Block 4 Study Guide
Know the parts of the scapula, clavicle, humerus, ulna, and radius.
arm: shoulder to elbow
shoulder dislocation: head of the humerus is displaced from the scapula
shoulder separation: torn ligaments
forearm/ antebrachial region : elbow to wrist
hand: wrist to fingers
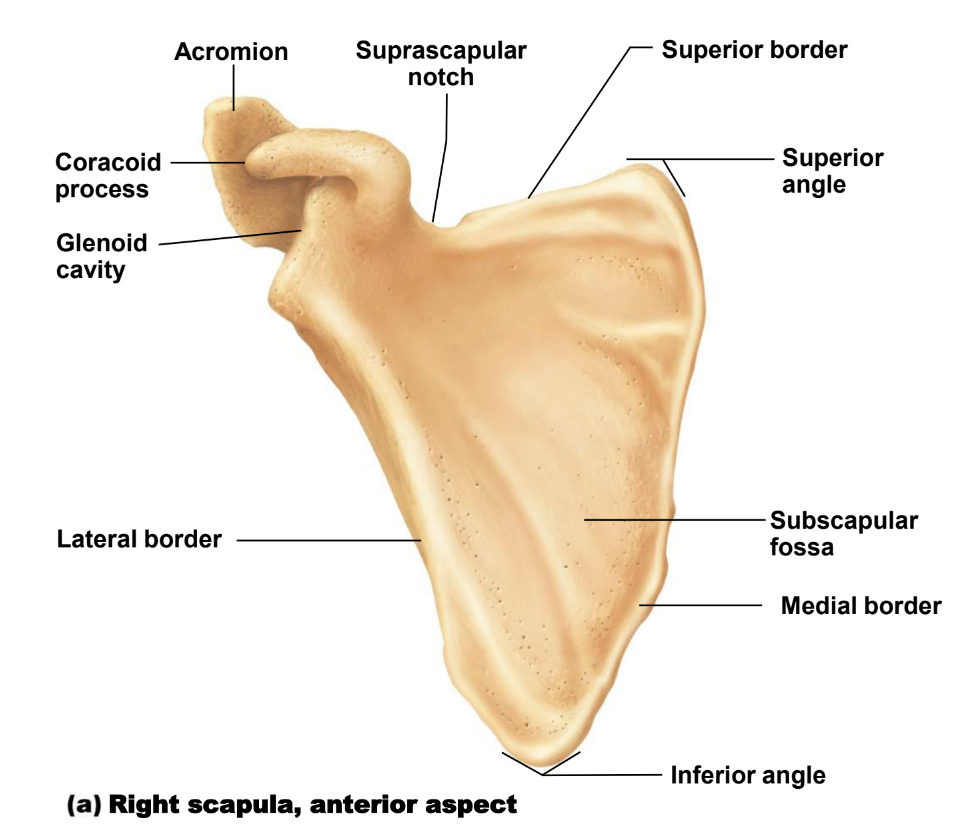
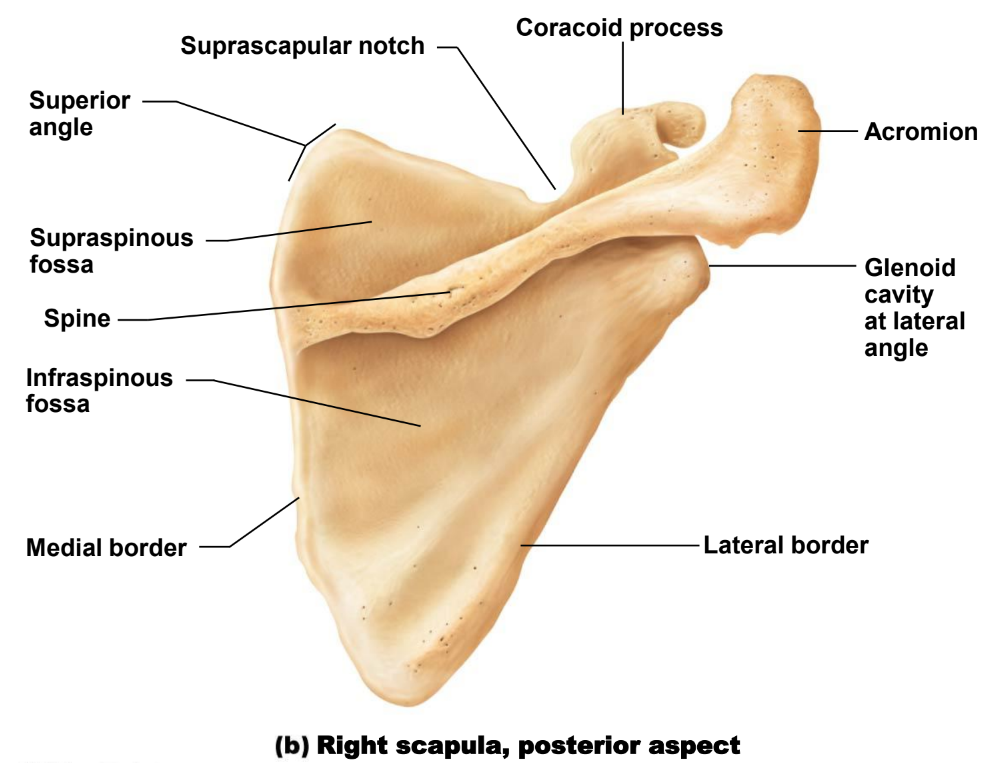
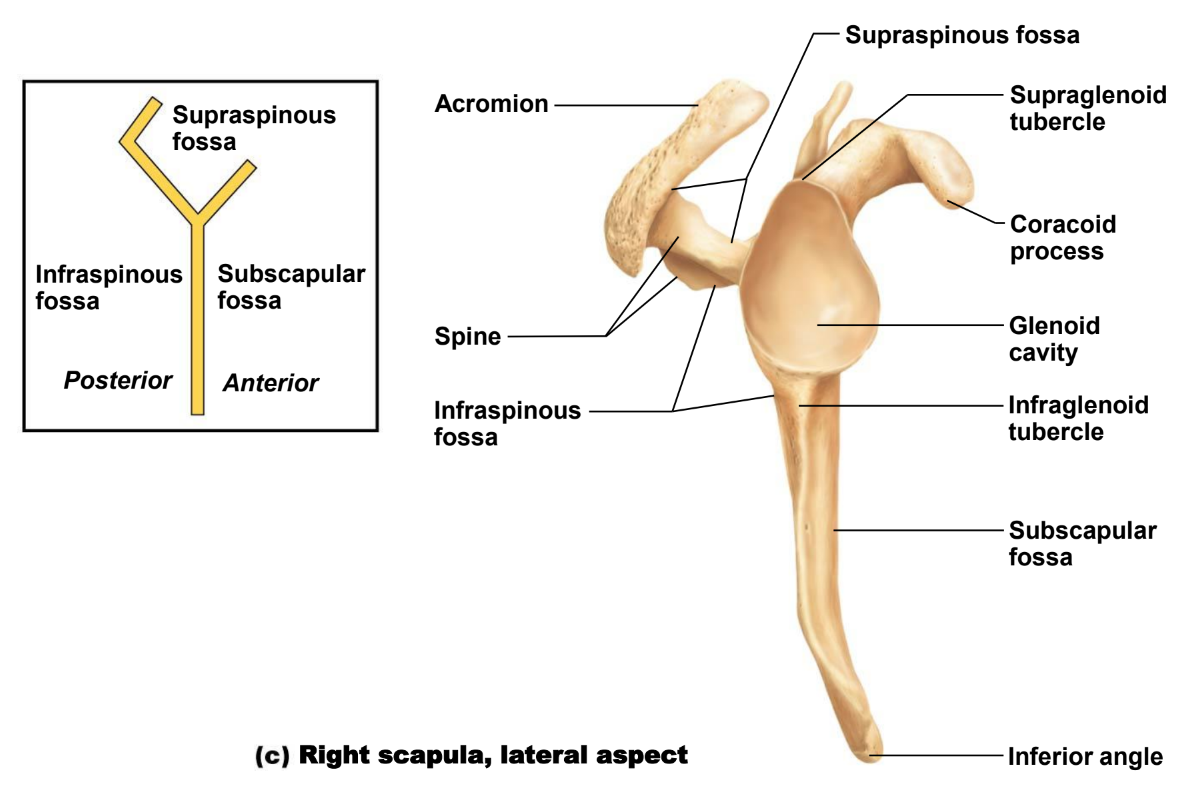
scapula:
weirdly shaped
no posterior articulation
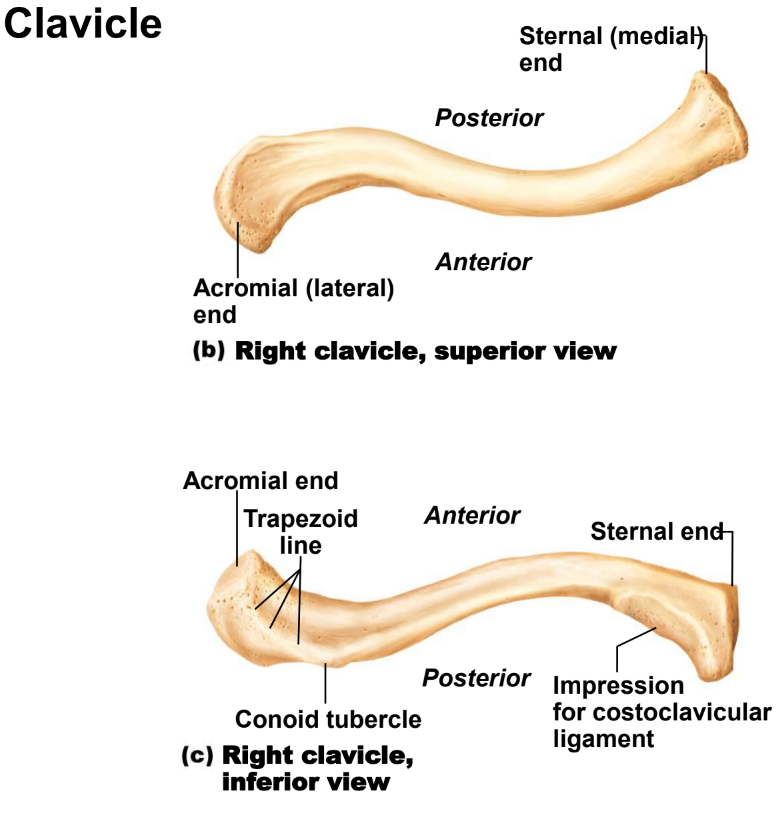
clavicle (collarbone)
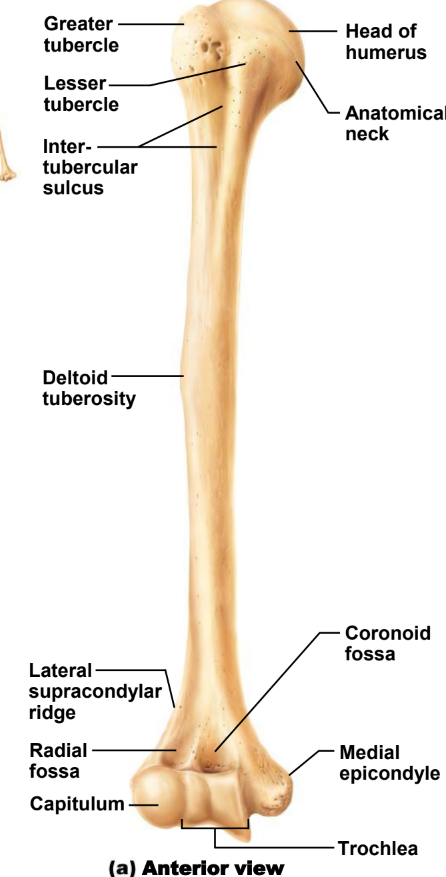
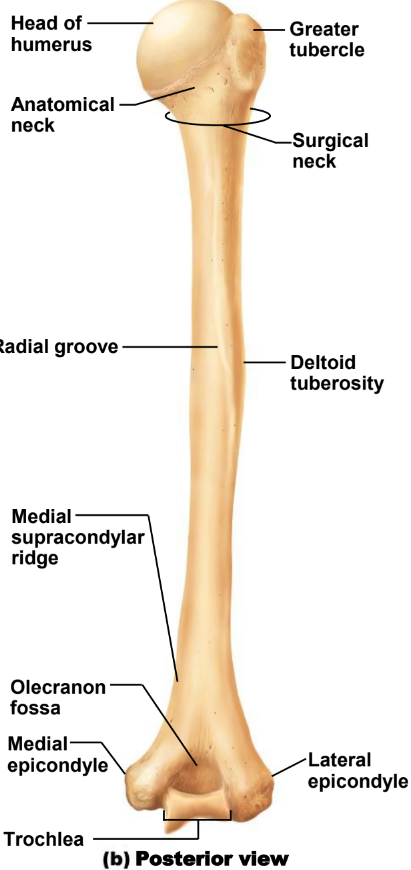
humerus
ulna
c - shaped proximal end
the head is on the distal end
radius
Know the names and locations of the carpals, metacarpals, and phalanges.
carpals (wrist):
hamate
capitate
pisiform
triquetrum
lunate (most dislocated)
trapezium
trapezoid
scaphoid (most frequent to fracture)
metacarpals (palm):
head, shaft, and base; numbered I-IV starting with the thumb
phalanges (finger):
distal
middle
proximal
Know the Clinical significance with fractures of the humerus.
surgical neck:
injury to axillary nerve
middle of shaft:
may cause injury to the radial nerve = wrist drop
distal end of humerus:
injury to median nerve
medial epicondyle:
injury to ulnar nerve
traumatic separation of the proximal epiphysis under 18-20 years old
dislocation of the shoulder joint
What are the four joints of the shoulder and where are each located?
acromioclavicular joint
location: where the clavicle meets the acromion of the scapula
scapulothoracic joint
location: where the scapula glides on the rib cage
sternoclavicular joint
location: where clavicle meets sternum
glenohumeral joint
location: where humerus meets scapula
Know the locations, function, and innervations of the following: all rotator cuff muscles, teres major, latissimus dorsi, trapezius, levator scapulae, rhomboid major, rhomboid minor, deltoid, coracobrachialis, pectoralis major, pectoralis minor, serratus anterior, subscapularis, biceps brachii, brachialis, triceps brachii, and aconeus.
rotator cuff muscles
supraspinatus
origin: scapula, supraspinatus fossa
insertion: humerus, greater tuberosity
innervation: suprascapular n (C4-C6)
action: abduction
infraspinatus
origin: scapula, infraspinous fossa
insertion: humerus, greater tuberosity
innervation: suprascapular n (C4-C6)
action: external rotation
teres minor
origin: scapula, lateral border
insertion: humerus, greater tuberosity
innervation: axillary n (C5,C6)
action: external rotation, weak adduction
subscapularis
origin: scapula, subscapular fossa
insertion: humerus, lesser tuberosity
innervation: suprascapular n (C5,C6)
action: internal rotation
teres major
origin: scapula (inferior angle)
insertion: crest of less tuberosity of the humerus (anterior angle)
innervation: lower subscapular nerve (C5-C7)
action: internal rotation, extension
latissimus dorsi (coughing muscles)
vertebral
origin: spinous process T7-T12 vertebrae; thoracolumbar fascia
insertion: crest of less tuberosity of the humerus (anterior angle)
innervation: thoracodorsal nerve (C6,C7,C8)
action: internal rotation, adduction, extension, respiration (cough muscle )
scapular
origin: scapula (inferior angle)
insertion: crest of less tuberosity of the humerus (anterior angle)
innervation: thoracodorsal nerve (C6,C7,C8)
action: internal rotation, adduction, extension, respiration (cough muscle )
costal
origin: 9th to 12th rib
insertion: crest of less tuberosity of the humerus (anterior angle)
innervation: thoracodorsal nerve (C6,C7,C8)
action: internal rotation, adduction, extension, respiration (cough muscle )
iliac
origin: iliac crest (posterior one third )
insertion: crest of less tuberosity of the humerus (anterior angle)
innervation: thoracodorsal nerve (C6,C7,C8)
action: internal rotation, adduction, and extension
trapezius:
descending part:
origin: occipital bone; spinous process C1-C7
insertion: clavicle (lateral 1/3)
innervation: accessory n (CN XI); cervical plexus (C3-C4)
action: draws scapula obliquely upward; rotates gleniod cavity superiorly; tilts head to same side and rotates it to opposite
transverse part:
origin: aponeurosis at T1-T4 spinous processes
insertion: acromion
innervation: accessory n (CN XI); cervical plexus (C3-C4)
action: draws scapula medially
ascending part:
origin: spinous process T5-T12
insertion: scapular spine
innervation: accessory n (CN XI); cervical plexus (C3-C4)
action: draws scapula medially downward, entire muscles; steadies scapula on thorax
levator scapula
origin: transverse process of C1-C4
insertion: scapula (superior angle )
innervation: dorsal scapular
action: draws scapula medially upwards while moving inferior angle ,medially; inclines neck to same side
rhomboid minor
origin: spinous process of C6,C7
insertion: medial border of scapula above (minor) and below (major) scapular spine
innervation: dorsal scapular n (C3,C4)
action: steadies scapula; draws scapula medially upward
rhomboid major
origin: spinous process of T1-T4 vertebrae
insertion: medial border of scapula above (minor) and below (major) scapular spine
innervation: dorsal scapular n (C3,C4)
action: steadies scapula; draws scapula medially upward
deltoid
function: most important abductor of the arm 90 degree
innervation: axillary nerve C5-C6
anterior part: flexes the arm (anteversion) + medial rotation of the arm
middle part: abducts the arm
posterior part: extends (retroversion) + lateral rotation
coracobrachialis
origin: scapula (coracoid process)
insertion: humerus
innervation: musculocutaneous n. C6,C7
action: flexion, adduction, internal rotation
pectoralis major
clavicular:
origin: clavicale
insertion: humerus
innervation: C5-T1
action: entire muscle: adduction, internal rotation, clavicular and sternocostal parts: flexion; assist in respiration when shoulder is fixed
sternocostal:
origin: sternum and coastal cartiale
insertion: humerus
innervation: C5-T1
action: adduction, internal rotation, clavicular and sternocostal parts: flexion; assist in respiration when shoulder is fixed
abdominal:
origin: rectus sheath
insertion: humerus
innervation: C5-T1
action: adduction, internal rotation, clavicular and sternocostal parts: flexion; assist in respiration when shoulder is fixed
pectoralis minor
orgin: 3rd-5th rib
insertion: coracoid process
innervation: medial and lateral pectoral n C6-T1
action: draws scapula downward, causing inferior angle to move posteromedially; rotates glenoid inferiorly; assists is respiration
serratus anterior
superior
origin: 1st - 9th rib
insertion: scapula
innervation: long thoracic n C5-C7
action: lowers raised arm
intermediate
origin: 1st - 9th rib
insertion: scapula
innervation: long thoracic n C5-C7
action: entire muscle draws scapula laterally forward; elevates ribs when shoulder is fixed
inferior
origin: 1st - 9th rib
insertion: scapula
innervation: long thoracic n C5-C7
action: rotates scapula laterally
subscapularis
origin:
insertion:
innervation: upper/lower subscapular nerves C5-C6-C7
action: arm adduction and medial roataion
biceps brachii
long head
origin: supraglenois tubercle of scapula
insertion: radial tuberosity
innervation: musculocutaneous C5-C7
action:
elbow join: flexion, supination
shoulder joint: flexion, stabilization of humeral head during deltiod contraction; abduction and internal rotation of the humerus
short head
origin: coracoid process of scapula
insertion: radial tuberosity
innervation: musculocutaneous C5-C7
action: flexion, stabilization of humeral head during deltiod contraction; abduction and internal rotation of the humeru
brachialis
origin: humerus
insertion: ulnar tuberosity
innervation: musculocutaneous n. C5-C7 and radian n. C7,minor
action: flexion at the elbow joint
triceps brachii
origin:
insertion:
innervation: olecranon of the ulna
action: elbow joint extension, shoulder joint long head extension and adduction
anconeus
origin: lateral epicondyle of humerus
insertion: olecranon of ulna
innervation: radial n. C6-C8
action: extends the elbow and tightens the joint
Know the Clinical significance of a “winged scapula.” How are two ways this could happen, i.e., what muscles and corresponding nerves would be damaged? How would you determine which muscles are compromised?
clin sig:
someone with a winged scapula would not be able to lift the arm beyond 90 degrees. It causes weakness in the muscles of your neck, shoulders, and arms
muscles damaged
1) Serratus Anterior (long thoracic)
2) Rhomboids (dorsal scapular)
if patient can lift arm over head; serratus anterior is fine and rhomboids are damaged. if they can only lift 90 degrees; serratus anterior is damaged.
Which veins are utilized during a venipuncture, and why?
veins of the (ante)cubital fossa (cephalic, median cubital, basilic) are frequently used due to the cross sectional area and visibility
Know all nerves of the brachial plexus and the roots from where the plexus originates.
musculocutaneous nerve- roots C5-C7
axillary nerve- roots C5 and C6
median nerve- roots C6-T1
radial nerve- roots C5-T1
ulnar nerve- roots C8-T1
additional brachial plexus nerves- dorsal scapular, suprascapular, subclavius, lateral pectoral, medial pectoral, upper subscapular (USS), thoracodorsal (TD), lower subscapular (LSS), medial brachial cutaneous (MBC), medial antebrachial cutaneous (MABC), lon thoracic
Know the Clinical significance of all brachial plexus injuries.
brachial plexus neuropraxia (stretch):
Root compression usually by rotation of the head; commonly seen in older individuals
Nerve traction is a result of a downward pull; common among adolescents and young adults
Both characterized as "burners" or "stingers" depending on the sensation felt with each injury
Brachial Plexus Rupture:
A forceful stretch resulting in the partial or complete tear of a nerve
Associated with muscle weakness and pain, severity depends on location and extent of injury
Often require surgery to repair
Brachial Plexus Neuroma:
Commonly occurs when a nerve is cut during surgery
Scar tissue forms a painful knot on the nerve, preventing it from healing itself
Surgery often required to remove scar tissue
Brachial Plexus Avulsion:
Nerve root is completely separated from spinal cord
Common injury during childbirth (2/1000 births), among athletes, and blunt trauma
Two types depending on nerves involved
Treatment depends on severity
What are the lymph node groups in the axillary region, and how are they involved in lymph drainage of the breast and upper limb?
groups:
pectoral, lateral, apical, central, and posterior
Drainage:
subclavian lymphatic trunk to right lymphatic duct to right venous angle
75% of breast lymphatics drain to the lymph nodes of the axillary region
What is the Clinical significance of Colle’s fracture?
clin sig:
fracture of the radial styloid process; posterior displacement forces the process into the shaf
this can happen by falling on the hand while the arm is extend and may be accompained by avulsion of ulnar styloid process
Know the locations, innervations, and origins/insertions of the following muscles of the Forearm:
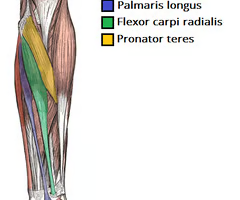
Anterior Compartment-Superficial
Pronator teres
innervated: by the median nerve
origin: Humeral head: medial supracondylar ridge of humerus Ulnar head: Coronoid process of ulna
insertion: Lateral surface of radius (distal to supinator)

Flexor carpi radialis
innervated: by the median nerve
inserts: at the bases of the 2nd and 3rd metacarpal bones
Palmaris longus
innervated by the median nerve
originates: at the medial epicondyle of the humerus and inserts: a bit, at the flexor retinaculum
Flexor carpi ulnaris
innervated: by the ulnar nerve (C7-T1)
inserts: at the base of the metacarpal bone 5
originates: from the Lateral epicondyle of humerus, posterior border of ulna
Anterior Compartment- Intermediate
Flexor digitorum superficialis
innervated: by the median nerve
origin/ insertion divided into two heads; a humeroulnar head and radial head.
its large muscular belly courses distally towards the wrist,
where it splits into four tendons and attaches to the middle phalanges of the second through fifth digits of the hand

Anterior Compartment- Deep
Flexor digitorum profundus
innervation: median n and median n
origin: ulna and interosseous membrane
insertion: distal phalanges 2nd and 5th digits
Flexor pollicis longus
innervation: median n
origin: radius and adjacent interosseous
insertion: distal phalanax of thumb
Pronator quadratus
innervation: median n
origin: distal quarter of ulna
insertion: distal quarter or radius

Posterior Compartment- Superficialis
Extensor digitorum
innervation: posterior interosseous nerve, which is a branch of the radial nerve
origin: common head
insertion: dorsal digit expansion of 2nd to 5th digits
Extensor digiti minimi
innervation: radial n
origin: common head
insertion: dorsal digit of 5th digit
Extensor carpi ulnaris
innervation: radianl n
origin: comon head and ulnar head
insertion: base of the 5th metacarpal

Posterior Compartment- Deep
Supinator
innervation: radianl n.
origin: olecranon, lateral epicondyle of humerus, radial collateral ligament annular ligament of radius
insertion: radius (b/w radial tuberosity and insertion of pronator teres)
Abductor pollicis longus
innervation: radial n
origin: radius and ulna
insertion: base of 1st metacarpal
Extensor pollicis brevis
innervation: radial n
origin: radius and interosseous membrane
insertion: base of proximal phalanx of thumb
Extensor pollicis longus
innervation: radial n
origin: ulna and interosseous membrane
insertion: base of distal phalanx thumb
Extensor indicis
innervation: radial n
origin: ulna and interosseous membrane
insertion: posterior digital extension of 2nd digit
Radialis Group
Brachioradialis
innervation: radial n
origin: dital humerus
insertion: radial styloid process
Extensor carpi radialis longus
innervation: radial n
origin: lateral supracondylar and ridge of distal humerus
insertion: 2nd metacarpal base
Extensor carpi radialis brevis
innervation: radial n
origin: lateral epicondyle of humerus
insertion: 3rd metacrapal base
Know the Clinical significance of carpal tunnel, including the associated tendons.
two rows of the carpal bones produce the carpal groove which is concave anteriorly
flexor retinaculum which is a Double layer of membrane covering the carpal groove anteriorly and produces the carpal tunnel for of flexor muscles and median nerve to pass through this tunnel
carpal tunnel syndrome:
compression to the median nerve in the tunnel due to hypothyroidism, rheumatoid arthritis, pregnancy, and amyloidosis
the structures that pass through this tunnel are
flexor digitorum superficialis and profundus
flexor pollicis longus
median nerve
Know the Clinical significance of scaphoid and lunate fractures and/or dislocations
ccaphoid fractures are the most common carpal bone fractures, generally occurring at the narrowed waist between the proximal and distal poles (A, right scaphoid)
bc blood supply to the scaphoid is transmitted via the distal segment, fractures at the waist can compromise the supply to the proximal segment, often resulting in nonunion and avascular necrosis (meaning the scaphoid bone can die)
Know the locations, functions, and innervation of the following:
Thenar muscles
Adductor pollicis
innervation: ulnar n
function: carpometacarpal joint of thumb; adduction and metacarpophalangeal joint of thumb: flexion
Abductor pollicis brevis
innervation: median n
function:carpometacarpal joint of thumb; adbuction
Flexor pollicis brevis
innervation: median n and ulnar n
function: carpometacarpal joint of thumb flexion
Opponens pollicis
innervation: median n
function: carpometacarpal joint of thumb; opposition
Hypothenar muscles
Opponens digiti minimi
innervation: ulnar n
function: draws metacarpals in palmar direction (opposition)
Flexor digiti minimi
innervation: ulnar n
function: metacarpophalangeal joint little fingers; flexion
Abductor digiti minimi
innervation: ulnar n
function: metacarpophalangeal joint little fingers; flexion and abduction of little fingers and helps in extension of little fingers
Palmaris brevis
innervation: ulnar n
function: Tightens the palmar aponeurosis (protective function)
Know the Clinical significance of the “anatomical snuffbox.0”
snuffbox borders:
tendon of extensor pollicis longus (superior), tendons of the extensor pollicis brevis, and abductor pollicis longus (inferiorly)
contents of snuffbox:
radial artery (gives blood to all of digit 1) and superficial radial nerve
this is significant b/c if you have a fracture at your scaphoid bone or a dislocation here, the scaphoid can be pushed in to that anatomical snuffbox
Know all Clinical symptoms regarding damage to the radial, median, and ulnar nerves.
radial nerve injury:
injury proximal to the origin of triceps
no extension of elbow
no triceps reflex
wrist drop, thumb is flexed and adducted
sensory loss: dorsolateral lower brachial region, posterior surface of forearm, dorsum of the hand and radial side of proximal phalanges
injury to the nerve on rdial grove:
fractures of humerus
triceps muscle is usally functioning
wrist drop and sensory loss in dorsolateral aspect of teh forearm and hand
nerve injury in foramen:
deep radial nerve is injured
extension of teh thumb and metacarpal joints is disturebed
sensation is usally preserved
median nerve injury: opponens splint, C-bar or thumb post splint
injury above the elbow:
only muscles in the forearm and hand muscles are affected
all flexors of the wrist are paralyzed except flexor carpi ulnaris and the ulnar part of flexor digitorum profundus
thumb flexors and abductor paralyzed but not the adductor (ulnar nerve)
flexion at metacarpophalangeal joints possible (intact interossei muscles innervation by ulnar nerve)
1st and 2nd Lumbricals lost function and are unable to fully flex index and middle finger -- hand of benediction
pronation of forearm paralyzed and sensory loss over the median nerve area
injury at wrist joint:
short muscles of the thumb paralyzed, not adductor
thenar muscles atrophy; flexor polliicis longus functioning
sensory loss over medial nerve area
ulnar nerve injury:
at wrist:
claw hand
injury at elbow:
paralysis of dlexor capri and medial portion of flexor digitorum profundus
ulnar deviation of teh wrist is weakened