Anxiety
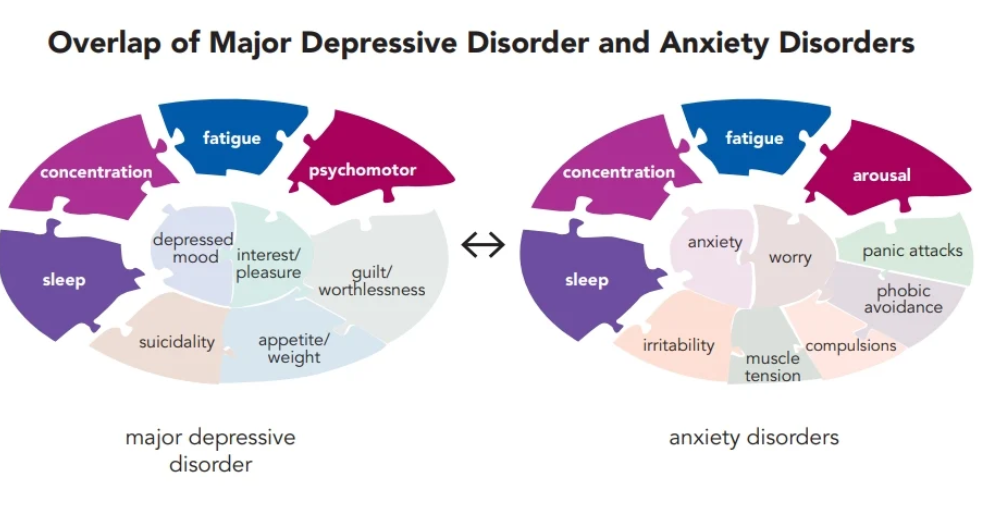
anxiety - - amygdala. worry/fear/trauma
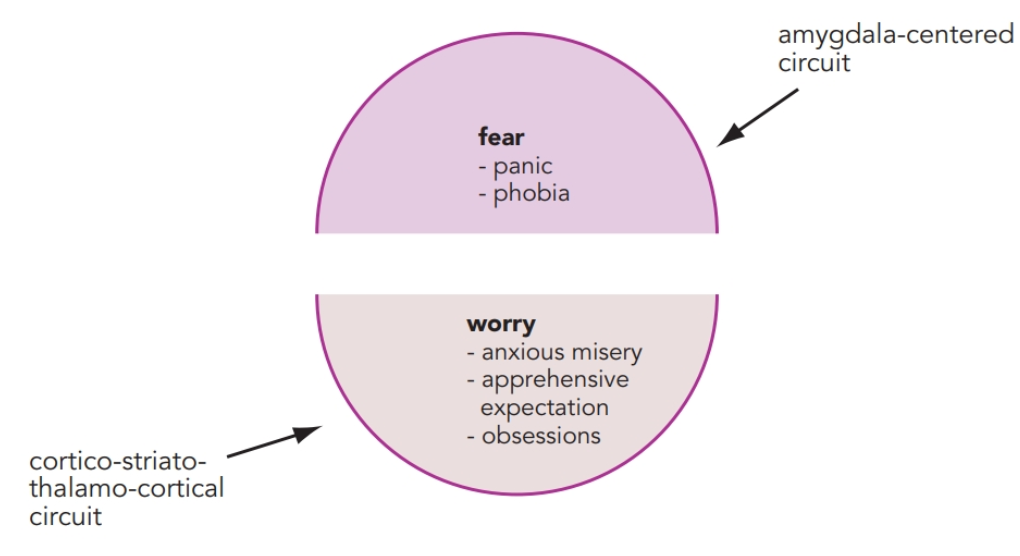
anxiety can be triggered internally from traumatic memories stored in the hippocampus and activated by connections with the amygdala
neurobiological regulator of amygdala is GABA, serotonin, and norepinephrine, and the voltage-gated calcium channels
neurobio regs of CSTC is 5HT, GABA, dopamin, norepinephrine, glutamate, and voltage gated ion channels
Benzos (diazepam alpralozam etc) - enhance phasic inhibition of GABA (γ-aminobutyric acid) by positive allosteric modulation of postsynaptic GABAA receptors. GABA more likely to bind. open ion channel, Cl in, less likely to fire action potential. modulate excessive output from worry loops by enhancing the actions of inhibitory interneurons in CSTC circuits
α2δ ligands (Gabapentin and pregabalin) - bind to the α2δ subunit of presynaptic N and P/Q VSCCs, block the release of excitatory neurotransmitters such as glutamate. α2δ ligands bind to open, overly active VSCCs in the amygdala to reduce fear, and in CSTC circuits to reduce worry. can ALSO be used in neuropathic pain, fibromyalgia, social anx disorder, panic disorder,epilepsy
Serotonin is a key neurotransmitter that innervates the amygdala as well as all the elements of CSTC circuits, namely, the prefrontal cortex, striatum, and thalamus. SSRIs SNRIs. buspirone, is recognized as a drug for generalized anxiety disorder, but not for treatment of the other anxiety/trauma disorder subtypes. 5HT1A agonists exert their therapeutic effects by virtue of adaptive neuronal events and receptor events. this means DELAYED response like SSRI etc. benzos FASTER
symptoms may be mediated in part by excessive noradrenergic input onto α1-and β1-adrenergic postsynaptic receptors in the amygdala. Symptoms of hyperarousal like nightmares can be reduced in some patients with α1-adrenergic blockers such as prazocin
symptoms of fear can be reduced by norepinephrine reuptake inhibitors. can be WORSE initially but eventually downregulate and desensitize postsynaptic norepinephrine receptors such as β1 receptors, and hypothetically lead to the delayed reduction in symptoms of fear and worry long term
Most contemporary psychopharmacological treatments for anxiety and fear act by suppressing the fear output from the amygdala, VMPFC processes it and if it doesn’t succeed VMPFC activates amygdala and fear response happens
Fear extinction is the progressive reduction of the response to a feared stimulus, and occurs when the stimulus is repeatedly presented without any adverse consequence. Modern research thus suggests that fear extinction theoretically predominates over fear conditioning when synaptic strengthening and long-term potentiation in the new circuit are able to produce an inhibitory GABAergic drive that can overcome the excitatory glutamatergic drive produced by the pre-existing fear-conditioning circuitry
Cognitive behavioral therapies that employ exposure techniques and that require the patient to confront the fear-inducing stimuli in a safe environment may come closest to facilitating fear extinction
pharmacologically boost N-methyl-D-aspartate (NMDA) receptor activation at the very time when a patient receives systematic exposure to feared stimuli during cognitive behavioral therapy sessions. enhance extinction
Therapeutic approach is to treat the acutely exposed patient immediately after a traumatic experience in order to block the initial fear from ever becoming conditioned or consolidated
the idea is to use both psychotherapeutic and psychopharmacological approaches to block reconsolidation of the fear memory. resconsol is when it is thought of again then stored again as a fear.
Early studies of β blockers suggest that they may also disrupt reconsolidation of fear memories as well as formation of fear conditioning. More recently, hallucinogens, dissociatives, and entactogens such as psilocybin, MDMA (3,4-methylene-dioxymethamphetamine), and ketamine have been employed in an attempt to block reconsolidation of activated memories during psychotherapy sessions
GAD
SSRIs, SNRIs, benzodiazepines, buspirone, and α2δ ligands. Other “off-label” treatments for anxiety can include mirtazapine, trazodone, vilazodone, tricyclic antidepressants sedating antihistamines such as hydroxyzine
CANT USE BENZOS IN ABUSE/ABUSE RISK PATIENTS
Social anx disorder
SSRIs and SNRIs and α2δ ligands, but NOT benzos. alch is risk here bc it works but bad idea. CBT can be strong
PTSD
SSRI monotherapy usually NOT used. Benzos w/ caution bc alch abuse is common. α1 antagonists (ex are doxazosin, terazosin, -osins and coreg) at night to prevent nightmares. Exposure therapy memes, blocking reconsolidation. Brexpiprazole, as a drug for psychosis, is in testing along with the SSRI sertraline for PTSD, with promising initial findings