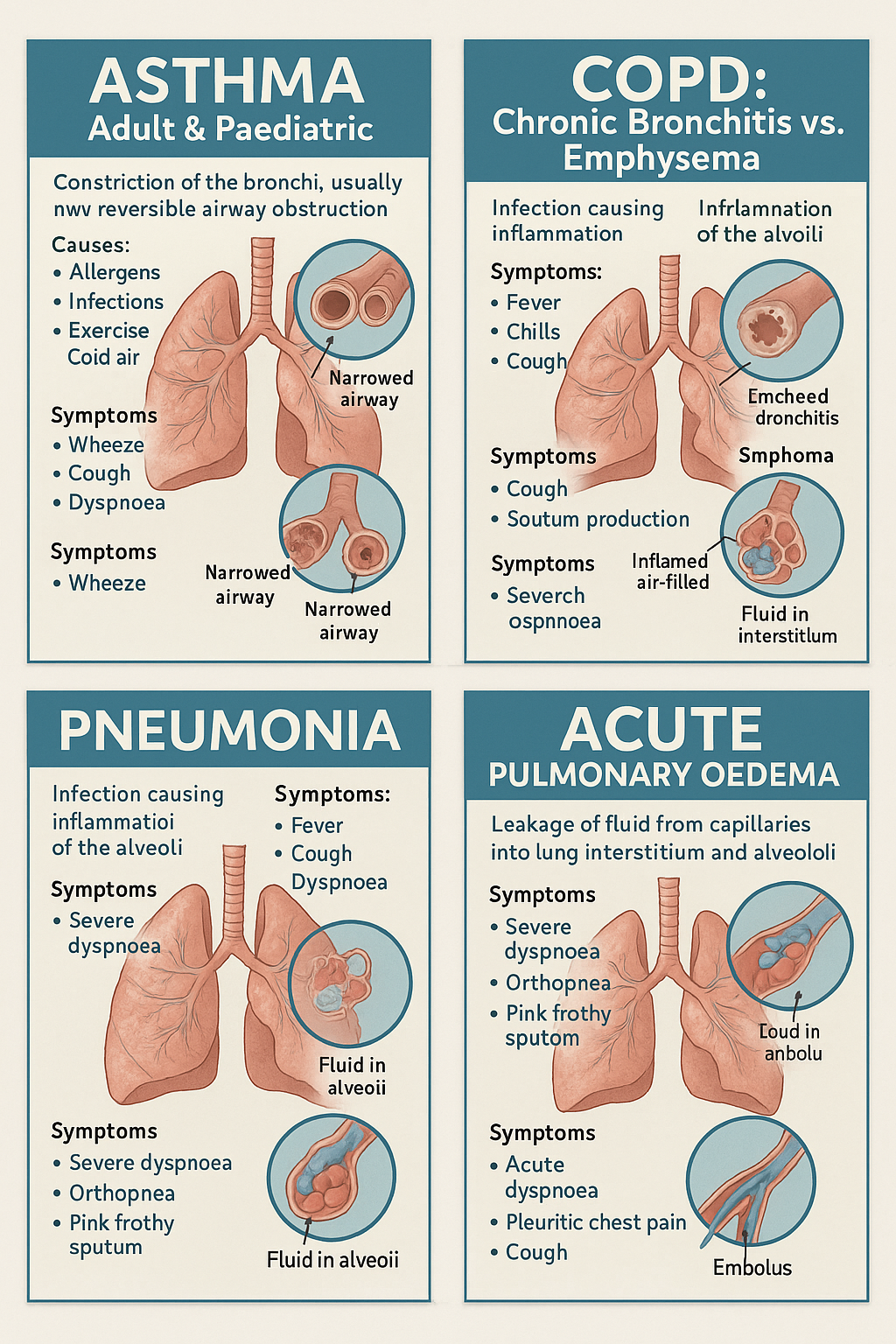
🌬 Asthma (Adult & Paediatric)
Patho: Chronic inflammation → bronchoconstriction + mucus
Triggers: Allergens, smoke, cold air, exercise, infections
Symptoms: Wheezing, SOB, cough, chest tightness
Assessment: PEFR, ABG, auscultation (wheezing)
Mnemonics:
ASTHMA
A – Accessory muscle use
S – SOB (shortness of breath)
T – Tight chest
H – High-pitched wheeze
M – Mucus
A – Anxiety
Nursing Care:
O2 if < 92%
Administer bronchodilators (e.g. albuterol)
Corticosteroids (e.g. prednisone)
Position upright
Educate on inhaler use & trigger avoidance
😤 COPD: Chronic Bronchitis vs. Emphysema
Chronic Bronchitis = "Blue Bloater"
Emphysema = "Pink Puffer"
Chronic Bronchitis Mnemonic – BLUE:
B – Big mucus (productive cough)
L – Lung sounds: wheeze/crackles
U – Underoxygenated (cyanosis)
E – Edema (cor pulmonale)
Emphysema Mnemonic – PINK:
P – Pursed lips
I – Increased CO2 retention
N – No cyanosis early
K – Keep using accessory muscles
Nursing Care (Same for both):
Administer O2 cautiously (target 88–92%)
Bronchodilators + steroids
Encourage fluids
Smoking cessation
Pulmonary rehab
🦠 Pneumonia
Patho: Infection → alveoli fill with fluid
Causes: Bacteria, viruses, fungi, aspiration
Symptoms: Fever, chills, cough, sputum, SOB, chest pain
Mnemonic: PNEUMONIA
P – Productive cough
N – Neuro (confusion in elderly)
E – Elevated WBC
U – Unusual breath sounds (crackles)
M – Mild to high fever
O – Oxygen ↓
N – Nausea
I – Increased HR/RR
A – Activity intolerance
Nursing Care:
Assess respiratory status
Antibiotics/antivirals
Fluids + nutrition
Incentive spirometry
Monitor ABGs, vitals, sats
💧 Acute Pulmonary Oedema
Patho: Fluid in alveoli due to left heart failure
Symptoms: Sudden SOB, pink frothy sputum, crackles, anxiety
Mnemonic: FLASH
F – Frothy sputum
L – Lung crackles
A – Anxiety
S – Sweating
H – Hypoxia
Nursing Care:
Sit upright
High-flow O2
Administer diuretics (furosemide)
Morphine for anxiety/SOB
Monitor ECG, BP, sats
🩸 Pulmonary Embolism (PE)
Patho: Blood clot in pulmonary artery
Causes: DVT, immobility, surgery
Symptoms: Sudden SOB, chest pain, cough, hemoptysis
Mnemonic: PE SMART
P – Pleuritic chest pain
E – Elevated HR
S – SOB
M – Mild fever
A – Anxiety
R – Respiratory alkalosis (early)
T – Tachypnea
Nursing Care:
O2 therapy
Anticoagulants (heparin/warfarin)
Thrombolytics if severe
Bed rest
Monitor ABG, ECG, vitals
CASE STUDY 1
1. Most likely asthma risk factor in Jason’s history:
Answer: Family history of asthma and allergies
His brother has asthma and both parents have pollen allergies, indicating a genetic predisposition, which is one of the strongest risk factors for pediatric asthma.
🧠 Mnemonic: "FAMILY TRAP"
Family history
Allergies
Male gender (higher risk in young children)
Infections (brother had URI)
Low birth weight (2.7kg is borderline)
Young age (under 5)
2. Main immunoglobulin in asthma pathophysiology:
Answer: IgE
IgE is involved in hypersensitivity reactions and activates mast cells, leading to inflammation, bronchospasm, and mucus production.
🧠 Mnemonic: "I Get Excited (IgE) = Allergies & Asthma"
3. Common acute asthma symptoms and mechanisms:
Symptoms Jason showed:
Non-productive cough, shortness of breath, wheezing, nasal flaring, prolonged expiration, flushed cheeks, laboured breathing
Mechanisms:
Bronchospasm → tight chest, wheeze
Mucosal edema → SOB
Mucus hypersecretion → cough
Air trapping → prolonged expiration
Hypoxia → flushed/pale skin, tachycardia
🧠 Mnemonic: "WHEEZE"
Work of breathing ↑
Hyperinflated lungs
Expiration prolonged
Edema of airway
Zip in air (air trapping)
Eosinophils ↑ in allergy/asthma (immunological cause)
4. Sign of ventilatory failure:
Answer: Increased CO₂ (hypercapnia) and signs of exhaustion
Jason’s pCO₂ = 47 mmHg, pH = 7.32 → shows respiratory acidosis → possible impending ventilatory failure
Signs: lethargy, decreasing LOC, fatigue, shallow breathing
5. Elevated white blood cell count suggests:
Answer: Infection or inflammation
WBC = 20 x 10⁹/L and neutrophils ↑ → likely viral or bacterial infection triggered the asthma attack.
6. Blood gas interpretation:
pH = 7.32 (low)
pCO₂ = 47 mmHg (high)
Respiratory acidosis due to CO₂ retention → indicates hypoventilation or worsening asthma
🧠 Mnemonic: "ROME" for ABGs
Respiratory
Opposite (pH ↓, CO₂ ↑ = respiratory acidosis)
7. How asthma can lead to pneumonia:
Answer:
Mucus stasis + air trapping → reduced clearance of microbes
Infection risk ↑ → secretions become a breeding ground → may progress to pneumonia
8. Rationale for physician’s orders:
Order | Rationale |
|---|---|
IV Hydrocortisone | Reduces inflammation of airways |
Cold air humidifier | Helps moisturize airway, prevents dryness, soothes irritated airways |
Chest physiotherapy | Aids mucus clearance and improves lung expansion |
Oxygen by nasal cannula | Maintains oxygenation during respiratory distress |
Clear, room-temp fluids | Prevents dehydration, easy to swallow without triggering bronchospasm |
Theophylline (oral) | Bronchodilator – relaxes airway smooth muscle |
Ventolin (albuterol) | Short-acting beta-agonist → immediate bronchodilation |
Alupent (metaproterenol) | Another bronchodilator for long-term control |
🧠 Mnemonic for Meds: "BROC-AID"
Bronchodilators (Ventolin, Alupent)
Respiratory support (O₂, humidifier)
Oral fluids
Corticosteroids
Avoid triggers
IV fluids/meds
Diet advancement as tolerated
CASE STUDY 2
1. What cause could have contributed to Sean’s disease? Other causes of emphysema?
Main cause (Sean’s case):
Chronic smoking for 40 years (20/day) → #1 risk factor for emphysema.
Other causes (etiologies):
Alpha-1 antitrypsin deficiency (genetic, early-onset)
Air pollution
Occupational exposure (e.g., dust, fumes)
Long-standing untreated asthma
🧠 Mnemonic: "S A M P"
Smoking (primary cause)
Alpha-1 antitrypsin deficiency
Mist (occupational exposure)
Pollution
2. Pathophysiology process leading to Emphysema:
Smoke/toxins → damage alveolar walls and activate inflammatory enzymes
These enzymes, especially elastase, break down elastin → loss of alveolar elasticity
Alveolar sacs merge (forming large air spaces) → ↓ surface area for gas exchange
Air trapping occurs → hyperinflated lungs → barrel chest
Gas exchange becomes inefficient → hypoxia & CO₂ retention
🧠 Mnemonic: "E-M-P-H-Y-S-E-M-A"
Enlarged alveoli
Merged air sacs
Protease overactivity
Hyperinflation
Yawning for air (SOB)
Surface area ↓
Elastic recoil ↓
Mucus may accumulate
Air trapping
3. Why does Sean have tachypnoea (↑ RR = 28/min)?
Reduced alveolar surface area → ineffective gas exchange
Body compensates by breathing faster to increase oxygen intake and CO₂ removal.
Also, hyperinflation reduces lung compliance, making breathing more laborious.
4. Clinical signs that indicate Sean has Emphysema:
✅ Key signs:
Barrel chest (↑ anterior-posterior diameter)
Tachypnoea (28/min)
Prolonged expiration
Reduced breath sounds (due to air trapping)
Expiratory wheeze
No cyanosis yet (early stage or “pink puffer” presentation)
🧠 Mnemonic: "PINK PUFFER"
Pink (not cyanotic)
Increased chest (barrel chest)
No cough or minimal sputum
Keeping weight low (weight loss)
Pursed lip breathing
Use of accessory muscles
Flat diaphragm (on x-ray)
Frequent SOB
Enlarged alveoli
Reduced breath sounds
5. Why is expiration prolonged in COPD (esp. emphysema & chronic bronchitis)?
Loss of elastic recoil in alveoli → air cannot be pushed out efficiently
Air trapping increases → takes longer time to fully exhale
Narrowed airways + thick mucus (in chronic bronchitis) further block airflow
Patient tries to breathe against resistance, especially during expiration.
🧠 Mnemonic: "LATE"
Lost recoil
Air trapping
Thick mucus (chronic bronchitis)
Expiration prolonged