Module 1: Healing After Debridement, Periodontal Re-Evaluation, Risk and Maintenance
Topic 1: Healing After Debridement
“Effects of Nonsurgical Periodontal Therapy” by Anita Badersten
reduction of probing depth increase in gingival recssion over 9 months
smaller probing depth bc of recession
loss of attachment occurs in shallow sites after thorough debridement
deeper the probing depth = likely to have less attachment
Gives concrete evidence that non-surgical root debridement reduces bleeding + reduce inflammation + gain attachment
Intro:
Ideal form of healing is regeneration however repair via long junctional epithelium is more predictable
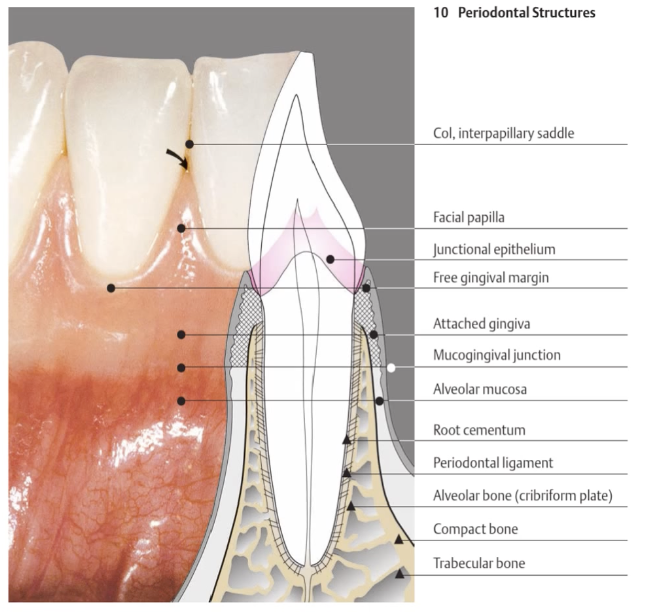
Periodontal Structures:
Healing:
Repair of periodontal structures comes from the blood vessels in periodontium
Junctional Epithelium
non-keratinized
fast tissue turnover
wide intercellular spaces
pathway for transudate + inflammatory exudate
anchors via hemidesmosomes
Reattachment + Restoration of JE occurs after:
periodontal probing
scaling + root debridement
curettage
flap surgery
gingivectomy
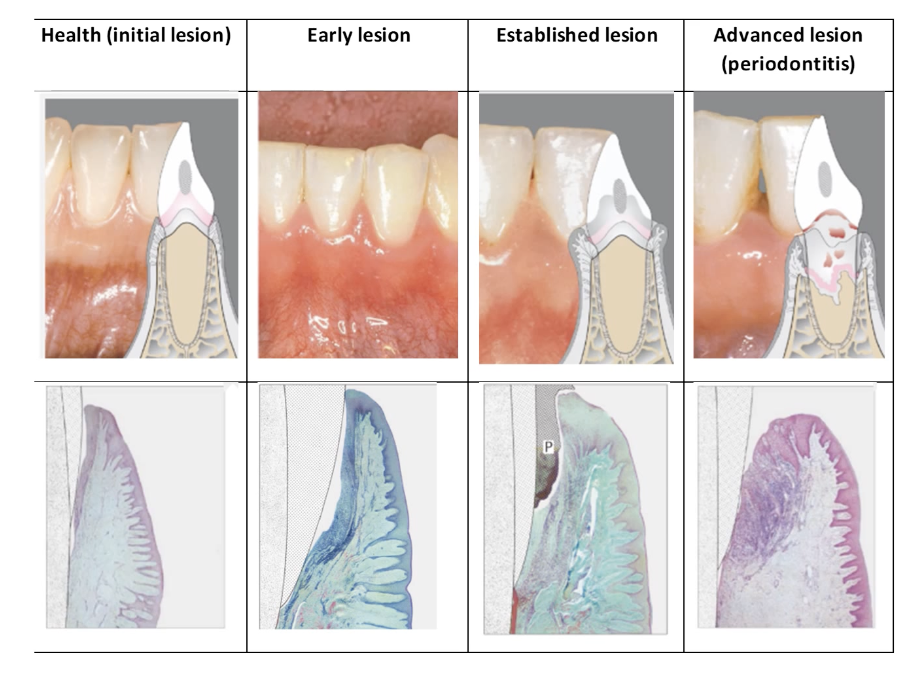
Healing Events:
Repair (scar)
after injury to re-establish functional tissue
principal tissue: long junctional epithelium

Regeneration
slower
replacement of lost damaged tissue w/ the same tissue prior to disease
restoration of PDL, alveolar bone, root cementum
Healing Events:
immediately after debridement: RBC adhere to root surface
60 mins: RBC form fibrin clot (inflammaroty cytokines are released, making capillaries bigger)
6 hours: early inflammation
3 days: late inflammation + granulation tissue formation
7 days: highly cellular connective tissue attachment to dentin
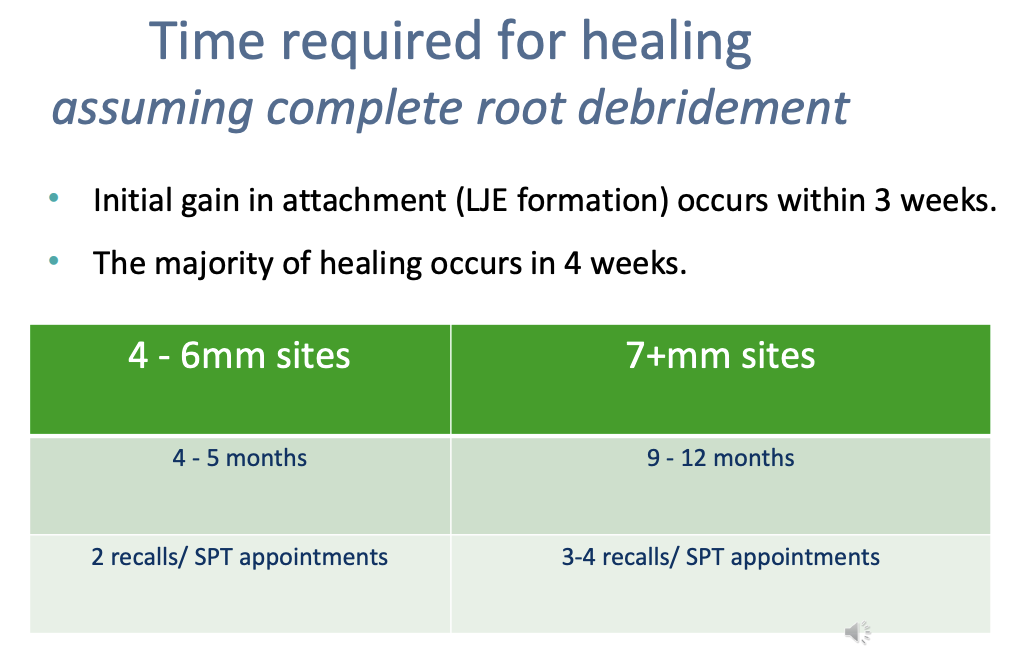
21 days: immature collagen present, junctional epithelium reattaches
Microbial Events of Debridement
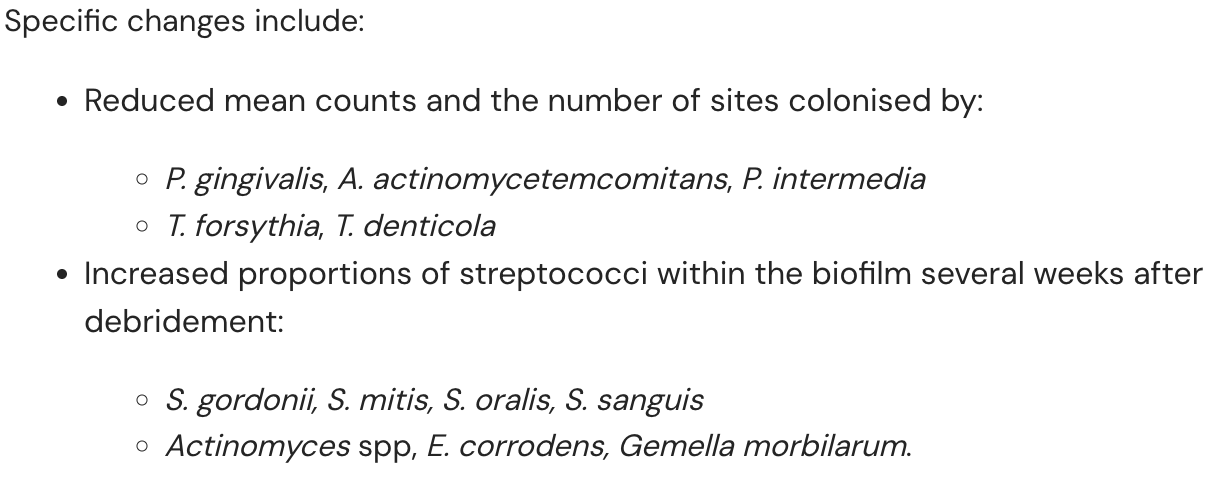
Effects of Poor Oral Hygiene after SRD
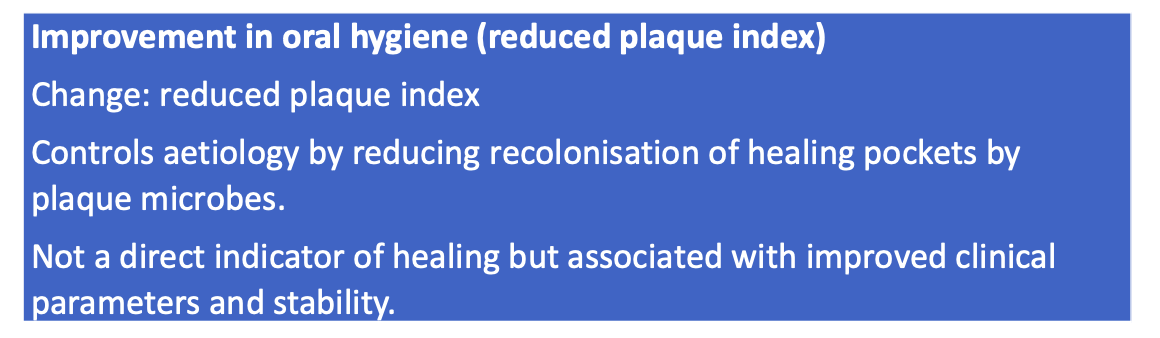
original microflora re-establishes itself within weeks of SRD
if patient doesn’t remove plaque, periodontal pockets won't heal
residual calculus + plaque disrupts healing
rough root surfaces result in plaque retention + inflammation
Factors that Affect Complete Debridement
access (probing depth)
access (tooth type)
presence of root irregularities + furcation
instrument
Topic 2: Periodontal Re-Evaluation
We know that SRD and oral hygiene works in the long-term from:
Randomised clinical trials demonstrate measurable clinical improvements were achieved through periodontal therapy in comparison to untreated controls. (Axelsson and Lindhe (1981) series)
Observable results from long-term, retrospective trials of patients treated for periodontal disease (maintenance populations). Long-term maintenance studies include Hirschfeld and Wasserman (1978), and McFall (1982).
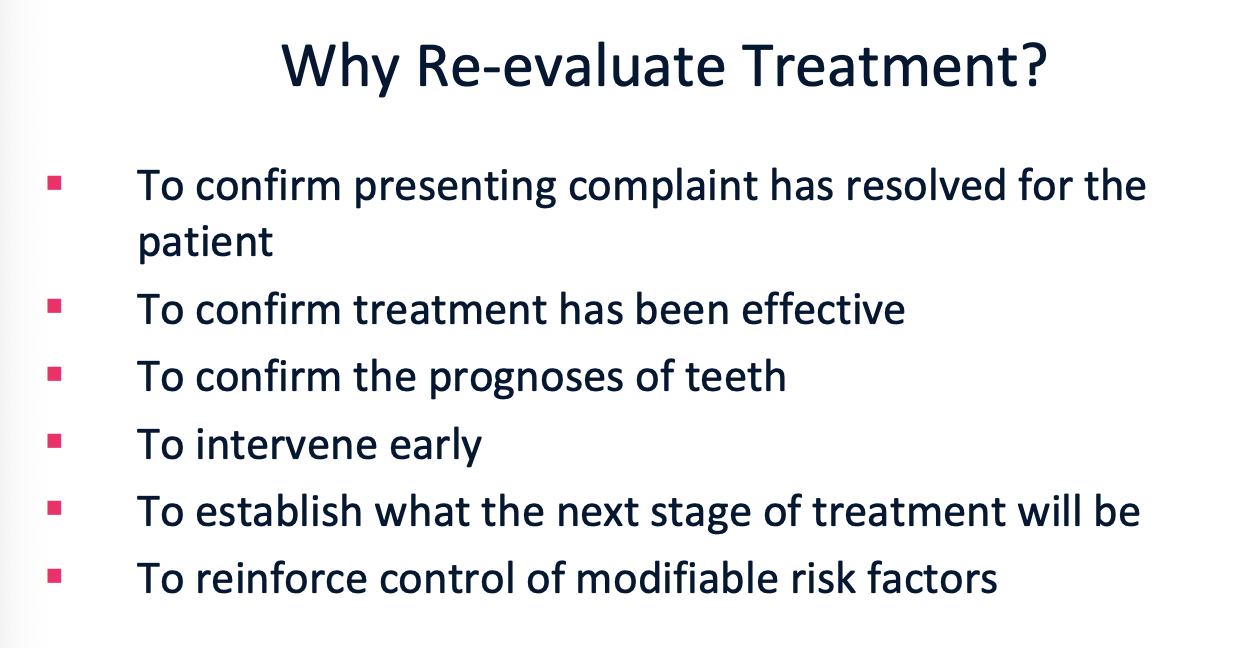
When Should We Re-Evaluate Patients? Why?
Gingivitis = 6 months
Moderate Periodontitis w/out systemic risk factors = 8-12 weeks
Severe Periodontitis w/ systemic risk factors = 6-8 weeks

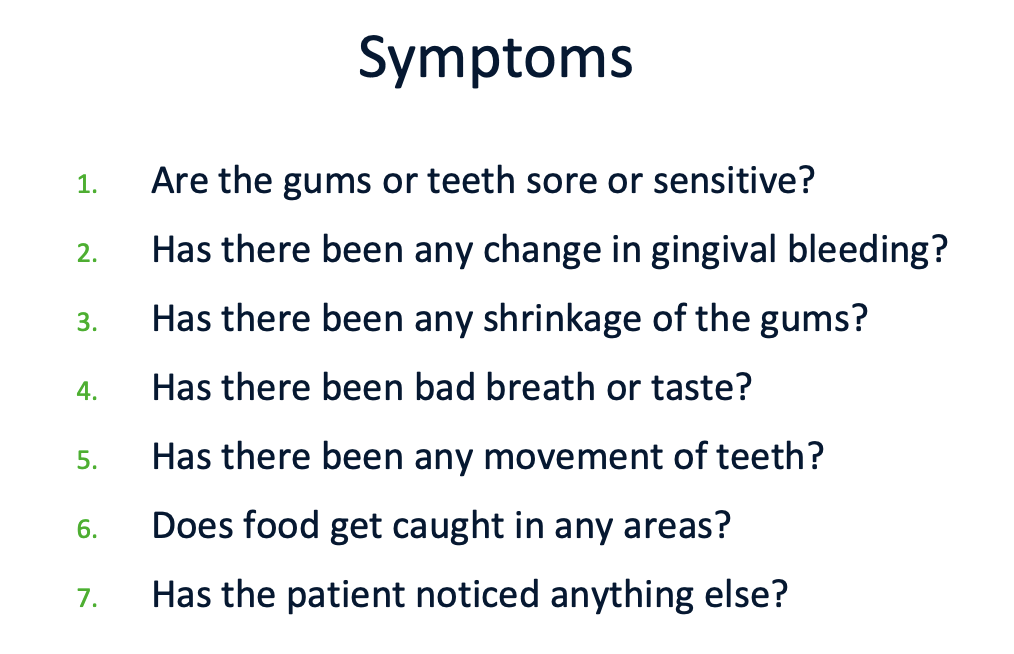
Questions for Patients:
has presenting complaint resolved?
any changes in medical history/smoking habits/stress?
oral hygiene
any dental treatment since debridement appointments
Baseline Exam Process
Review teeth
new carious lesions
review restorations + appliances
Visual Evaluation of Gingival Tissues
colour/contour/attachment
Review Oral Hygiene Routine
Repeat Diagnostic Tests
visual exam
perio chart
review radiographs
supplementary tests
COMPARE THESE RESULTS W BASELINE

What are some reasonable changes in probing depth + CAL after debridement?
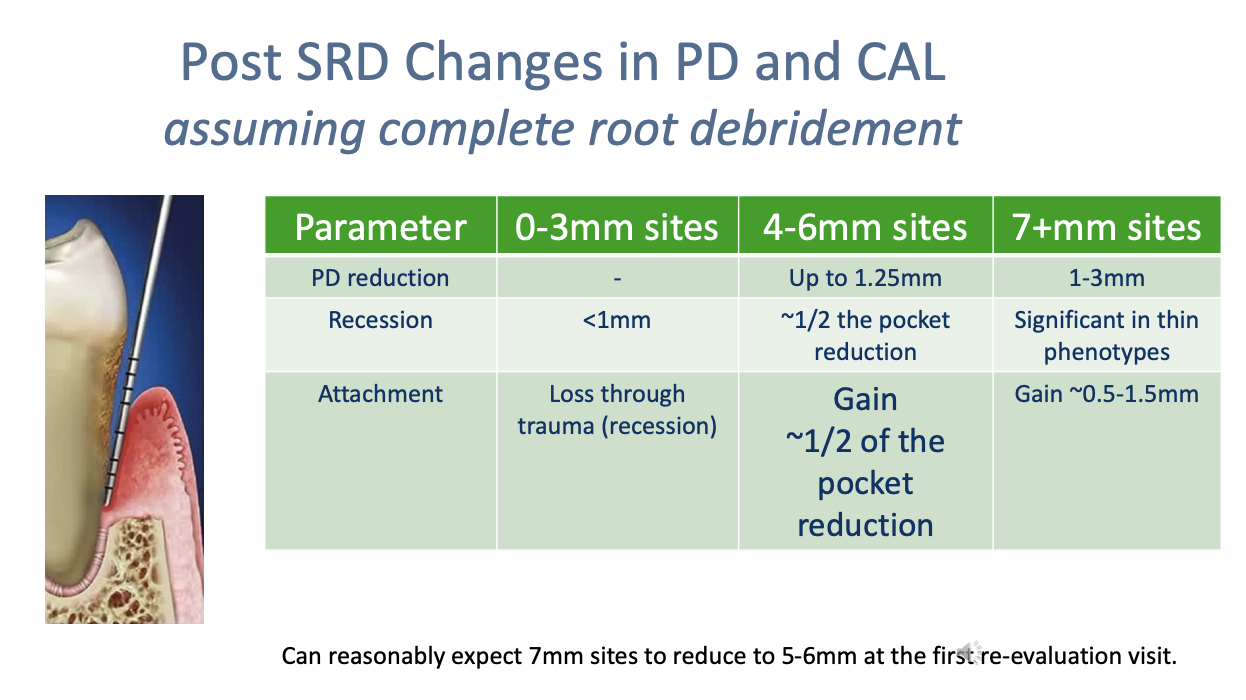
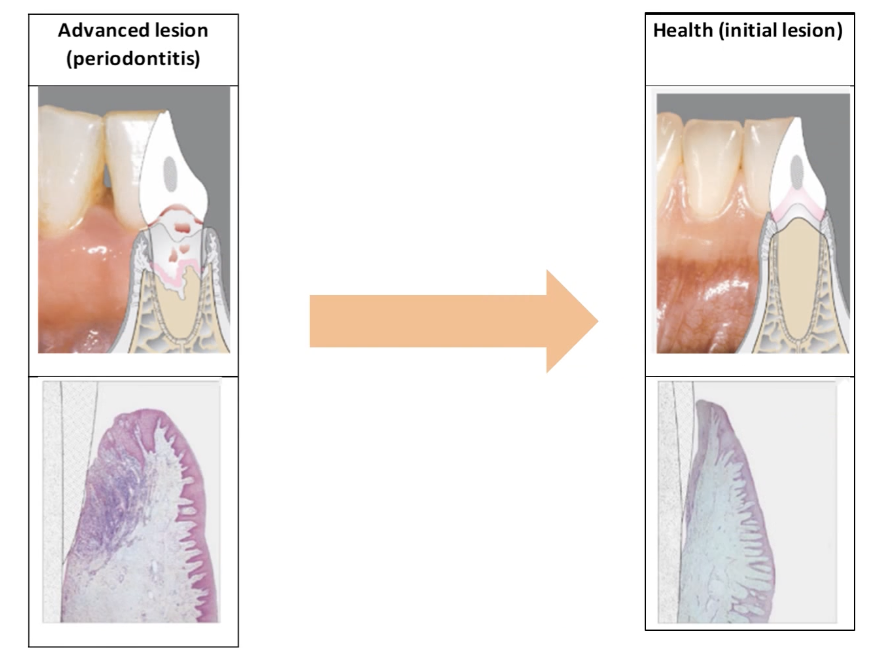
Once a patient has periodontitis, the damage to the periodontal ligament and alveolar bone is irreversible.
The pocket heals and reduces in depth by recession of the gingival tissue, formation of repair tissue (long junctional epithelium) and a small amount of regenerated PDL and bone in the most apical part of the pocket.
Topic 3: Risk Assessment in Periodontics
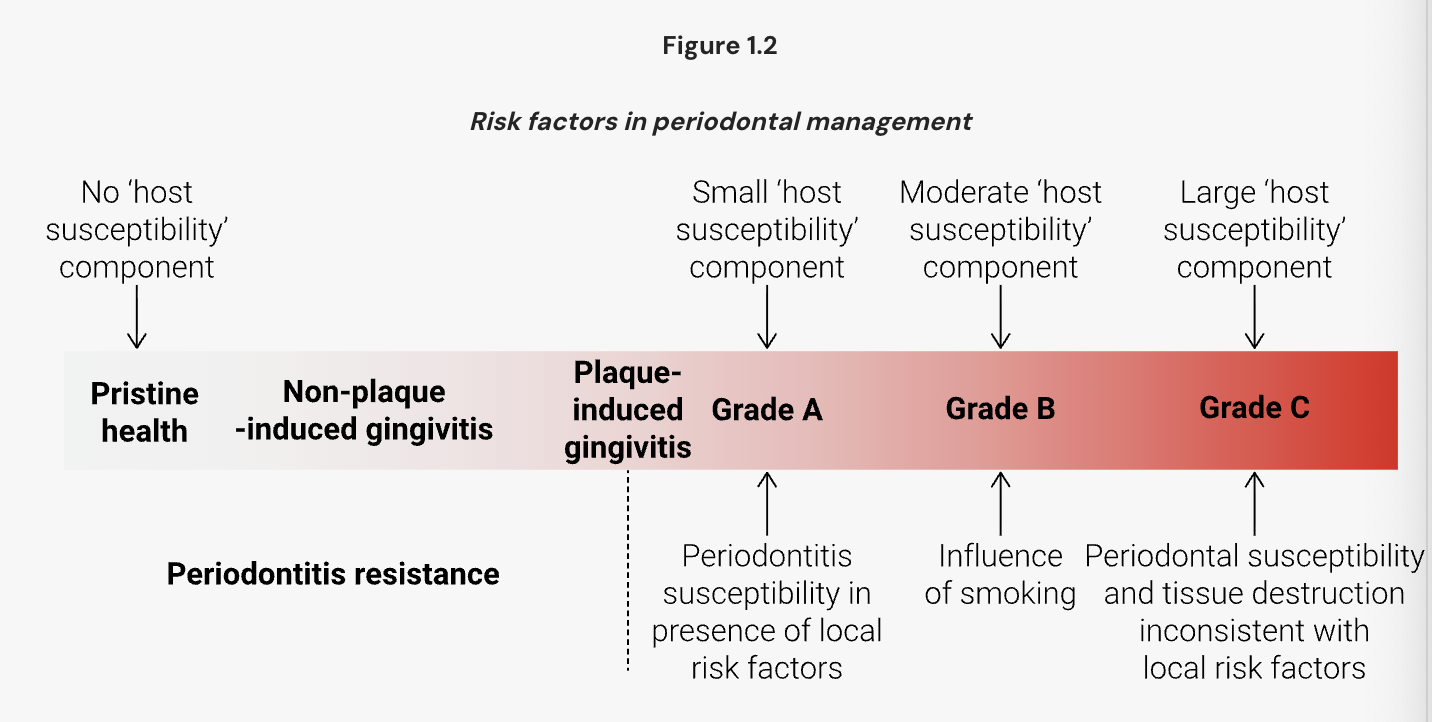
2 Types of Risk Factors:
Modifiable Risk Factors
Fixed Risk Factors
Patient Level Risk Factor:
Patient Level
— systemic, genetic, social, behavioural factors
— medical status
— full mouth plaque score
— loss of teeth (lost more than 8 = risk)
— compliance w/ treatment
Tooth Level
— restorative status (caries, fractures, resorptive lesions)
— tooth position/crowding
— furcation involvement (plaque retention)
— residual support
— mobility
— Iatrogenic factors (clinician errors such as overhangs)
— open contacts
— ortho
— mouth breathing
— xerostomia
Site Level
— Periodontal parameters (probing depth, recession, CAL, furcation lesions)
— Root grooves
— Developmental anomolies
— Vertical bone loss
Topic 4: Periodontal Maintenance or Supportive Periodontal Therapy
Why isn’t non-surgical periodontal treatment not enough to treat periodontitis?
perio patients are always susceptible to breakdown in the presence of plaque
pockets recolonize even with good oral hygiene
periodic debridement is required to reduce bacteria and disrupt the biofilm
periodic exams are to detect sites breaking down and to detect other oral conditions
How does recolonisation happen?
bacerial resevoirs on the tongue/tonsils
bad oral hygiene
incomplate plaque/calculus removal
deep residual pockets hide bacteria well

Control Group:
Excellent plaque control
healthy gingiva
shallow PD
stable attachment levels
no tooth loss
No Recall Group:
Recurrent periodontitis
GIngivitis
Deep pocjets
Ongoing attachment loss
Some tooth loss

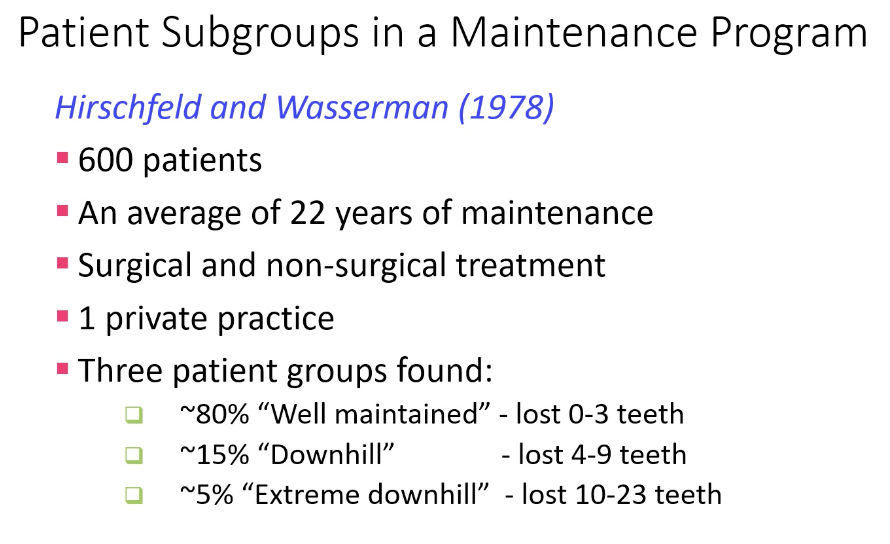
Results:
tooth loss was related to patient type (rather than the treatment provided)
most teeth lost in each group were furcation-involved molars
What are the aims of periodontal maintenance?
Preserve periodontal attachment
Resolve inflammation
Re-evaluate home care
Maintian a healthy + functional oral environment
Prevention of re-infection of pockets
Periodically disturb sub-gingival plaque to prevent establishment of pathogens
Does SPT (supportive periodontal therapy) help to compensate for poor oral hygiene?
yes
“Ramfjord and coworkers (1982) observed 78 periodontitis patients over seven years of maintenance. Baseline treatment consisted of scaling and root planing and occlusal adjustment as required. The cohort was then divided into four groups according to plaque control. The long-term results of the group with the worst oral hygiene were compared to those of the best plaque control group.”
How do we improve patient compliance?
simplify routine
accomodate for the patient’s needs
keep records of compliance
involve patients in treatment
positive reinforcement
identify non-compliers to adjust treatment
hygienists ensure dentist is involved in maintenance visit
explain what gingivitis/periodontitis is (why, who, how)
Summary:
Healing after debridement
Ideally periodontal wound healing would predictably result in formation of new cementum, periodontal ligament (PDL) and alveolar bone.
Most of the healing is achieved via a long junctional epithelial scar.
Excellent plaque control is vital for healing to prevent re-infection of the healing pocket.
Periodontal re-evaluation
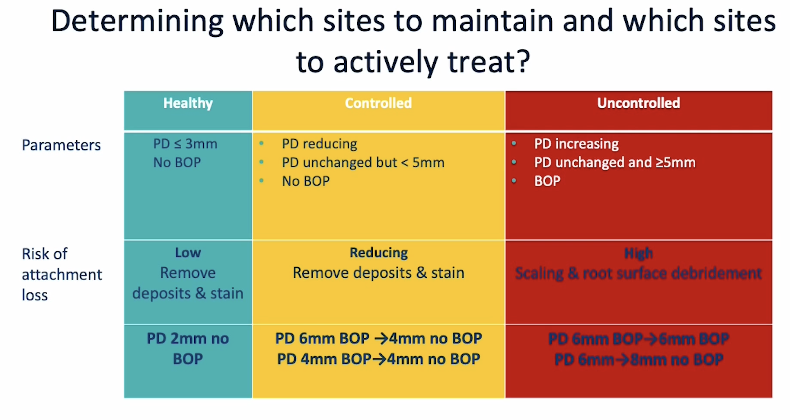
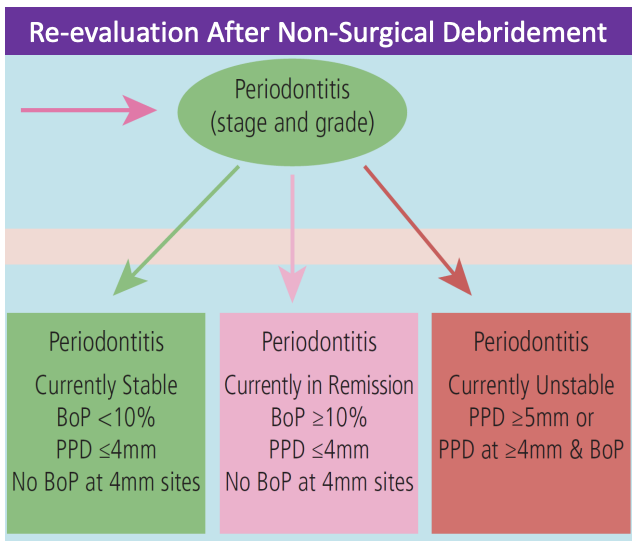
Periodontal re-evaluation detects uncontrolled periodontal risk factors.
Re-evaluation identifies the need for active treatment of unresponsive sites.
Changes in a patient’s periodontal risk profile are accounted for by formulating a new post-treatment diagnosis statement.
Periodontal risk assessment
Periodontal re-evaluation identifies changes in periodontal parameters that occur after non-surgical debridement and also during the maintenance phase of periodontal treatment.
Patient-level risk assessment:
determines the risk profiles of a patient at baseline, re-evaluation and during the maintenance phase.
is used to schedule appropriate recall periods for a patient to remain periodontally stable by adequate control of risk factors.
Tooth and site-level risk assessment:
identifies teeth and sites that are at high risk of ongoing attachment loss.
determines the treatment needs for a site which is breaking down.
Changes in a patient’s periodontal risk profile are accounted for by formulating a new post-treatment diagnosis statement.
Periodontal maintenance
Supportive periodontal therapy (SPT) plays a big role in controlling and reducing modifiable risk factors on a patient, tooth and site level.
The reduction in risk over consecutive appointments can be demonstrated using serial spiderwebs (PRA).
SPT aims to prevent periodontal breakdown by periodically breaking up subgingival plaque to maintain symbiosis and to reinforce oral hygiene practices with the patient.
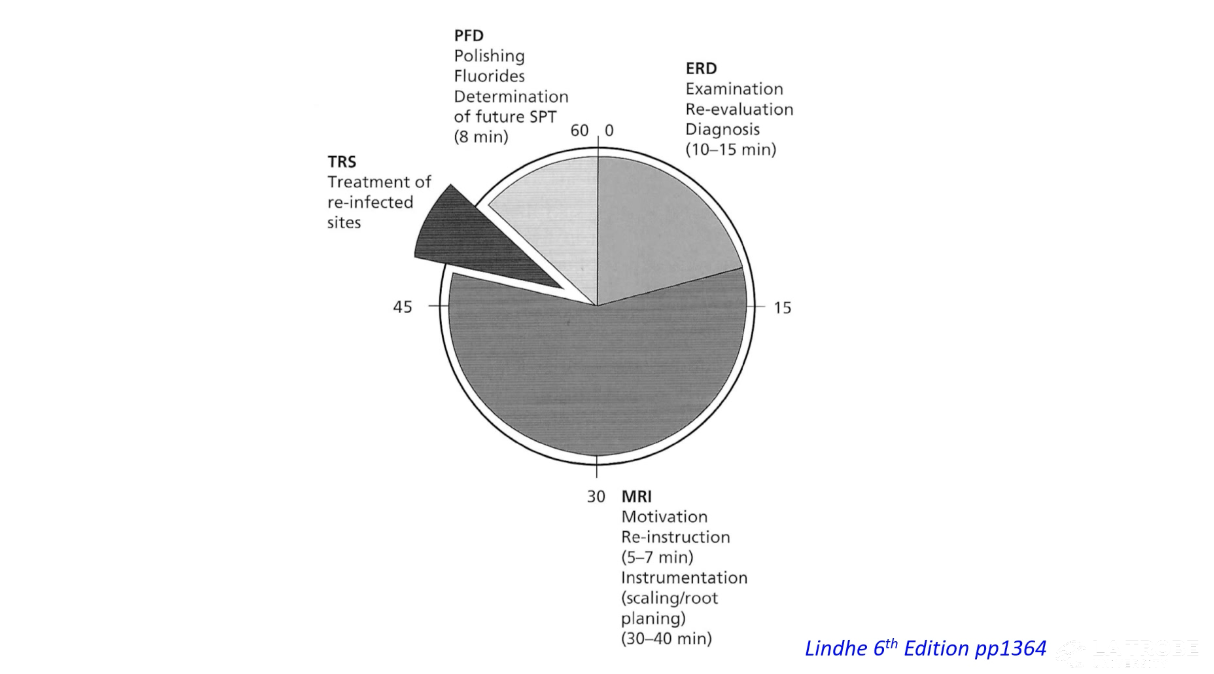
SPT visits include a re-evaluation phase, a reinstruction phase, an instrumentation phase, treatment of reinfected sites and a polishing phase.
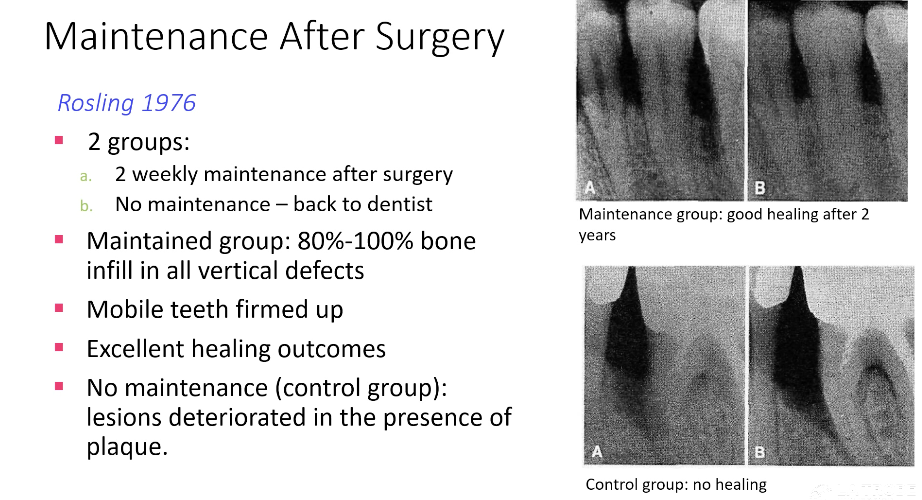
Excellent oral hygiene and SPT visits are required for good healing outcomes, irrespective of the type of periodontal therapy provided (i.e. nonsurgical or surgical).
SPT can compensate for poor plaque control provided patients are compliant with appointments.
Patient motivation for oral hygiene can be improved by simplifying their routine, accommodating their needs, keeping records and showing patients their current status, involving patients in their treatment and providing positive reinforcement.