Introduction + Plasma proteins
Blood Overview
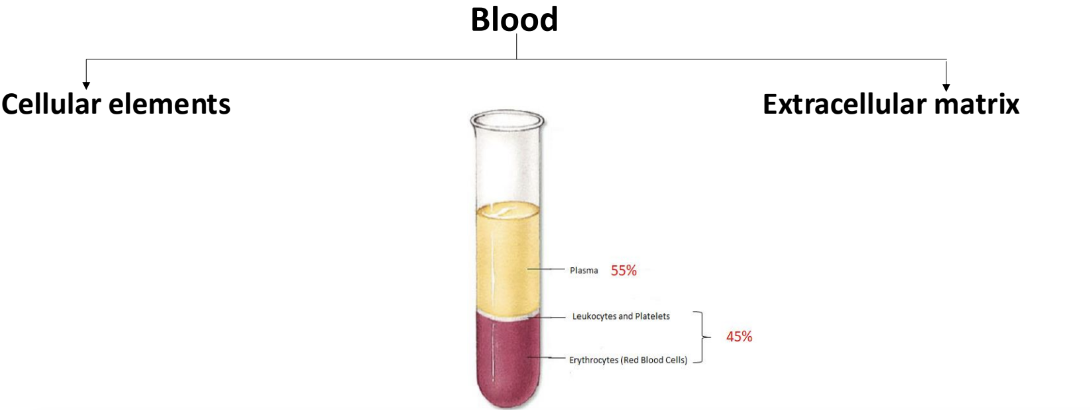
Haematology :- the study of the structure and function of blood- circulatory fluid of the body - it is a connective tissue made up of cellular elements and an extracellular matrix
Introduction & Plasma Components
Blood constitutes about 5-6 liters in males and 4-5 liters in females, weighing approximately 5.5 kg in total. It plays a crucial role in the body's physiological processes, being composed of both cellular elements and a fluid extracellular matrix known as plasma. The blood is vital for maintaining homeostasis, transporting nutrients and oxygen, and protecting against disease.
Average volume of blood: 5-6L for males and 4-5L for females (normovolemia)
viscosity - thicknness : 4-5 - where water is 1
the pH of blood: 7.35-7.45 - average is 7.4 - slightly alkaline
osmolarity: 300mOsm or 0.3 Osm
Salinity- 0.85% , isotonic - reflects the concentration of NaCl in the blood
Colour - colour of the blood varies with its oxygen content - when it has high oxygen content it is bright red
Cellular Components:
45% Red Blood Cells (RBCs)
The primary component of blood responsible for oxygen transport.
1% Buff coat (White blood cells and Platelets)
Critical for immune function and hemostasis.
55% Plasma
The liquid matrix that carries proteins, nutrients, hormones, and waste products.
Functions of Blood
Primary Functions:
Transportation- primary function → Carries oxygen from the lungs to the body tissues and carbon dioxide-which travels through the blood mostly as bicarbonate is transported from tissues as a waste product of cellular respiration to the lungs lungs for exhalation. It also transports nutrients and waste materials such as urea and creatinine for excretion support critical metabolic processes - all cells require oxygen and glucose to undergo cellular respiration .
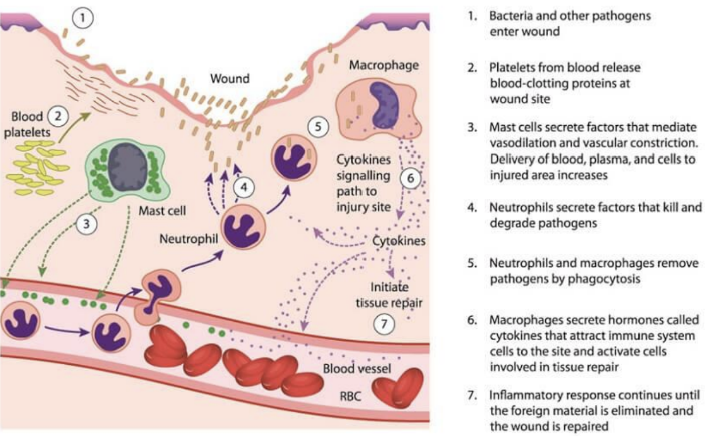
Defense: Acts as a key component of the immune system, defending against pathogens and foreign substances- activating WBCs to defend the body against foreign invaders
Thermoregulation: Distributes heat throughout the body, helping maintain a stable internal temperature.
Homeostasis: Maintains pH balance (7.35-7.45) and fluid volume, crucial for cellular functions.
Protection_ blood prevents blood loss by :
Activating plasma proteins and platelets - Plasma proteins include albumin, immunoglobulins, fibrinogens, alpha 1-antitrypsin, regulatory proteins etc. Immunoglobulins include alpha, beta and gamma (IgA, IgD, IgE, IgG, IgM)
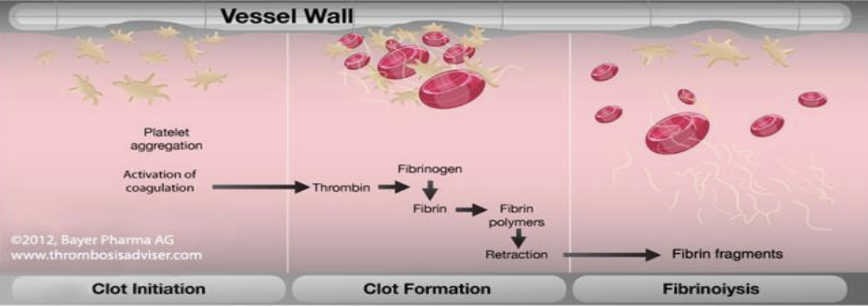
Initiating clot formation when a vessel is broken
Specific Roles of Blood:
Facilitates the transport of hormones from endocrine glands to their target cells, regulating various physiological activities.
Helps to remove excretory products and metabolic waste, contributing to the body's detoxification processes.
Blood Composition
Blood Cellular Elements
Red Blood Cells (Erythrocytes):
Characteristics: Most numerous blood cells- makes up half of blood volume; approximately 4.2-6.2 million cells per mm³. They have a unique biconcave shape - 7microm in diameter and 3.3microm thick that maximizes surface area for gas exchange and allows flexibility to navigate through capillaries - shape relates to its function
lack nuclei and mitochondria - fully packed with haemoglobin
Function: Primarily transport oxygen bound to haemoglobin and facilitate the exchange of carbon dioxide.
have a relatively short circulating life span - 120 days - older erythrocytes are removed from circulation by phagocytic cells in the liver, spleen and bone marrow
RBC investigations look into : number , size and Hb content and quality
White Blood Cells (Leukocytes):
Abundance: Less abundant than RBCs, around 5,000-9,000 per mm³.
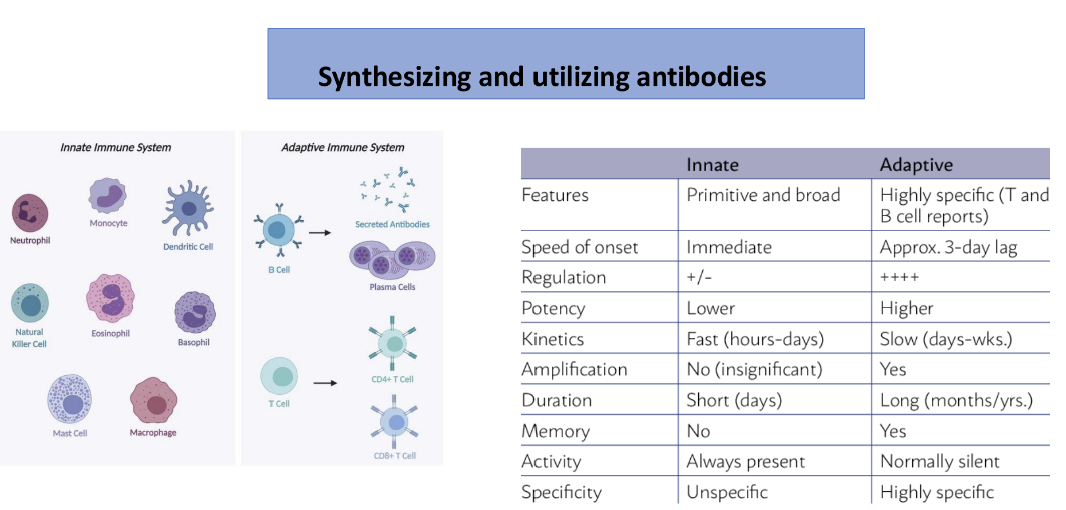
Responsible for defence & protection against invading organisms and foreign antigens - immunity
Differ from red blood cells – contain a nuclei and mitochondria
Can move in an amoeboid fashion – squeeze through pores in capillary walls and move to site of infection
Invisible under the light microscope – stained and classified according to their staining properties - Granular Leukocytes
and Agranular leukocytes
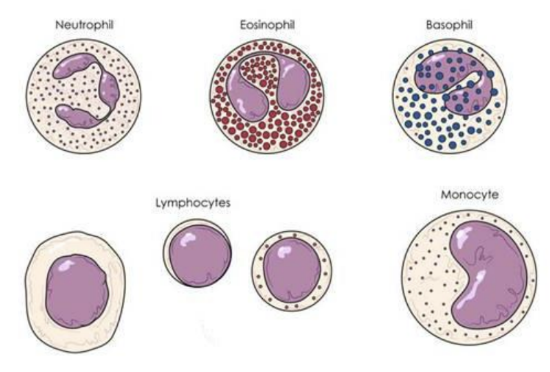
Classifications:
Neutrophils (50-70%): - most abundant
Engage in innate immune responses, recognizing and attacking pathogens through phagocytosis.
multilobed nucleus joined by thin chromatin strand -polymorphonuclear
cytoplasm- contains numerous fine granules staining pale pink with romanowksy dyes
spend 8-10 hours in circulation
exit into tissues → non-specific defense against bacterial and fungal infections
Lymphocytes (20-25%):- second most common Involved in adaptive immunity, including B-cells (produce antibodies) and T-cells (destroy infected cells).
Small cells (10-12mm diam.) with little cytoplasm -Round nucleus filling most of the cell
Variable lifespan from a few days to many years
Different types play distinct roles in specific immunity
T-lymphocytes – 40-80% of blood lymphocytes (cellular immunity) ; B-lymphocytes – 10-30% of blood lymphocytes - humoral immunity
Monocytes (5%): Differentiate into macrophages in tissues, aiding in phagocytosis and secretion of cytokines.
Large cell (16-22m diam.) with a kidney-shaped clefted nucleus
Fine granules & vacuoles in cytoplasm
Cells circulate for ~10 hours → exit into tissues → mature into actively phagocytic tissue macrophages
Responsible for removal and processing of aged cells and other cellular debris (tissue scavengers)
Important role in processing & presentation of Ag to T- lymphocytes
Eosinophils (1%): Combat parasitic infections and are involved in allergic reactions.
Large cytoplasmic granules which stain strongly with acidic dye eosin
Bilobed nucleus
Circulate for 4-5 hours → exit into tissues
Basophils (0.5-1%): Release histamine during allergic reactions and contribute to inflammation
Large cytoplasmic granules stain blue with basic dye methylene blue
Cells involved in - Hypersensitivity reactions, Inflammatory reactions, Anaphylactic reactions
WBC investigations look into : number of each type, morphology/ maturity
Platelets (Thrombocytes):
Count: Approximately 250,000-400,000 per mm³; critical for clot formation and wound healing.
Lifespan: Survive about 10-12 days in circulation before being removed by the spleen and liver.
Discoid and a nucleate cells with a granular cytoplasm- cytoplasm rich in granules and organelles that promote blood clotting
although small - they have a greater variety of functions than any other blood cell
Platelets can become activated → change shape → release granule contents → form aggregates (clots) → trigger coagulation
platelet investigations look into count and function :-increased platelet count or increased activity - thrombosis; reduced platelet counts or activity - haemorrhage and other bleeding disorders ex. haemophilia
Plasma Components
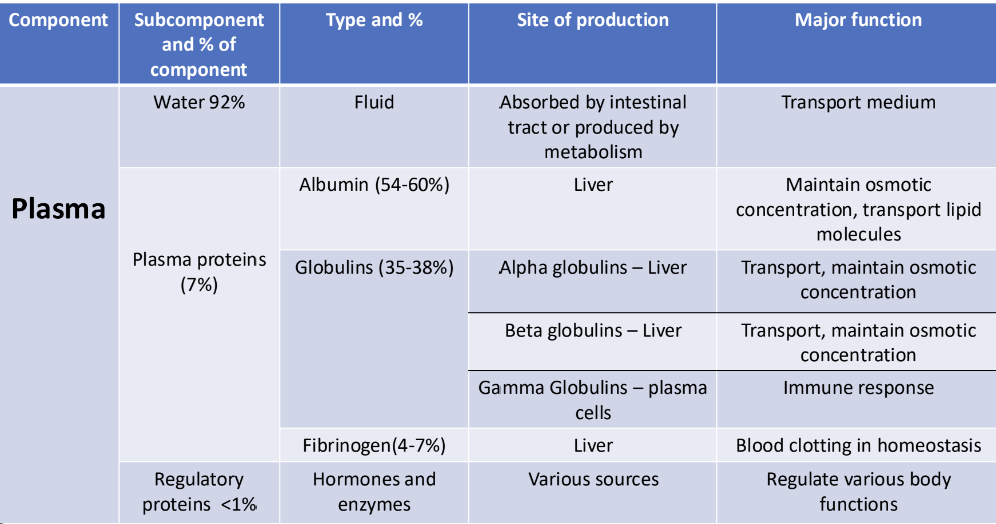
Composition: Plasma is composed of 92% water and 7% plasma proteins, with the remaining 1% making up electrolytes, nutrients, and waste products.
plasma proteins - play a number of important roles in the human body and measurement of plasma proteins is a routine laboratory test - 7% of total blood volume which levels can fluctuate at times
Plasma and Serum
• Plasma is composed of serum + clotting factors
• Serum is the part of blood that lacks clotting factors
• Plasma – clotting factors = Serum
Major Plasma Proteins:
Albumin (54-60%): Helps maintain osmotic pressure, ensuring fluid balance between blood and tissues; transports various substances.
Globulins (35-38%): Include immunoglobulins (antibodies) that defend against pathogens, and other proteins involved in transport and immune responses.
Fibrinogen (4-7%): Essential for blood clotting; converted to fibrin, forming a mesh that impedes blood loss from damaged vessels.
Plasma Proteins - Functions
1. Essential for Blood clotting – Fibrinogen and prothrombin are essential for coagulation of blood
2. Maintain Colloidal Osmotic Pressure of Blood and Aid in Regulating the Distribution of Fluid between blood and tissue
3. Maintain Viscosity and Blood Pressure – plasma proteins mainly globulins due to larger molecules and asymmetry of their structure are responsible to some extent for the viscosity of blood. Viscosity is an important factor in maintaining blood pressure
4. Act as Buffers – to maintain acid-base balance
5. Act as a Protein Reserve – plasma proteins serve as a store of proteins during starvation or inadequate protein diet
6. Immune Response - Immunoglobulins, Complement proteins involved in Inflammatory responses:
• Acute phase response proteins: C-reactive protein (CRP) produced by the liver and increase in inflammation
7. Help Transport of Certain Substances in blood – some plasma proteins combine with certain substances and carry them in blood stream ex some hormones, enzymes and clotting factors are part of the globulin fraction, iron (transferrin) and copper (ceruloplasmin) are bound to globulin fraction.
Albumin
smallest and most abundant plasma protein - 60-80% plasma protein
its role is to transport various plasma solutes and buffer the pH of the blood plasma - acts as carriers for other substances such as steroids, thyroid hormones fatty acids , bilirubin
makes a major contribution to 2 physical properties of the blood- viscosity and osmolarity
synthesised in the liver
its half life in plasma is 20 days
changes in albumin levels affect blood viscosity and osmolarity
hypoalbunemia - decreased albumin levels
Decreased synthesis
• May be due to malnutrition or mal-absorption • May be a feature of advanced liver disease
Abnormal distribution or dilution
• May be induced by overhydration,
• May be caused by increased capillary permeability as occurs in septicaemia
Abnormal excretion or degradation
• Excessive excretion by the kidneys (renal disease) • Burns • Haemorrhage
Dehydration on the other hand causes an increase in albumin levels
Globulins
Globulins are further divided into three subclasses
i. Alpha (α) globulins
• Synthesized in the liver
•Can be further subdivided into:
➢ α1 globulins
➢ α2 globulins
ii. Beta (β) globulins
• Synthesized in the liver
• Most clinically significant β globin include transferrin
• Transferrin plays an important role in the body’s metabolism of iron – it binds free iron and transports it
• Transferrin levels are decreased in liver disease, chronic infections, and nephrosis
• Transferrin levels are increased in iron deficiency anaemia
Globulins
-Gamma (y) globulins (predominantly immunoglobulins and CRP)
• Major part are immunoglobulins (antibodies)
• They are produced by the lymphocytes and their main function is in immunity
• Each immunoglobulin is composed of two heavy chains and two light chains. There are five classes of immunoglobulins:
➢ IgG – Major immunoglobulin present. Involved in memory response to antigens already encountered
➢ β IgM - Synthesized by the cells in primary immune response.
➢ IgE – involved in allergic response
➢ IgA – 1st antibody synthesized in primary immune response
➢ IgD – Function mainly as antigen on receptor on B cells that have not yet been exposed to antigens
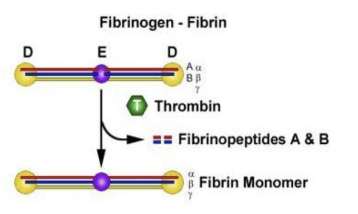
Fibrinogen
also known as coagulation factor 1
fibrinogen accounts for 4% of plasma proteins
produced by the liver
important as a clotting factor
fibrinogen plays an important role in clotting of blood where it is converted to fibrin by thrombin
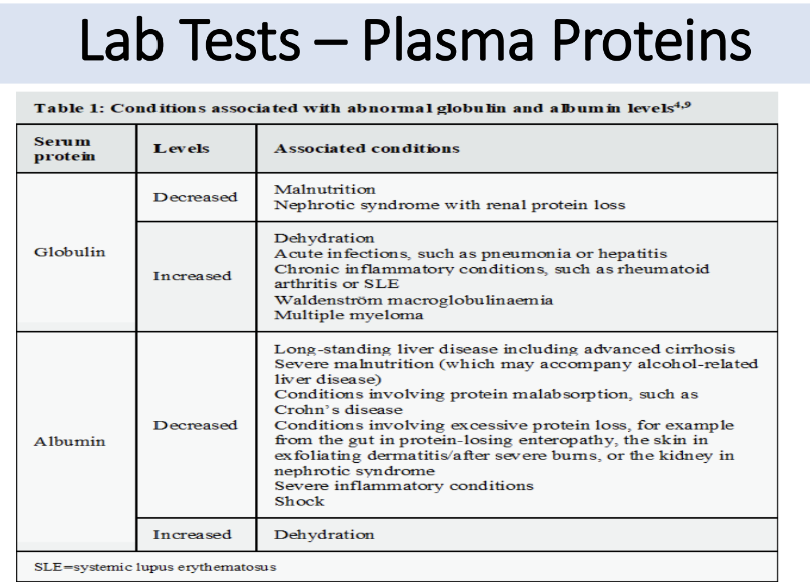
Lab tests - Plasma Proteins
plasma proteins - heterogenous in nature and involved in many complex functions within the body
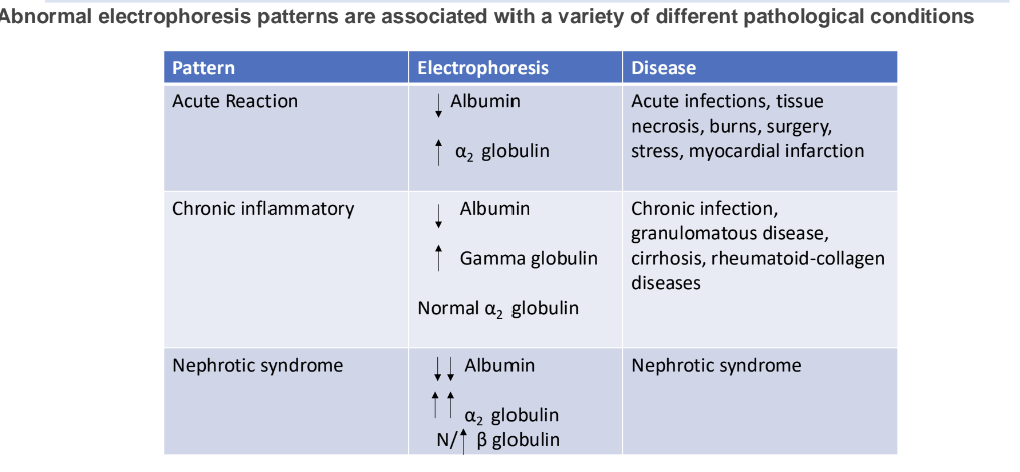
abnormalities in plasma proteins may be primary- the cause of specific pathologies or secondary - the result of a wide range of disease processes.
abnormal proteinuria can also result from various medical conditions
clinical biochemistry labs routinely measures total protein and albumin usually in serum
globulin fraction = total protein- albumin
other plasma proteins ex. immunoglobulins are measured as classes
immunochemical methods are use to measuring specific plasma proteins , hormones or enzymes
serum albumin and globulin are a measure of nutrition
decreased protein levels is seen in:
malnourished patients especially after surgery
burn patients
pregnancy during the third trimester
decreased albumin and normal or increased globulin levels:
collagen vascular diseases ex. lupus erythematosus - where capillary permeability is increased and albumin being smaller than globulin is lost in the extravascular space
chronic liver disease - liver can’t produce albumin, but globulin is adequately made in the reticuloendothelial systems
in these diseases the albumin level is low but total protein level is normal because of increased globulin level- these changes can be detected if one measures the albumin/globulin ratio; increased protein and albumin levels can be seen in dehydration
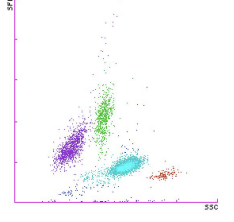
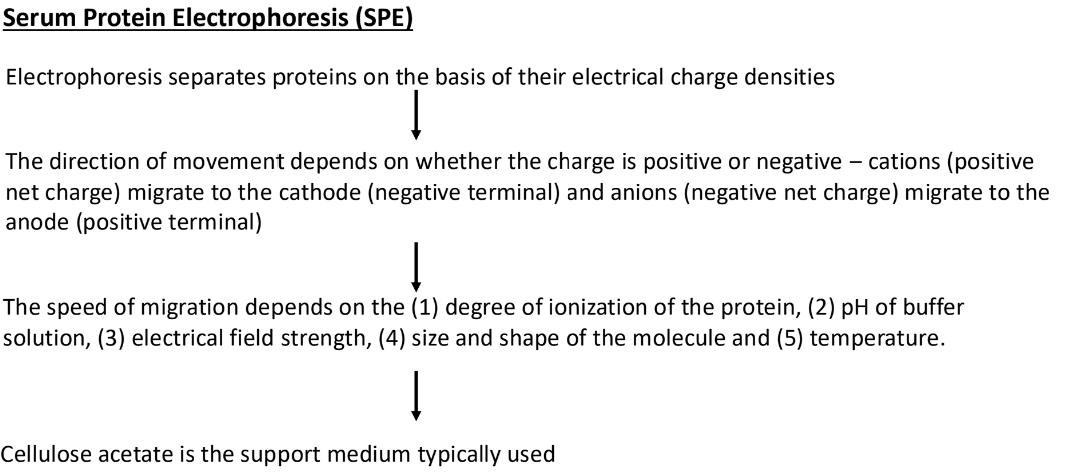
Serum Protein Electrophoresis
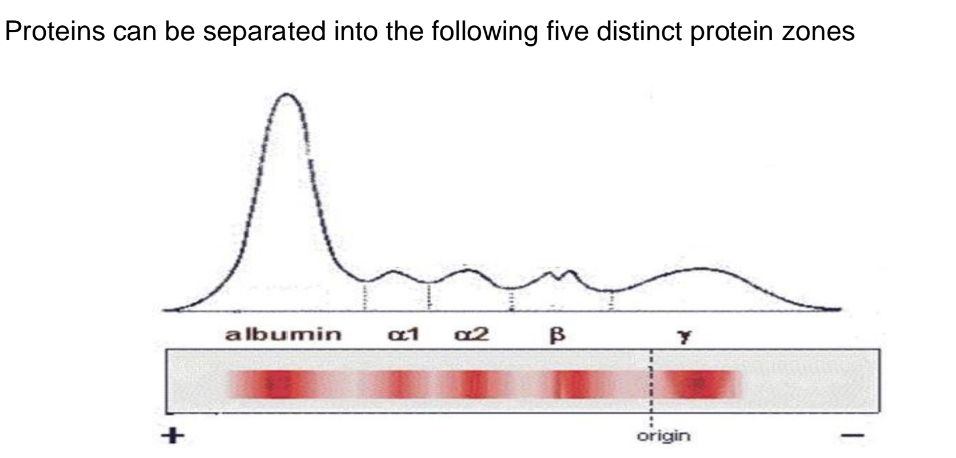
Serum protein electrophoresis is generally considered in any patient with an elevated total protein, especially those with elevated globulin level relative to albumin, or any signs and symptoms suggestive of an underlying plasma cell disorder such as multiple myeloma, Waldenstrom’s macroglobulinemia, or primary amyloidosis. These include any of the following:
• Unexplained anaemia, back pain, bone pain, fatigue
• Unexplained pathologic fracture or lytic lesions
• Unexplained peripheral neuropathy
• Hypercalcemia secondary to possible malignancy
• Hypergammaglobulinemia
• Rouleaux formation noted on peripheral blood smear
• Renal insufficiency with bland urine sediment
• Unexplained proteinuria
• Bence Jones proteinuria
• Recurrent infections
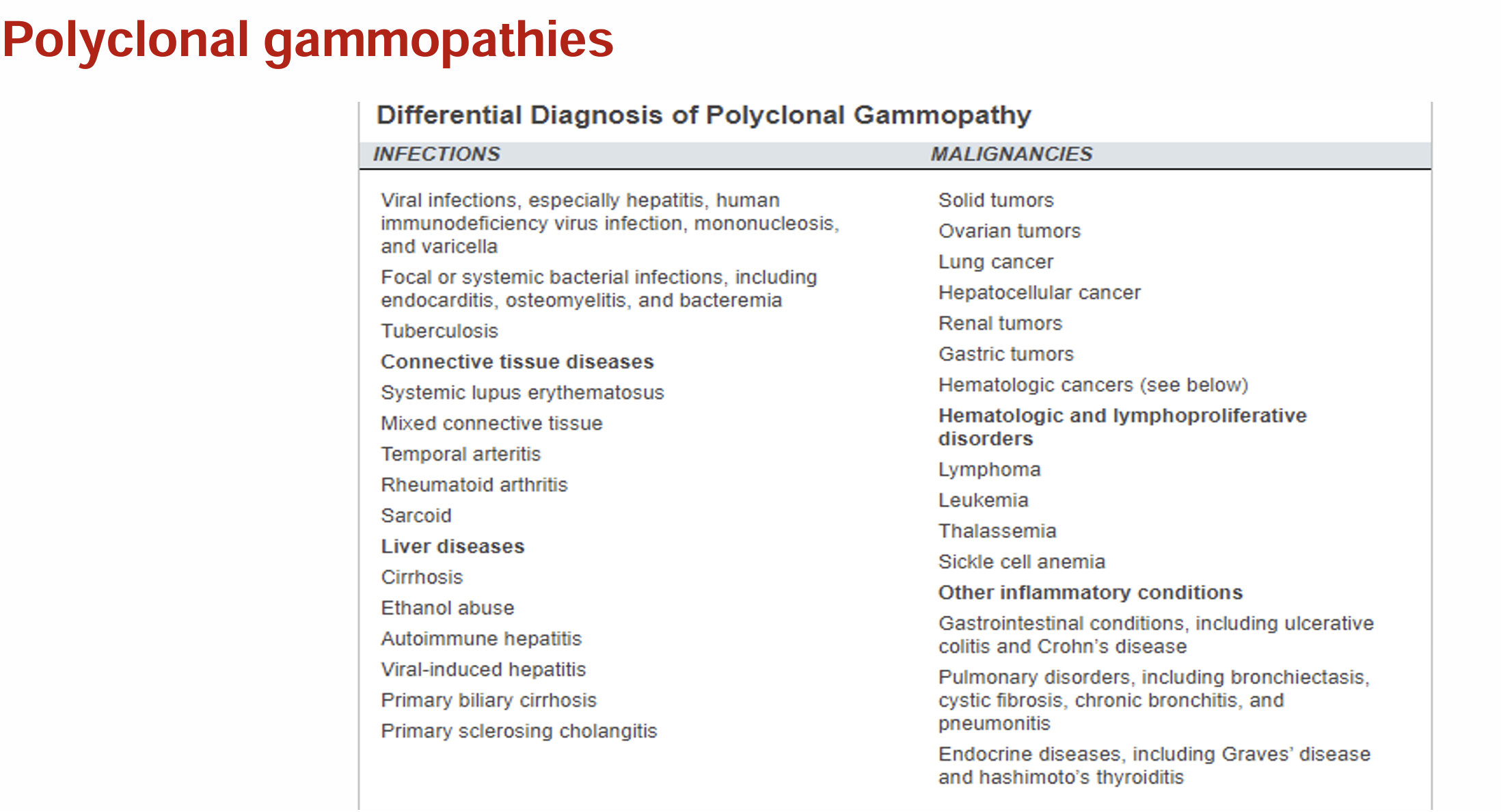
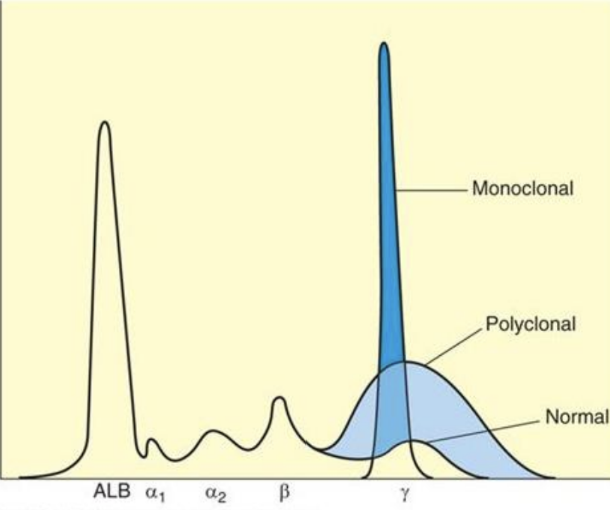
increase in gamma globulins can be either monoclonal or polyclonal
it is extremely important to differentiate monoclonal from polyclonal gammopathies: -
monoclonal gammopathies - associated with a clonal process that is malignant or potentially malignant
polyclonal gammopathies - may be caused by any reactive or inflammatory process, and they usually are associated with non-malignant conditions
Monoclonal Gammopathies
multiple myleoma- neoplastic proliferation characterized by plasma cell accumulation in the bone marrow; 98% of cases occur over the age of 40 yrs with a peak incidence in the 7th decade ; Signs of monoclonal gammopathies :-
monoclonal protein in serum and/or urine
increased plasma cells in bone marrow
bone pain resulting from verbal collapse and pathological fractures
features of anaemia
recurrent infections
features of renal failure
abnormal bleeding tendency
examples of monoclonal gammopathies:-
Waldenstrom’s macroglobulinaemia – rare condition seen most frequently in men over 50 years of age. 1st finding is the monoclonal band on SPE together with bone marrow showing infiltration of lymphocytes and plasma cells.
Solitary plasmacytoma – Isolated plasma cell tumours, usually of bone or soft tissue (e.g.the mucosa of the upper respiratory and gastrointestinal tracts or the skin).
Plasma cell leukaemia – Occur either as a late complication of myeloma or as a primary disease characterized by the presence of 20% or more of plasma cells in blood.
Monoclonal gammopathy of undetermined significance (MGUS) – when you have a monoclonal band on SPE without any evidence of myeloma or other underlying disease. Its common with age. These subjects show no bone lesions and the proportion of plasma cells in the marrow is normal.