Male Physiology
male system produces sperm and semen, then transfers them into a female body
testes produce sperm via spermatogenesis
prostate, seminal vesicles, and spermatic duct produce secretions that form semen for protecting sperm and facilitating transfer
penis is used for transporting sperm
Penis Movement
sympathetic and parasympathetic innervation
pudendal n. supplies sympathetics
branches into the dorsal n. of the penis, which recieves signals from the glans, corona, and penile skin (touch, temperature, and pain signals)
gives rise to the perineal n., which supplies the bulbospongiosus and ishiocavernosus mm.
hypogastric n. supplies sympathetics for smooth muscle contraciton of the penis
spinal cord → superior hypogastric plexus → pelvic plexus → cavernous nn.
flaccid = tonic contraction of helicine aa. and trabecular smooth muscle
Erection
parasympathetic fibers in the pelvic nn. join the fibers from the superior hypogastric plexus at the pelvic plexus and cavernous nn.
responsible for smooth muscle relaxation
mediated by acetylcholine (ACh)
ACh binds to muscarinic receptors in endothelium → increases endothelium nitric oxide synthase (eNOS) activity → cleaves to create nitric oxide (NO)
NO activates secondary messenger system (cyclic guanosine monophosphate or cGMP) for helping to relax smooth muscles
causes vasodillation and blood flows in → erection
erection = penis engorged with blood
may occur in response to sexual arousal or may occur spontaneously
occurs in 5 stages:
latent phase
impulses from the barin signal sexual arousal
penis relaxes to allow corpora caernosa to fill with blood
tumescence
penis is slightly swollen as penile arteries dilate to allow more blod flow
erection
tunica albuginea restricts venous blood flow
blood cannot exit the penis
the increased blood volume forces the penis to stand erect
rigidty
ishiocavernosus and bulbospongiosus contract
penis continues to become engorged with blood and veins become more restricted
engorgement of the corpus spongiosum (and bulbosponhiosus contraction) constricts the urethra → pressurized to facilitate ejaculation
detumescence
return to flaccidity followig climax
tunica albuginea relaxes allowing blood to drain from the penis
penile swelling goes down as blood drains out
rigidity of the penis decreases until flaccid
followed by refractory period
penis unable to become erect again even if stimulated (15 min. to days)
Scrotum
maintains cool environement (35C) for
spermatogenesis requires thermoregulation
pampiniform plexus
vein network with countercurrent heat exchange
dartos fascia
changes scrotal surface area for cooling
cremaster m.
moves testes
Testes
both endocrine and exocrine glands
exocrine products = sperm cells
nurse (sertoli) cells
activated by FSH → supports and nourish the developing sperm cell
form the blood-testis barrier and control the entry/exit of nutrients, hormones, etc.
endocrine products = gonadal hormones
testosterone, androgens, estrogens, and inhibin
stimulate development and sex drive
sustains sperm production
Spermatogenesis
production of sperm takes 70-90 days
~300,000 sperm/min (400 million/day)
occurs in seminiferous tubules
embryonic development:
primordial germ cells form yolk sac and colonize gonadal ridges
differentiate into stem cells
stem cells (a.k.a spermatogonia) remain dormant during childhood
during puberty, testosterone activates spermatogonia to undergo mitosis
spermatogenesis - process of developing spermatogonia into immature sperm cells
spermatogonia divide into 2 types:
type A spermatogonia are replacement stem cells that activaly continue dividing
type B spermatogonia develop intot primary spermatocytes
primary spermatocytes undergo meiosis I to become secondary spermatocytes
secondary spermatocytes undergo meiosis II to form spermatids
spermatids undergoes spermiogenesis to gain flagella and shed excess cytoplasm
spsermiogenesis is the maturation process
spermatids become spermatozoa
4 phases:
golgi phase
head starts to form with golgi apparatus at one end
creates enzymes that gather within the acrosomal vesicle
mitochonria move to oppposite end
distal centriole begins to form an axoneme (will support flagellum)
DNa undergoes packing
protamines replace histones making the chromatin transcriptionally inactive
cap phase - formation of the acrosomal cap
golgi surrounds anterior of the spermatids to form the acrosomal cap (acrosome)
tail phase - tail formation
centriole microtubules elongate to form axoneme
flagellum extends
mitochondria reorganize to form the midpiece
growing tail oriented towards the lumen
maturation phase (spermiation)
cytoplasm and excess organelles shed
nurse cells phagocytize and secrete testicular fluid
final product is non-motile, mature spermatozoon
spermatozoon (pl. spermatozoa) moved to the epididymis via peristalic contractions
interact with the protein-rich microenvironement
plasma membrane surface antigens get organized
Sperm Cells
head region
features a nucleus and acrosome
enzymes for ovum penetration
feature basal body
attachment of the flagellum
midpiece of tail
contains mitochondria for producing energy for movement
principal piece of tail
contains support fibers
endpiece of tail
tapers down to the tip of the flagellum
Semen
alkaline fluid expelled during orgasm (2-5mL)
60% seminal vesicle fluid
carbohydrates, vitamin C, prostaglandins (thin muscus), and prosemigelin (sticky zymogen)
clotting enzymes later converts proseminogelin to seminogelin to form a gel matrix (coagulum) that protects sperm within the vagina
30% prostatic fluid
calcium, zinc, citric acid, phosphate, and enzymes
various proteases that break down semen
prostate-specific antigen (PSA) - breaks down coagulum to activating sperm motility
10% sperm and spermatic duct secretions
sperm count 50-120 million/mL
infertility if less than 20-25 million/mL
Post-Ejaculation
degradation begins ~20-30min.post ejaculation
serine protease liquefies semen
stickiness promotes fertilization
seminogelin entangles sperm and sticks mass to the inner wall of the vagina and cervix
promotes uptake of semen clots into the uterus
prostaglandins stimulate uterine peristalsis
sperm motility
prostatic fluuid buffers vaginal acids (from 3.5-7.5)
fructose and other sugars fuel ATP production
prostagladins also thin cervical mucus to make it easier for sperm to move
Sex Hormones
gonadotropin-releasing hormone (GnRH)
stimulates pituitary to secrete LH and FSH
luteninizing hormone (LH)
stimulates interstitial endocrine cells to produce testosterone
follicle-stimulating hormone (FSH)
makes seminiferous tubules more sensitive to testosterone
stimulates nurse cells to secrete androgen-binding protein (ABP) → binds testosterone
testosterone needed for spermatogenesis
testosterone
sustains reproductive tract, sperm production, and sex drive (libido)
Puberty
puberty - period in which adolescents reach sexual maturity
typically starts between 9-14 years of age
initiated by pulsatile secretion of GnRH
regulated by LH and FSH
levels increase and stimulate development of the seminiferous tubules and spermatogenesis
testicles grow in size and cause the scrotal skin to become thinner and darker
first ejacualtion often occurs 1 year after testicles begin to grow (fertile after 2 years)
secondary sex characteristics externally
testicles grow first, then penis grows
first in lengthm then in width
glans penis and corpus cavernosum enlarge
pubic hair grows first, then other hir
2 years after onset = axillary, chest, and facial hair
sex steriods increase levels of growth hormone (GH), causing a growth spurt
increase in bone density/length and muscle mass
after growth spurt, the laryx and vocal cords enlarge, creating larger resonance space
increase laryngeal prominence and deeper voice
starts and peaks later in boys
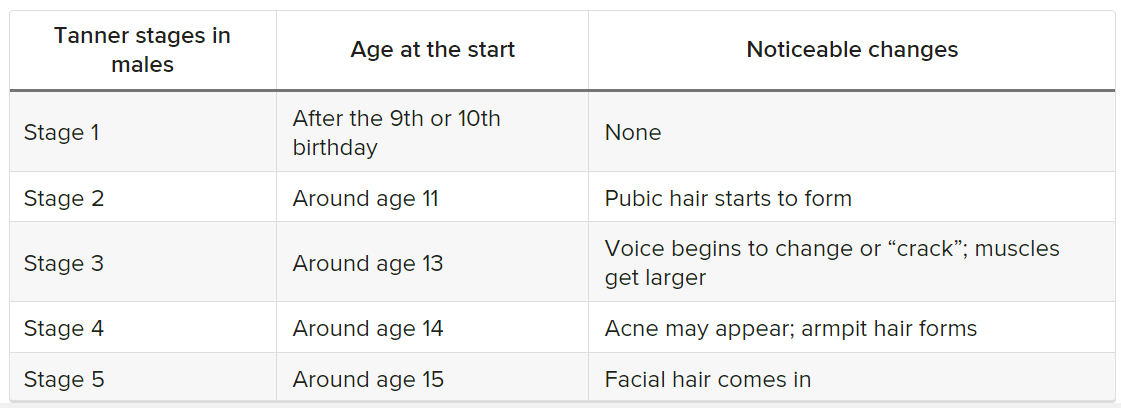
occurs in 5 stages (tannter stages) defined by James M. Tanner
a.k.a sexual maturity ratings (SMRs)
onset influenced by:
genetic factors
genes regulate GnRH release timing
variations in GnRH signaling pathways can delay or advance onset of puberty
nutrition and physical activity
less of a growth spurt of undernourished or obese
less of a growth spurt if less active
obese boys often start earlier
leptin (from adipose tissue) and ghrelin can influence GnRH signaling pathways
Andropause
andropause is the gradual decline in circulating testosterone
by age 30 testosterone levels start decreasing by about 1% each year
symptoms become more noticable around age 45
by age 50, low levels in about 50% of men
by age 60, over half of men are in andropause
aromatization - process of testosterone converting to estrogen via aromatase
increase in sex hormone binding globulin
(SHBG) produced by the liver
binds testosterone, preventing bioavailbility
high SHBG can cause brain fog, mood changes, fatigue, reduced mscule mass, low sex drive, and erectile dysfunction
low SHBG associated with metabolic issues and fluid retention
e.g type 2 diabetes and obesity
often asymptomsatic or symptoms that could be caused by age, medications, etc.
symptoms may include:
sexual symptoms: reduced libido, infertility, and/or erectile dysfunction
somatic symptoms: loss in height/bone density, reduced muscle bulk/strength, discomfort/swelling of the breasts, sweats/hot flashes, unexplained anemia, increased body fat, sleep disturbances, and/or fatigue
psychological symptoms: decreased motivation/confidence, poor concentration, and/or depression
often worse in obese/overweight patients
increased body fat accelerates aromatization
stress trigger release of cortisol
suppresses testosterone production
treatments often include testosterone therapy
doesnt work for all and could increase the risk of stroke, prostate/breast cancer, heart attack, and blood clots
may also contribute to infertility or exacerbate sleep apnea or other preexisiting conditions
limiting sugar and alcohol, lowering stress, increasing exercise, and tkaing vitamin D and zinc supplements can help increase testosterone