Notes topic 9-
9. Post-translational modifications and IC targeting of proteins with special respect to the properties and functions of the participating biomolecules as well as the related characteristics of the participating cell organelles
Basics
the product of translation: nascent poly peptide chain
often not ready to be a biologically active protein
modifications are often needed
Modifications on the N- and C-terminus
The methionine is usually cleaved off, the N-terminus
Amidation of the C-terminus
eg. vasopressin, oxytocin and cyclic peptides
Cleavage of signal sequences
the signalling sequences are usually cleaved off once it enters its compartment
one exception is nuclear proteins
Modification of individual aa?
Phosphorylation - ser, thr, tyr
methylation
carboxylation
sulfation - e.g. gastrin
hydroxylation - pro, lys in collagen and HIF-1⍺
One example of post-translational modification is hydroxylation in collagen synthesis:
in conversion of pre-pro-collagen to pro-collagen, some lysine and proline residues must be hydroxylated to create strong cross-striations in the finished product
this hydroxylation requires vtit. C
vit. C def. → scurvy ; bleeding gums due to dysfunctional collagen synthesis
Glycosylation, the attachment of carbohydrate side chains, is especially important in EC proteins, occurs in ER and golgi
Prenylation and farnesylation is typical in membrane anchoring proteins
farnesyl and prenyl actas as anchors
Acetylation/deacetylation is very important in the case of histones, but also TFs and chaperones
ADP-ribosylation, catalysed by PARP in eukaryotes
Toxins causing ADP-ribosylation:
Diphtheria toxin → ADP-ribosylation of EF-2 inhibiting it → cell death
cholera toxin →ADP-ribosylation of Gs proteins → stimulates adenylyl cyclase → increased secretions of ions to GI → diarrhea
pertussin toxin → ADP-ribosylation of Gi proteins → stimulates adenylyl cyclase → interrupts normal cell signalling pathways
Prostethic groups
some peptides needs other non-peptide units to function → these are prosethic groups
hemoglobin → heme
ferrition → iron
alcohol DH → zinc
Proteolytic prosessing
some poly-peptide chains are inactive, and must have some parts cleaved off in order to be activated
pro-enzymes or zymogens
Disulfide cross link formation
the formation of strong disulphide bonds may be necessary for proteins to protect their 3D-structure
this is especially important for EC proteins, as the EC environment is oxidizing, which would comprize the structures if not for these bonds
Protein targetting
proteins are synthesized on ribosomes in the cytosol, but other cell compartments needs proteins aswell
they are transported by the help of signal sequences, a short sequence of aa on the N-terminus (more common) or c-terminus (less common)
these sequences are recognized on the membrane of the target organelle. once inside the signal sequence is usually cleaved off
Transport to ER
a protein called SRP binds to the signal sequence on the N-terminus - SRP consumes GTP during this process
SRP then carries the ribosome-polypeptide complex, which has stopped translation, to the ER.
SRP binds to SPR-R on the ER and resumes translation, which is now feeding the polypeptide into the ER
Inside the ER, the signal is removed by signal peptidase
Inside the ER the protein can be further modified, like with disulphide bonds or glycosylation
tunicamycin is an antibiotic which inhibits glycosylation.
Following this, the protein travels from ER to golgi in transport vesicles in golgi proteins may be further modified
after this golgi sorts the proteins, and sends them to their final destination
Protein targeting to the nucleus
the signal sequence to the nucleus is not cleaved, the reason: nuclear envelope during cell division
the signal sequence for proteins targeted to the nucleus in NLS, nuclear localization sequence
it may be found anywhere on the peptide and not only on the termini
a protein called importin is involved in the import of NLS tagged proteins. GTP is hydrolysed
Protein targeting to mitochondria
protein targeted to mitochondria are fully synthesized in the cytosol, their signal sequences are recognized by proteins called TOM and TIM
TOM 20, TOM 22, TOM 40 are involved in transport across the outer mitochondrial membrane
TIM 22, TIM 23/17 and TIM 44 are involved in transport across the inner mitochondrial membrane
after entry to mitochondria, the signal seq. is cleaved
Protein targeting to peroxisomes
signal sequence PTS-1 on C-terminus or PTS-2 on N-terminus
PTS-1 is one of few C-terminal signal sequences (Ser-Lys-Leu)
So called peroxins recognize the PTS signal and transport them into the peroxisome
Protein targeting to lysosomes
the signal sequence for proteins targeted to the lysosome is mannose-6-P residue
on the membrane of lysosome there are mannose-6-P receptors, which recognizes and binds the protein, which is then transported into the lysosome
Protein targeting of transmembrane proteins
transmembrane proteins reach their target by containing special signal sequences called “internal stop-transfer anchor sequences” and “internal signal-anchor sequences”
they are transported through the membrane, but at the STA and SA sequences it is embedded into the membrane
Receptor-mediated endocytosis
receptor-mediated endocytosis is a process by which cells can take in EC proteins
cells depend on external proteins to a large degree
for cells to take up for example LDL, transferrin, peptide hormones or circulatory proteins from the outside, receptor-mediated endocytosis is needed
there are 3 main pathways of receptor-mediated endocytosis
clathrin-dependent endocytosis (most common)
caveolin-dependent endocytosis
clathrin- and caveolin- independen endocytosis
in clathrin-dependent endocytosis the EC protein in questions binds to receptors on the cell surface, the IC protein clathrin then binds to the inside of the cell membrane at the area where the EC protein is bound to its receptor
clathrin then forms an invagination in the cell membrane, first forming a pit and later a vesicle, containing the receptor and EC protein and internalises it
a protein called dynamin holds the clathrin-coated vesicle together
the EC protein dissociates form the receptor inside the vesicle, and the vesicle is split to two, one contains the receptor, which is moved back to the membrane, and the other w. the EC protein.
The protein can then be transported to where it is needed
12. Plasma proteins: classification, properties, biochemical-physiological role
Basics
blood has several functions in the body → it transports O2 and nutrients, metabolic waste, hormones.
it also has regulatory functions: thermoregulation, pH reg. (buffer)
protective functions: hemostasis by activating platelets and initiating blood clots, prevents infection by antibodies and WBC
blood has two major components:
liquid: plasma (55%)
formed elements (45%): RBC, WBC, platelets
blood plasma
water (90-92%)
proteins (6-8%): albumin, globulins, fibrinogen
organic nutrients: Glc, carbs, aa’s
electrolytes: Na+, K+, Ca++, Cl-, HCO3-
non-protein nitrogenous substances: urea, creatine
respiratory gases
Families of blood proteins
Blood proteins | Normal levels | % | Functions |
|---|---|---|---|
Albumins | 3,5-5 g/dl | 55 | Create oncotic pressure and transport insoluble molecules |
Globulins | 1-1,5 g/dl | 38 | Participate in immune system (𝛾), transport (⍺/β) |
Fibrinogen | 0,2-0,45 g/dl | 7 | Blood coagulation |
Regulatory proteins | <1 | Reg. of gene expression | |
Clotting factors | <1 | Conversion of fibrinogen into thrombi |
Protein electrophoresis
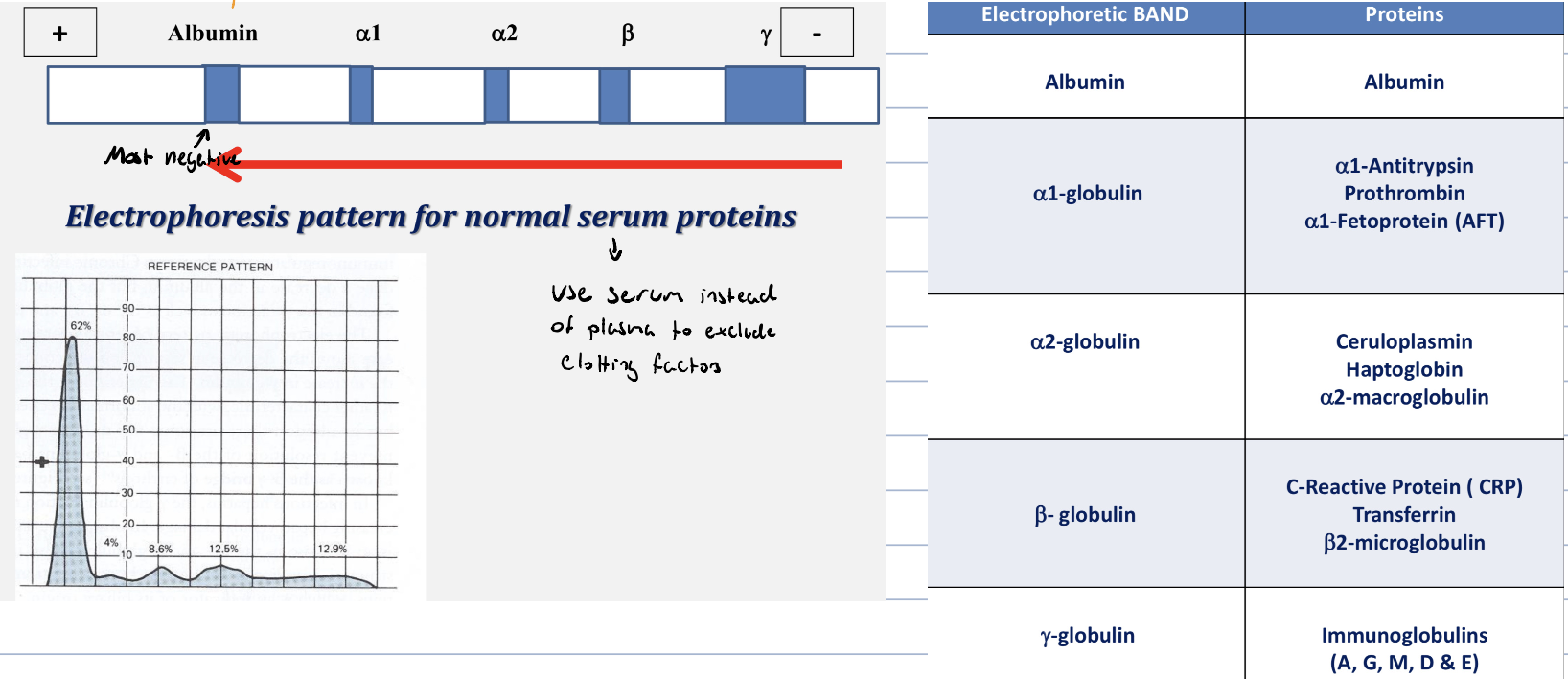
Prealbumin
named as prealbumin, as it migrates faster than albumin in classic electrophoresis
aka. transthyretin
it is the transport protein for thyroid hormones and Vit. A (retinol)
prealbumin is decreased in:
liver disease
nephrotic syndrome
acute inflammatory response
malnutrition
Albumin
family of water soluble proteins which are able to transport other molecules non-specifically
it is the most abundant protein in the blood
albumin is synthetized in the liver and has a half-life of ∽20 days, making it a good indicator for liver funtion
it is the main constituent for oncotic pressure
albumin should not be present in urine
this condition is called albuminuria and is mostly pathological, traces can be seem in pregnancy or after running marathons, but normally it should not be present in urine
functions
oncotic pressure
albumin is responsible for ∽80% of the plasma oncotic pressure
hypoalbunemia leads to edema
buffering
transports
hormones, calcium, drugs (salicylates), FFA, bilirubin
causes of hypoalbunemia
arteficial: diluted sample
physiological: pregnancy
decreased aa: reduced synthesis of non-essential or low dietary essential aa’s
increased catabolsim: surgery, trauma and infections
liver disease
inc. loss from kidney
Prothrombin
a glycoprotein occuring in blood plasma and is an essential component of the blood-clotting mechanism
prothrombin is converted into thrombin by clotting factor X or prothrombinase
thrombin then acts to transform fibrinogen to fibrin
under normal conditions, prothrombin is changed into thrombin only when injury occurs to the tissue or circulatory system
synthesis of thrombinogen requires vit. K, and hypothrombinemia causes prolonged bleeding
⍺1-antitrypsin
a protein synthetized by liver and macrophages
it is an acute-phase protein, meaning that it is produced upon a stress
causing secretion of cytokines (IL-1, IL-6, TNF-⍺)
it’s function is to inhibit proteases, this is due to bacterias and leukocytes can release proteases, especially elastase, which is breaking down elastin in the lungs
in antitrypsin deficiency, 1aa can be wrong
liver produce antitrypsin, but can’t release it, this causes liver cirrhosis, neonatal jaundice and pulmonary emphysema in adults
Alpha-fetoprotein
a glycoprotein which is the major plasma protein produced by the yolk sac and the liver during fetal development
it is thought to be the fetal form of serum albumin
AFP can bind copper, nickel, FA, bilirubin and is found in mono-, di- and trimeric form
levels of AFP above 500ng/ml can be indications of hepatocellular carcinoma, germ cell tumors and metastatic cancers of liver
Positive acute phase protein
inc. during stress/inflammation due to production of cytokines (IL-1, IL-6, TNF-⍺)
these are:
⍺1-antitrypsin
heptaglobulins
ceruloplasmin
fibrinogen
C-reactive protein (CRP)
C-reactive peptide
is an acute phase protein synthetized by liver
it precipitates the polysaccharide (fraction C) of pneumococcal cell walls
it’s important for phagocytosis
in inflammation CRP plasma levels increase
in physiological cells it binds to phosphatidylcholine on apoptotic cells and activates the complements system
Ceruloplasmin
synthetized by liver
binds and transport serum copper
it is important in acute phase response, as it can inactivate ROS and prevent tissue damage
plasma levels is lower in Wilson’s disease in which copper is accumulating in liver leading to cirrhosis
Haptoglobin
synthesized by liver
it binds free hemoglobin to form complexes which are metabolized in the RES
it limits iron loss, as Hgb is small enough to be filtered by glomeruli
decrease: hemolysis
increase: acute phase response
Finbrinogen
synthetized in liver, is an acute phase protein
its function is to form a fibrin clot, when activated by thrombin
removed in the clotting process, not seen in serum
its level increases during pregnancy and by using oral contraceptives
Alpha-2-macroglobulin
synthetized by liver, macrophages, fibroblasts and adrenocortical cells
is the largest major non-immunoglobulin protein in plasma
acts as an antiprotease, supressing many proteases
acts as a carrier protein, binds cytokines, GFs, insulin, TGF-β
Hypergammaglobulinemia
increased immunoglobulin levels may be result of stimulation of many clones of β-cells (polyclonal hypergammaglobulinemia) or monoclonal differentiation (paraproteinemia)
Polyclonal hypergammaglobulinemia
stimulation of many clones of β-cells produce a variety of antibodies that appear as diffuse increase of 𝛾-globulins on electrophoresis
e.g. acute and chronic infections, auto-immunity
Monoclonal hyperproteinemia
proliferation of a single B-cell clone
produces a single antibody, which appears as a distinct densely stained line on electrophoresis (paraproteins or M band)
paraproteins are characteristic of malignant B-cell proliferation
multiple myeloma
14. Alterations of protein metabolism in various physiological and pathological conditions
Basic
proteins are essential molecules for normal cellular functions while at the same time containing lots of amino acids, which can in low energy state be broken down to produce energy
Well-fed stage
in the well fed state, there are surplus of energy in the body, meaning that we have sufficient amounts of ATP
as we know, protein is heavily dependent on ATP/GTP to proceed
the availability of AA’s, which are substrates of protein synthesis also increases the protein synthesis
lastly, we know that insulin is a so-called anabolic hormone, this means that it promotes the synthesis of protein
insulin also suppress the activity of gluconeogenesis by activating PFK-2
this reduces the need for gluconeogenetic substrates, which is exactly what the carbon skeleton of glucogenic amino acids yield
Fasting stage
when it is long since the last meal, the glycogen storage has been depleted, and the body starts to search for alternate methods to produce glucose to feed the important organs, like the brain
the AAs are good substrates for producing both glucogenic and ketogenic substrates, both which can fuel the brain
proteins should be broken down in order to produce free AAs to fuel gluco- and ketogeesis
it is important to notice than even though protein gets broken down, there is still production of proteins, but the type of proteins differ
in pathological condition the acute phase proteins are typically increased in synthesis
Cortisol
during stress response, cortisol is secreted from the adrenal gland
cortisol has an catabolic effect on muscle tissue and cause breakdown of proteins into AA’s, so that they can be used as substrates for gluconeogenesis
Diabetes mellitus
in DM our body enters a “pretend” starvation
our body does not send (type 1) or receive (type 2) the insulin signal which is the body’s way to signal when we have a enough glc
so processes in the body, starts to break down proteins in order to produce glc
remember that insulin signalled to not break down proteins, so in this case the preventative signal is not sent, so proteins are broken down
Different alterations that shift protein metabolism
in different pathological (and physiological) conditions some proteins will be more or less synthetized
Hsp
heat shock protein are produced when the temp incr. or other environmental stress occur
hypoxia can promote it
HIF-1⍺
protein which in normal conditions are constantly hydroxylated and degraded, however in hypoxia, it will not be degraded
it will then promote Cox 4-2, promote angiogenesis, and other hypoxic stress factors
15. Antibiotics
Basics
antibiotics are molecules or substances produced to kill microorganisms
more than half of them act agains protein synthesis, most of them act on the ribosomes
the fact that it acts on the ribosomes makes it problematic, as the ribosomes are highly conserved, this it is hard to find a specific inhibitor which is not toxic to the host
Aminoglycosides (streptomycin)
inhibit initiation and causes misreading of mRNA in bacteria (prokaryotes)
Tetracycline
binds to the 30s subunit and inhibits the binding of aminoacyl-tRNA
prokaryotes
Chloarmphenicol
Inhibits the peptidyl transferase activity of 5os ribosomal subunit in prokaryotes
Cycloheximide
inhibits translocation in eukaryotes
Erythromycin
binds to 5os and inhibits translocation in prokaryotes
Puromycin
causes premature chain termination by acting as an analogue of aminoacyl-tRNA in both eukaryotes and prokaryotes
Neomycin
Inhibits binding of AA-tRNA to bacterial ribosome
Antibiotics that do not inhibit protein translation
Penicilin
block formation of peptide cross links in peptidoglycans, weakening the bacterial cell wall
Antimycin
inhibits complex III in the rep. chain
inhibits oxidation of ubiquinol
Oligomycin
Inhibits proton flow through F0 of F1/F0 complex
ABC-transporters importance in antibiotics resistance
ABC-transporters are multidrug transporters that are able to export antibiotics out of the cell
β-lactamase in penicillin resistance
penicillin and related antibiotics contain β-lactam rings, these can be destroyed by β-lactamase, thus making penicillin ineffective
an idea could be to administer β-lactamase inhibitor with the antibiotics
17. Biochemical background of dysfunction associated with hemoglobin variants
Hemoglobin
Hgb is a heterotetromer consisting of 2⍺ and 2β subunits in adult hgb
heme is a porphyrin ring with central iron (Fe⁺⁺), iron is the site of O2 binding
Genes
the chromosome 16 codes the ⍺-chains + ɸ chain
the chromosome 11 codes the β, δ, 𝛾, 𝛆
Fetal development of Hgb
in the first weeks the phi and 𝛆 are the dominant subunit
after approx 3 week the ⍺ subunit is synthetised as well as the 𝛾
after birth more and more β-subunits are produced
why is this important → ⍺𝛾 Hgb has higher affinity towards O2 so the fetus can “steal” O2 from the maternal ⍺β Hgb
Hemoglobinopathies
structurally abnormal Hgb is synthetised
more than 1.000 exists, but ∼100 are associated with disease
sickle cell disease (Hb S) and hemoglobin C have a similar structurally deficiency, where the 6th AA from the N-terminus is changed from glutamate to valine-Hb S or lysine-Hb C (negative AA → neutral or positive AA)
Sickle cell disease (Hb S)
in sickle cell disease there is a point mutation in the gene coding for hemoglobin
the point mutation leads to substitution of glutamate to valine in the 6th AA from the N-terminus
Hb S polymerizes when deoxygenated and cause the sickle shape of the blood cells
the deformation reduces its ability to circulate and will be able to cause infarction and hypoxia
Hbs is usually diagnosed early in life, when Hb F levels decrease, patients have severe chronic anemia with several complications
clincial features incl.:
abnormal growth of bone and joints (hand-foot syndrome)
renal complications
spleen and liver (autosplenectomy, hepatomegaly and jaundice)
enlarged heart, pulmonary infarction
leg ulcers
infections - main cause of mortality
Hemoglobin C
in the case of Hb C it is the same 6th N-terminal AA, glutamate, which is switched to lysine
it is associated with splenomegaly, abdominal discomfort and hemolytic anemia
diagnosed by Glod-ber formations in a blood smear
most common in West-Africa
⍺-Thalassemia
this is a quantitative Hb disorder
absence of ⍺-chains will result in increase of 𝛾-chains in fetal life and β-chains in adults
the severity will depends on how many of the 4 genes (2 per chromosome 16) are affected
silent carrier: aa/a-
minor: —/aa or a-/a-
Hg H: a-/—
Barts hydrops fetalis — / — (non compatible with life)
⍺-thalassemia trait (minor)
aa/a- or —/aa
exhibits mild microcytic /hypochromic anemia
normal Hb electrophoresis, may be mistaken for iron def. anemia
Hemoglobin H disease
second most severe form
only one functioning gene for ⍺-chain
excessed unpaired 𝛾 or β chain can form stable complexes which bind O2 with high affinity
RBCs are microcytic, hypochronic
lower Hb and Hb H can be oxidized and be percipitated for form heinz bodies
GOLF apperance can be seen in blood smear with cresyl-blue stain
Bart hydrops fetalis syndrome
most severe form, incompatible with life
there are no functioning genes for ⍺-chain (—/—)
babies born with hydropsis fetalis has acites and edema, hepato- and splenomegaly
severe anemia and no normal RBC
β-Thalassemia
usually caused by mutations on the 11th chromosome
unlike in ⍺-thalassemia, the excess ⍺-globin will not form complexes with high O2 affinity
β-thalassemia trait (minor)
caused by heterozygous mutation
usually presented with mild hemolytic anemia, although during stress it can increase
Hgb levels are normal
they have high HbA2 and normal/slightly elevated HbF levels
β-thalassemia intermedia
there is an increase in HbA2 production and HbF
anemia, jaundice, spleno- and hepatomegaly may occur
significant increase in bilirubin levels
β-thalassemia major
characterized by very severe microcytic, hypochromic anemia
low levels of Hb (2-8 g/dl) - normal 14-18 g/dl
bone changes due to expansion of bone marrow for erythropoesis
no normal RBCs on blood smear
have skull deformation, hepato- and splenomegaly + growth retardation
requires transfusion
risk for AIDS
iron overload → chelation required to prevent cardiac problems
alloimmunization
18. Molecular processes affected and biomolecules participating in certain acquired disorders of protein metabolism with special respect to ER stress and neurodegenerative diseases
ER stress
the ER is under constant stress but the degree of which can be influenced by external factors
ER stress can be induced by inhibitors of protein glycosylation (physiologically by starvation, by tunicamycin)
decrease of intraluminar Ca⁺⁺ conc. by inhibition of SERCA (sacroendoplasmatic reticulum calcium ATPase) or ionsphoresis
intraluminar reducing agents and protein overproduction (e.g. viral infection)
Response
the ER will respond by increasing the ER volume and functional capacity
also it will decrease the protein overload but inhibiting protein synthesis and protein degradation
worst case: apoptosis
Role of ER stress
sensing of fuel molecule levels, conversions of β-cells to plasma cells and in biotransformation of exogenous enzyme in liver
Unfolded protein response (UPR)
the ER stress is sensed by molecules that are embedded into the ER membrane (IRE1, PERK, AFT6)
the IRE1 (serine/threonine - protein kinase /endoribonuclease ) forms homodimers
form complexes with BiP (Hsp) when there is excess of unfolded protein in the lumen
IRE is released from ER membrane and splices XDP-1 mRNA, allowing expression of XRP-1
XRP-1 is a transcription factor for chaperones and proteins for upr, this leads to the early response of UPR
the early response increase volume of ER and expression of folding machinery. also ERAD (ER associated degradation of protein)
in case of continued signalling after early response, the late response will be activated (via ATF-4 and chop) → apoptosis
PERK (PKR (RNA-activated kinase) - like ER-kinase) is activated by BiP and phosphorylates eIF2⍺
this stops all protein synthesis except for ATF-4
ATF-4 is a TF for AA-import, GSH synthesis and CHOP
CHOP induced apoptosis
PERK also also phosphorylates Nrf 2 which is an TF for oxidative defense, expressing anti-oxidants
ER overload response
If there is an overload of proteins (viral inf.) the ER overload response starts. This response increases inflammation
the 3 steps of this response is:
Ca⁺⁺ outflow from ER
ROS formation
Activation of NF-kβ → cytokine production
this response is associated with many diseases like: Alzheimers, CF and marfan syndrome
Cystic fibrosis
disease of the lungs associated with misfolded CTRF (ABC-transporter), causing water retention and more viscous mucus
Neuodegenerative diseases
Demenita - revesible
some forms of dementia can be reversed
that can be in case of vitamin B12 and folate def,, hematomas etc
dementia is not a disease, but rather a symptom that may be caused by several diseases and underlying factors
Irreversible dementia
many dementias are not-reversible, such as: Alzheimer, Parkinsons, Huntingtons, Pich’s and Balo’s
a common feature of dementias are atrophy of the brain → narrower gyri and wider sulci, due to death of neurons
Amyloids
amyloids are aggregates of proteins that has been folded into a special shape that allows them to stick together and form fibrills
These amyloids are usually comprised of β-sheets, and are sometimes called β-amyloids
when proteins are clumped together like this, cells are damaged
a disease where amyloid formation occur is a type of amyloidosis
the specific protein that form amyloids vary from disease to disease
in alzheimers amyloids are formed from fragments of APP(amyloid precursor protein)
in parkinson, ⍺-synuclein form amyloids
Alzheimers disease
alzheimers disease in an amyloidosis
the fibrils formed are called Aβ-plaques and are caused by specific cleaving of APP by ⍺ or β-secretase
in addition to being amyloidosis, alzheimer’s is also associated with formation of “neurofibrillary tangles”
to musch phosphorylation of a microtubule stabilizing protein called TAU, is associated with many diseases, they are called taupathies
the hyperphosphorylated TAU causes disintegration of the microtubules and TAU aggregates as neurofibrilar tangles
Parkinson’s disease
parkinson’s is caused by loss of dopaminergic neurons in the substantia nigra → this leads to the loss of inhibition of striatum, through the nigrostriatal tract
as there is no inhibition, cells of the striatum dies from excitocytotoxicity
many proteins and genes are associated with parkinson’s
under pathological conditions, a protein called ⍺-synuclein aggregates and forms amyloids, which eventually form lewy bodies, a classical histological marker for parkinson
dopamine stabilizes the oligomers of the lewy body formation
PlNK-1 and LRRK2 mutation can inappropriatly phosphorylate proteins, which disturbs signalling and eventually leads to cell death
DJ-1 mutation leads to proteasome inhibition, abnormal phosphorylation and oxidative stress → neuronal cell death
Parkin, a ubiquitin ligase, mutation leads to less proteosomal degradation of misfolded proteins → accumulation of misfolded proteins → neuronal cell death
Parkin/PlNK-1 mediated mitophagy
in normal conditions, mitochondria goes through fusion and fission
it is essential for biogenesis and quality control of mitochondria
the mitochondria which are unable to fuse are degraded by mitophagy
for fusion, adequate membrane pot. is needed and leads to accumulation of mitofusion, a prot. which initiates fusion
mitofusion can be excessively phosphorylated by parkinin and PlNK
Huntington’s disease
huntington is raised by a loss of neurons in the caudate nucleus
when the gene that codes for a protein called huntingtin, has too many CAG sequences in the gene
this occurs due to a special type of mutation called trinucleotide repeat expansion, which causes the trinucleotide CAG to repeat many times in a gene
healthy people has less than 26 repeats, as the number of CAG repeats increase, the risk for disease increases
CAG codes for glutamine
the result is a huntingtin with too many glutamine residues, having a polyglutamine tract
huntingtin normally increase SRE-regulated proteins
they are proteins important for cholesterol synthesis in the CNS
Friedrich’s Ataxia
chromosome 9
is also a trinucleotide expansion disorder, where the GAA is repeated to many times in the Frataxin gene
this reduces expression of frataxin
Frataxin is a protein involved in formation of iron-sulphur clusters and several proteins will lose function due to the frataxin mutation (succinate DH, ferrochetalase, aconitase..)
Prion related diseases
prions are misfolded proteins which acts as chaperons, but they will cause misfolding of proteins, forming β-plated sheet which are depositing
in humans, the most important protein is PrP which usually is in the c-conformation PrPc, however sometimes this folds into PrPsc form which is resistant to proteolysis and cannot be broken down
when the PrPsc comes in contact with another PrPc it changes conformation to PrPsc
many proteins in PrPsc form clump together and forms amyloids which causes neurodegradation
19. The composition and physicochemical characters of biofluids
Biofluids
in the body there are several types of biofluids, one group can be considered as filtrate of blood
they are in constant exchange of substances with blood, so the number of various solutes in them are in dynamic equilibrium with their conc. in blood
the filtrates are: urine, saliva, CSF and synovial fluid
Gastric juice, duodenal fluid, semen and amniotic fluid, as well as exudates and transudates (which are found in pathological conditions)
Lymph is also an important biofluid
Blood plasma
blood plasma contributes to ∽55% of total blood volume, and is a protein-salt solution which acts as a suspension for RBCs and WBCs
Composition
90% water
8% protein
albumin, globulins
0.9% Inorganic salts
Na⁺, K⁺, Ca⁺⁺, HCO3⁻ and PO43⁻
1.1% Organic substances
Glc, urea, uric acid
Urine
the average amount of urine is 800-1500ml, it depends on liquid intake and other ways of liquid (sweat, stool, respiration)
the color of urine normally falls between pale straw yellow to amber depending on its concentration
color can be influenced by solute conc., pathological molecules, drugs and diet
red color suggests blood or free Hgb is in urine (hemogloburia)
brown color - bilirubin
composition
the chemical composition of urine is constantly changing and depending on diet
conc. of solutes keep changing throughout the day
dry weight of excreted materials = 60 g/day
hormones can be found
hCG: pregnancy test
LH: ovulation test
Stuff that should not be in urine
proteins → proteinuria
glucose → DM / glucosuria
RBCs → hematuria
Hemoglobin → hemoglobinuria
Lymph
a clear to white fluid made of WBCs and chyle (a fluid form the intestine)
lymph is involved in many processes in the body
chylomicrons will be transported from the intestines to the liver in lymphatics
it is also involved in the immune system
Composition
composition of lymph is roughly equal to that of blood plasma
Synovial fluid
found within the synovial/joint capsule and is produced by the synovium
it is a slippery fluid which lubricates the joint surfaces in order to reduce friction and pain
Composition
proteoglycan - Lubricin
GAGs - Hyaluronan
proteins below 12kD due to non-selective plasma filtration → plasma content is roughly equal to plasma
Functions
reduce friction
shock absorption - non-newtonian character
nutrient and waste transport from chondrocytes
20. Osmosis, osmolarity with contribution of different solutes
Osmosis
in general, osmosis is the movement of the solvent from the higher place of solvent concentration, to a place of lower solvent concentration, through a semipermanent membrane
Osmotic pressure
the pressure that is needed to counteract the flux of solvent, given by the formula: ∏ = icRT
∏: osmotic pressure
i: van’t hoff factor
c: molarity of all dissolved substances
R: universal gas constant
T: temp in Kelvin
the osmotic pressure is a colligative property of a solution, colligative means that the property depends only on the number of the dissolved particles but not on their type or chemical composition
in living organism, osmosis is related to the movement of water across the cell membrane, it will flow from the place of higher water concentration to the place of lower water concentration
Osmolarity
total number of all osmolytes (in moles) in 1L solution
Osmolality
total number off all osmolytes (in moles) in 1kg solution
Osmolytes
osmotically active dissolved particles (AAs, sugars, polyols, urea)
Blood plasma
the osmolarity of blood plasma is 290 < Cbp < 310 milliosmoles
this equals a NaCl solution of ∽150 mM NaCl (0.9% NaCl) → physiological saline solution, this is isotonic
if we were to place a blood cell in sterile water, which is hypotonic water will flow into the cell to counteract the osmotic difference → burst of RBC
if we place and RBC in hypertonic solution, e.g 20% NaCl, the water will flow out of the cell and the RBC shrints
Importance of osmosis in humans
Blood plasma
there is a regulation of BP in the kidneys, by water flow into urine
ANP will decrease BP by increasing water in the urine, this is accomplished by increasing excretion of Na⁺ into the urine
Na⁺ is an osmolyte which “drags” water with it into the urine
Diarrhea
in the case of osmolytes in high conc. in the intestinal lumen, like lactose due to lactase def.
these is an increase of lactose, an osmolytic in the lumen, water is dragged into the intestine and watery stool is the result
Sense of thirst
intiated by osmoreceptors cells outside the BBB
Edema
albumin is an important osmolyte in blood plasma in order to keep plasma oncotic pressure
in case of liver failure the oncotic pressure of plasma falls, filtration occur and water sieves out of the blood
accumulation usually occur in legs due to gravity