Ethical and Legal Issues (Part 3)
Implied Consent
Implied consent differs from that of informed consent in that the client is not required to express their permission for care, an intervention, or other activities, verbally or in writing.
In other words, it is implied by the circumstances or actions surrounding a medical or nursing action, and the client isn’t required to verbally state that they give consent. A client gives implied consent by allowing themselves to be examined or treated by a health care provider, even if they do not clearly state their approval of treatment.
It should be noted that, just like cases of informed consent, the client has the right to withdraw implied consent at any time. Additionally, the client must have the mental capacity to provide such consent; the nurse must inform the client about the action or intervention planned, such as administering an injection, otherwise the nurse can be considered to have committed battery.
In some instances, health care is provided with the assumption that the client has given consent unless they express otherwise. Consider the client who extends their arm when the nurse states they need to obtain the client’s blood pressure. This is a form of implied consent as the client’s action, extending their arm, implies that there is no objection to the nurse carrying out the procedure.
In some instances, the client may not be able to provide verbal/written consent. For example, if a client who is in the hospital experiences a stroke or becomes hypoglycemic and has a diminished level of consciousness, it can be implied that the client would want aid provided if a delay in acting could potentially pose an increased risk to their life. Implied consent in these cases is supported by the client’s inpatient status in the facility.
Further, there is a duty of care that exists between the nurse and the client, meaning that the nurse should take reasonable and appropriate actions to limit the risk of negative outcomes. Failure to do so is considered professional negligence.
Advance Directives
Advance directives are legal documents in which a client’s decisions related to health care are documented. It is important for nurses to promote the development of advance directives with clients. With the aging population and growing number of clients who have dementia, health care workers are increasingly involved with concerns regarding autonomy and end-of-life care decisions.
There are two types of advance directives. The first type is a living will, which is a document where a client can clearly state which life-sustaining treatment(s) they wish to have performed if they become incapacitated and are unable to make decisions for themselves. The second type of advance directive is the durable power of attorney for health care. In this document, a client can appoint an individual to make health care decisions on their behalf if they are unable to do so. Advance directives (ADs) are written documents that allow patients to maintain their autonomy during end of life care. ADs accomplish this by clarifying patient-specific preferences for difficult medical decisions.
Nurses play a pivotal role in advance care planning by respecting people’s values, ensuring compliance with their wishes, and supporting people’s choices throughout the advance care planning process. These conversations allow the client’s provider and surrogate to know first-hand what the client’s wishes are. The client’s wishes, along with the name of their surrogate, should be documented. Determining the client’s literacy level and identifying any need for assistance in obtaining or completing the form is another important aspect of the nurse’s role. The nurse is regarded as a vital coordinating person with knowledge of patients' needs and the ability to solve any issues and and pass questions on to the physician or other professionals when more assistance is needed.
Good Samaritan Laws
A nurse does not have a legal obligation to provide care to anyone outside of their employment obligations. However, many nurses do stop and render care in emergency situations because they feel ethically responsible. When a nurse chooses to do this, states have Good Samaritan laws to protect them. These laws do vary by state, and nurses should review the laws carefully for the state in which they practice.
Good Samaritan laws protect and encourage people (including nurses) to provide aid in the event of an emergency, without fear of being held liable for their well-intentioned actions. These laws will protect a nurse if they perform reasonable behavior to protect the life of an injured person and save this person from further harm until emergency personnel arrive to assume the care.
For these laws to protect the nurse, there are requirements. First, the nurse will not be protected if care is rendered without due care or with a disregard of the safety of the individual, often referred to as “grossly negligent” care.
Secondly, the nurse cannot know of any medical or other condition of the person to whom they are providing care. Lastly, the nurse can receive no compensation for the care provided.
Whistleblowing
Whistleblowing describes a nurse formally reporting on illegal acts, wrongdoing, or unethical practice within an organization to the national and/or state agency that is responsible for regulation of the organization. Whistleblowing is a serious matter that can result in punitive actions against the organization, but can also cause stress and fear of reprisal or retaliation for the whistleblower.
Mandatory Reporting
Legislation mandates that certain officials have a legal duty to report information that can prevent maltreatment and provide safety to another individual(s). Licensed nurses are mandatory reporters. The nurse should be familiar with their state regulations and facility’s specific reporting procedures.
Reporting of Maltreatment
Reporting of suspected maltreatment is the first step to providing compassionate care for that individual. If a nurse suspects that a client or individual is experiencing maltreatment, it must be reported to the appropriate agency. Maltreatment may present itself in many forms, including but not limited to the following:
Physical maltreatment or denying food, shelter, or comfort
Neglect, denial or delaying of care
Verbal or emotional maltreatment
Sexual maltreatment
Financial exploitation
Educational maltreatment or neglect
Lack of protection from harm
Older adults, children, and those who have mental or physical impairments are at increased risk for maltreatment. The nurse has a legal duty to advocate for the welfare of clients, which includes speaking up if there is evidence of suspected maltreatment. In the event that the investigation reveals that maltreatment is not present, a nurse acting in good faith is not held liable for reporting suspicions. If maltreatment is suspected, the nurse should inform any charge nurse, unit manager, and staff nurse assigned to the client of the findings in accordance with facility policies.
Reporting of Incidence of Disease
There are several specific diseases and illnesses that also must be reported. The Centers for Disease Control and Prevention tracks certain diseases and illnesses that can pose a threat to the general public. The intent of this tracking is to monitor, control, and prevent the spread of diseases. Public health departments monitor and report occurrences of these diseases and illnesses. These include, but are not limited to:
Anthrax
Botulism
Chlamydia
Foodborne disease outbreak
Hepatitis A–C
HIV
Influenza
Measles
Rubeola
Tuberculosis
Zika virus
Reporting Incidents
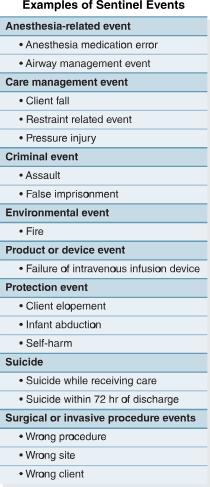
A sentinel event is an occurrence that resulted in the permanent disability, temporary severe injury, or the death of the client. Nurses at the point of care have an opportunity to identify errors and prevent them from occurring. However, when errors do occur, nurses have a responsibility to report the incident. There are several reasons to report errors. First and foremost, reporting of an error is done to protect the client from further harm.
Incident, or occurrence, reporting should occur in the following instances.
Any event that is outside the routine care of a client, such as a medication error or a missed provider prescription
Incidents involving workplace violence
Any near-miss event, such as an expired medication that is identified before it is administered to a client
Any adverse event that occurs to a client, staff member, or visitor, such as a fall
Any sentinel event
Although each facility has their own specific policies and forms for completing the documentation of an unusual occurrence, several rules apply regardless of the facility.
Include the names of the individuals involved in the event.
Use objective language that presents just the facts that were observed and the actions that were taken.
If possible, include direct quotes of the individuals involved in the event.
Report the event to supervising staff immediately.
Follow all facility policies regarding the documentation and reporting of the event.
Complete the incident report as soon as possible following the incident.
The individual who discovers the unexpected event is the one to file the incident report.
Delegation
Five Rights of Delegation
Right task: The task being delegated must be within the job description of the delegatee. Expectations and limitations of the task should also be clearly outlined in the policies and procedures of the facility.
Right circumstance: The nurse should ensure that the client’s condition is stable. The delegatee must also communicate any changes in the client’s condition.
Right person: The delegatee must have the ability and knowledge to perform the task.
Right directions and communications: The nurse must communicate specific instructions to the delegatee. The delegatee should clarify these instructions and ask questions, if needed.
Right supervision and evaluation: When delegating, the nurse is responsible for monitoring and ensuring that the task is completed appropriately. The nurse must also evaluate the client outcome and ensure that appropriate documentation is completed.
Client Abandonment
Client abandonment is an action in which the provider deserts a client for whom they have established a provider–client relationship without ensuring the continuation of care.
Examples of client abandonment include leaving the unit without arranging for another nurse to provide care for assigned clients, failure to provide report to another nurse prior to leaving the unit, and sleeping while assigned to provide care for a client. Nurses have a moral and ethical obligation to provide care to clients for whom they have accepted an assignment of care in the following circumstances.